Mapping the Mind: A Network Meta-Analysis of Mindfulness and Traditional and Digital Interventions for Cognitive and Behavioral Enhancement in Children With Attention-Deficit/Hyperactivity Disorder (ADHD)
Hosam Hadi Hassan Awaji, Rawan A Alharbi, Manal B Mokli, Ghadh M Balawi, Yahya S ALzahrani, Alaa R Khan, Tebra A Bima, Maha G Atwie, Amal O Alatwai, Sarah A Alatawi, Rawan M Albalawi

TL;DR
This study compares non-drug treatments for ADHD in children, finding that mindfulness and parent training are most effective.
Contribution
The study provides a network meta-analysis comparing various non-pharmacological ADHD interventions for children.
Findings
Family-based mindfulness therapy was most effective for reducing inattention and hyperactivity symptoms.
Behavioral parent training significantly reduced parental stress.
Mindfulness-based interventions consistently ranked highest in effectiveness compared to control groups.
Abstract
Pharmacological and behavioral interventions are commonly used to manage attention-deficit/hyperactivity disorder (ADHD). This disorder is highly prevalent among children and adolescents. New non-pharmacological approaches, including mindfulness-based therapies (MBT), neurofeedback, and working memory training (WMT), may represent potential alternatives. This network meta-analysis aims to assess the comparative effectiveness of various nonpharmacological interventions for pediatric ADHD. Electronic databases were searched to identify clinical trials that compared different treatments in ADHD to each other, usual care, or waiting list from inception to March 22, 2025. Sixteen studies representing 806 participants were included in this study. The network compared several intervention types: MBT, neurofeedback, cognitive-behavioral therapy (CBT), WMT, and behavioral parent training (BPT)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
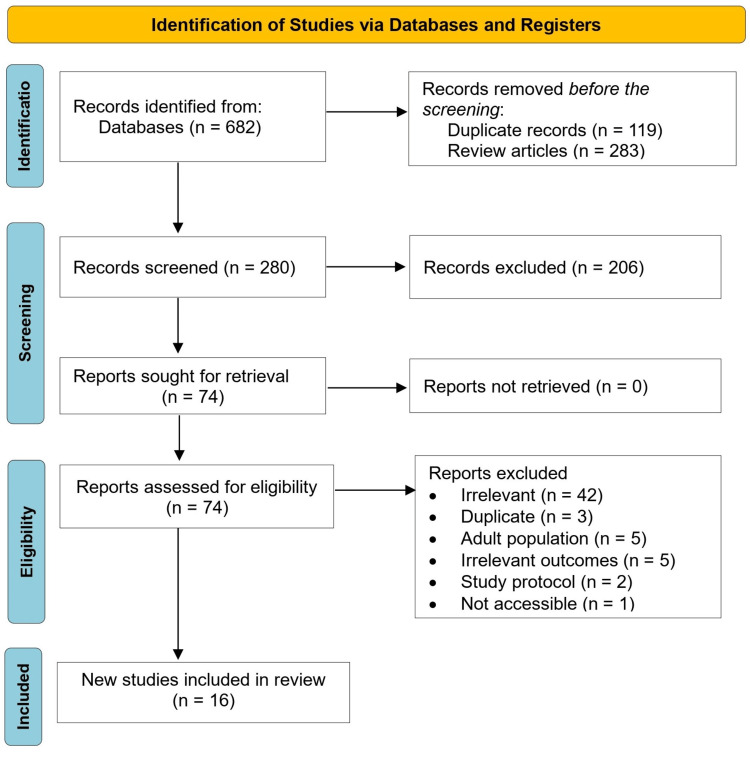 Figure 1
Figure 1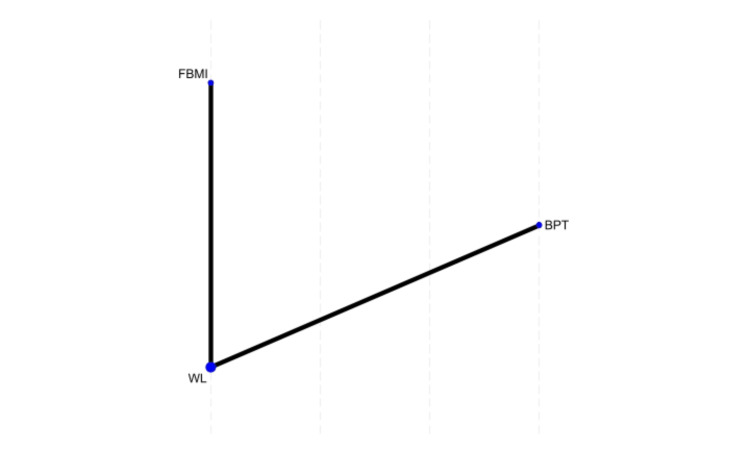 Figure 2
Figure 2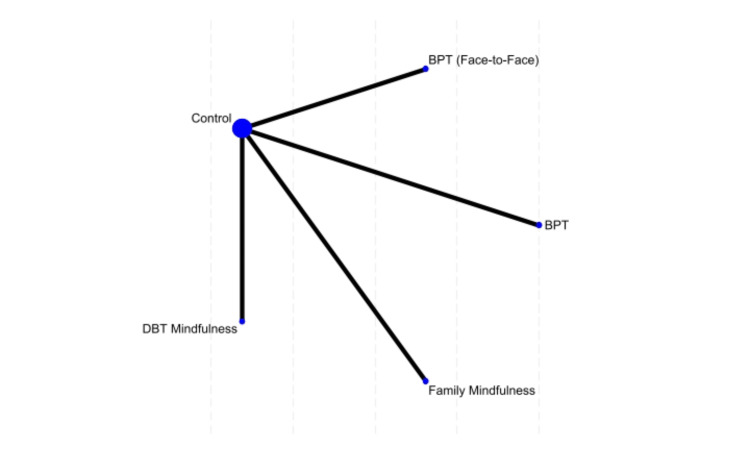 Figure 3
Figure 3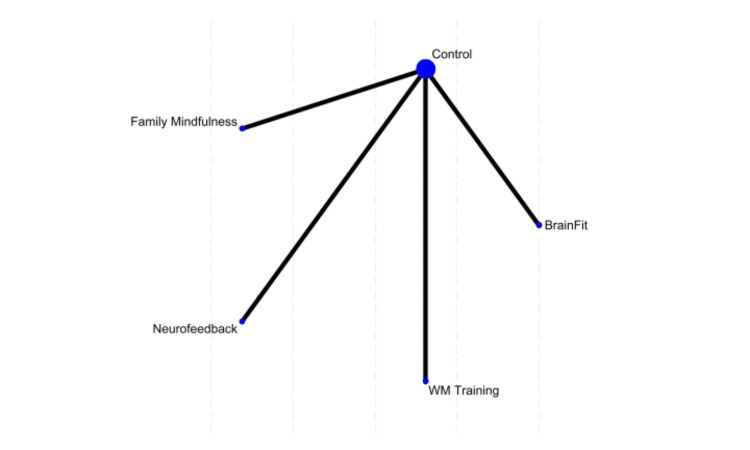 Figure 4
Figure 4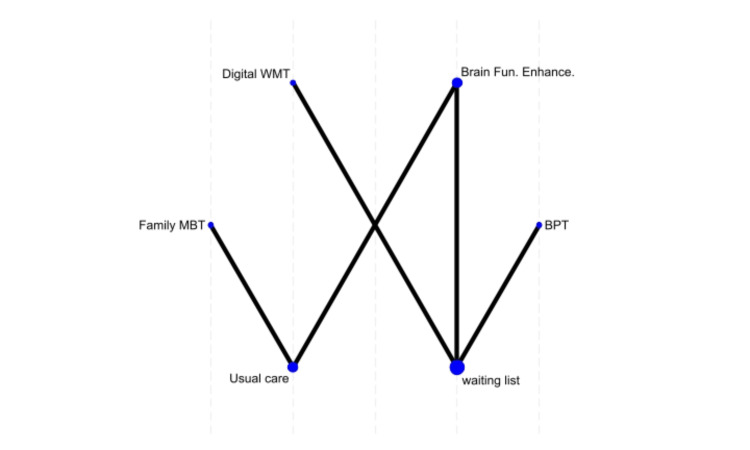 Figure 5
Figure 5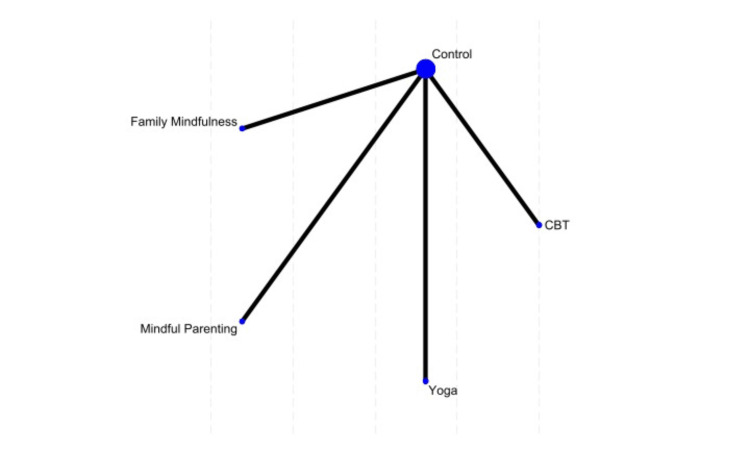 Figure 6
Figure 6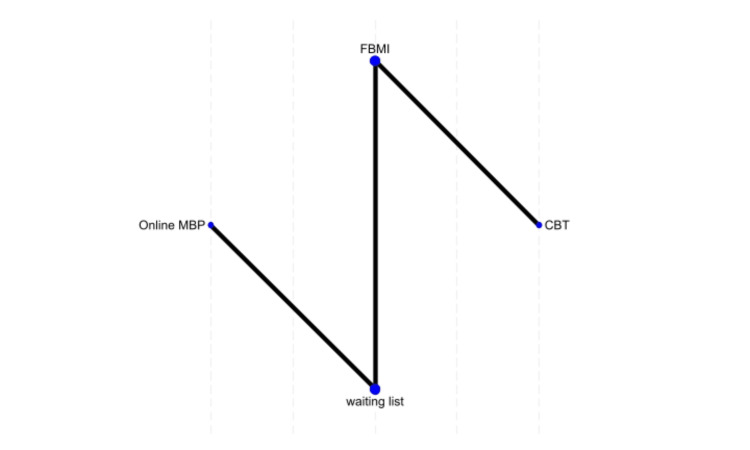 Figure 7
Figure 7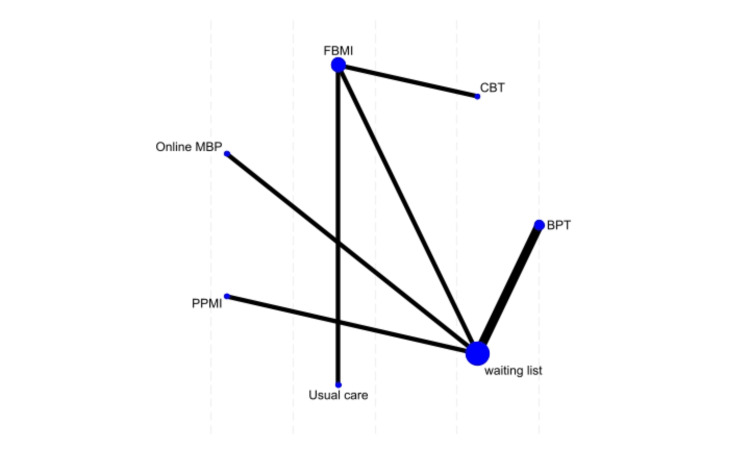 Figure 8
Figure 8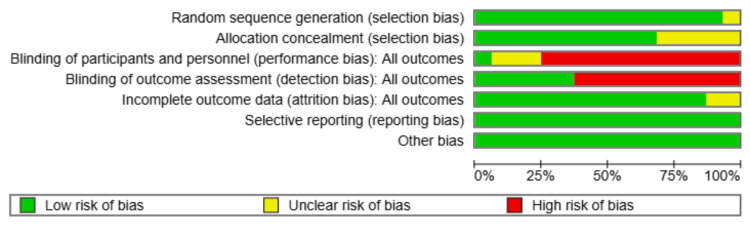 Figure 9
Figure 9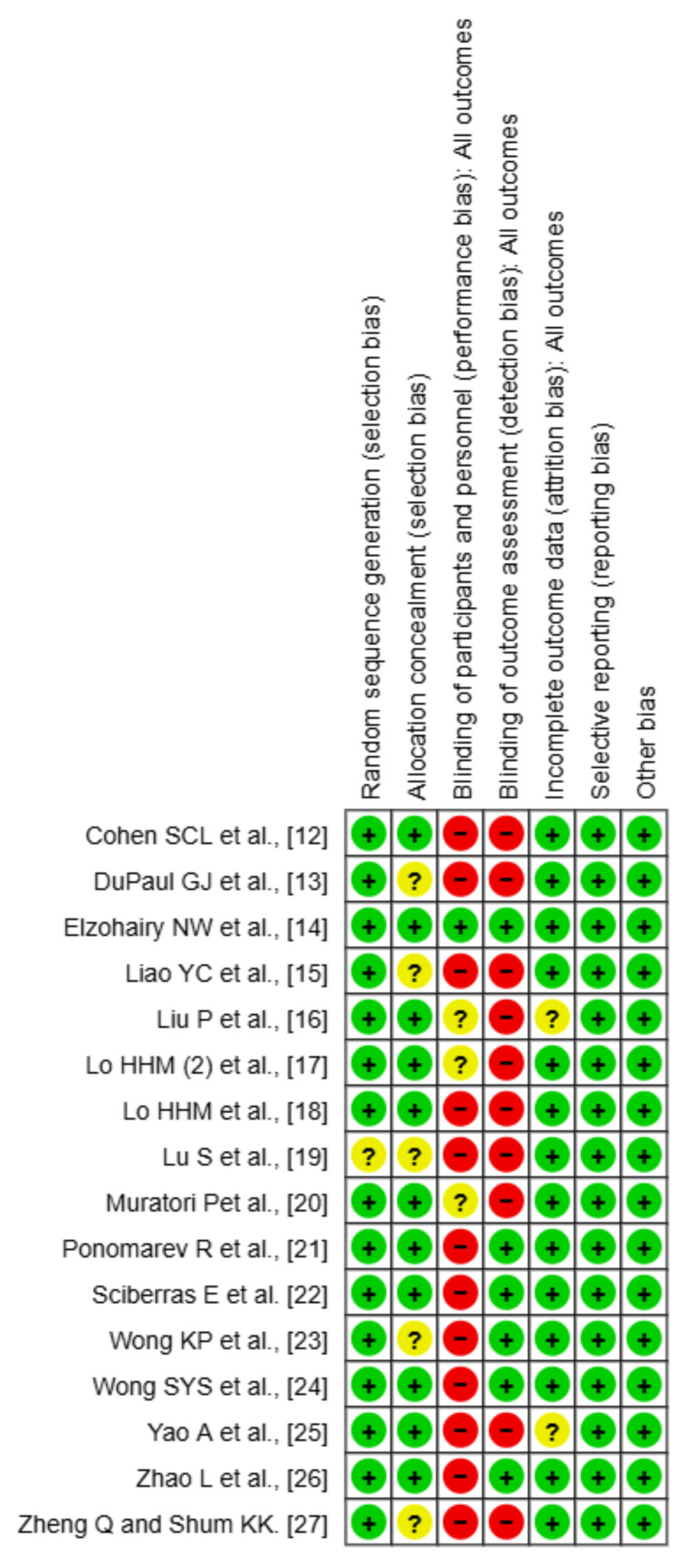 Figure 10
Figure 10| Author | Year | Country | Design | Population | Sample Size (No. of total interventions/controls) | Age (Mean ± SD) | Sex | ADHD Type | Intervention | Control | Duration | Measured outcomes |
| Cohen SCL et al. [ | 2018 | USA (University of California, Davis) | RCT | Preschool-aged children (3-5 years) with ADHD symptoms | 23 total (12 intervention / 11 control) | Group 1: 52 ± 7 months, Group 2: 46 ± 10 months | 15 male (65.2%), 8 female (34.8%) | ADHD symptoms (not formally diagnosed) | 6-week yoga intervention (home & school-based) | waiting list | 6 weeks | ADHD symptoms (ADHD-RS-IV Preschool), Behavior (SDQ), Attention (KiTAP), Heart rate variability (HRV) |
| DuPaul GJ et al. [ | 2018 | USA | RCT | Preschool children (ages 3-5 years, Mean = 4.43) | N = 47 (F2F: 16, Online: 15, Waitlist Control (WLC): 16) | (ages 3-5 years, Mean = 4.43) | 30 male (63.8%), 17 female (36.2%) | Combined (61.7%), Inattentive (4.3%), Hyperactive-Impulsive (34%) | Behavioral Parent Training (BPT), either face-to-face (F2F) or online | waiting list | 10 weeks | ADHD Symptom Severity (Conners Scales, Vanderbilt ADHD Diagnostic Parent Rating Scale), Parenting Stress (PSI-SF), Treatment Fidelity, Emotional Regulation, Child Behavior (Conners Global Index, Mood/Affect), Executive Function (Go/No-Go, BRIEF), Parenting Efficacy (Parenting Scale) |
| Elzohairy NW et al. [ | 2024 | Egypt | RCT | Children with ADHD | 50 (26/24) | 8.98 ± 0.76 | 24 male (48%), 26 female (52%) | Mixed (Inattentive & Hyperactive-Impulsive) | Mindfulness-Based Training (MBT) | Usual care | 12 weeks | ADHD Symptoms (Vanderbilt ADHD Diagnostic Parent Rating Scale - VADPRS): Inattention, Impulsivity/ Emotion Regulation Questionnaire (ERC), Emotion Lability/Negativity, Emotion Regulation Score, Total Emotion Regulation Score |
