Outcomes of Cardiac Repair in Heterotaxy Syndrome Patients—Tertiary Center Experience
Mohammad A. Ebrahim, Nada T. Alzayed, Sakeena M. Alsahhaf, Mohammad A. Almulla, Karim M. Yassin, Leina A. Shabaan, Moustafa A. Elsayed, Vadim G. Lyubomudrov

TL;DR
This study examines outcomes and risk factors in patients with heterotaxy syndrome who underwent cardiac repair, focusing on mortality and arrhythmia.
Contribution
The study identifies risk factors for mortality and arrhythmia in HS patients based on atrial isomerism and repair type.
Findings
Patients with right atrial isomerism had a higher mortality rate compared to those with left atrial isomerism.
Pulmonary venous anomalies were more common in patients with right atrial isomerism.
Lower initial operation age was a significant risk factor for mortality.
Abstract
This study aims to determine factors associated with poor outcomes and frequency of arrhythmia incidence in patients with heterotaxy syndrome (HS). A retrospective cohort study in a single tertiary center was conducted and included patients with operated HS between 2011 and 2020. A total of 52 patients were included. Relevant factors associated with mortality that were considered included univentricular (UV) or biventricular (BV) physiology, prematurity, low weight/age at surgery, the presence of atrioventricular valve regurgitation, anomalous pulmonary veins drainage, and type of atrial isomerism. Thirty-three patients (63.4%) were diagnosed with left atrial isomerism (LAI), whereas the remaining 19 (36.5%) were diagnosed with right atrial isomerism (RAI). Thirty-eight patients (73%) underwent UV repair, whereas 14 patients (27%) had BV physiology. Patients were followed up for an…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
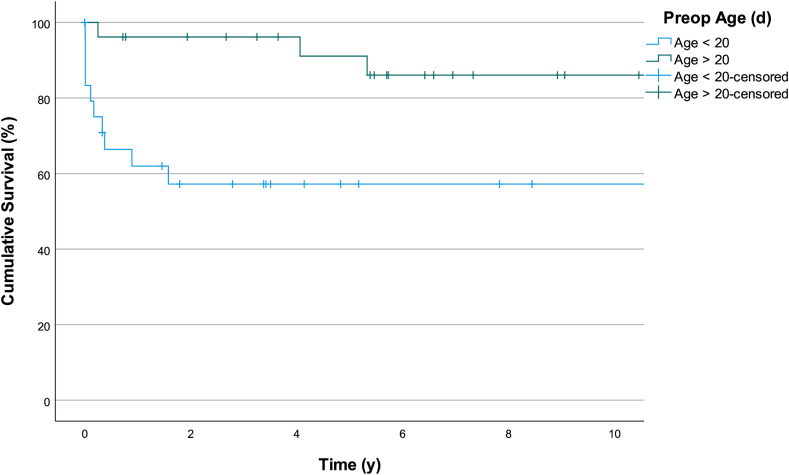 Figure 1
Figure 1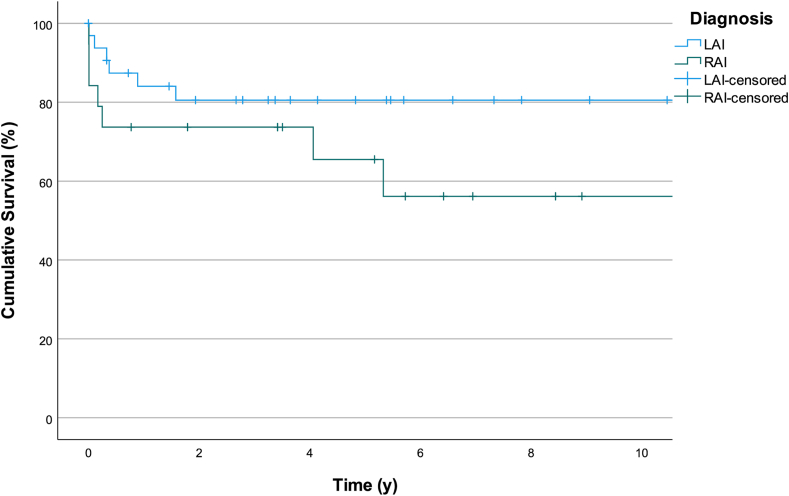 Figure 2
Figure 2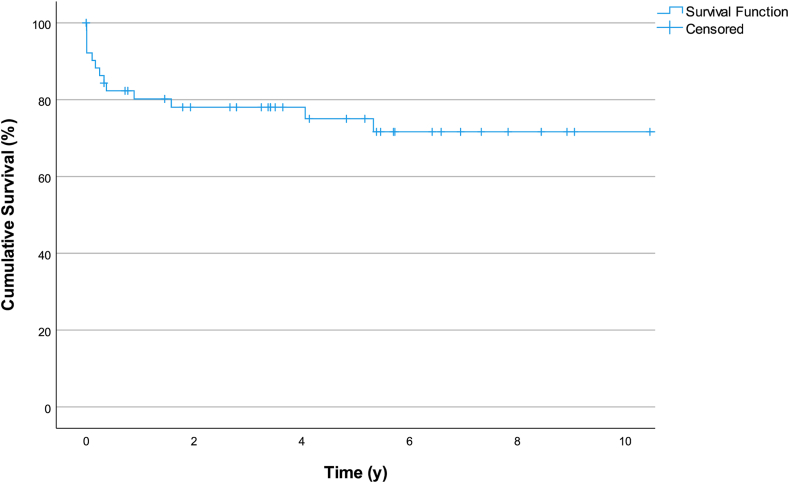 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Heart Disease Studies · Cardiac Structural Anomalies and Repair · Cardiovascular Issues in Pregnancy
Heterotaxy syndrome (HS) is defined as an abnormal arrangement of viscera across the left-right axis that differs from situs solitus and situs inversus totalis.1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11 This rare condition, estimated to impact 1 to 5000-7000 live births, has 2 variants: right atrial isomerism (RAI) and left atrial isomerism (LAI).1^,^4, 5, 6^,^11 Both variants are associated with complex intracardiac abnormalities; however, RAI is linked to a higher incidence of univentricular (UV) physiology, complete atrioventricular (AV) septal defect, total anomalous pulmonary venous drainage (TAPVD), and pulmonary stenosis.1^,^4, 5, 6^,^11
