Aetiology of sepsis in adults living with HIV in East Africa: a secondary analysis of an open-label, multicentre, randomised, controlled phase 3 trial
Eva Otoupalova, Lucas Ampaire, Megan Null, Buliga Mujaga, Jie Liu, Bibie Said, Edwin Nuwagira, Margaretha Sariko, Geofrey Gidoi, Antony Gulinja, Samuel Jjunju, Arestaricky Rimoy, Fredrick C. Mwita, Jeremiah Kidola, Oscar Atwiine, David Ocaaki, Dalton K. Munyambalu, Prakruti Rao

TL;DR
This study identifies Mycobacterium tuberculosis as the most common cause of sepsis in HIV-positive adults in East Africa, highlighting limitations in current diagnostic methods.
Contribution
The study provides new insights into sepsis etiology in HIV-positive adults in East Africa, emphasizing the under-detection of tuberculosis by rapid tests.
Findings
Mtb was detected in 52% of sepsis cases and 50% of bloodstream infections.
Conventional diagnostics missed 32% of Mtb bloodstream infections.
High ceftriaxone resistance was observed in non-mycobacterial bacteria.
Abstract
Sepsis in people living with HIV (PLWH) in East Africa has high mortality. Regionally, the etiology of sepsis is incompletely understood. We performed a planned analysis of the microbiological data obtained from a randomised clinical trial of early empiric anti-Mycobacterium tuberculosis (Mtb) therapy for sepsis (ATLAS) in Tanzania and Uganda. We present a prespecified, secondary analysis of a phase three, open-label, multicentre, randomised, controlled trial conducted at four regional referral hospitals in Tanzania and Uganda. Participants were adults living with HIV admitted with concern for infection and a modified quick sepsis-related organ failure assessment (qSOFA) ≥2. Participants were randomised to (1) immediate or diagnosis-dependent antituberculosis therapy and to (2) high-dose or conventional-dose antituberculosis therapy. Tests for sepsis etiology included bacterial blood…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
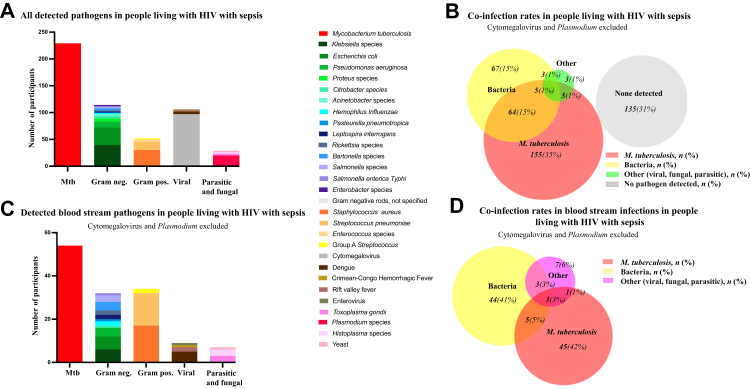 Figure 1
Figure 1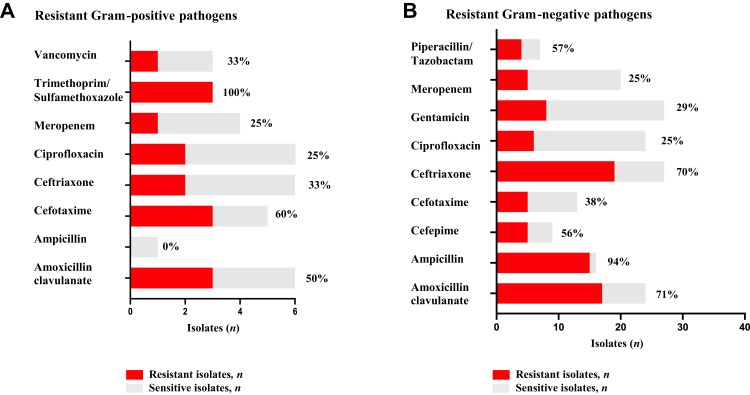 Figure 2
Figure 2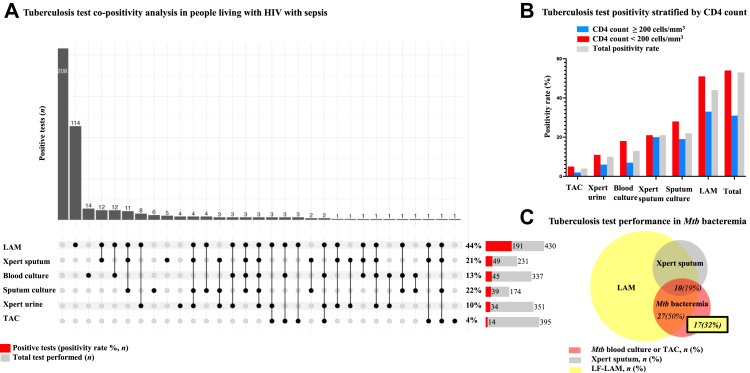 Figure 3
Figure 3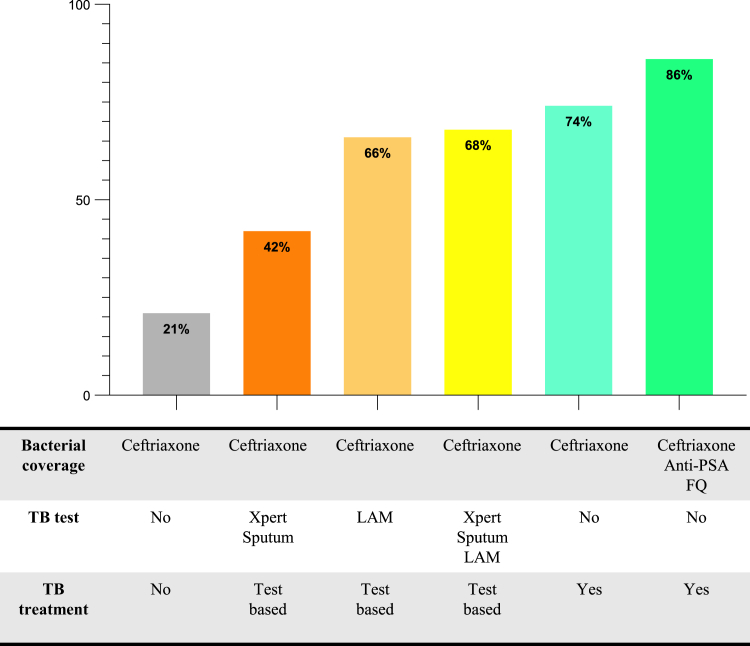 Figure 4
Figure 4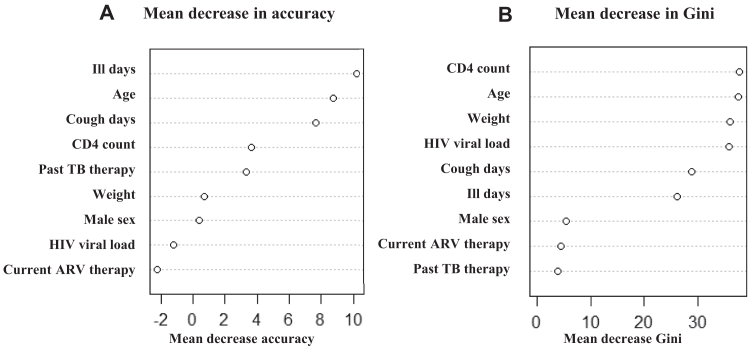 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPneumocystis jirovecii pneumonia detection and treatment · Tuberculosis Research and Epidemiology · Sepsis Diagnosis and Treatment
Research in contextEvidence before this studyWe searched PubMed, Embase, and MEDLINE for studies investigating sepsis etiology in low- and middle-income countries (LMICs) from database inception up to July 29, 2025, with the terms “sepsis”, “etiology” and “Africa”. Of the 20 studies that we identified from Africa that examined sepsis etiology, 11 were performed in adults, and out of those, most studies included a subgroup of PLWH. The most frequent cause of HIV-associated sepsis in Africa was Mtb infection (9–27%) followed by Streptococcus pneumoniae (9%–15%). Although Mtb was the most frequently isolated pathogen, only a small number of studies specifically assessed for Mtb bacteremia. Furthermore, only one study performed WHO-recommended rapid tuberculosis (TB) testing with urine lateral flow lipoarabinomannan antigen (LF-LAM) and sputum nuclear acid amplification tests on all enrolled participants. Additionally, most of the studies were only able to identify a small proportion of causative sepsis pathogens, and only three studies included blood or