Vitamin D Level in Blood Serum and Its Connection with Helicobacter pylori Infection: A Systematic Review
Yasmine A Mohammed, Mariam R Elkhayat, Osama M El-Asheer, Medhat A Saleh, Nermeen A Gendy, Aml E Metwally, Amira T Anees, Mervat A Melek, Usama M Hasan, Doaa M Genena

TL;DR
This study reviews evidence suggesting a link between low vitamin D levels and Helicobacter pylori infection, but causality remains unproven.
Contribution
The study systematically reviews the association between vitamin D levels and H. pylori infection, highlighting genetic factors involved.
Findings
H. pylori-positive individuals tend to have lower vitamin D levels than those who are negative.
VDR gene polymorphisms and TLR4 gene variants are significantly associated with H. pylori infection and vitamin D status.
The study identifies a potential role for vitamin D in gastric immunity and as a modifiable risk factor.
Abstract
Helicobacter pylori (H. pylori) is widely recognized for its role in gastric pathologies, including ulcerative disease and malignant transformation of the gastric mucosa. Lower serum concentrations of 25-hydroxyvitamin D may impair immune responses, potentially influencing colonization dynamics and persistence of H. pylori infection. A systematic review was conducted to critically evaluate the current evidence on the association between serum vitamin D levels and H. pylori infection. PubMed, Scopus, Cochrane Library, and Web of Science databases were comprehensively searched for relevant articles from their inception until May 28, 2025. Twenty observational studies, including 167,903 cases, were included in the review. Our results suggest a possible link between vitamin D deficiency and the risk of H. pylori infection, as the H. pylori-positive population was more likely to have lower…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
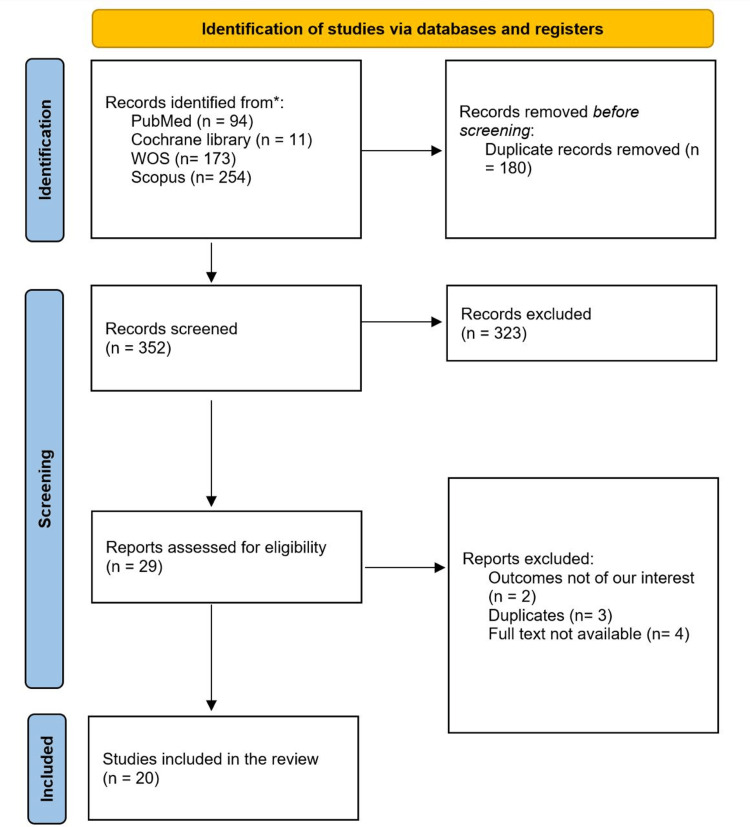 Figure 1
Figure 1| ID | Study design | Study groups | Number | Age in years, M ±SD | Male sex, N (%) | Other coexisting conditions, N (%) | BMI | Diagnostic method | Conculosion | |||||
| M ±SD | N (%) | |||||||||||||
| Renal disease | Liver disease | < 18.5 | 18.5–24.9 | 25–29.9 | ≥ 30 | |||||||||
| Bahsi et al., 2020 [ | Cross-sectional |
| 32 | 75.48 ±5.85 | 59 (58.4) | NA | NA | 27.76 ±5.31 | NA | NA | NA | NA | Histopathological examination of the gastric biopsy | Patients with sarcopenia and |
|
| 69 | NA | NA | NA | NA | NA | NA | |||||||
| Agin et al., 2021 [ | Prospective cohort |
| 199 | 13.47 ±4.49 | 197 (68) | 0 | 0 | NA | NA | NA | NA | NA | Histopathological examination of the gastric biopsy | There is a significant association between low serum vitamin D levels and the development of peptic ulcers. No significant association was detected between serum vitamin D levels and |
|
| 92 | 0 | 0 | NA | NA | NA | NA | NA | ||||||
| Rysbekov et al., 2024 [ | Prospective cohort |
| 63 | 13 ±3.03 | 20 (30.8) | NA | NA | NA | NA | NA | NA | NA | Histopathological examination of the gastric biopsy and instant urease test | The study indicated that lower vitamin D levels (<20 μg/L) could be a predisposing factor for |