| Liao YC et al. [ | 2022 | Taiwan | RCT | Children with ADHD | Total = 50 (Intervention = 25, Control = 25) | Experimental: 9.82 ± 1.32, Control: 10.07 ± 2.12 | Experimental: 22 male (88%), 3 female (12%); Control: 19 male (76%), 6 female (24%) | NM | Neurofeedback-based neuropsychotherapy + computerized training (20 hours) | Usual care | 10 weeks | ADHD Symptoms (SNAP-IV) - Parent report, Inattention Symptoms (SNAP-IV) - Parent report, Hyperactivity/Impulsivity Symptoms (SNAP-IV) - Parent report, Daily Attention Function, Daily Executive Function, Daily Time Management, EEG Theta/Beta Ratio (TBR), Comprehensive Nonverbal Attention Test (CNAT) - Focus, Search, Inhibition, Distract subtests, Tower of London (ToL) - Planning ability, Wisconsin Card Sorting Test (WCST) - Cognitive flexibility, perseverative errors, Math Achievement Test, Mandarin Literacy Test |
| Liu P et al. [ | 2021 | China | RCT | Parents of children diagnosed with ADHD | 113 total (58 intervention / 55 control) | Parents: MPP group = 40.81 ± 4.62; TAU group = 38.71 ± 4.54 | Parents:10 male (8.8%), 103 female (91.2%) | ADHD-I (66%), ADHD-HI (34%), ADHD-C (31%) | Mindful Parenting Program (MPP) | usual care | 8 weeks | parental stress, mindfulness, self-compassion, children's ADHD symptoms (ADHD-RS-IV) |
| Lo HHM (2) et al. [ | 2020 | Hong Kong, China | RCT | Young children (5-7 years) with ADHD symptoms and their parents | 100 total (50 intervention / 50 control) | Children: 6.25 years ± 0.87 | 83 male (83%), 17 female (17%) | ADHD symptoms | Family-Based Mindfulness Intervention (FBMI) | waiting list | 6 weeks | ADHD symptoms (SWAN), Behavior (CBCL), Attention (ANT), Parental stress (PSI), Parent well-being (WHO-5), Parent ADHD symptoms (ASRS) |
| Lo HHM et al. [ | 2024 | Hong Kong, China | RCT | Parents of children with ADHD | 43 parents (23 intervention, 20 control) | Parents: 42.26 ± 5.27 years; Children: 10.80 ± 3.33 years (intervention), 9.53 ± 2.98 years (control) | The majority were mothers: 3 male (7.0%), 40 female (93.0%) | ADHD children with and without comorbidities | Online Mindfulness-Based Program (MBP) for parents | Waitlist control (received the program after 3 months) | 4 weeks (28 days) | ADHD symptomology (SWAN, SNAP-IV), Emotional regulation (HADS-A, CES-D), Parenting stress (PSI-SF), Behavioral checklists (CBCL, CGI-I, etc.) |
| Lu S et al. [ | 2022 | China (Shenzhen) | Quasi-experimental feasibility study (non-randomized) | Low-income migrant families (parent–child dyads) | 21 families (11 intervention, 10 control) | Children: 9.29 ± 1.96 years, Parents: 35.19 ± 4.03 years | 12 male children (57.1%), 9 female children (42.9%) | NM | Parallel Parent-Child Mindfulness Intervention (PPMI) | waiting list | 8 weeks (weekly sessions, mindfulness exercises at home) | Parenting Stress: Parenting Stress Index Short Form (PSI-SF), Mindful Parenting: Interpersonal Mindfulness in Parenting (IMP) Scale, Child Mindfulness: Child and Adolescent, Mindfulness Measure (CAMM), Child Behavioral Problems: Strengths and Difficulties Questionnaire (SDQ), Parent–Child Relationship: Inventory of Parent and Peer Attachment (IPPA) |
| Muratori P et al. [ | 2021 | Italy | RCT | Boys with ADHD and Oppositional Defiant Disorder (ODD) | 50 total (25 intervention / 25 control) | Experimental: 8.75 ± 0.71, Control: 9.05 ± 1.05 | 50 male (100%) | ADHD with ODD comorbidity | Mindfulness-based intervention for children and parents | waiting list | 8 weeks | ADHD symptoms, Aggression (MOAS), Hyperactivity (SDQ), Sustained attention (Bells Test), Impulsivity (MF-20), Mindfulness (CAMM), Psychological inflexibility (AFQ-Y) |
| Ponomarev R et al. [ | 2023 | Kazakhstan & Russia | RCT | Children with ADHD (8–10 years old) | 90 (45 intervention, 45 control) | 8.73 ± 0.85 years | 61 male (67.8%), 29 female (32.2%) | Mixed types (Inattentive, Hyperactive-Impulsive, Combined) | Digital Cognitive Mindfulness Training (DBT-based Mindfulness Program) | Waitlist Control | 4 weeks (4 sessions, 1 hour per week) | ADHD symptoms: Conners-3 (Inattention, Hyperactivity, Learning Problems, Executive Functioning, Aggression, Peer Relations), Executive Function: WISC-IV (Working Memory Index), NEPSY-II (Inhibition, Switching Tasks) |