tissue PCR to evaluate for less common bacterial and viral pathogens. Therefore, the underlying microbiology of sepsis is in PLWH in Africa is unclear, and the optimal diagnostic and treatment strategies remain unknown.Added value of this studyIn this study, we identified Mtb in 229 (52%) of 437 study participants presenting with sepsis, which was a higher proportion than previous studies given our comprehensive testing. We found that combined urine LF-LAM and sputum GeneXpert MTB/RIF testing missed 32% of Mtb bloodstream infections and identified a high prevalence of ceftriaxone resistance among non-Mtb bacterial isolates. These findings highlight the limitations of current WHO tuberculosis diagnostics, the need to evaluate test performance in HIV-related sepsis, and the importance of developing evidence-based, pathogen-specific empiric antibiotic strategies in high HIV/tuberculosis prevalence settings.Implications of all the available evidenceOur study, in combination with previous literature, suggests that empirical regimens for PLWH with sepsis in tuberculosis endemic regions should include treatment of Mtb and account for other ceftriaxone-resistant bacteria. Our study is a pre-specified secondary analysis of a clinical trial and as such was not designed for assessing drug resistance; however, the detected resistance patterns agree with reported rising rates of cephalosporin resistance in the African continent.
Introduction
Sepsis is a syndrome of dysregulated host response to infection leading to organ dysfunction and has a high associated mortality.1^,^2 The annual incidence of sepsis is estimated at 48 million cases worldwide, and 85% of cases occur in low- and middle-income countries (LMICs). Despite advances in sepsis diagnostics and treatment, sepsis continues to cause approximately 11 million deaths globally every year, most of which are preventable.3 Despite the disproportionate burden of sepsis in LMICs, the data that support recommendations for sepsis management come overwhelmingly from high-income countries (HICs). Furthermore, some treatments adopted from HICs, such as liberal administration of fluids to patients presenting with sepsis, are harmful to patients in LMICs.4^,^5
With case fatality rates as high as 39%, Africa is one of the regions most affected by sepsis.6 The reasons are likely multifactorial and include the relative lack of high-quality studies on sepsis etiology and antimicrobial resistance. Importantly, most sepsis-related deaths in Africa occur among people living with human immunodeficiency virus (PLWH).7 Sepsis in PLWH can be caused by a wide spectrum of pathogens including Mycobacterium tuberculosis (Mtb), other non-Mtb bacteria, fungi, viruses, and other co-infections. We and others have shown in observational studies that 37–55% of PLWH with sepsis in East Africa tested positive for Mtb, and a third were co-infected with another pathogen.8^,^9 Despite the high prevalence of Mtb sepsis, few studies from Africa have focused on Mtb detection from blood and have instead used urine diagnostics such as lateral flow testing for lipoarabinomannan (LF-LAM) or sputum-based diagnostics such as GeneXpert MTB/RIF or GeneXpert MTB/RIF Ultra. Sputum testing may lead to an underestimation of Mtb as a causative pathogen in PLWH with sepsis in Africa given the paucibacillary nature and extrapulmonary dissemination of tuberculosis among PLWH, and the difficulty with expectoration among the critically ill.