This study aims to present the most recent experience in managing patients with HS, along with midterm outcomes at Chest Diseases Hospital in Kuwait, which is the only hospital to provide congenital cardiac surgeries in the country. Risk factors (RFs) for mortality were assessed, alongside documenting arrhythmia incidence throughout follow-up.
Methods
Study population
A retrospective cohort study in a single tertiary center was conducted and included patients with operated HS between 2011 and 2020 with follow-up until March 2024. Such patients were identified using a surgical database, created in 2008, which incorporated all pediatric cardiac surgeries performed at Chest Diseases Hospital. HS was further confirmed through review of digital patient files and imaging, with patients categorized as having either RAI and LAI. RAI is characterized by bilateral right-sided atrial appendages, trilobed lungs, a midline liver, and frequently, bilateral superior vena cava, whereas LAI features bilateral left-sided atrial appendages, bilobed lungs, interrupted inferior vena cava, and polysplenia.12
Inclusion criteria were patients with HS who underwent primary cardiovascular repair at our center during the study period. Exclusion criteria included all patients who underwent primary cardiovascular repair at an outside institution or patients with situs inversus totalis. Each subject was assigned a unique identifier number, which was used to reference the data during analysis. This study was approved by the Ministry of Health Standing Committee for Coordination of Health and Medical Research.
Variables
Data collected for each patient included demographic information (gestational age, birth weight, and sex), clinical characteristics (age and weight at the time of initial surgery, type of atrial isomerism, presence of dextrocardia, and fetal diagnosis status), anatomic and echocardiographic findings (AV septal defect, pulmonary venous anatomy, presence, and degree of AV valve regurgitation), and perioperative variables (type of surgical procedure, cardiopulmonary bypass, and aortic cross-clamp times). Postoperative data, including duration of mechanical ventilatory support, in-hospital mortality, and other surgical complications, were recorded. Rhythm status (presence of nonsinus atrial rhythm, high-grade heart block (HB), and supraventricular tachycardia [SVT]) was also recorded. For some patients, computed tomography and/or cardiac catheterization were performed to better delineate the cardiac anatomy. Follow-up information was obtained from clinical notes and imaging during routine outpatient visits.
