Association Between Stress Management Interventions and Symptom Severity in Adults With Irritable Bowel Syndrome (IBS) in Saudi Arabia
Randa M Alharazi, Intessar Sultan, Gharam A Alahmadi, Renad Ghandour, Mohamad B Dahha, Yousef T Rajikhan, Emad Al Takroni, Layan Alahmadi, Shatha Almahwzi, Salman alhrbi

TL;DR
This study shows that stress management techniques like deep breathing and meditation reduce IBS symptoms and stress in Saudi adults.
Contribution
The study provides new evidence on the effectiveness of stress management in reducing IBS symptoms in Saudi Arabia.
Findings
Stress management users had significantly lower symptom severity scores for abdominal pain and distension.
Participants using stress management reported lower perceived stress and better daily functioning.
Gender and lifestyle were significantly linked to IBS symptom burden.
Abstract
Background: Psychological stress is a major contributing factor to irritable bowel syndrome (IBS), a widespread functional gastrointestinal disorder. Consequently, understanding the relationship between stress management strategies and the severity of IBS symptoms is crucial. Aim: This study sought to assess the association between stress management interventions and symptom severity among adults with IBS in Saudi Arabia. Furthermore, it investigated the associations between IBS, demographic data, lifestyle habits, and perceived stress levels. Methodology: We conducted a cross-sectional study involving adults aged 18 and older in Saudi Arabia who had a clinical diagnosis of IBS. Participants completed a validated, bilingual web-based survey that incorporated the Rome IV diagnostic criteria, the IBS Symptom Severity Scale (IBS-SSS), and the Perceived Stress Scale (PSS). Statistical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
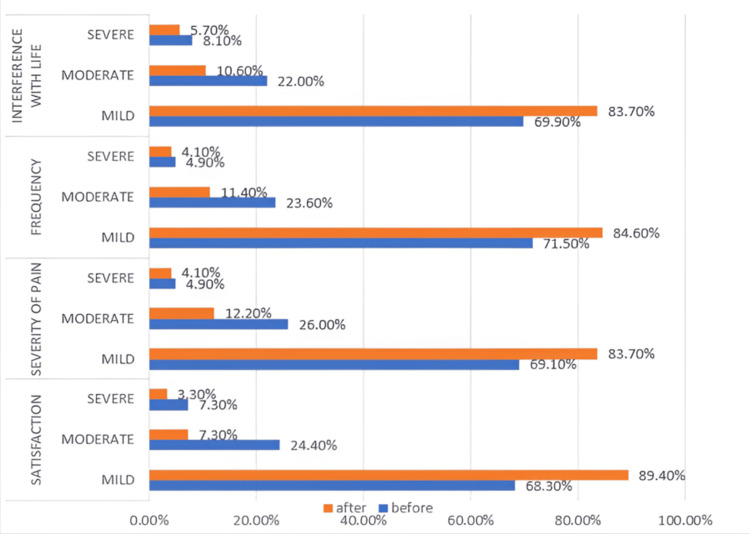 Figure 1
Figure 1| Characteristics | Participants (N = 517; 100%) | No stress management (n = 393; 76%) | Received stress management (n = 124; 24%) | p-value | ||||
| Number | Percentage | Number | Percentage | Number | Percentage | |||
| Gender | Female | 326 | 63.1 | 280 | 71.1 | 46 | 37.4 | <0.001* |
| Male | 191 | 36.9 | 114 | 28.9 | 77 | 62.6 | ||
| Age, years (median, IQR) | 26 (13) | 27.0 (17) | 23.0 (9) | 0.005* | ||||
| Education | Post-graduate studies | 32 | 6.2 | 20 | 5.1 | 12 | 9.8 | 0.124 |
| Bachelor's degree | 323 | 62.5 | 246 | 62.4 | 77 | 62.6 | ||
| High school | 135 | 26.1 | 104 | 26.4 | 31 | 25.2 | ||
| < High school | 27 | 5.2 | 24 | 6.1 | 3 | 2.4 | ||
| Occupation | Employed | 206 | 39.8 | 151 | 38.3 | 55 | 44.7 | 0.136 |
| Student | 189 | 36.6 | 142 | 36.0 | 47 | 38.2 | ||
| Unemployed | 122 | 23.6 | 101 | 25.6 | 21 | 17.1 | ||
| Duration of IBS | <1 year | 229 | 44.3 | 120 | 30.5 | 42 | 34.1 | 0.292 |
| 1-3 years | 162 | 31.3 | 182 | 46.2 | 47 | 38.2 | ||
| >3 years | 126 | 24.4 | 92 | 23.4 | 34 | 27.6 | ||
| Dietary habits | Healthy | 50 | 9.7 | 32 | 8.1 | 18 | 14.6 | 0.004* |
| Moderately healthy | 331 | 64.0 | 246 | 62.4 | 85 | 69.1 | ||
| Unhealthy | 136 | 26.3 | 116 | 29.4 | 20 | 16.3 | ||
| Exercise | Daily | 51 | 9.9 | 33 | 8.4 | 18 | 14.6 | <0.001* |