Delayed diagnosis and inappropriate initial antibiotic selection correlate with increased sepsis mortality.10 Current antimicrobial treatment for sepsis in most regions of Africa consists of a third-generation cephalosporin, which is typically ceftriaxone. Per World Health Organization guidelines, tuberculosis treatment is initiated only after a positive result from a rapid diagnostic test, or when clinical deterioration occurs despite several days of standard antibiotic therapy.11 It is therefore imperative to develop regionally appropriate standard diagnostic algorithms and antibiotic regimens for PLWH with sepsis that more accurately reflect the underlying sepsis etiology. Since inappropriate antibiotic therapy is associated with an increased risk of death from sepsis, understanding regional microbiology is key to improving sepsis survival. However, a significant knowledge gap regarding sepsis etiology in regions of Africa, especially among PLWH, still exists. Therefore, we performed an analysis of comprehensive microbiological testing of blood, urine, and sputum from all participants enrolled in a multicenter randomised controlled trial of immediate and/or high dose antituberculosis therapy compared to standard therapy in PLWH presenting with sepsis in Tanzania and Uganda.12
Methods
Study design, settings, and participants
This study is a prespecified, secondary analysis of a randomised clinical trial of early empiric anti-M. tuberculosis therapy for sepsis in sub-Saharan Africa (ATLAS trial).12 ATLAS trial was a multicenter, phase three, open label, randomised, 2 × 2 factorial trial to evaluate empiric early and/or high dose anti-TB therapy versus standard antibiotic therapy in participants admitted with clinical concern for sepsis to the regional referral hospitals Kibong'oto Infectious Diseases Hospital and Sekou Toure Regional Referral Hospital in Tanzania, and the Mbarara Regional Referral Hospital and Fort Portal Regional Referral Hospital in Uganda (NCT 04618198). We enrolled participants if they were ≥18 years old, living with HIV in Tanzania or Uganda, and were admitted to one of the study hospitals with presumed sepsis. We defined sepsis as clinical concern for infection and a modified quick sepsis-related organ failure assessment (qSOFA) ≥2 of the following: Glasgow coma scale score <15, a respiratory rate ≥22 breaths per minute, a systolic blood pressure ≤90 mmHg, or a mean arterial pressure of ≤65 mmHg. We excluded potential participants if they were treated with antibiotics at another inpatient facility for over 24 h prior to screening, were receiving or had received antituberculosis therapy in the last year, were pregnant, or had known liver disease or end-stage renal disease. We excluded potential participants with a positive whole blood cryptococcal antigen (CrAg) test from further testing and treatment due to their high case fatality rates, which would have biased the trial results. We collected clinical and laboratory data from each participant. Participants were randomised to (1) immediate or diagnosis-dependent antituberculosis therapy, and (2) high-dose rifampicin (30 mg/kg) and isoniazid (7.5 mg/kg) with conventional-dose ethambutol and pyrazinamide, or conventional-dose four-drug antituberculosis therapy for 28 days. Each patient also received ceftriaxone for 7 days. Randomisation was performed with computer-generated permuted-block algorithm which randomly assigned participants with equal probability to receive either immediate or diagnosis-dependent antituberculosis therapy and either high-dose or conventional WHO-recommended weight-based dose antituberculosis therapy. Only the trial coordinator and statistician were aware of mortality outcomes before study completion. All analyses presented in the manuscript were included as part of the prespecified secondary outcome of final sepsis etiology. The ATLAS trial received approval from the University of Virginia (HSR200253), the Tanzania Medicines and Medical Devices Authority (TMDA-WEB0021/CTR/0008/03) and National Institute for Medical Research (NIMR/HQ/R.8a/Vol. IX/3554), and the Uganda National Council for Science and Technology (HS1272ES). Informed consent was obtained from all individual participants included in the study, or, if unable to consent, from their caregiver or next of kin. The trial was performed according to published trial protocol.12^,^13 Sex at birth was obtained by self-report. As the study did not investigate identity or other psychosocial or cultural factors, gender was not assessed. The trial was conducted in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines to ensure transparency and completeness in reporting randomized controlled trials.
Pathogen testing
Each participant underwent testing for sepsis etiology with blood (BacTec 9050) and urine culture. For evaluation of tuberculosis, all participants able to produce specimens underwent WHO-approved rapid tuberculosis diagnostic testing including GeneXpert MTB/RIF or GeneXpert MTB/RIF Ultra on sputum and urine, Alere Determine LF-LAM on urine, as well as mycobacterial culture of sputum (MGIT 960 system) and blood (BACTEC Myco/F system). Additionally, we tested blood with the multiplex qPCR TaqMan Array Card (TAC) assay, which targeted 43 pathogens (Supplementary Table S1) associated with febrile illness in East Africa, in batch analysis as previously described.14 We defined a positive target in the TAC assay as a cycle threshold <35. We tested for malaria parasites with the qPCR TaqMan Array Card (TAC) assay.
We defined tuberculosis as one or more positive tuberculosis test results. We defined a sepsis pathogen as any pathogen detected in urine or blood except for cytomegalovirus (CMV) and Plasmodium species, as they uncommonly cause sepsis in adults in East Africa,15^,^16 and incidental parasitemia or CMV antigenemia can occur asymptomatically in people with other critical illness. We defined bloodstream infection as a positive Mtb or non-Mtb bacterial blood culture, or a positive blood TAC assay for other causative pathogens except for CMV or Plasmodium species. We classified coagulase-negative staphylococci, Micrococcus, or further unidentifiable anaerobic bacterial growth as culture contaminants. The ATLAS trial did not include mandatory drug sensitivity testing; however, it was performed at the treating physician's discretion per local practice.