| Sciberras E et al. [ | 2018 | Australia | RCT | Children with ADHD and comorbid anxiety | N = 12 (Intervention = 6, Control = 6) | Intervention: 10.4 ± 1.3 years, Control: 11.6 ± 0.6 years | Intervention: 5 male (83.3%), 1 female (16.7%); Control: 6 male (100%), 0 female (0%) | Combined: 3 (Intervention), 3 (Control), Inattentive: 3 (Intervention), 3 (Control) | Adapted Cool Kids Cognitive-Behavioral Therapy (CBT) Program (10 sessions) | Usual care | 10 weeks + follow-up at 5 months | ADHD Symptom Severity (ADHD Rating Scale IV), Anxiety Severity (Spence Children’s Anxiety Scale - SCAS), Child Anxiety Life Interference Scale (CALIS), Pediatric Quality of Life Inventory (PedsQL), Parent Mental Health (Depression Anxiety Stress Scales - DASS), Parenting Consistency & Irritability Measures |
| Wong KP et al. [ | 2024 | Hong Kong, China | RCT | Children aged 6–12 years diagnosed with ADHD | Total = 90 (VR Training = 30, Traditional Social Skills Training = 30, Waitlist Control = 30) | VR: 8.63 ± 1.90, Traditional: 8.30 ± 1.70, Waitlist: 8.67 ± 1.45 | VR: 23 male (76.7%), 7 female (23.3%); Traditional: 26 male (86.7%), 4 female (13.3%); Waitlist: 24 male (80%), 6 female (20%) | Combined (63.3% VR, 80.0% Traditional, 86.7% Waitlist), Inattention, Hyperactivity/Impulsivity | Virtual Reality (VR) social skills training (12 sessions over 3 weeks) | Traditional Social Skills Training or Waitlist Control | 3 weeks | Social Skills Improvement System (SSIS-RS) – Parent Report, Executive Function – Behavior Rating Inventory of Executive Function (BRIEF-P) Inhibition/ Emotional Control, Clinical Psychologist Social Skills Assessment, Motion Sickness Questionnaire (VR Group Only) |
| Wong SYS et al. [ | 2023 | Hong Kong, China | RCT | Children with ADHD (8–12 years) and one parent per child | 138 families (69 MYmind, 69 CBT) | Children: MYmind: 8.9 ± 1.0 years, CBT: 9.2 ± 1.1 years, Parents: MYmind: 42.5 ± 5.0 years, CBT: 41.6 ± 5.1 years | Children: MYmind: 52 male (75.4%), 17 female (24.6%); CBT: 47 male (68.1%), 22 female (31.9%) | Inattentive and combined types | MYmind (Mindfulness-Based Intervention) | Cognitive Behavioral Therapy (CBT) | 8 weeks | Primary: Attention score (Sky Search, TEA-Ch), Secondary: ADHD symptoms (SWAN), executive function (BRIEF), disruptive behavior (ECBI), emotional regulation (RRS, WHO-5), parental stress (PSI) |
| Yao A et al. [ | 2022 | Japan | RCT | Children with ADHD (6–12 years old) & their parents (mothers) | 30 total (17 BPT, 13 Waitlist Control) | BPT: 8.96 ± 1.65 years, Control: 9.70 ± 1.82 years | BPT: 13 male (76.5%), 4 female (23.5%); Control: 13 male (100%), 0 female (0%) | All ADHD types included (diagnosed via DSM-5) | Behavioral Parent Training (BPT) – 13 weekly sessions | waiting list | 13 weeks | ADHD Symptoms (SNAP-IV) (Inattention, Hyperactivity/Impulsivity), Child Behavior Checklist (CBCL) – Attention Problems, Executive Function Tests (Go/No-Go Task (Response Inhibition), Single Response Selection Task (Response Selection Time)), Parenting Stress Index (PSI) – Child Domain |
| Zhao L et al. [ | 2024 | China | RCT | Children with ADHD (6-12 years old) | 90 (44 intervention, 46 control) | 8.4 ± 1.3 years | 71 male (78.9%), 19 female (21.1%) | Hyperactive/impulsive (68%), Combined (26%), Inattentive (6%) | BrainFit (Digital Cognitive-Physical Training, Augmented Reality-Based) | waitlist control | 4 weeks (12 sessions, 30 min each, 3x per week) | ADHD symptoms: SNAP-IV (Inattention, Hyperactivity/Impulsivity, Total ADHD Score, Oppositional Defiant Disorder), Executive Function: BRIEF (Metacognition Index, Behavioral Regulation Index, Global Executive Composite) |