|
| 65 | 12 ±3.03 | 29 (46.0) | NA | NA | NA | NA | NA | NA | NA | ||||
| Kuang et al., 2022 [ | Cross-sectional |
| 2100 | NA | 1131 (53.85) | NA | NA | NA | NA | NA | NA | NA | Detection of H. pylori CagA antibody | The study stated a nonsignificant association between serum vitamin D levels and |
|
| 1412 | NA | 747 (52.9) | NA | NA | NA | NA | NA | NA | NA | ||||
| Habbash et al., 2022 [ | Retrospective cross-sectional |
| 111 | NA | 48 (55.8) | NA | NA | NA | NA | NA | NA | NA | Either upper GI tract endoscopy biopsy examination, urea breath testing, or both | There is a significant association between vitamin D deficiency and the development of |
|
| 89 | NA | 38 (44.2) | NA | NA | NA | NA | NA | NA | NA | ||||
| Liu et al., 2023 [ | Retrospective cohort |
| 415 | 47.3 ±12.8 | 194 (46.75) | 0 | 0 | NA | 0 | 289 (69.64) | 112 (26.99) | 14 (3.37) | 13 C-urea breath test | The study indicated that lower Vitamin D levels could be a risk factor for |
|
| 257 | 48.5 ±10.1 | 127 (49.42) | 0 | 0 | NA | 0 | 168 (65.37) | 70 (27.24) | 19 (7.39) | ||||
| Askar et al., 2022 [ | Cross-sectional |
| 644 | NA | 334 (51.86) | NA | NA | NA | NA | NA | NA | NA | H.pylori stool antigen test | There is a significant relationship between vitamin D deficiency and the development of |
|
| 956 | NA | 586 (61.29) | NA | NA | NA | NA | NA | NA | NA | ||||
| Assaad et al., 2019 [ | Cross-sectional |
| 225 | 39.28 ±13.9 | 88 (39.1) | NA | NA | NA | 0 | 109 (48.44) | 116 (51.56) | Histopathological examination of the gastric biopsy | SNPs in TLR4 were inversely associated with vitamin D serum levels, which were negatively related to | |
|
| 235 | 41.86 ±14.26 | 80 (34) | NA | NA | NA | 0 | 128 (54.47) | 107(45.53) | |||||
| Shafrir et al., 2021 [ | Retrospective cohort |
| 75640 | 40.95 ±14.72 | 38576 (51) | NA | 2663 (3.52) | 26.89 ±5.64 | NA | NA | NA | NA | 90% Urea breath test (UBT) and the rest done by H. pylori stool antigen tests | The study indicated that lower vitamin D levels are associated with |
|
| 74,843 | 42.15 ±16.65 | 37422 (50) | NA | 3465 (4.63) | 26.45 ±5.62 | NA | NA | NA | NA | ||||
| Korkmaz et al., 2015 [ | Prospective cohort |
| 43 | 30.58±8.79 | 23 (53.49) | 0 | 0 | 25.2±4.2 | NA | NA | NA | NA | Histopathological examination of gastric biopsy and rapid urease test | The incidence of |
| Surmeli et al., 2018 [ | Cross-sectional study |
| 43 | 74.27 ±6.06 | 11 (25.6) | 7 (16.3) | NA | NA | 0 | 14 (32.6) | 18 (41.9) | 8 (18.6) | Histopathological examination of the gastric biopsy | The study indicated that lower Vitamin D levels could be a risk factor for |
|
| 211 | 77.53 ±7.76 | 91 (43.1) | 52 (24.6) | NA | NA | 2 (1) | 86 (40.8) | 79 (37.4) | 24 (11.4) | ||||
| Chen et al., 2016 [ | Survey | Metabolic syndrome (+)a | 557 | 59.9±12.2 | 220 (39.49) | NA | NA | 27.3 ±3.3 | NA | NA | NA | NA | Urea breath test | The study found no significant difference regarding serum vitamin D levels in patients with and without |