Statistical analysis
We used descriptive statistics to calculate the distribution of non-Mtb bacterial, viral, fungal, protozoal, and Mtb infections and bloodstream infections in our cohort. We performed all descriptive analyses with simple frequencies. We used GraphPad Prism (version 10.2.3) for data analysis and data visualization. We created proportional Venn diagrams to determine the percentage of co-infections using the DeepVenn application,17 and non-proportional Venn diagrams using the online tool https://bioinformatics.psb.ugent.be/cgi-bin/liste/Venn. We created UpSet plots to determine the rates of TB tests co-positivity using the “Upset” package in RStudio (Version 2024.09.0+375).
We determined the most important variables predicting Mtb as a causative organism of sepsis through multivariable logistic regression analysis and a random forest algorithm conducted with the “randomForest” package in RStudio.18 Predictors included age, sex, weight, past Mtb disease, duration of illness before hospitalization, days of cough, current antiretroviral treatment, CD4+ T-cell concentration, and detectable HIV viral load. For the random forest model, we performed imputation for variables missing data and we generated the final dataset after ten iterations using the rfImpute function from the “randomForest” package. We stratified the sample into training (67%) and validation (33%) datasets, then performed Bootstrap sampling to generate multiple training datasets of the same total sample size for improved model robustness and to reduce overfitting. We calculated the mean decrease in accuracy, which measures the individual contribution of each variable, and the mean decrease Gini, to rank the importance of variables. We considered the remaining 33% of the dataset, which was not part of the bootstrap sample, to be out-of-bag samples. We determined the out-of-bag error rate, which indicated the model performance, through the “caret” package.19 Finally, we calculated accuracy, precision, recall, and F1-scores. Missing data for variables studied in random forest model was approximately 10%.
To determine to what degree an expanded antimicrobial regimen could improve antimicrobial coverage of sepsis in PLWH, we calculated the proportion of patients with Mtb that was missed by conventional WHO recommended GeneXpert MTB/RIF or GeneXpert MTB/RIF Ultra, and urine LF-LAM, and the proportion of pathogens that would not be expected to be treated with ceftriaxone alone.
Role of the funding source
The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. The authors had full access to the data in the study. EO and CCM had final responsibility for the decision to submit for publication.
Results
Baseline characteristics
The ATLAS trial screened 707 participants for eligibility. We excluded 30 (4%) for positive cryptococcal antigen test and 240 (34%) for other reasons. Between January 5, 2022 and December 9, 2024, we randomised 437 participants. After late exclusions due to kidney or liver injury, we included 395 participants in the analysis of the primary 28-day mortality outcome; however, we included all 437 randomised participants in our secondary microbiology analysis (Supplementary Figure S1). A cryptococcal antigen test was positive in 30 (4%) of 707 screened potential participants, while TAC detected Cryptococcus in 1 (<1%) of 437 randomised participants. The median (interquartile range [IQR]) participant age was 42 (33–51) and 233 (53%) of 437 participants were female (Table 1). All participants were PLWH with a median (IQR) CD4+ T-cell concentration of 120 (29–332) and 244 (73%) of 337 tested patients had a detectable HIV viral load. Of the 437 randomised participants, 209 (48%) were receiving antiretroviral at the time of presentation. Those not already receiving antiretroviral therapy initiated it after admission to hospital per standard of care and treating physician discretion. The median (IQR) qSOFA score and Universal Vital Assessment (UVA) score were 2 (2) and 4 (4–6), respectively.20Table 1. Baseline characteristics of participants in a randomized clinical trial of early empiric anti-Mycobacterium tuberculosis therapy for sepsis in sub-Saharan Africa (ATLAS trial).VariableValueAge, years, median [IQR]42 [33–51]Female sex, n participants (%)233 (53)ART on admission, n participants (%)209 (48)Baseline CD4 count, cells/mm^3^, median [IQR]120 [29–332]Viral load, detectable, n participants (%)244 (73)Duration of illness prior to admission, days [IQR]29 [14–60]History of TB treatment prior to admission, n participants (%)38 (9)Systolic blood pressure mmHg, median [IQR]88 [82–90]Heart rate, beats/min, median [IQR]120 [104–127]Respiratory rate, beats/min, median [IQR]26 [24–30]Oxygen saturation, %spO 2, median [IQR]95 [92–98]qSOFA score [IQR]2 [2]UVA score [IQR]4 [4–6]All values rounded to integer except frequencies lower than 1. ART = anti-retroviral therapy; qSOFA score = modified quick sequential organ failure assessment score; UVA score = universal vital assessment score.