| Zheng Q and Shum KK. [ | 2024 | Hong Kong, China | RCT | Preschoolers displaying ADHD symptoms | Total = 50 (Working Memory (WM) Training = 14, Social-Emotional (SE) Training = 15, Waitlist Control = 21) | Working Memory = 5.02 ± 0.73, SE = 4.94 ± 0.55, Waitlist Control = 4.89 ± 0.82 | WM: 9 male (64.3%), 5 female (35.7%); SE: 12 male (80%), 3 female (20%); Waitlist Control: 14 male (66.7%), 7 female (33.3%) | Children with diagnosed ADHD or meeting ADHD criteria based on SNAP-IV | Digital Working Memory (WM) training (5 weeks, 3 sessions per week, 10 minutes per session) | Active Control (Social-Emotional Training) and Waitlist Control | 5 weeks | ADHD Symptoms (SNAP-IV) – Parent report, Working Memory (Digit Span, Color Word Span, Picture Location), Executive Function (BRIEF-P Working Memory subscale), Time Perception (Time Production, Time Discrimination, Time Reproduction), Social-Emotional Skills (Situation Knowledge, Theory of Mind), Academic Abilities (Chinese Word Reading, Numeration) |
| Rank | Treatment | Probability of Best (%) | Probability of Worst (%) | Mean Difference (95% CI) |
| 1st | Family MBT | 92.3% | 0.0% | -8.88 (-13.50, -4.26) |
| 2nd | BPT (Face-to-Face) | 64.9% | 0.8% | -6.15 (-14.49, 2.19) |
| 3rd | SWAN (Online MBP) | 49.3% | 2.1% | -1.66 (-4.58, 1.26) |
| 4th | ADHD RS-IV (CBT) | 48.2% | 16.2% | -2.70 (-14.02, 8.62) |
| 5th | ADHD RS-IV (Yoga) | 38.6% | 8.9% | -0.90 (-14.74, 12.94) |
| 6th | BrainFit | 38.1% | 2.1% | -5.49 (-8.65, -2.33) |
| 7th | SWAN (FBMI) | 38.4% | 0.9% | -1.60 (-4.45, 1.25) |
| 8th | DBT Mindfulness | 34.5% | 0.2% | -4.3 (-9.37, 0.77) |
| 9th | Neurofeedback | 2.4% | 40.4% | 2.40 (-0.53, 5.33) |
| 10th | WM Training | 0.8% | 7.2% | 2.22 (-0.31, 4.75) |
| 11th | Control | 0.0% | 54.7% | 3.40 (1.24, 5.56) |
| 12th | Waiting List | 1.2% | 62.4% | 1.81 (-1.24, 4.86) |
| Rank | Treatment | Probability of Best (%) | Probability of Worst (%) | Mean Difference (95% CI) |
| 1st | BPT (PSI-SF) | 65.9% | 0.1% | -7.33 (-8.42, 23.08) |
| 2nd | Online MBP | 13.6% | 2.1% | -1.66 (-4.58, 1.26) |
| 3rd | CBT | 11.2% | 5.4% | -2.70 (-14.02, 8.62) |
| 4th | Usual Care | 8.1% | 10.3% | 3.40 (1.24, 5.56) |
| 5th | Waiting List | 1.2% | 69.2% | 20.90 (4.67, 37.13) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAttention Deficit Hyperactivity Disorder · Mindfulness and Compassion Interventions · Children's Physical and Motor Development
Introduction and background
Attention-deficit/hyperactivity disorder (ADHD) is among the most prevalent neurodevelopmental conditions that manifest during childhood, featuring symptoms including inattention, hyperactivity, and impulsivity. Conventional approaches to treatment have focused on pharmacological interventions, most notably with stimulant medications. However, increasing concerns about side effects and long-term effectiveness have turned the spotlight on non-pharmacological interventions. These include mindfulness-based interventions (MBIs), cognitive-behavioral therapy (CBT), behavioral parent training (BPT), neurofeedback techniques, virtual reality (VR), and digital working memory training (WMT). Although research on these interventions is abundant, no comparative analysis of their relative effectiveness in managing childhood ADHD has been conducted [1,2].
MBIs, as a behavioral strategy to enhance attention control and emotional self-regulation in children with ADHD, have received considerable research attention [3]. These practices promote present-moment awareness and nonjudgmental acceptance, leading children to identify distractions and exercise better impulse control. A wide range of MBI models have been adapted for ADHD populations, including mindfulness-based stress reduction (MBSR), mindfulness-based cognitive therapy (MBCT), acceptance and commitment therapy (ACT), dialectical behavior therapy (DBT), compassion-focused therapy (CFT), and mindful self-compassion [4]. Mindfulness-based approaches may also include yoga, which includes physical postures, breathing exercises, and meditation for self-regulation and awareness of the body (both are areas often compromised in children with ADHD) [5].
Research shows these interventions improve executive function, decrease hyperactivity, and increase emotional regulation, making them a worthwhile non-pharmacological treatment option for ADHD management. Furthermore, mindfulness interventions may be implemented in a family-based or parent-based format, recognizing the significant role that caregivers play in shaping a child's emotional and behavioral responses [5].