| Several times a week | 132 | 25.5 | 90 | 22.8 | 42 | 34.1 | ||
| Once a week | 134 | 25.9 | 97 | 24.6 | 37 | 30.1 | ||
| Rarely | 157 | 30.4 | 133 | 33.8 | 24 | 19.5 | ||
| No | 43 | 8.3 | 41 | 10.4 | 2 | 1.6 | ||
| Smoking | No | 448 | 86.7 | 343 | 87.1 | 105 | 85.4 | 0.630 |
| Yes | 69 | 13.3 | 51 | 12.9 | 18 | 14.6% | ||
| Perceived stress | Low stress | 20 | 3.9 | 15 | 3.8 | 5 | 4.1 | 0.007* |
| Moderate stress | 440 | 85.1 | 326 | 82.7 | 114 | 92.7 | ||
| High stress | 57 | 11.0% | 53 | 13.5 | 4 | 3.3 | ||
| Stress management variables | Participants (n = 124) | Percentage | |
| Types of stress management | Deep breathing | 83 | 66.9 |
| Meditation | 63 | 50.8 | |
| Yoga | 38 | 30.6 | |
| Cognitive behavioral therapy | 29 | 23.4 | |
| Number of stress management types | 1 | 66 | 53.7 |
| 2 | 34 | 27.6 | |
| 3 | 13 | 10.6 | |
| 4 | 10 | 8.1 | |
| Frequency of stress management sessions | Rarely | 24 | 19.5 |
| Once a week | 36 | 29.3 | |
| Several times a week | 43 | 35.0 | |
| Daily | 20 | 16.3 | |
| IBS symptoms | Stress management | p-value | ||||
| Without stress management | With stress management | |||||
| n | % | n | % | |||
| Abdominal pain | No | 73 | 18.5 | 20 | 16.3 | 0.119 |
| Rarely | 126 | 32.0 | 40 | 32.5 | ||
| Sometimes | 104 | 26.4 | 45 | 36.6 | ||
| Often | 62 | 15.7 | 14 | 11.4 | ||
| Very often | 29 | 7.4 | 4 | 3.3 | ||
| Distension | No | 78 | 19.8 | 21 | 17.1 | 0.028* |
| Rarely | 129 | 32.7 | 40 | 32.5 | ||
| Sometimes | 97 | 24.6 | 44 | 35.8 | ||
| Often | 58 | 14.7 | 16 | 13.0 | ||
| Very often | 32 | 8.1 | 2 | 1.6 | ||
| Change in bowel habits | No | 92 | 23.4 | 30 | 24.4 | 0.004* |
| Rarely | 125 | 31.7 | 42 | 34.1 | ||
| Sometimes | 98 | 24.9 | 42 | 34.1 | ||
| Often | 43 | 10.9 | 9 | 7.3 | ||
| Very often | 36 | 9.1 | 0 | 0.0 | ||
| Severity of pain | Mild | 244 | 61.9 | 88 | 71.5 | <0.001* |
| Moderate | 90 | 22.8 | 31 | 25.2 | ||
| Severe | 60 | 15.2 | 4 | 3.3 | ||
| Frequency | Mild | 248 | 62.9 | 88 | 71.5 | 0.001* |
| Moderate | 94 | 23.9 | 29 | 23.6 | ||
| Severe | 52 | 13.2 | 6 | 4.9 | ||
| Distension severity | Mild | 243 | 61.7 | 85 | 69.1 | 0.001* |
| Moderate | 100 | 25.4 | 32 | 26.0 | ||
| Severe | 51 | 12.9 | 6 | 4.9 | ||
| Satisfaction with bowel habits | Mild | 251 | 63.7 | 84 | 68.3 | 0.060 |
| Moderate | 96 | 24.4 | 30 | 24.4 | ||
| Severe | 47 | 11.9 | 9 | 7.3 | ||
| Interference with life | Mild | 235 | 59.6 | 86 | 69.9 | <0.001* |
| Moderate | 91 | 23.1 | 27 | 22.0 | ||
| Severe | 68 | 17.3 | 10 | 8.1 | ||
| Perceived stress | Low | 15 | 3.8 | 5 | 4.1 | 0.007* |
| Moderate | 326 | 82.7 | 114 | 92.7 | ||
| High | 53 | 13.5 | 4 | 3.3 | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal motility and disorders · Music Therapy and Health · Inflammatory Bowel Disease
Introduction
The status of one's gastrointestinal system is pivotal to overall well-being, influencing both physical and mental health. A functioning digestive tract is required for the absorption of nutrients essential for cellular repair, energy, and growth. However, common disorders such as constipation, bloating, and irritable bowel syndrome (IBS) often disrupt daily functioning, causing anxiety, discomfort, and a diminished quality of life [1].