Sepsis etiology
Of the 437 randomised participants, 302 (69%) had a detectable sepsis pathogen, 31 (7%) from blood alone, 146 (33%) from urine alone, 11 (3%) from sputum alone, and 77 (18%) from blood and another source (Supplementary Figure S2). We detected Mtb from one or more specimens in 229 (52%) participants*,* bacterial pathogens in 139 (32%) participants and other non-CMV viral, fungal, and non-Plasmodium parasitic pathogens in 16 (4%) participants (Fig. 1A and B and Table 2). We did not detect any non-tuberculous mycobacteria. Co-infection with non-CMV and non-Plasmodium organisms occurred in 77 (18%) of 437 participants (Fig. 1B). Of the 229 participants with tuberculosis identified by any test, 74 (17%) had a co-infection other than Plasmodium or CMV. CMV was detected concomitantly with 55 (24%) of 229 Mtb infections and 31 (22%) of 139 non-tuberculosis bacterial infections (Supplementary Figure S3A). Plasmodium was detectable with 6 (3%) of 229 Mtb infections and 14 (10%) of 139 bacterial infections (Supplementary Figure S3B).Fig. 1Sepsis etiology in sub-Saharan Africa. (A) Bar graph showing number of participants with detected pathogen. (C) Bar graph showing number of participants with detected pathogen bloodstream infection. Cytomegalovirus, Cryptococcus and Plasmodium were excluded. (B) Proportional Venn Diagram showing rates of co-infections in the study (n = number of participants; % percent of all participants included). (D) Proportional Venn Diagram showing rates of blood stream co-infections (n = number of participants; % percent of all participants with bloodstream infection); Cytomegalovirus, Cryptococcus and Plasmodium were excluded.Table 2. Microbiology of all detected organisms from participants in a randomized clinical trial of early empiric anti-Mycobacterium tuberculosis therapy for sepsis in sub-Saharan Africa (ATLAS trial).OrganismBlood (n isolates, positive)Urine (n isolates, positive)Sputum (n isolates, positive)Total (n, participants)Total (% of all participants)Mycobacterium tuberculosis542004922952.4Gram positive bacteria Staphylococcus aureus1717306.7 Streptococcus pneumoniae15153.4 Enterococcus species551.1 Group A Streptococcus220.5Gram negative bacteria Klebsiella species733398.9 Escherichia coli628337.6 Pseudomonas aeruginosa47112.5 Proteus species661.4 Citrobacter species1451.1 Bartonella species440.9 Salmonella species330.7 Acinetobacter species330.7 Coxiella burnetii220.5 Haemophilus influenzae220.5 Leptospira interrogans220.5 Rickettsia species220.5 Enterobacter species220.5 Salmonella enterica Typhi110.2 Pasteurella Pneumotropica110.2 Gram negative rods, unspecified110.2Viruses Cytomegalovirus969622.0 Dengue551.1 Rift Valley Fever220.5 Crimean Congo Hemorrhagic Fever110.2 Enterovirus110.2Fungi and parasites Plasmodium species20204.6 Yeast1230.7 Histoplasma species330.7 Toxoplasma gondii330.7 Cryptococcus neoformansa31a31aNAaa31 out of 707 screened participants were positive for cryptococcus (30 with positive CrAg, 1 with TAC). Participants with positive CrAg were excluded from the trial, therefore % positive participants is not available.
Of 108 participants with a bloodstream infection, we detected Mtb, non-Mtb bacterial pathogens, or other pathogens in 54 (50%), 55 (51%), and 14 (13%) participants, respectively (Fig. 1C and D and Table 3). Of the 54 Mtb positive test results from blood samples, we detected 45 (83%) by mycobacterial blood culture only, 5 (9%) from blood culture and qPCR TAC assay, and 9 (17%) from qPCR TAC assay only. Of the 55 cases of non-Mtb bacterial bloodstream infection, we detected 12 (22%) by bacterial blood culture and 45 (82%) by TAC (Table 3). Seven participants tested positive for more than one non-Mtb bacterial pathogen in blood. Staphylococcus aureus and S. pneumoniae were the most common non-Mtb bacterial bloodstream pathogens*,* followed by Klebsiella species, Escherichia coli, Pseudomonas aeruginosa and Bartonella species (Fig. 1C and Table 3). We also detected Group A Streptococcus, Salmonella, Citrobacter, Coxiella burnetii and Leptospira by TAC and in culture. Additionally, we detected several non-bacterial pathogens including Dengue*,* Rift Valley Fever*,* Enterovirus, Histoplasma, and Toxoplasma in blood by TAC*. Klebsiella* species, E. coli, and S. aureus were the most frequently isolated urinary pathogens. The prevalence of Mtb sepsis in Tanzania was 60% compared to 43% in Uganda (odds ratio [OR] 2.01, 95% confidence interval [CI] 1.37–2.95, p = 0.0004) (Supplementary Table S2).Table 3. Bloodstream infection etiology in participants in a randomized clinical trial of early empiric anti-Mycobacterium tuberculosis therapy for sepsis in sub-Saharan Africa (ATLAS trial).OrganismCulture (n, positive isolates)TaqMan Array (n, positive isolates)Total (n, patients)Total (% of patients with blood stream infection)Mycobacterium tuberculosis45145442Gram positive bacteria Staphylococcus aureus4131716 Streptococcus pneumoniae2131514 Group A Streptococcus0222Gram negative bacteria Escherichia coli0666 Klebsiella species1666 Pseudomonas aeruginosa3144 Bartonella species0444 Salmonella species1233 Coxiella burnetii0222 Haemophilus influenzae0222 Leptospira interrogans0222 Rickettsia species0222 Citrobacter species1011 Salmonella enterica Typhi0111 Pasteurella pneumotropica0011Viruses Dengue555 Rift Valley Fever222 Crimean Congo Haemmorhagic Fever111 Enterovirus111Fungi and parasites Yeast111 Histoplasma species333 Toxoplasma gondii333All frequencies rounded to integer.