| Metabolic syndrome (-)b | 1556 | 55.1 ±13.1 | 572 (36.76) | NA | NA | 23.8 ±3.3 | NA | NA | NA | NA | ||||
| Martins et al., 2018 [ | Cross-sectional |
| 117 | 51.38 ±15.22 | NA | NA | NA | NA | NA | NA | NA | NA | Histopathological examination of gastric biopsy | BsmI polymorphism could have a possible association with |
|
| 91 | 55.18 ±14.98 | NA | NA | NA | NA | NA | NA | NA | NA | ||||
| Mihalache et al., 2016 [ | Cross-sectional |
| 47 | NA | NA | 0 | NA | 44.04 ±5.992 | 0 | 0 | 0 | 47 (100) | Histopathological examination of gastric biopsy | The level of vitamin D was higher in |
|
| 46 | NA | NA | 0 | NA | 44.27 ±6.927 | 0 | 0 | 0 | 46 (100) | ||||
| Gao et al., 2020 [ | Cross-sectional |
| 2113 | 1.0475 ±0.693 | 1,202 (30.9) | 0 | 0 | NA | NA | NA | NA | NA | H. pylori serum antibody test | There is a significant association between vitamin D deficiency and the development of |
|
| 4783 | 1.09 ±0.785 | 2685 (69.1) | 0 | 0 | NA | NA | NA | NA | NA | ||||
| Mohamed et al., 2020 [ | Cross-sectional |
| 127 | 39.47 ±8.77 | NA | NA | NA | NA | NA | NA | NA | NA | Histopathological examination of the gastric biopsy | The FokI and Apal VDR polymorphism could have a possible association with |
|
| 97 | 40.14 ±8.02 | NA | NA | NA | NA | NA | NA | NA | NA | ||||
| Nasri et al., 2007 [ | Cross-sectional |
| 36 | 47 ±17 | 21 (58.33) | 36 (100) | NA | 22 ±4.4 | NA | NA | NA | NA | Serum H. pylori-specific IgG antibody | There is a significant association between serum vitamin D levels and the development of |
| Han et al., 2019 [ | Prospective cohort |
| 496 | 47.1 ±12.6 | 236 (47.58) | NA | NA | NA | NA | NA | NA | NA | Urea breath test | The study stated that serum vitamin D levels may affect |
|
| 257 | 48.1 ±10.2 | 127 (49.42) | NA | NA | NA | NA | NA | NA | NA | ||||
| Gerig et al., 2013 [ | Retrospective cohort |
| 85 | 42.3 ±10.0 | 21 (24.71) | NA | NA | 45.2 ±6.0 | NA | NA | NA | NA | Histopathological examination of the gastric biopsy | The study stated no significant difference in serum vitamin D levels between the two groups |
|
| 319 | 40.9 ±11.8 | 85 (26.65) | NA | NA | 45.9 ±8.8 | NA | NA | NA | NA | ||||
| Sorokman et al., 2020 [ | Retrospective cohort |
| 86 | NA | NA | 0 | NA | NA | NA | NA | NA | NA | Histopathological examination of the gastric biopsy | The study stated significantly lower serum vitamin D levels in patients with |
| ID | Study groups | Number | Serum vitamin D level, M ±SD | Serum vitamin D level < 20 μg/L | Serum vitamin D level ≥ 20 μg/L |
| Bahsi et al., 2020 [ |
| 32 | 24.31 ± 13.77 | 21 (65.6) | 11 (34.38) |
|
| 69 | 29.4 ± 14.59 | 32 (46.38) | 37 (53.6) | |
| Agin et al., 2021 [ |
| 141 | NA | 85 (60.3) | 56 (39.7) |
|
| 150 | 36 (24) | 114 (76) | ||
| Rysbekov et al., 2024 [ |
| 63 | 17.57 ± 9.41 | 35 (55.55) | 28 (44.44) |
|
| 65 | 14.63 ± 6.9 | 51 (78.46) | 14 (21.5) | |
| Habbash et al., 2022 [ |
| 61 | NA | 49 (80.33) | 12 (19.67) |
|
| 56 | 28 (50) | 28 (50) | ||
| Liu et al., 2023 [ |
| 415 | 16.7 ± 6.6 | 311 (74.94) | 104 (25.06) |