The primary outcome was all-cause mortality during follow-up. Secondary outcomes included the occurrence of significant arrhythmias and postoperative complications. Factors assessed for association with mortality included type of atrial isomerism, type of physiology (UV or biventricular [BV]), prematurity, low birth weight, early age or weight at surgery, presence of AV valve regurgitation, and anomalous pulmonary venous return.
Statistical analysis
Statistical analysis was performed with the IBM Statistical Product and Service Solution 26 (SPSS; IBM Corporations, Armonk, NY). Continuous variables were expressed as median, with interquartile ranges [Q1-Q3] in brackets. Differences in categorical variables were compared using the χ^2^ or the Fisher exact test, and the Mann-Whitney U test, Kruskal-Wallis test, or analysis of variance test was used to compare continuous variables, as appropriate. Patient data were processed through Kaplan-Meier survival analysis. RFs for mortality were identified by using Cox proportional hazards regression. A P value of <0.05 was considered significant and was used for variable inclusion on multivariate analysis.
Results
Fifty-two patients were included in the final data analysis. Thirty-three patients (63.4%) were diagnosed with LAI, whereas the remaining 19 (36.5%) were diagnosed with RAI. Table 1 illustrates the characteristics of the entire cohort. Very few patients had fetal diagnosis. The median age at diagnosis was 1 day (0-6.5 days). Thirty-eight patients (73%) underwent UV repair, whereas 14 patients (27%) had BV repair. Eight patients (15.2%) underwent a bidirectional Glenn procedure, and 17 patients (32.7%) eventually received Fontan palliation. The median age at the initial operation was 19 days (5-144 days), and the median operation weight was 3.7 kg (2.8-5 kg). Patients were followed up for an average of 4.8 years (0-12.8 years). Lastly, 14 patients (27%) had died during the follow-up period.Table 1. Main preoperative characteristics and types of surgical palliation or complete repair for the entire cohort including intraoperative data, mortality, and follow-up per type of atrial isomerismCharacteristicsRAI (n = 19)LAI (n = 33)P valueFetal diagnosis, n (%)1 (5)9 (27)0.053Age at diagnosis (median/d)110.917Initial operation age (median/d)18200.918Initial operation weight (median/kg)3.23.70.423Gestational age (wk)38370.193Pulmonary venous anomalies7 (6 SV patients)5 (all BV patients)0.074Obstructive TAPVD, n (%)2 (11)00.057Initial surgery, n (%) BTS10 (53)10 (30)0.111 PAB1 (5)6 (18)0.189 Norwood1 (5)4 (12)0.419 BDG3 (16)00.019 TAPVD repair1 (5)2 (6)0.906 TAPVD repair/BTS1 (5)00.183 TAPVD/BDG1 (5)00.183 Hybrid02 (6)0.274 PM02 (6)0.274 PM/PAB01 (3)0.444 AVSD repair01 (3)0.444 POTTS shunt1 (5)00.183 PAPVD/VSD repair02 (6)0.274 DORV/PS (TAP)01 (3)0.444 Kawashima01 (3)0.444 VSD closure01 (3)0.444Biventricular repair, n (%)1 (5)13 (39)0.008Univentricular repair, n (%)18 (95)20 (61)0.008Bidirectional Glenn, n (%)3 (16)5 (15)0.951Fontan, n (%)10 (53)7 (21)0.02CPB/ACC time (min)66.5/3178/510.462/0.062Nonsinus atrial rhythm, n (%)10 (53)17 (52)0.938SVT, n (%)3 (16)5 (15)0.9562:1 or higher grade HB, n (%)04 (12)0.114Dextrocardia, n (%)11 (58)11 (33)0.084Death, n (%)8 (42)6 (18)0.061Follow-up (y)45.30.258ACC, aortic cross-clamp; AVSD, atrioventricular septal defect; BDG, bidirectional Glenn; BTS, Blalock-Taussig shunt; BV, biventricular; CPB, cardiopulmonary bypass; DORV, double outlet right ventricle; HB, heart block; LAI, left atrial isomerism; PAB, pulmonary artery banding; PAPVD, partial anomalous pulmonary venous drainage; PM, pacemaker; PS, pulmonary valve stenosis; RAI, right atrial isomerism; SV, single ventricle; SVT, supraventricular tachycardia; TAP, transannular patch; TAPVD, total anomalous pulmonary venous drainage; VSD, ventricular septal defect.