Bacterial resistance
Drug susceptibility data from routine clinical care were available for 46 (33%) of 139 cultured non-Mtb bacterial isolates. We detected ceftriaxone resistance in 21 (64%) of 33 isolates for which the drug was tested (Fig. 2A and B and Supplementary Tables S3 and S4). We isolated P. aeruginosa, which is intrinsically resistant to ceftriaxone, in 5 (11%) of 46 cultures with available drug sensitivity, and in 4 (7%) of 55 non-Mtb bloodstream infections.Fig. 2Proportion of resistant bacterial pathogens isolated in people living with HIV with sepsis. Bar graph showing frequency of detected Gram-positive (A) and Gram-negative (B) drug resistant bacteria in the subset of isolates with DST (n = number of resistant isolates; % = percent resistant isolates; Pseudomonas counted as resistant to Ampicillin, Ceftriaxone, Cefotaxime, Amoxicillin clavulanate, Trimethoprim/Sulfamethoxazole and Vancomycin regardless of in vitro DST results). DST = Drug sensitivity testing.
Tuberculosis testing
Of the 437 randomised participants 229 (52%) had a positive tuberculosis test result. Urine LF-LAM and Mtb blood cultures were the most common tests to be positive alone without another positive tuberculosis test (positive alone in 114 and 14 participants, respectively) (Fig. 3A and Table 4). There was no other common pattern of overlapping test positivity. LF-LAM was positive in 191 (44%) of 430 tests, sputum culture was positive in 39 (22%) of 174 tests, sputum GeneXpert MTB/RIF was positive in 49 (21%) of 231 tests, and urine GeneXpert MTB/RIF was positive in 34 (10%) of 351 tests. One MTB/RIF test revealed rifampin resistance and 5 had indeterminate results. All cultured Mtb was rifampin susceptible by phenotypic testing.Fig. 3Tuberculosis test diagnostic performance in people living with HIV with sepsis in sub-Saharan Africa. (A) Upset plot showing intersection size of performed TB tests in all included trial participants with sepsis, and associated bar graph showing positivity rate for each test. N = intersection size. LAM = urine lateral flow lipoarabinomannan; Xpert = GeneXpert MTB/RIF or GeneXpert MTB/RIF Ultra; TAC = TaqMan Array Card PCR assay. (B) Rate of TB test positivity based on CD4 count. (C) Proportional Venn Diagram showing detection of Mtb bacteremia by LF-LAM and Xpert Sputum (n = number of participants; % = percent of all participants with Mtb bacteremia).Table 4TB test positivity rate stratified by CD4+ T-cell concentration among participants in a randomized clinical trial of early empiric anti-Mycobacterium tuberculosis therapy for sepsis in sub-Saharan Africa (ATLAS trial).TB testTotal testedTotal resultedPositive of resulted (%)CD4 < 200 (%)CD4 ≥ 200 (%)TaqMan Array426395452Xpert MTB/RIF urine35135110116Mtb blood culture36733713187Xpert MTB/RIF sputum231231212120Mtb sputum culture184174222819Urine LF-LAM430430445133All437435535431All frequencies rounded to integer. LAM = urine lateral flow lipoarabinomannan; Gene/Xpert MTB/RIF or Gene/Xpert MTB/RIF Ultra; TAC = TaqMan Array Card PCR assay.
Of the 162 participants with a positive tuberculosis test and known CD4+ T-cell concentration, 103 (64%) had a CD4+ T-cell concentration <200 cells/mm^3^. Among participants with a CD4+ T-cell concentration <200 cells/mm^3^, the LF-LAM test positivity rate was 51% compared to 33% for those with ≥200 cells/mm^3^ (OR 0.47, 95% CI 0.30–0.77, p = 0.0023) and Mtb blood culture positivity was 18% compared to 7%, respectively (OR = 0.33, 95% CI 0.12–0.84, p = 0.02) (Fig. 3B and Supplementary Figures S4 and S5). Of the 54 Mtb bloodstream infections detected by culture or TAC, urine LF-LAM was positive in 27 (50%) and sputum GeneXpert MTB/RIF and urine LF-LAM were both positive in 10 (19%) instances. Therefore, rapid WHO-recommended tests missed 17 (32%) of Mtb bloodstream infections (Fig. 3C).
Predicted improvement in sepsis antimicrobial coverage with expanded diagnostics and regimen composition
Based on the observed frequency of ceftriaxone-resistant pathogens and the proportion of patients with Mtb infection that were missed by conventional WHO-recommended first-line diagnostics, a regimen consisting of only ceftriaxone without TB testing or anti-Mtb treatment would appropriately treat 21% of identified pathogens (Fig. 4 and Supplementary Table S5). In comparison, urine LF-LAM and sputum GeneXpert MTB/RIF testing-based early anti-TB therapy initiation, in combination with ceftriaxone treatment, would appropriately treat 68% of identified pathogens. An expanded spectrum antimicrobial regimen that included empirical anti-TB therapy and antibacterials active against ceftriaxone susceptible and resistant non-Mtb bacteria such as P. aeruginosa, would treat 86% of identified and plausibly causative sepsis pathogens (not accounting for Cryptococcus species excluded from the patient population, and possible pathogens of Plasmodium species).Fig. 4Predicted antimicrobial coverage of people living with HIV with sepsis with expanded diagnostics and regimen composition. Bar graph showing predicted antimicrobial coverage in PLWH with sepsis with ceftriaxone only, ceftriaxone and TB testing-based TB treatment, and expanded antimicrobial regimen with ceftriaxone, anti-PSA antibiotics and anti-Mtb antimicrobials. Xpert = GeneXpert MTB/RIF or GeneXpert MTB/RIF Ultra; LAM = urine lateral flow lipoarabinomannan; anti-PSA FQ = anti-pseudomonal fluoroquinolone.