However, CBT has been shown to provide one of the more effective interventions for ADHD, due to improving emotional regulation and coping strategies over time. Unlike MBIs, which focus on attentional training and self-awareness, CBT addresses maladaptive thought processes and behavioral responses in children, providing them with structured strategies for managing impulsivity and inattention. While CBT addresses the cognition, BPT addresses the environment by using reinforcement-based approaches to address the behavior and functioning of the child. Parent-mediated interventions have been shown to have considerable effectiveness in ameliorating disruptive behaviors and improving parental responsiveness [6].
New technological developments have led to innovative interventions that incorporate digital and AI-enabled techniques to improve cognitive and behavioral outcomes in children who have ADHD. Virtual reality interventions serve as simulated real-world environments, fostering behavioral training under safe conditions. Digital WMT programs target weaknesses in executive functioning (a primary deficit in ADHD) through interactive cognitive exercises that work to strengthen attention span and the duration of information retention [7].
Neurofeedback and brain-fit are other promising techniques that are just coming into interest as ways to stimulate brain activity. Such methods target patterns of neural activity that govern attention and impulse control. Neurofeedback is particularly exciting because it allows children to self-modulate their attention states and improve executive function by providing feedback on brainwave activity in real-time. The results are promising, but these methods need to be compared to find out how long they work and how they compare with other well-known interventions [8].
However, despite the diverse nature of these interventions [9], a direct comparison between them in terms of effectiveness for the treatment of childhood ADHD is not available. This network meta-analysis aimed to provide a rigorous methodological approach to combine evidence from multiple treatment comparisons, enabling a more comprehensive assessment of both direct and indirect evidence. The comparative effectiveness of MBIs, CBT, BPT, brain enhancement techniques, VR interventions, and digital WMT were explored in terms of their ability to address ADHD symptoms (attention, impulsivity, hyperactivity). The results provide a ranked ordering of these interventions, which would be invaluable for clinicians, educators, and policymakers who are searching for evidence-based alternatives/developments to pharmacological treatment.
Review
Methods and research question
This network meta-analysis was conducted and reported according to the principles of STATA 18 [10]. The research question was: What is the comparative effectiveness of the following interventions that have been investigated using controlled clinical trials on core symptoms and executive functioning in children with ADHD: mindfulness-based interventions (parent-based, family-based, yoga, or digital cognitive mindfulness training (DPT) based), CBT, BPT, techniques to enhance brain activity, VR interventions, and digital working memory (DWM) training, assessed by a network meta-analysis?
Research Aims and Objectives
The aim of this study was to assess and compare the relative effects of mindfulness-based interventions (including parent-based, yoga, family-based, or DPT-based), CBT, BPT, techniques for the enhancement of brain activity such as neurofeedback, VR interventions, and DWM training on inattention, hyperactivity, and executive functioning in children with ADHD. The objectives of this study were to: a) compare the efficacy of non-pharmacological interventions in reducing core symptoms of childhood ADHD (inattention, and impulsivity) and their impact for family and parents; b) evaluate the effectiveness of mindfulness-based interventions in managing ADHD symptoms compared to control interventions; and c) quantify the relative ranking of non-pharmacological interventions for childhood (ADHD) based on effectiveness using a network meta-analysis approach and providing evidence-based recommendations for clinicians and educators regarding the effectiveness of these interventions.