Surgical results
Surgical and intraoperative data are summarized in Table 1. Notably, most patients with complete repair are among the LAI group, and high-grade HB only occurred in patients with LAI. Moreover, patients with LAI were more likely to receive a BV repair (13/33 [39%]), compared with patients with RAI (1/19 [5%]), whereas patients with RAI were more likely to receive UV repair (18/19 [95%]), compared with patients with LAI (20/33 [61%]) (P = 0.008). In addition, pulmonary venous anomalies occurred more frequently among the RAI vs the LAI groups (37% vs 15%, P = 0.074). Furthermore, the malignant combination of obstructed anomalous pulmonary venous return with single-ventricle (SV) physiology only occurred in the RAI cohort (11%, P = 0.057). As expected, nonsinus rhythm was frequently present among the cohort (approximately 50%). In addition, dextrocardia was more associated with RAI (58% vs 33%, P = 0.084). Finally, the mortality rate was significantly higher among the RAI group than the LAI cohort (42% vs 18%, P = 0.06).
Table 2 shows the postoperative complications identified from the patient data after undergoing an initial surgical repair. Eight different complications were identified, and their rates are shown for the total patient group and the subgroups. The most common identified complication was the need for prolonged mechanical ventilatory support (>72 hours), which was identified in 34.6% of the total patient group (P = 0.8). The small sample size of our cohort limited the statistical significance of the complication rates with the exception of “intraventricular hemorrhage/clot,” which was identified in 15.8% of patients with RAI compared with none among the LAI cohort (P = 0.02).Table 2. Initial postoperative data and mortality per type of atrial isomerismInitial repairTotal (n = 52)RAI (n = 19)LAI (n = 33)P valuePostoperative dataComplications, n (%) Sternum left open6 (11.5)3 (15.8)3 (9.1)0.46 Hypoxia8 (15.4)3 (15.8)5 (15.2)0.96 Prolonged mechanical ventilatory support (>72 h)18 (34.6)7 (36.8)11 (33.3)0.80 Wound infection4 (7.8)0 (0)4 (12.1)0.11 Pleural effusion11 (21.2)4 (21.1)7 (21.2)>0.99 Diaphragmatic palsy4 (7.7)1 (5.3)3 (9.1)0.25 Bleeding11 (21.2)5 (26.3)6 (18.2)0.48 IVH/clot3 (5.8)3 (15.8)0 (0)0.02IVH, intraventricular hemorrhage; LAI, left atrial isomerism; n, number; RAI, right atrial isomerism.
Tachy/bradyarrhythmia
At least 27 patients had documented nonsinus atrial rhythm during their follow-up (equally split between both groups), representing around 50% of the cohort. In terms of tachyarrhythmia, 8 patients had documented sustained SVT that required medical management during their follow-up (approximately 15% of each group), and 1 patient had evidence of twin AV nodes. On the other hand, 2 patients had postoperative HB, and another patient had congenital HB requiring pacemaker insertion; otherwise, 1 patient had 2:1 conduction postoperatively without the need for permanent pacing. As previously mentioned, all patients with bradyarrhythmia had LAI-type HS.
Pulmonary venous anomalies
Twelve patients (23%) had anomalous pulmonary venous anomalies (Table 1): supracardiac (nonobstructive) in 3, intracardiac (nonobstructive) in 7, and infracardiac (obstructive) in 2. TAPVD was present in 9 patients, and the remaining 3 patients had partial anomalous pulmonary venous return. All patients with partial anomalous pulmonary venous return were associated with LAI, and all patients with LAI-TAPVD combined had BV physiology.