IBS is defined clinically by chronic abdominal pain and irregular bowel habits, affecting a large demographic. Typical presentations include bloating and constipation, which can further aggravate emotional distress [2]. For patients with IBS, regulating stress is critical for improving both physical and mental health outcomes. Stress triggers the gut-brain axis, resulting in symptoms such as altered bowel motility and abdominal pain. Furthermore, stress-induced hormonal fluctuations can heighten gut sensitivity, thereby complicating the clinical picture [3].
Adopting stress management strategies offers substantial advantages for individuals with IBS, including symptom alleviation, enhanced coping mechanisms, and improved quality of life. Effectively addressing stress allows individuals to better manage gastrointestinal issues. Globally, the importance of stress management in healthcare is increasingly recognized. Many nations are adopting mental wellness programs, integrating techniques like mindfulness and yoga into medical care. Consequently, organizations are developing wellness initiatives to help personnel manage stress, which ultimately boosts productivity and general health [4].
In the context of Saudi Arabia, stress management is particularly relevant due to specific cultural and lifestyle dynamics. Rapid modernization has introduced new stressors impacting public health. However, traditional practices, such as prayer and meditation, can be effectively incorporated into stress reduction strategies. Additionally, social support through family and community ties remains essential. Given the pressures of education and employment, effective stress management is vital for improving life quality in this region [5].
This study aimed to evaluate the effect of stress management interventions on symptom severity in adults with IBS in Saudi Arabia. It further examined the relationship between stress levels and IBS symptoms, explored the influence of lifestyle and dietary factors, and assessed changes in symptom severity before and after intervention.
Materials and methods
Study design
We utilized a cross-sectional, questionnaire-based design. A self-administered online survey was designed to evaluate the relationship between stress management interventions and symptom severity among adults diagnosed with IBS in Saudi Arabia.
Sampling and population
A non-probability convenience sampling approach was employed to recruit participants from the general public. The survey link was disseminated electronically via major social media platforms to ensure a broad reach. The cohort comprised male and female residents of Saudi Arabia, aged 18 years and older, with a clinical diagnosis of IBS. The sample represented diverse demographic characteristics, dietary patterns, and gastrointestinal symptom profiles.
Data collection
Following a comprehensive literature review and expert consultation, a structured bilingual questionnaire (Arabic and English) was created using Google Forms (Google, Mountain View, CA, USA). The instrument comprised the following sections: (1) informed consent form; (2) demographic information; (3) lifestyle and dietary habits; (4) Rome IV diagnostic criteria for IBS [6]; (5) IBS Symptom Severity Scale (IBS-SSS) [7] (permission to use this scale was obtained from the copyright holder via the Copyright Clearance Center); (6) Perceived Stress Scale (PSS) [8] (permission for its use was obtained in accordance with the author’s requirements); and (7) details of stress management interventions.
For the purpose of this study, a "healthy diet" was defined as the self-reported regular consumption of nutrient-dense foods (such as fruits, vegetables, and whole grains) and the limitation of processed foods, consistent with general dietary guidelines.
Instrument validation and reliability
Subject matter experts validated the questionnaire content. A pilot study involving 10% of the calculated sample size was conducted to ensure comprehension, clarity, and feasibility. Cronbach’s alpha was utilized to evaluate internal consistency and reliability.
Sample size calculation
The sample size was calculated using the Cochran formula (n = z^2^pq/d^2^) based on an estimated IBS prevalence of 17% in Saudi Arabia, a 95% confidence level, and a 5% margin of error. This calculation indicated a minimum required sample size of 217 participants, which was exceeded by our final sample of 517.
Ethical considerations
The study adhered to ethical standards and guidelines. Ethical approval was obtained from the Institutional Research Review Board (IRRB) of Ibn Sina National College for Medical Studies (No: IRRB-01-07092025). Participation was voluntary, with informed consent obtained electronically. No personal identifiers were collected, and data were stored anonymously and securely for research purposes.