Clinical prediction of Mtb detected by one or more laboratory methods
The baseline clinical variables in participants with and without positive TB tests are depicted in Table 5. Multivariable logistic regression analysis of these variables did not yield any significant predictors of TB tests positivity (Supplementary Table S6). From the random forest analysis, a greater number of ill days before presentation, younger age, a greater number of days of cough, lower CD4+ T-cell concentration, no prior anti-TB therapy, and male sex were associated with Mtb as a sepsis etiology. The mean decrease in accuracy and mean decrease in Gini are shown in Fig. 5 and Supplementary Table S7. However, the out-of-bag error rate was high at 41%, with accuracy and precision of 0.6 and 0.5, respectively. The recall was 0.6, and the F1-Score was 0.5. The Lasso regression model and XGBoost analysis results are shown in Supplementary Table S8 and Supplementary Figure S6, respectively.Table 5. Baseline variables of participants with TB positive or TB negative test results in a randomized clinical trial of early empiric anti-Mycobacterium tuberculosis therapy for sepsis in sub-Saharan Africa (ATLAS trial).VariableMtb positiveMtb negativeOdds ratio95% Confidence intervalp-valueAge (years), median (IQR)40 (32–50)43 (35–54)---****---****0.007Weight (kg), median (IQR)48.5 (44–55)50 (45–58)---****---****0.025Sex, male (%)4944**------nsPast TB treatment (%)6120.44[0.22–0.88]0.02Ill days, n, median (IQR)30 (14–60)21 (14–56)------0.005Cough days, n, median (IQR)30 (14–30)30 (17–45)------nsCD4 cells/mm^3^, median (IQR)90 (27–322)138 (37–352)------nsCurrent ART (%)4453------nsAll values rounded to integer except values lower than 1. Mann–Whitney test and odds-ratios were used for statistical analysis. p values < 0.05 were considered significant and are indicated in bold.Fig. 5Contribution of variables to random forest model of tuberculosis sepsis prediction**. Random forest plot analysis of clinical variables and tuberculosis positivity is showing the mean decrease in accuracy (A) and Gini (B) in the accuracy of prediction of tuberculosis infection with each variable. ARV = antiretroviral.
Discussion
Unlike previous studies of sepsis etiology from Europe and North America where a causative sepsis pathogen is identified in only a minority of patients, in this study of PLWH in semi-urban settings of Tanzania and Uganda, we detected a plausible pathogen of sepsis in 69% of patients. Mtb was the most frequently detected pathogen of sepsis and accounted for 50% of bloodstream infections. S. pneumoniae, S. aureus, Klebsiella species*,* and E. coli were the most frequently isolated non-tuberculosis sepsis pathogens, and over 50% of the bacterial isolates tested were resistant to ceftriaxone. We also established that a greater number of ill-days before presentation, younger age, a greater number of days of cough, and low CD4+ T-cell concentration best indicated Mtb as a sepsis pathogen.
These findings are particularly concerning given that one in four critically ill patients in Africa has an infection, and infection and HIV are independently associated with increased mortality.21 The biologically plausible associations between clinical risk factors and tuberculosis were reassuring regarding the high prevalence of tuberculosis-sepsis identified in our study. Yet, none of the variables or the associated random forest model could confidently rule-in or rule-out tuberculosis sepsis, suggesting that tuberculosis sepsis cannot be predicted based on clinical variables alone in this critically ill population. Our findings help to inform the construction of a comprehensive empirical antimicrobial regimen for PLWH with sepsis in East Africa that may also be applicable to other tuberculosis-endemic settings.
While other observational studies have demonstrated that Mtb is the most common cause of sepsis in Africa,6^,^9^,^14^,^22 our study demonstrated a higher than previously reported prevalence of Mtb. This is likely related to our focus on a critically ill population, the rigorous testing for Mtb, which included mycobacterial blood culture and blood qPCR, in addition to conventional rapid diagnostics, and the high proportion of participants with a CD4+ T-cell concentration <200 cells/mm^3^ in whom LF-LAM is more sensitive and specific.23 Since our study was limited to East Africa, further studies in Africa and other TB-endemic regions are needed to determine if there are regional variations in sepsis etiology related to the proportion of adult PLWH.
WHO guidelines recommend initiating antituberculosis treatment to adult PLWH with critical illness when there is a high clinical suspicion for tuberculosis or a positive tuberculosis test including urine LF-LAM and sputum nuclear acid amplification test.24 However, our findings demonstrate that combined testing with sputum GeneXpert MTB/RIF and urine LF-LAM missed 32% of patients with Mtb bloodstream infection. Higher sensitivity LF-LAM designs and other novel rapid molecular diagnostics including those that test blood, may close this diagnostic gap. Limited autopsy studies of individuals with and without HIV in sub-Saharan Africa indicate that the prevalence of disseminated Mtb as a cause of death may be significantly higher than what can be detected during hospitalization.25 In sepsis treatment, effective antimicrobial therapy should start as soon as possible, as even hours of delay, which may be required for a tuberculosis test result to return, may lead to higher mortality.26, 27, 28 Our findings suggest that an immediate empirical antimicrobial regimen for sepsis in PLWH from tubercluosis-endemic regions should include antituberculosis treatment.
Empirical antimicrobial therapy in this population should additionally account for the high rate of predicted resistance to ceftriaxone among non-Mtb bacteria. The non-Mtb species distribution and resistance patterns found in this cohort were reflective of consistent trends in related populations across the continent, which show that Africa has some of the highest rates of antimicrobial resistance worldwide.29^,^30 Despite efforts to implement national action plans on antimicrobial resistance,31 many district hospitals in Africa, where PLWH with sepsis often seek care, do not routinely perform blood or urine cultures, or drug susceptibility testing. Instead, antibiotic selection is often influenced by cost and availability. In such a context, an empiric antimicrobial regimen for sepsis that includes an anti-pseudomonal fluoroquinolone would likely have activity against Pseudomonas infections, many Enterobacteriales that are resistant to ceftriaxone, and Mtb. Similarly, bacterial species such as methicillin resistant S. aureus and Enterococcus spp. could be targeted with linezolid which also treats Mtb. While specific combinations, companion drugs with ceftriaxone, routes of administration, doses, and duration would require comparative prospective study, our findings suggest that a regimen that targets Mtb and ceftriaxone-resistant bacteria would treat greater than 80% of all plausible pathogens of sepsis at our study hospitals.