|
| 257 | 19.2 ± 8.0 | 157 (61.09) | 100 (38.9) | |
| Askar et al., 2022 [ |
| 644 | NA | 282 (43.79) | 362 (56.2) |
|
| 956 | 311 (32.53) | 645 (67.47) | ||
| Assaad et al., 2019 [ |
| 225 | 18.04 ± 7.16 | 56 (24.89) | 148 (65.78) |
|
| 235 | 30.74 ± 15.66 | 109 (46.39) | 119 (50.64) | |
| Shafrir et al., 2021 [ |
| 75,640 | 18.6 ± 9.8 | NA | NA |
|
| 74,843 | 20.1 ± 9.4 | |||
| Korkmaz et al., 2015 [ |
| 43 | 14.7 ± 8.5 | NA | NA |
| Surmeli et al., 2018 [ |
| 43 | 10.63 ± 8.67 | 37 (86.04) | 6 (13.9) |
|
| 211 | 14.6 ± 11.35 | 142 (67.3) | 69 (32.7) | |
| Mihalache et al., 2016 [ |
| 47 | 17.25 ± 10.92 | NA | NA |
|
| 46 | 14.7 ± 7.72 | |||
| Gao et al., 2020 [ |
| 2,113 | 25.2 ± 5.27 | 437 (20.68) | 1676 (79.32) |
|
| 4,783 | 25.93 ± 4.52 | 578 (12.08) | 4205 (87.92) | |
| Nasri et al., 2007 [ |
| 36 | 10.5 ± 18.7 | NA | NA |
| Han et al., 2019 [ |
| 496 | 17 ± 6.9 | NA | NA |
|
| 257 | 19.2 ± 8 | |||
| Gerig et al., 2013 [ |
| 81 | 49 ± 30 | NA | NA |
|
| 315 | 52 ± 29 | |||
| Sorokman et al., 2020 [ |
| 86 | 15.4 ± 1.1 | 60 (69.77) | 26 (30.23) |
|
| 42 | 25.3 ± 1.4 | 15 (35.7) | 27 (64.29) |
| Study ID | Selection | Comparability | Outcome | Total score |
| Liu et al., 2023 [ | ★★★☆ | ★☆ | ★★★ | 7 |
| Agin et al., 2021 [ | ★★★☆ | ★☆ | ★★★ | 7 |
| Rysbekov et al., 2024 [ | ★★★☆ | ☆☆ | ★★★ | 6 |
| Shafrir et al., 2021 [ | ★★★☆ | ★☆ | ★★★ | 7 |
| Korkmaz et al., 2015 [ | ★☆★☆ | ☆☆ | ★★☆ | 4 |
| Han et al. 2019 [ | ★★★☆ | ★☆ | ★★★ | 7 |
| Gerig et al., 2013 [ | ☆★★☆ | ★★ | ★★★ | 7 |
| Sorokman et al., 2020 [ | ★★★☆ | ☆☆ | ★★★ | 6 |
| Askar et al., 2022 [ | ★☆★★★ | ☆☆ | ★★☆ | 6 |
| Assaad et al., 2019 [ | ★☆★★★ | ★★ | ★★★ | 9 |
| Bahsi et al., 2020 [ | ★☆★★★ | ☆☆ | ★★★ | 7 |
| Kuang et al., 2022 [ | ★★★★★ | ★☆ | ★★★ | 9 |
| Habbash et al., 2022 [ | ★★☆★★ | ★★ | ★★★ | 9 |
| Surmeli et al., 2018 [ | ★☆★★★ | ★☆ | ★★★ | 8 |
| Chen et al., 2016 [ | ★★★★★ | ☆☆ | ★★★ | 8 |
| Martins et al. 2018 [ | ★☆★★★ | ☆☆ | ★★★ | 7 |
| Mihalache et al., 2016 [ | ☆☆★★★ | ★★ | ★★★ | 8 |
| Gao et al., 2020 [ | ★★★★★ | ★☆ | ★★★ | 9 |
| Mohamed et al., 2020 [ | ★☆★★★ | ☆☆ | ★★★ | 7 |
| Nasri et al., 2007 [ | ☆☆★★★ | ☆☆ | ★★★ | 6 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVitamin D Research Studies · Helicobacter pylori-related gastroenterology studies · Gut microbiota and health
Introduction and background
Helicobacter pylori (H. pylori) is a Gram-negative, spiral-shaped bacterium that colonizes the human gastric mucosa and affects over half of the global population [1]. It is recognized as a Group 1 carcinogen by the World Health Organization. It is strongly implicated in the pathogenesis of chronic gastritis, peptic ulcer disease, mucosa-associated lymphoid tissue lymphoma, and gastric adenocarcinoma [2]. The burden of H. pylori infection disproportionately affects populations in low- and middle-income countries, where socioeconomic factors such as overcrowding, poor sanitation, and limited access to healthcare contribute to increased transmission and reinfection rates [3,4].