Mortality
Table 3 describes all the deceased patient anatomies, palliative or corrective procedures performed, morbidities, timing, and cause of death. All deceased patients were palliated, and none had complete repair. All but one died while being admitted following a specific procedure.Table 3. Diagnosis, surgical procedures, morbidities, and causes of deathsubjectDiagnosisOperationMajor morbiditymortalityCause of death1RAI, unbalanced AVSD, TAPVD to LSVC, b/l SVC, PS, malposed GABTS → vertical vein stent → TAPVD repair, BDG (left), ligation of RSVC and MPA → Redo TAPVD repair → fenestrated Fontan, AVV annuloplastyDextrocardia, brain infarction, convulsions, tracheostomy, cardiac arrest, open chestHospital death (immediate postoperative)Desaturation, hypotension, VF2LAI, HLHS, interrupted IVCNorwood/BTSSevere bleedingHospital death (immediate postoperative)Mediastinitis, sepsis3RAI, HLHS variant, AS, LSVC to common atrium, HAANorwood/BTSDextrocardia, high coronaries takeoffIntraoperative deathDecreased CO, hypoxia4RAI, AVSD (balanced), PA, infracardiac obstructive TAPVDTAPVD repair, BTSBleeding and cardiac arrest, open sternumHospital deathHypoxia, sepsis5LAI, unbalanced AVSD, interrupted IVC, RAA with aberrant subclavian, congenital complete HBTemporary PM → permanent PM, PA banding → PA band tightening → Kawashima procedureDextrocardia, sternal wound gapping/oozing. Pulmonary hypertensive crisisHospital deathHypoxia6RAI, DORV, PS, AVSD, b/l SVC, interrupted IVC, TAPVD to RABDG → nonfenestrated Fontan → AVV repairModerate—severe AVVR, cardiac arrestHospital deathFontan failure (generalized edema with poor function)7LAI, unbalanced AVSD, PS, b/l SVCBTS → BDGDextrocardia, SVTHospital deathDied overseas8LAI, MAPCAS, VSD, PA, b/l SVCBTS and PA plastyHospital deathSepsis and multiorgan failure9RAI, unbalanced AVSD, PABTS35 weeks GAHospital deathShunt obstruction10RAI, AVSD, PA, hypoplastic branch PAs, MAPCAS, b/l SVC, RAAPOTTS shuntDextrocardiaLate deathNA11RAI, unbalanced AVSD, PABTSHospital deathAspiration pneumonia12RAI, unbalanced AVSDPA banding → BDG → nonfenestrated Fontan → Fontan + RPA stentingDextrocardia, protein losing enteropathyHospital deathDepressed function, cardiac arrest13LAI, unbalanced AVSD, PA, b/l SVCBTSSVTHospital deathSepsis, pneumothorax, hypoxia, bradycardia, hypotension, acidosis14LAI, CAVB, partial AVSDPMAnasarca, candidemiaHospital deathSepsis, heart failureAS, aortic stenosis; AVSD, atrioventricular septal defect; AVV, atrioventricular valve; AVVR, AVV regurgitation; b/l SVC, bilateral superior vena cava; BDG, bidirectional Glenn; BTS, Blalock-Taussig shunt; CAVB, complete atrioventricular block; CO, cardiac output; DORV, double outlet right ventricle; GA, great arteries; HAA, hypoplastic aortic arch; HB, heart block; HLHS, hypoplastic left heart syndrome; IVC, inferior vena cava; LAI, left atrial isomerism; LSVC, left superior vena cava; MAPCAS, major aortopulmonary collateral arteries; MPA, main pulmonary artery; NA, not available; PA, pulmonary atresia; PM, pacemaker; PS, pulmonary valve stenosis; RAA, right aortic arch; RAI, right atrial isomerism; RPA, right pulmonary artery; RSVC, right superior vena cava; SVT, supraventricular tachycardia; TAPVD, total anomalous pulmonary venous drainage; VF, ventricular fibrillation; VSD, ventricular septal defect.