Our study had several limitations. First, although we performed an extensive evaluation for TB, there is no “gold standard” for TB diagnosis in the critically ill given the low sensitivity of cultures and limited sensitivity and specificity of LF-LAM. Additionally, our bacterial blood culture positivity rates were low. This may be due to some participants being referred from rural clinics, where they may have received an antibacterial prior to transfer. We hypothesize this as a reason for the higher rate of bacterial bloodstream infection detected by qPCR compared to bacterial culture. Conversely, while we detected multiple urinary pathogens we cannot confirm they were causative organisms for sepsis. The study excluded those with positive serum CrAg at screening or by history prior to other comprehensive testing. CrAg positivity was low (4% of screened participants); however, given this exclusion criterion, we were unable determine the rate of cryptococcal co-infection with other putative pathogens of sepsis. Our study also did not include systematic drug susceptibility testing for each positive bacterial culture, which instead was only performed at the treating clinician's discretion. While there is a risk of overestimating ceftriaxone resistance if clinicians preferentially tested samples from patients that were not responding to standard treatments, our data are consistent with prior studies showing high rates of ceftriaxone-resistant Gram-negative bacteria regionally.32^,^33 Finally, we detected region-specific differences in Mtb sepsis and bacterial sepsis prevalence between Tanzania and Uganda, which highlights the need for more studies investigating region-specific sepsis etiology and resistance patters.
In conclusion, in a large cohort of PLWH with sepsis from representative referral hospitals in Tanzania and Uganda that reflect regionally common clinical settings and practice patterns, we conducted a comprehensive analysis of sepsis etiology. An enhanced spectrum antimicrobial therapy that targets Mtb and other ceftriaxone-resistant bacterial pathogens should be considered for empirical treatment of sepsis in PLWH in similar populations in East Africa and potentially other areas with high HIV and TB prevalence.
Contributors
E.O. and L.A. conceptualized the manuscript, reviewed, analyzed, and interpreted data, and wrote the manuscript. L.A. also supervised molecular testing at the Uganda study site, and E.O. performed literature search and review and visualized the data. The first co-authors contributed equally. M.N. and P.R. analyzed data, visualized data, and contributed to reviewing the manuscript. E.O. and M.N. had access to and verified the underlying study data. C.C.M., C.M., S.M., D.B., and S.H. designed the ATLAS trial, acquired funding, and served as co-investigators for the trial. They also reviewed the data and the manuscript draft. C.C.M. supervised the manuscript data collection, presentation, analysis, and interpretation. B.S., M.S., E.N., G.G., A.G., S.J., A.R., F.M., J.K., O.A., D.O., and D.M. recruited participants, collected and analyzed data, and edited the manuscript draft. J.L. contributed to supervising molecular testing, data analysis, and reviewing the manuscript. B.M. contributed to molecular testing and edited the manuscript. T.T. led LF-LAM testing during the ATLAS trial and reviewed and edited the data and manuscript.
Data sharing Statement
Metadata and standard operating procedures are available upon request to the corresponding author with publication and following approval of the proposal by the trial executive committee.
Declaration of interests
All authors declare no competing interests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nguyen H.B.Jaehne A.K.Jayaprakash N.Early goal-directed therapy in severe sepsis and septic shock: insights and comparisons to Pro CESS, Pro MI Se, and ARISE Crit Care 20120161602736462010.1186/s 13054-016-1288-3PMC 4929762 · doi ↗ · pubmed ↗
- 2Singer M.Deutschman C.S.Seymour C.W.The third international consensus definitions for sepsis and septic shock (Sepsis-3)JAMA 315820168018102690333810.1001/jama.2016.0287 PMC 4968574 · doi ↗ · pubmed ↗
- 3Rudd K.E.Johnson S.C.Agesa K.M.Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the Global Burden of Disease Study Lancet 3951021920202002113195446510.1016/S 0140-6736(19)32989-7PMC 6970225 · doi ↗ · pubmed ↗
- 4Rossi G.The FEAST trial of fluid bolus in African children with severe infection Lancet 3799816201261461510.1016/S 0140-6736(12)60263-322340296 · doi ↗ · pubmed ↗
- 5Andrews B.Muchemwa L.Kelly P.Lakhi S.Heimburger D.C.Bernard G.R.Simplified severe sepsis protocol: a randomised controlled trial of modified early goal-directed therapy in Zambia Crit Care Med 42112014231523242507275710.1097/CCM.0000000000000541 PMC 4199893 · doi ↗ · pubmed ↗
- 6Lewis J.M.Feasey N.A.Rylance J.Aetiology and outcomes of sepsis in adults in Sub-Saharan Africa: a systematic review and meta-analysis Crit Care 23120192123118606210.1186/s 13054-019-2501-y PMC 6558702 · doi ↗ · pubmed ↗
- 7Pyarali F.F.Iordanov R.Palacio A.Tamariz L.Excess mortality risk from sepsis in patients with HIV—a meta-analysis J Crit Care 5920201011073259030210.1016/j.jcrc.2020.05.018 · doi ↗ · pubmed ↗
- 8Byashalira K.Mbelele P.Semvua H.Clinical outcomes of new algorithm for diagnosis and treatment of Tuberculosis sepsis in HIV patients Int J Mycobacteriol 8420193133193179349910.4103/ijmy.ijmy_135_19 · doi ↗ · pubmed ↗