Vitamin D plays a vital role in innate and adaptive immunity, influencing monocyte and cytokine regulation and macrophage differentiation, and regulating antimicrobial peptide expression such as cathelicidin and β-defensin [5]. Moreover, its receptor, the vitamin D receptor (VDR), is expressed in immune cells, gastric epithelium, and hepatic tissue, suggesting its involvement in mucosal defence and inflammatory modulation [6-8]. The immunological relevance of vitamin D in infectious disease contexts has gained traction, with emerging evidence suggesting a potential inverse relationship between serum 25-hydroxyvitamin D levels and increased susceptibility to bacterial infections, including H. pylori, reduced eradication success, and enhanced inflammatory responses [5,9].
Recent epidemiological and molecular studies have substantiated this link. A retrospective study in Lebanese adults demonstrated significantly lower serum 25(OH)D levels in H. pylori-infected individuals compared to uninfected controls (p < .001), with deficiency strongly associated with infection risk [10]. Adding to this narrative, a recent meta-analysis synthesized findings from 12 observational studies encompassing diverse geographic regions. The pooled standardized mean difference (SMD) indicated that H. pylori-positive individuals had serum vitamin D levels 0.76 ng/ml lower than uninfected controls, while patients with successful eradication exhibited levels 1.53 ng/ml higher than those with eradication failure. Despite heterogeneity in study design and population characteristics, sensitivity analyses and publication bias assessments reinforced the robustness of these estimates [11]. Collectively, these findings suggest a multifactorial interplay between vitamin D metabolism, genetic predisposition, and host immune responses in determining the susceptibility and clinical manifestations of H. pylori infection. Elucidating these relationships may enhance risk stratification and inform novel adjunctive strategies in H. pylori management. Existing studies vary in inclusion criteria, vitamin D thresholds, and eradication protocols, necessitating a more rigorous synthesis. Furthermore, mechanistic pathways, such as VDR-mediated transcriptional regulation, autophagic clearance of H. pylori, and vitamin D's effect on gastric mucosal integrity, remain underexplored in clinical contexts.
In light of these gaps, this systematic review aims to critically evaluate the current evidence on the association between serum vitamin D levels and H. pylori infection. By integrating observational data, mechanistic insights, and geographic variability, we seek to determine whether vitamin D serves as a modifiable biomarker or adjunctive therapeutic target in the management of H. pylori. This investigation holds relevance not only for gastroenterology but also for public health strategies in regions burdened by both hypovitaminosis D and high H. pylori prevalence.
Review
Methods
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist guidelines [12].
Literature Search
PubMed, Scopus, Cochrane Library, and Web of Science databases were comprehensively searched for relevant articles from inception until May 28, 2025. We used a combination of the following terms: “Helicobacter pylori” OR “H. pylori” AND “Vitamin D” OR “Vit. D”.
Eligibility Criteria and Procedure for Study Selection
Our study question was, “Is there any connection between H. pylori infection and vitamin D levels in blood serum?” According to PECOS, P (population) refers to the general population with no restriction on age, sex, or race; E (exposure) refers to H. pylori infection; C (comparator) refers to individuals with no H. pylori infection; O (outcome) refers to serum vitamin D levels; and S (study design) refers to observational studies (cohort, case-control, and cross-sectional). There were no restrictions regarding the publication date or country. The exclusion criteria included any editorial, case reports, case series, reviews, non-English studies, and studies with abstracts only available.
The Rayyan website (http://rayyan.qcri.org) [13] was used to combine all the retrieved records from the databases, which are free online, and throughout the entire screening process, which consisted of two steps: title and abstract screening, followed by full-text screening. At least two authors did each step, and blinding was maintained throughout the process using the blinding tool on the Rayyan website. Any disagreements were solved by discussion with an experienced author.
Data Extraction
We used a pre-formed Microsoft Excel (Microsoft Corporation, Redmond, WA) spreadsheet to extract the population baseline characteristics, study outcomes, summary of the studies, and data for quality assessment. Data for baseline characteristics and study summary included study ID, study design, study groups, and number in each group, age, male sex, BMI, alcohol and smoking status, presence of other comorbidities, the method used to diagnose H. pylori infection, and the conclusion of each study. Outcomes included serum vitamin D levels and genetic polymorphism.