Inclusion Criteria
This study included randomized and non-randomized controlled studies published in English from the beginning until March 22, 2025. Eligible studies included controlled clinical trials that compared some non-pharmacological interventions with waiting list or usual care in children with ADHD. Although a restriction concerning adult age was made, no restrictions were made regarding the sex or race of the participants.
Interventions
This meta-analysis included clinical trials that enrolled school and preschool children and assessed one or more of the following non-pharmacological interventions compared with waiting list (no intervention), usual care, or active treatment: Mindfulness-Based Interventions (MBIs), including parent-based, DPT-based, yoga, and family-based mindfulness; CBT; BPT; Brain Activity Enhancement Techniques (e.g., neurofeedback, BrainFit); VR Interventions; and Digital WMT.
Exclusion Criteria
We excluded animal studies, retrospective studies, conference abstracts, duplicate records, case reports, reviews, commentaries, case series, studies included only adult population and studies that lacked a control group (e.g., waiting list, usual care, non-pharmacological modality), studies that did not report relevant outcomes (e.g., studies, in which, quality of life or emotional regulation were the principle outcomes).
Search Strategy
Electronic searches: We searched the following electronic databases for eligible studies: MEDLINE/PubMed, Cochrane Central Register of Controlled Trials (CENTRAL), Web of Science, ProQuest, and Scopus. The search was limited to articles published in English from the inception of the databases until March 22, 2025.
The following search terms were used: ("Attention Deficit Hyperactivity Disorder" OR "ADHD" OR "ADD"OR "Hyperkinetic Disorder")AND("Mindfulness" OR "Mindfulness-Based" OR "Mindfulness Training" OR "Mindfulness-Based Cognitive Therapy" OR "MBCT"OR" Mindfulness-Based Stress Reduction" OR "MBSR"OR "Acceptance and Commitment Therapy" OR "ACT" OR "Dialectical Behavior Therapy" OR "DBT" OR "Mindful Awareness Practices" OR "Meditation" OR "Yoga") AND ("Cognitive Behavioral Therapy" OR "CBT" OR "Behavioral Therapy" OR "Pharmacotherapy" OR "Stimulants" OR "Methylphenidate" OR "Amphetamines" OR "Non-Stimulants" OR "Atomoxetine" OR "Guanfacine" OR "Usual Care" OR "Waitlist Control")AND("Randomized Controlled Trial" OR "RCT" OR "Clinical Trial")AND("pediatric" OR child*). We searched the reference lists of the obtained articles for other potentially relevant studies that were not retrieved through an electronic search.
Selection of studies and data extraction: The retrieved reports were screened for eligibility based on their title and abstract, and then further evaluated through full-text screening. We extracted data from the included studies using a standardized data sheet that included the following: (a) the study’s characteristics (the author, year, the country, study design); (b) patients’ characteristics (age at the time of treatment, sex, sample size, study population, and ADHD type); (c) intervention and control groups' details (active intervention, comparison arm, treatment period), and (d) the outcomes based on the child behavior checklist (CBCL), Conners' rating scale (CRS), hypercompulsivity and inattention, total ADHD rating scale (RS)-IV, (e) total SWAN (strengths and weaknesses of ADHD symptoms and normal behaviors), and (f) parenting stress index-short form (PSI-SF). We checked the collected data for consistency and clarity.
Measured Outcomes (All Were Measured As Mean and Sd)
These included: a) CBCL: parent-reported questionnaire designed to assess internalizing problems (e.g., anxiety, depression, social withdrawal), externalizing problems (e.g., aggression, rule-breaking behavior), and attention problems by a three-point Likert scale for each behavioral item, where parents rate their child’s behavior based on the past six months; b) CRS: parent-reported scale that uses a four-point Likert scale to assess inattention, impulsivity, executive function, and behavioral problems. There is a version suitable for preschool and other for schoolchildren; c) Inattention and impulsivity measurement (multiple used scales reported by parents); d) Total ADHD rating scale (RS)-IV: a behavioral rating scale designed to assess the severity of ADHD symptoms in children and adolescents, based on DSM-IV ADHD criteria and includes 18 core ADHD symptoms divided into inattention subscale (9 items) and the hyperactivity-impulsivity subscale (9 items); e) Total SWAN: a behavioral rating scale designed to assess ADHD symptoms in children and adolescents using a seven-point Likert scale; and f) PSI-SF: a measurement for parental stress related to child-rearing in 15-20 minutes, containing 36 items (compared to the full PSI).
Risk of Bias Assessment and Data Synthesis
We assessed the risk of bias (ROB) in the included studies using the National Institute for Health and Care Excellence (NICE) checklists for randomized controlled clinical trials [11]. Initially, 682 records were retrieved from electronic database searches. After removing duplicates and excluding studies, 74 studies were finally eligible, of which 16 were double-armed clinical trials, 15 were randomized studies, and 1 was a non-randomized study (806 participants) (Table 1). Of the 16 studies included [12-27], nine examined different mindfulness-based practices for children with ADHD [12,14,16-21,24]. Two studies were on BPT [13,25], one on CBT [22], one study on VR training [23], one on working memory training [27], and two studies about brain function enhancement techniques [15,26]. The usual control was a waitlist control or usual care in most studies, but one study compared CBT directly with a mindfulness-based intervention. Concerning the 58 excluded clinical trials from the MA, they were either studies that were irrelevant (n=42), duplicates (n=3), had an adult population (n=5), had irrelevant outcomes (n=5), study protocol (n=2), or were not accessible (n=1) (Figure 1).
PRISMA flow chartPRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Statistical Analysis
This network meta-analysis was conducted using STATA 18, employing a frequentist approach with a fixed-effects model due to minimal heterogeneity across studies (Df = 0 in most comparisons). Treatment effects were estimated using multivariate meta-analysis with the mvmeta command, and indirect comparisons were made within a fully connected network. Consistency between direct and indirect estimates was assessed using the design-by-treatment interaction model, which showed no significant inconsistency. Treatment rankings were derived using the surface under the cumulative ranking (SUCRA) method, providing probabilities for each intervention’s relative effectiveness. Between-study heterogeneity was evaluated using the tau-squared (τ²) statistic, indicating minimal variability. Sensitivity analyses were performed by excluding studies with extreme values to test the robustness of findings. Graphical representations, including network plots, ranking probability distributions, and league tables, were generated to summarize results and facilitate interpretation.
Results
Overview of Included Studies
We included a total of 16 studies, comprising 806 participants [12-27]. The network compared various interventions for pediatric ADHD, including mindfulness-based therapies and other active treatments, across multiple outcome measures.
Child Behavior Checklist Outcomes
The network analysis included two studies evaluating the impact of different treatments on CBCL scores [17,25]. The results showed that FBMI and WL had slightly higher mean values compared to BPT, but neither difference was statistically significant (family-based mindfulness intervention (FBMI) vs. BPT: MD = 1.93, p = 0.075; WL vs. BPT: MD = 1.95, p = 0.071), as the confidence intervals included zero. Treatment rankings based on the SUCRA analysis showed that BPT was the most likely to be the best treatment (95.8%), followed by FBMI (2.7%) and WL (1.5%), suggesting that BPT was the most effective intervention in this network, while WL was the least effective (Figure 2).