Statistical analysis
Data was coded, cleaned, and analyzed using IBM SPSS Statistics for Windows, Version 23.0 (Released 2015; IBM Corp., Armonk, NY, USA). Descriptive statistics summarized variables, with categorical data presented as frequencies and percentages, and continuous variables as means ± standard deviations (SD). To examine associations between stress management and IBS symptom severity, chi-square or Fisher’s exact tests were used for categorical variables, independent t-tests or ANOVA were used for continuous variables, and a p-value < 0.05 was considered statistically significant.
Results
Demographic and lifestyle factors
A total of 517 adults diagnosed with IBS were included, of whom 124 (24%) practiced stress management. The cohort was predominantly female (63.1%); however, the proportion of females was significantly higher in the non-stress management group compared to the stress management group (71.1% vs. 37.4%, respectively; p < 0.001). The median age was significantly lower in the stress management group (23 years, IQR 9) compared to the non-management group (27 years, IQR 17; p = 0.005). Education level, occupation, and duration of IBS did not differ significantly between the groups. Participants practicing stress management showed significantly higher engagement in healthy dietary and exercise habits compared to non-practitioners (p = 0.004 and p < 0.001, respectively). Smoking status did not differ significantly (p = 0.630). Notably, perceived stress was significantly lower in the stress management group, with fewer participants reporting high stress levels (3.3%) compared to the non-management group (13.5%; p = 0.007) (Table 1).
*Table 1: Characteristics of IBS patients who received and did not receive stress management Data are presented as numbers and percentages. p-values were calculated using the Pearson chi-square test (χ2). Significant associations were found for gender (χ2 = 30.01, df = 1), dietary habits (χ2 = 10.99, df = 2), exercise (χ2 = 23.36, df = 4), and perceived stress (χ2 = 9.87, df = 2).Statistically significant difference (p < 0.05).
Characteristics of Stress Management
Among the 124 participants utilizing stress management, the most common methods were deep breathing (66.9%) and meditation (50.8%), followed by yoga (30.6%) and cognitive behavioral therapy (23.4%). Over half of the participants (53.7%) used a single method, while 8.1% combined all four methods. Practice frequency varied, with "several sessions a week" being the most common (35.0%), followed by once a week (29.3%), rarely (19.5%), and daily sessions (16.3%) (Table 2).
Comparison of IBS symptoms before and after stress management
Significant improvements were noted after adopting stress management. The frequency of abdominal pain declined, with 84.6% reporting mild pain post-intervention compared to 71.5% beforehand (p = 0.010). Abdominal distention improved, with 83.7% reporting mild distention compared to 69.1% previously (p < 0.002). Satisfaction with bowel habits rose significantly, with 89.4% reporting mild dissatisfaction post-intervention compared to 68.3% before (p < 0.001). Interference with daily life also decreased, with 83.7% reporting mild impact compared to 69.9% before (p = 0.007). While the severity of abdominal pain decreased (81.3% mild severity post-intervention vs. 71.5% before), this change was not statistically significant (p = 0.141) (Figure 1).
Significant differences in IBS symptom severity before and after stress management
Comparison of IBS symptoms between participants with and without stress management
Compared to non-practitioners, those who practiced stress management reported significantly less severe abdominal pain (3.3% vs. 15.2%; p < 0.001), less frequent abdominal pain (4.9% vs. 13.2%; p = 0.001), milder abdominal distention (69.1% vs. 61.7%; p = 0.001), less interference with daily life (69.9% vs. 59.6%; p < 0.001), and lower perceived stress (3.3% vs. 13.5%; p = 0.007). No significant difference was observed regarding satisfaction with bowel habits (p = 0.060) (Table 3).
*Table 3: Comparison between IBS participants who received and who did not receive stress managementData are presented as numbers and percentages. p-values were calculated using the Pearson chi-square test (χ2). Significant differences were observed for abdominal distension frequency (χ2 = 10.87, df = 4), change in bowel habits (χ2 = 15.34, df = 4), pain severity (χ2 = 15.22, df = 2), pain frequency (χ2 = 14.28, df = 2), distension severity (χ2 = 13.91, df = 2), interference with life (χ2 = 20.35, df = 2), and perceived stress (χ2 = 9.87, df = 2).Statistically significant difference (p < 0.05).