Quality Assessment
The Newcastle-Ottawa Scale (NOS) was used to assess the risk of bias of the included studies [14]. It consists of three main domains. The first domain assesses participant selection (a maximum of five stars for cross-sectional and four for cohort studies), the second evaluates the comparability between the different study groups (a maximum of two stars), and the last domain assesses the outcomes and statistical analysis (a maximum of three stars). Hence, the maximum score was 10 stars for cross-sectional and nine for cohort studies. The studies were judged to have a low risk (high quality) if the score was greater than seven stars, a moderate risk (medium quality) if the score was between four and seven stars, and to have a high risk of bias (low quality) if the score was less than four stars.
Results
Search Results
The flow diagram of the screening process and studies' inclusion is shown in Figure 1. We retrieved 532 results from different databases; 180 were excluded as duplicates. Out of the remaining 352 results, 323 were excluded for not meeting the inclusion criteria, leaving 29 studies that went through the full-text screening phase. After excluding two studies for not meeting our inclusion criteria, three duplicates, and four studies because of the unavailability of their full texts, 20 studies were included in our systematic review.
The PRISMA figure showing the steps to choose the studies for systematic reviewPRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; WOS: Web of Science
Study Characteristics and Baseline Data
Out of the 20 [10,15-33] included studies in our systematic review, nine were observational cohort studies (four prospective and five retrospective studies), and 11 were cross-sectional studies. The included studies addressed about 167,903 cases, with a male percentage of 50.6% (84,970 cases). The mean age of the included population ranged between 1.04 (0.69) years old and 75.48 (5.85) years old. The diagnostic tool for H. pylori infection varied between the studies, including histopathological examination of gastric biopsy (nine studies), which is the most common tool. Other diagnostic methods included the urea breath test, serum antibodies, or stool examination. Other coexisting conditions and baseline characteristics are represented in Table 1.
Outcomes
Serum vitamin D level: Seven studies found that the serum vitamin D level was statistically significantly lower in cases of positive *H. pylori *infection (P < 0.05) [10,20,22,24,28,31,33]. Only one study found a statistically significantly higher level of serum vitamin D in the positive H. pylori infection cases compared to the negative cases (P < 0.05) [17]. In the study by Chen et al. (2016), the study evaluated the associations between H. pylori infection, serum vitamin D level, and metabolic syndrome (MS). The study stated a significant association between vitamin D deficiency and MS (p < 0.05). However, they found no significant association between serum vitamin D and H. pylori infection (p > 0.05) [25]. In the study by Agin et al. (2021), they evaluated serum vitamin D levels in patients with peptic ulcers and patients without peptic ulcers, and they found that serum vitamin D levels were higher in people without peptic ulcers. However, H. pylori infection was more prevalent in patients with vitamin D deficiency [16]. Kuang et al. (2022) [18] evaluated the relationship between vitamin D and H. pylori CagA. The study found no significant association between serum vitamin D and CagA (p > 0.05); therefore, H. pylori infection. Moreover, Gerig et al. (2013) stated no statistically significant correlation between the *H. pylori *infection and serum vitamin D level [32]. This finding was also reported in the study by Mihalache et al. (2016). The study was conducted on obese patients with and without H. pylori and found no significant correlation between H. pylori infection and serum vitamin D level [27]. In the study conducted by Bahsi et al. in 2020 on sarcopenic patients, the study found that H. pylori in sarcopenic patients may lead to serum vitamin D deficiency ( Table 2) [10, 15-17, 19-24, 27-28, 30-33].
Table 2: Serum vitamin D level in the included populationM ±SD: mean ±standard deviation; vitamin D level <20 μg/L is considered insufficient or inadequate for most people for bone health and overall health.NA: not available
Association between H. pylori and the level of vitamin D, either < or ≥ 20 ug/L: Regarding the association between H. pylori and vitamin D deficiency, seven studies showed that the frequency of vitamin D deficiency (<20 ug/L) was higher in the H. pylori-positive cases than in the negative cases [16,19-21,24,28,33]. Also, Bahsi et al. in 2020 [15] reported that *H. pylori *positivity increased the odds of vitamin D deficiency in sarcopenic patients. However, in two studies, the decline of serum vitamin D below 20 ug/L was higher in the negative cases of H. pylori compared to the positive cases [10,17]. In cases where the serum vitamin D level was ≥ 20 μg/L, eight studies reported that the level of serum vitamin D ≥ 20 μg/L was more common in negative H. pylori cases [15,16,19-21,24,28,33]. Only two studies reported that the association of the level of serum vitamin ≥ 20 μg/L was more common in positive cases of *H. pylori *[10,17]. However, Chen et al. (2016) found no significant difference regarding vitamin D serum levels in patients with and without H. pylori infection (Table 2) [25].