Relevant factors associated with mortality that were considered included UV or BV physiology, prematurity, low weight/age at surgery, presence of AV valve regurgitation, anomalous pulmonary veins drainage, and type of atrial isomerism. Table 4 demonstrates univariate survival analysis of the collected patient data with HR of 4.12 for patients with operated age < 20 days compared to operated age > 20 days (P = 0.019) [Fig. 1]. Figure 2 and Figure 3 shows survival rates for RAI vs LAI and survival analysis for the entire cohort.Table 4. Factors associated with mortalityOutcomeUnivariate analysisHR[95% CI]POperation weight (kg) <2.50.59[0.75-4.59]0.612 >2.51.00[Reference]Operation age (d) <204.12[1.26-13.41]0.019 >201.00[Reference]Gestational age Preterm0.77[0.16-3.62]0.740 Full term1.00[Reference]Birth (kg)Weight >2.53.486[0.436-27.873]0.239 <2.51.00[Reference]Diagnosis RAI2.758[0.946-8.043]0.063 LAI1.00[Reference]Procedure SV1.43[0.40-5.14]0.581 BV1.00[Reference]AVVR Significant1.076[0.24-4.86]0.92 Nonsignificant1.00[Reference]TAPVD Present0.87[0.19-3.91]0.85 Absent1.00[Reference]AVVR, atrioventricular valve regurgitation; BV, biventricular; CI, confidence interval; HR, hazard ratio; LAI, left atrial isomerism; RAI, right atrial isomerism; SV, single ventricle; TAPVD, total anomalous pulmonary venous drainage.Figure 1. Kaplan-Meier curve survival analysis for patients undergoing surgery before 20 days of age vs beyond 20 days of age.Figure 2. Kaplan-Meier curve survival analysis for patients with RAI vs LAI. LAI, left atrial isomerism; RAI, right atrial isomerism.Figure 3. Kaplan-Meier curve survival analysis for the entire cohort.
Discussion
The incidence for HS in the country was similar to previous publications with a reported incidence of around 1%-3% among patients with congenital heart disease.1^,^5 Specifically, LAI was more prevalent than RAI, similar to other reports from the United States and Europe, but unlike reports from East Asia.8 Herein, we describe a single center’s most recent experience, aiming to review the surgical results, midterm outcomes, and assess RFs for mortality in patients with HS.
The main observation within this cohort is the high mortality rate. Nevertheless, published mortality rates in the literature may reach up to 40% depending on duration of follow-up, surgical era, institutional expertise, and complexity of the cohort.1, 2, 3, 4, 5^,^11^,^13 However, none of the mortalities occurred among the BV group, suggesting that mortality is primarily due to the complex subset of SV patients with HS. Undoubtedly, HS is frequently associated with UV physiology.1^,^3, 4, 5, 6^,^11^,^13 Furthermore, there is a high rate of associated pulmonary venous anomalies complicating patients’ surgical procedures.3^,^5^,^13 Specifically, to this cohort, the low rate of fetal diagnosis, birth at noncardiac centers, care provided at tertiary cardiac center and not multispecialty children’s hospital, and the unavailability of cardiac transplant option might have contributed to the increased mortality. RAI was associated with greater mortality due to the highly associated SV physiology (95%) and the higher incidence of associated pulmonary venous anomalies (37%), 2 of which had the malignant combination of obstruction and UV physiology.11^,^14 Similarly, globally the mortality of HS patients with congenital heart disease remains high, despite improvement in the current era.1^,^2^,^6 This improvement is likely due to the advances in the diagnostic tools, cardiac surgical techniques, and the intensive care milieu.2
The highest complication rate was prolonged intubation times. Understandably, this could be partly related to the associated ciliary dyskinesia in patients with HS2^,^4^,^5^,^11^,^13 and the accompanying reactive pulmonary vasculature, in addition to the intrinsically smaller pulmonary veins at least among the patients with RAI.6^,^11 Moreover, the frequent association with anomalous pulmonary venous anomalies (23%) in patients with HS may also prolong the intubation times.1^,^3^,^4^,^6^,^11^,^13