Discussion
This research sought to assess the value of stress management in alleviating IBS symptoms among adults in Saudi Arabia. Regarding demographics, our data indicates a female predominance among IBS patients, a finding consistent with existing literature [9,10]. Conversely, stress management techniques were utilized most frequently by younger individuals and males.
Significant differences in lifestyle behaviors were noted between those who practiced stress management and those who did not. The stress management group was more inclined toward regular physical activity and healthier dietary habits. These behaviors are known to modulate IBS symptoms and may work synergistically with stress reduction to enhance outcomes. Consistent with the systematic review by Sirri et al., our results showed no significant correlation between smoking status and the severity of IBS symptoms [11].
Analysis of perceived stress revealed a distinct pattern: while moderate stress was common across the board, high stress levels were significantly more prevalent in the non-intervention group. This corroborates prior research identifying perceived stress as a core component of IBS pathophysiology, where elevated stress exacerbates visceral hypersensitivity and disrupts gut-brain signaling [12,13]. Our data support previous assertions that high stress predicts poorer IBS prognoses [14].
Interventions such as cognitive behavioral therapy (CBT), mindfulness, and relaxation training have been proven to lower perceived stress and mitigate IBS severity [15,16]. This underscores the dual role of stress management in providing symptom relief and reducing the psychological burden of the disorder.
Furthermore, participants engaging in stress management reported significant reductions in abdominal distension, pain frequency, and interference with daily life, alongside higher satisfaction with bowel habits. Yoga, meditation, and deep breathing were the primary methods used, typically practiced several times weekly. These results align with previous studies linking CBT and mindfulness-based interventions to improved health-related quality of life and reduced symptom severity [16-18]. Consequently, stress reduction should be prioritized as a non-pharmacological strategy in IBS care, especially for patients with psychological symptoms or in resource-constrained environments.
Strengths and limitations
This study's strengths include a relatively large sample size and its focus on the Saudi Arabian population, an underrepresented demographic in IBS research. However, limitations exist. The cross-sectional design restricts causal inference. Reliance on self-reported measures may introduce recall and social desirability biases. Additionally, the assessment of stress management was limited to binary values without accounting for the quality, duration, or specific type of intervention.
Conclusions
This study examined the association between stress management interventions and symptom severity among adults with IBS in Saudi Arabia. Significant associations were found between gender, lifestyle factors, perceived stress, and IBS symptom burden. Stress management practices were common, with deep breathing, meditation, and yoga being the most frequently used. Symptom severity, including abdominal pain, distention, bowel habit dissatisfaction, and interference with daily life, was significantly lower among participants practicing stress management. Moreover, participants who utilized stress management reported lower rates of severe symptoms compared to those who did not. These findings highlight the importance of integrating stress reduction strategies into the holistic management of IBS.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Irritable bowel syndrome Am J Nurs Weaver KR Melkus GD Henderson WA 4855117201710.1097/01.NAJ.0000520253.57459.01PMC 545330528541989 · doi ↗ · pubmed ↗
- 2Probiotics and prebiotics in intestinal health and disease: from biology to the clinic Nat Rev Gastroenterol Hepatol Sanders ME Merenstein DJ Reid G Gibson GR Rastall RA 6056161620193129696910.1038/s 41575-019-0173-3 · doi ↗ · pubmed ↗
- 3Effects of different coping strategies on physical and mental health of patients with irritable bowel syndrome Clin Gastroenterol Hepatol Dindo L Lackner J 150015031520172839243910.1016/j.cgh.2017.03.041 · doi ↗ · pubmed ↗
- 4Systematic review with meta-analysis: stress-management interventions for patients with irritable bowel syndrome Stress Health Horn A Stangl S Parisi S 6947073920233664916610.1002/smi.3226 · doi ↗ · pubmed ↗
- 5Prevalence, risk factors, and management of irritable bowel syndrome in Saudi Arabia: a systematic review Cureus Makkawy EA Abdulaal IE Kalaji FR Makkawi M Alsindi N 015202310.7759/cureus.47440 PMC 1065881938021554 · doi ↗ · pubmed ↗
- 6Rome IV Criteria 8 2025 2006642325<-block 2016 https://theromefoundation.org/rome-iv/rome-iv-criteria/
- 7The irritable bowel severity scoring system: a simple method of monitoring irritable bowel syndrome and its progress Aliment Pharmacol Ther Francis CY Morris J Whorwell PJ 395402111997914678110.1046/j.1365-2036.1997.142318000.x · doi ↗ · pubmed ↗
- 8A global measure of perceived stress J Health Soc Behav Cohen S Kamarck T Mermelstein R 3853962419836668417 · pubmed ↗