Genetic polymorphism and H. pylori infection: On assessing the relation between vitamin D genetic polymorphisms and H. pylori infection, three studies reported a significant association [10,26,29]. The studies collectively highlight that polymorphisms in the VDR gene, particularly rs2228570 (FokI), rs7975232 (ApaI), and rs1544410 (BsmI), as well as the TLR4 gene (rs4986790 and rs4986791), are significantly associated with H. pylori infection and vitamin D status. In Assad et al. (2019), the study reported that the TLR4 polymorphisms rs4986790G>A and rs4986791T>C were linked to vitamin D levels, which in turn influenced susceptibility to H. pylori infection, suggesting these SNPs may exert an indirect effect. Notably, individuals infected with *H. pylori *exhibited vitamin D deficiency, and their white blood cells expressed TLR4 at levels three times lower than those of their uninfected counterparts [10]. In the study by Martins et al. (2018), FokI, ApaI, and TaqI polymorphisms of the VDR gene did not show any difference between H. pylori-positive and H. pylori-negative groups. However, rs1544410 (BsmI) was the only VDR SNP that showed a significant association with H. pylori-positive individuals [26]. In the study by Mohamed et al. (2020), statistically significant differences were observed between H. pylori-infected and non-infected groups in the distribution of VDR gene polymorphisms. Regarding the rs7975232 variant, the CC genotype was more noticed among H. pylori-negative individuals, whereas the AC and AA genotypes were more common in the infected group. Similarly, for the rs2228570 variant, the TT genotype predominated in the non-infected group, while CT and CC genotypes were more frequently seen in those infected. The A allele of rs7975232 was significantly associated with *H. pylori *infection, in contrast to the C allele, which was more common among uninfected individuals. Likewise, the C allele of rs2228570 showed a higher frequency in the infected group, whereas the T allele was significantly enriched in the non-infected group [29].
Correlation between H. pylori CagA seropositivity and serum vitamin D levels: H. pylori CagA seropositivity refers to the presence of antibodies in the blood against the CagA protein, a virulence factor produced by certain strains of H. pylori. Two studies have reported the relation between H. pylori CagA seropositivity and vitamin D [18,33]. Kuang et al. (2022) [18] reported that there was no significant association between serum vitamin D levels and H. pylori CagA seropositivity in the general population. After adjusting for confounders, vitamin D levels were found to be positively associated with CagA seropositivity among different ethnicities and individuals born outside the US. However, in Sorokman et al. 2020, the study found that CagA-seropositive children had the lowest levels of serum vitamin D, averaging 12.1 (0.9) ng/mL, which was significantly lower than in CagA-negative children [33].
Quality assessment
The quality assessment of the included studies is shown in Table 3. Using the NOS, we assessed seven studies as having high quality [10,18,19,24,25,27,28] and 13 studies as having moderate quality [15-17,20-23,26,29-33].
Discussion
This systematic review and meta-analysis synthesized evidence from 20 observational studies that examined the association between serum vitamin D levels and H. pylori infection. The results of our study underscore a potentially bidirectional interplay between vitamin D status and H. pylori pathogenesis, suggesting that vitamin D may serve not only as a biomarker of disease susceptibility but also as a modifiable factor influencing treatment outcomes.
Our study results reflect a consistent trend of reduced serum vitamin D levels among H. pylori-positive individuals across multiple geographic populations and age cohorts. While certain studies, such as Kuang et al. [18] and Chen et al. [25], reported non-significant associations, the overall effect size observed across 11 studies provides robust support for an inverse relationship. Additionally, the majority of the included studies showed an increased risk of serum vitamin D levels falling below 20 µg/L among H. pylori-infected individuals. This threshold is clinically relevant, as serum vitamin D levels <20 µg/L have been associated with impaired immune responses and increased susceptibility to bacterial infections [34]. This level was used by Chen et al., who documented successful eradication of H. pylori with increased serum vitamin D level equal to or above 20 µg/L, which provides a promising result of continuous increase in the serum vitamin level with time [25].
In addition to the quantitative serum analysis, we targeted the genetic analyses from three included studies to highlight key polymorphisms in the VDR and TLR4 genes that appear to modulate host susceptibility to H. pylori. Variants such as BsmI, ApaI, and FokI were significantly associated with H. pylori status, indicating a potential gene-environment interaction wherein host genetic predisposition amplifies the impact of hypovitaminosis D on infection risk. The findings add to the expanding evidence that vitamin D's immunomodulatory action mediated through the VDR plays a role in enhancing gastrointestinal mucosal immunity and modulating inflammatory signaling pathways.