Network plot of treatment comparisons for child behavior checklist outcomesFBMI, Family-Based Mindfulness Intervention; WL, Waitlist; BPT, Behavioral Parent Training
Conners' Rating Scale (CRS) Outcomes
For CRS scores, BPT (face-to-face) showed the greatest reduction, though not statistically significant (MD = -6.15, 95% CI: -14.49 to 2.19, p = 0.148). DBT mindfulness also showed improvement (MD = -4.3, 95% CI: -9.37 to 0.77, p = 0.096). Control and family mindfulness showed slight increases in CRS scores (MD = 1.95 and 3.18, respectively), indicating less effectiveness (Figure 3).
Network plot of treatment effects for Conners’ rating scale outcomesBPT, Behavioral Parent Training; DPT, Digital Cognitive Mindfulness Training
Hyper-compulsivity Outcomes
In the hyper-compulsivity analysis, family mindfulness showed the highest probability (61.5%) of being the best treatment, while BrainFit was the second-best option (38.1%). Control performed the worst (MD = 2.60, p = 0.041), while neurofeedback (MD = 2.40, p = 0.109) and WMT (MD = 2.22, p = 0.086) had intermediate but statistically non-significant effects (Figure 4).
Network plot of treatment effects for hyper-compulsivityWM, Working Memory
Inattention Outcomes
Family MBT significantly reduced inattention symptoms (MD = -8.88, 95% CI: -13.50 to -4.26, p < 0.001) and had a 100% probability of ranking as the best intervention. Brain function enhancement was most likely to rank second (76.5%), whereas digital WMT (70.2%) and waiting list (76.4%) ranked among the least effective interventions (Figure 5).
Network plot of treatment effects for inattentionWMT, Working Memory Training; MBT, Mindfulness-Based Therapies; BPT, Behavioral Parent Training
ADHD Rating Scale-IV (Total ADHD RS-IV) Outcomes
Four studies assessed ADHD RS-IV scores across different interventions. Family mindfulness had the highest probability of being the best treatment (48.2%), followed by yoga (38.6%). Mindful parenting was most likely to be the least effective intervention (43.2% probability of ranking last). None of the treatments showed statistically significant differences from CBT (Figure 6).
Network plot of treatment effects for ADHD rating scale-IV (total ADHD RS-IV) outcomesCBT, Cognitive Behavioral Therapy References [12,16,17,22]
SWAN Total Outcomes
Three studies evaluated SWAN total scores for different interventions. Online MBP was ranked as the best treatment (49.3%), followed by FBMI (38.4%), CBT (11.1%), and waiting list (1.2%). However, none of the comparisons showed statistically significant differences from CBT, suggesting comparable effectiveness among these interventions (Figure 7).
Network plot of treatment effects for strengths and weaknesses of attention-deficit/hyperactivity disorder symptoms and normal behaviors (SWAN) total outcomesFBMI, Family-Based Mindfulness Intervention; MBP, Mindfulness-Based Program; CBT, Cognitive Behavioral TherapyReferences [17,18,24]
Parenting Stress Index-Short Form (PSI-SF) Outcomes
Seven studies evaluated parenting stress across different interventions. BPT had the highest probability (65.9%) of being the most effective intervention, followed by online MBP (13.6%) and CBT (11.2%). Usual care had the highest probability of ranking as the least effective intervention (69.2%) (Figure 8).
Network plot of treatment effects for parenting stress index-short formFBMI, Family-Based Mindfulness Intervention; MBP, Mindfulness-Based Program; CBT, Cognitive Behavioral Therapy; PPMI, Parallel Parent–Child Mindfulness InterventionReferences [13,14,17-19,24,25]
Treatment Ranking
We ranked treatments using the SUCRA and the mean rank for each outcome to assess the relative effectiveness and safety of the interventions. SUCRA values range from 0% to 100%, where higher values indicate a greater likelihood that treatment is among the most effective or safest options. While SUCRA and mean rank provide a useful summary of treatment hierarchy, they should be interpreted with caution, considering the uncertainty in effect estimates and the clinical relevance of absolute differences between treatments.
The results suggested that mindfulness-based interventions, particularly Family MBT and BPT (face-to-face), showed promise in improving ADHD-related symptoms. Family mindfulness was highly effective for hyperactivity and inattention outcomes, while ADHD RS-IV scores favored CBT and yoga. SWAN results suggested online MBP and FBMI were the most effective interventions. In contrast, control groups consistently underperformed, emphasizing the value of active treatments. The PSI-SF analysis highlighted that parenting stress was most effectively reduced by BPT (Tables 2, 3).
Risk of Bias
Based on the RoB assessment, the quality of included studies varied across different domains. Random sequence generation was generally well-conducted, with most studies rated as low risk, except for a few with unclear risk. Allocation concealment showed a mix of low and unclear risk, indicating that some studies lacked sufficient details on whether allocation was adequately concealed. Blinding of participants and personnel (performance bias) exhibited notable concerns, with many studies rated as high risk, as blinding for active treatment was not applicable in most of the studies. Similarly, blinding of outcome assessment (detection bias) varied, with several studies showing unclear or high risk, potentially impacting the objectivity of outcome evaluation. Incomplete outcome data (attrition bias) was generally well-handled across studies, with most rated as low risk. Selective reporting (reporting bias) was also mostly low risk, indicating that most studies reported their outcomes as intended. Other bias domains showed minimal concerns. Overall, while certain domains, such as sequence generation and attrition bias, were well-addressed, issues with blinding and allocation concealment suggest potential methodological weaknesses that could influence the reliability of the findings (Figures 9, 10).
Risk of bias graph
Risk of bias summaryReferences [12-27]
Discussion
ADHD is one of the most common neurodevelopmental disorders in children and adolescents, characterized by symptoms of inattention, hyperactivity, and impulsivity. While most conventional treatment methods (e.g., stimulant medications and behavioral therapy) are effective, they are not appropriate for everyone due to side effects, accessibility issues, and patient variability in response. Therefore, other therapeutic alternatives are increasingly emphasized for controlling ADHD symptoms, such as mindfulness-based therapies (MBTs), neurofeedback, and WMT [2].
This study aimed to simultaneously compare the effect of different interventions for pediatric ADHD on multiple symptom measures and parenting stress indices. We performed a network meta-analysis of data from 16 studies with 806 participants to compare the relative efficacy of different interventions, offering a complete ranking of interventions according to their effectiveness across ADHD symptoms and family-specific outcomes.
Concerning CBCL scores, family mindfulness showed the most substantial improvement, with a significant reduction in CBCL scores compared to the reference treatment, BrainFit. These findings are consistent with a study by van de Weijer-Bergsma et al., which showed improvements at the CBCL with mindfulness-based interventions among children with ADHD [28]. However, our findings are contrary to the findings of Van der Oord et al., who reported only small improvements in CBCL with mindfulness compared to CBT [29].
Control groups exhibited the least improvement, whereas neurofeedback and WMT were intermediate across studies; however, neurofeedback did not reach statistical significance. These results are somewhat in line with Gevensleben et al. [30], who found positive but small effects of neurofeedback, whereas a meta-analysis by Cortese et al. [31] reasoned that neurofeedback is not a reliable long-term treatment for the reduction of ADHD symptoms.