Independent RFs included lower operation age (Table 4), which is similar to other reports.2, 3, 4, 5 Other RFs analyzed did not reach statistical significance, likely secondary to the low number of studied patients. Specifically, the type of atrial isomerism, specifically RAI, appeared to approach significance on univariate analysis. Indeed, RAI is a surrogate for more complex cardiac anatomies (Table 2) with UV physiology and hence is associated with poorer prognosis.1^,^2^,^6
HB and LAI association is further seen in this cohort, especially when associated with abnormal AV septation.7^,^8^,^15, 16, 17, 18 Indeed, 3 of the 4 patients with HB in this cohort had abnormal septation. None of the RAI had HB similar to other report,15 perhaps related to the more frequent incidence of twin AV nodes among patients with RAI.8^,^15 An absent sinus node frequently seen in patients with LAI and bilateral sinus nodes commonly seen in patients with RAI explain the high incidence of non-right sinus rhythm observed in this cohort.8, 9, 10^,^18^,^19
Finally, patients frequently developed SVT during the study period, mostly among the subset of UV patients, similar to the largest report available20 but unlike other reports.7 It is well known that patients with HS, especially RAI type, have twin AV nodes and, hence, are predisposed to nodal to nodal reentry tachycardia.7^,^8^,^15^,^18^,^20^,^21
Limitations
Limitations of this study included the small sample size. The small number of subjects limits statistical power and the feasibility of subgroup analysis in the cohort of the current study. The retrospective nature of the study limits the study with the risk for selection bias. Causation assessment was not possible. The usual limitations of a single-center retrospective study, such as interobserver variability for clinical and echocardiographic evaluations performed by different physicians, apply to this data analysis.
Conclusion
Managing HS patients with UV physiology still remains a challenge in this day and age. RFs for mortality included RAI and lower initial operation age. Postoperatively, prolonged intubation times were the commonest complications observed. These data may assist with risk stratification and patient counseling.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mc Govern E.Kelleher E.Potts J.E.Predictors of poor outcome among children with heterotaxy syndrome: a retrospective review Open Heart 32016 e 00032810.1136/openhrt-2015-000328 PMC 507356027843561 · doi ↗ · pubmed ↗
- 2Loomba R.S.Nijhawan K.Anderson R.Impact of era, type of isomerism, and ventricular morphology on survival in heterotaxy: implications for therapeutic management World J Pediatr Congenit Heart Surg 7201654622671499510.1177/2150135115601831 · doi ↗ · pubmed ↗
- 3Banka P.Adar A.Schaetzle B.Changes in prognosis of heterotaxy syndrome over time Pediatrics 1462020 e 2019334510.1542/peds.2019-334532647064 · doi ↗ · pubmed ↗
- 4Alsoufi B.Mc Cracken C.Schlosser B.Outcomes of multistage palliation of infants with functional single ventricle and heterotaxy syndrome J Thorac Cardiovasc Surg 151201613691377.e 22708561810.1016/j.jtcvs.2016.01.054 · doi ↗ · pubmed ↗
- 5Brueckner M.Heterotaxia, congenital heart disease, and primary ciliary dyskinesia Circulation 1152007279327951754873910.1161/CIRCULATIONAHA.107.699256 · doi ↗ · pubmed ↗
- 6Ota N.Fujimoto Y.Murata M.Improving outcomes of the surgical management of right atrial isomerism Ann Thorac Surg 9320128328392211279510.1016/j.athoracsur.2011.05.110 · doi ↗ · pubmed ↗
- 7Wu M.-H.Wang J.K.Lin J.L.Supraventricular tachycardia in patients with right atrial isomerism J Am Coll Cardiol 321998773779974152610.1016/s 0735-1097(98)00307-6 · doi ↗ · pubmed ↗
- 8Wu M.-H.Wang J.K.Chiu S.N.Twin atrioventricular nodes, arrhythmias, and survival in pediatric and adult patients with heterotaxy syndrome Heart Rhythm 1820216056123332119810.1016/j.hrthm.2020.12.012 · doi ↗ · pubmed ↗