For CRS outcomes, BPT in a face-to-face format showed the largest symptom reduction, though not statistically significant. These results align with a meta-analysis by Daley et al. [32], which found that BPT effectively reduces ADHD symptoms but noted variability in its impact across different studies.
In contrast, both family mindfulness and control groups experienced minimal increases in CRS scores, indicating that neither treatment improved behavioral regulation. These findings are contrary to those of Ridderinkhof et al., who noted that mindfulness interventions had moderate effects on improved CRS scores [33]. The difference might, however, be explained by differences in intervention duration and characteristics of participants from different studies.
Family mindfulness demonstrated the highest probability (61.5%) of being the most effective treatment for hyperactivity/impulsivity, with BrainFit as the second-best option (38.1%). Conversely, control performed the worst, while neurofeedback and WMT had non-significant effects. These findings are consistent with those of Sonuga-Barke et al., who found limited evidence for cognitive training’s direct impact on core ADHD symptoms [34].
For inattention symptoms, family MBT was highly effective, ranking as the best intervention (100% probability). These findings align with the results of Zylowska et al., who observed significant reductions in inattention symptoms following mindfulness interventions [35]. However, brain function enhancement (76.5%) ranked as the second-best intervention, contrasting with previous studies that have reported mixed results regarding its efficacy.
Four studies evaluated ADHD RS-IV scores [12,16,17,22]. Family mindfulness ranked first (with 48.2%), while the second one was yoga (38.6%). Cohen et al. support these results, identifying yoga-based interventions as a benefit for symptom reduction [12]. On the other hand, Mindful Parenting appeared to be the least effective (43.2% probability of being last), which could indicate that parent-directed mindfulness approaches had a lower effect on the severity of child ADHD symptoms.
Three studies evaluated SWAN total scores, with online MBP (49.3%) and FBMI (38.4%) ranking as the most effective treatments, while CBT (11.1%) and waiting list (1.2%) ranked among the least effective [17,18,24]. However, no comparisons showed statistically significant differences from CBT, suggesting that these interventions may be comparable in effectiveness. These findings contrast with a meta-analysis by Cairncross M and Miller CJ, which found CBT to be a superior intervention for ADHD symptom management [36].
Seven studies assessed parenting stress levels across different interventions, with BPT showing the highest probability (65.9%) of being the most effective intervention [13,14,17-19,24,25]. These findings align with the results of Theule et al., who reported that BPT consistently reduces parenting stress in families of children with ADHD [37].
In contrast, usual care was ranked as the least effective (69.2%), supporting the notion that structured interventions provide superior benefits compared to passive control conditions. Online MBP (13.6%) and CBT (11.2%) ranked as intermediate interventions, suggesting potential benefits but with lower efficacy compared to BPT.
The SUCRA values provided a hierarchy of treatment effectiveness. Mindfulness-based interventions (family MBT, online MBP, and FBMI) consistently ranked among the top treatments for ADHD-related symptoms, particularly inattention and hyperactivity. In contrast, control groups consistently performed the worst, reinforcing the necessity of active interventions.
However, it is important to interpret SUCRA rankings cautiously, as they do not account for absolute treatment effects. Additionally, while some interventions showed promising effects, their clinical significance remains uncertain due to high variability across studies. Future research should incorporate larger sample sizes, longer follow-up durations, and direct head-to-head comparisons to validate these findings.
The risk of bias assessment revealed potential methodological concerns, particularly regarding blinding and allocation concealment. While random sequence generation and attrition bias were well-addressed, the lack of blinding in some studies may have introduced performance and detection bias, affecting the reliability of certain findings. These methodological weaknesses should be considered when interpreting the results.
Limitations
Several limitations of this network meta-analysis should be considered when interpreting the results. First, the studies had different levels of risk of bias, especially in the areas of allocation concealment and blinding of participants and outcome assessors. The lack of blinding in many studies may have introduced performance and detection biases, which could have influenced the reported treatment effects. Second, the small sample sizes in some studies may have limited the statistical power to detect significant differences between interventions, leading to wider confidence intervals and increased uncertainty in treatment rankings. Third, while the fixed-effects model was used due to minimal observed heterogeneity, unmeasured sources of heterogeneity, such as variations in intervention protocols, participant characteristics, and outcome measures, may still impact the generalizability of findings.
Conclusions
This network meta-analysis provides a comprehensive comparison of various interventions for pediatric ADHD, highlighting the potential benefits of mindfulness-based therapies and BPT. Family mindfulness emerged as the most effective intervention for reducing ADHD symptoms, particularly inattention and hyperactivity. BPT also demonstrated significant benefits, especially in improving attention and reducing parenting stress.
The analysis consistently showed that control conditions and WL ranked among the least effective interventions, reinforcing the importance of active treatments. Despite some methodological limitations, including potential biases and small sample sizes in some studies, these findings provide valuable insights into treatment hierarchies for ADHD interventions. To validate these results and enhance their clinical applicability, future research should focus on large-scale, high-quality randomized controlled trials with longer follow-up periods and rigorous blinding procedures.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1ADHD: current concepts and treatments in children and adolescents Neuropediatrics Drechsler R Brem S Brandeis D Grünblatt E Berger G Walitza S 3153355120203255980610.1055/s-0040-1701658 PMC 7508636 · doi ↗ · pubmed ↗
- 2Non-pharmacologic management of attention-deficit/hyperactivity disorder in children and adolescents: a review Transl Pediatr Shrestha M Lautenschleger J Soares N 0249202010.21037/tp.2019.10.01PMC 708224532206589 · doi ↗ · pubmed ↗
- 3Effects of mindfulness-based interventions in children and adolescents with ADHD: a systematic review and meta-analysis of randomized controlled trials Int J Environ Res Public Health Lee YC Chen CR Lin KC 151981920223642991510.3390/ijerph 192215198 PMC 9690476 · doi ↗ · pubmed ↗
- 4Cognitive-based interventions for improving psychological health and well-being for parents of children with developmental disabilities: a systematic review and meta-analysis J Autism Dev Disord Li S Yong Y Li Y Li J Xie J 331633355420243766885010.1007/s 10803-023-06063-x PMC 11362495 · doi ↗ · pubmed ↗
- 5A systematic review of yoga and meditation for attention-deficit/hyperactivity disorder in children Cureus Gonzalez NA Sakhamuri N Athiyaman S 015202310.7759/cureus.36143 PMC 1010123837065343 · doi ↗ · pubmed ↗
- 6Cognitive-behavioural interventions for attention deficit hyperactivity disorder (ADHD) in adults Cochrane Database Syst Rev Lopez PL Torrente FM Ciapponi A 03201810.1002/14651858.CD 010840.pub 2PMC 649439029566425 · doi ↗ · pubmed ↗
- 7Exploring virtual reality and exercise simulator interventions in patients with attention deficit hyperactivity disorder: comprehensive literature review JMIR Serious Games Sarai G Jayaraman PP Tirosh O Wickramasinghe N 013202510.2196/57297 PMC 1182232839879092 · doi ↗ · pubmed ↗
- 8Benefits of a 12-week non-drug “brain fitness program” for patients with attention-deficit/hyperactive disorder, post-concussion syndrome, or memory loss J Alzheimers Dis Rep Fotuhi M Khorrami ND Raji CA 675697720233748332210.3233/ADR-220091 PMC 10357116 · doi ↗ · pubmed ↗