Regarding the relationship between vitamin D levels and H. pylori virulence factors such as CagA, it remains inconclusive. We found controversial findings across the studies reporting this outcome. While Sorokman et al. observed significantly lower serum vitamin D levels among CagA-seropositive children [33]. Kuang et al. reported no significant association in general populations after adjustment for confounders [18]. This discrepancy may stem from variations in study design, population demographics, or assay sensitivity, highlighting the need for further research into the potential role of vitamin D in modulating the host response to distinct H. pylori strains.
The biological plausibility of our findings is supported by multiple proposed mechanisms through which vitamin D influences host defense against H. pylori. Vitamin D enhances expression of antimicrobial peptides such as cathelicidin and β-defensin, which disrupt bacterial membranes and suppress microbial colonization [35]. Moreover, activation of VDR in gastric epithelial cells has been shown to modulate autophagy and cytokine secretion, reducing gastric inflammation and facilitating bacterial clearance [36-38].
Emerging evidence also suggests that vitamin D may preserve gastric mucosal integrity through its role in epithelial barrier maintenance and oxidative stress reduction [39]. These pathways are particularly relevant given the chronic inflammation caused by H. pylori infection. Thus, vitamin D sufficiency may provide a protective immunological and epithelial milieu, reducing both initial susceptibility to infection and subsequent disease progression.
An updated systematic review and meta-analysis by Albatineh et al. in 2023 reported that serum vitamin D levels were significantly lower in infected cases with H. pylori compared to healthy controls. Also, the infected cases that were successfully managed and achieved complete eradication showed a higher level of serum vitamin D compared to those that did not achieve complete eradication [11]. The results of this previous systematic review align with our results. Also, Cai et al. evaluated the overall vitamin levels across infected, non-infected, completely eradicated, and non-eradicated H. pylori patients. The study agreed with our findings on the finding that serum vitamin D level was higher in non-infected cases compared to the infected individuals. Also, patients with complete eradication showed a significantly higher level of serum vitamin D compared to those with unsuccessful eradication [40]. Additionally, in the study conducted by Banama et al. in 2022, the study found that the addition of vitamin D supplementation to H. pylori eradication improved the eradication rate significantly (p < 0.05), showing promising results of serum vitamin D as a modifiable factor that would improve H. pylori treatment strategy [41]. Finally, a recent study done by Khan et al. in 2025 found that a deficiency in vitamin D could be a modifiable risk factor related to the development of H. pylori infections. These results highlight the necessity for additional long-term and interventional research to assess the possible benefits of vitamin D supplementation in preventing or managing H. pylori infections [42].
Limitations
Several limitations should be acknowledged. First, substantial heterogeneity was observed across studies (I² > 90%), likely reflecting differences in study design, diagnostic criteria for H. pylori, vitamin D assay methods, and population characteristics. Due to the substantial heterogeneity found across the studies, we adopted the use of a systematic review only without meta-analysis. Second, causality cannot be inferred from the included cross-sectional studies; it remains unclear whether vitamin D deficiency predisposes to *H. pylori *infection or vice versa. Longitudinal cohort studies and interventional trials are needed to elucidate temporal dynamics and therapeutic efficacy.
Third, variability in vitamin D thresholds and assay standardization presents a challenge. Definitions of deficiency ranged from <20 ng/mL to <30 ng/mL, and methods for measuring serum vitamin D (e.g., such as enzyme-linked immunosorbent assay (ELISA) and liquid chromatography-tandem mass spectrometry (LC-MS/MS)) may impact inter-study comparability. Future studies should adopt standardized protocols for vitamin D measurement and H. pylori diagnosis to enhance reproducibility and comparability.
Additionally, genetic analyses were limited to three studies, with varying degrees of statistical power. Although the associations reported are promising, replication in larger multiethnic cohorts and functional assays is required to validate these findings and elucidate their mechanistic significance.
Implications and Future Recommendations
Our findings carry a significant impact on H. pylori management and prevention. The vitamin D factor would serve as an adjunct in risk stratification and treatment strategy in settings with a high burden of H. pylori and prevalent vitamin D deficiency, such as low- and middle-income countries. Identifying individuals with concurrent H. pylori infection and vitamin D deficiency may allow for tailored interventions, including nutritional supplementation and lifestyle modifications.
Moreover, future randomized controlled trials should evaluate the efficacy of vitamin D supplementation as an adjunct to standard triple or quadruple therapy for H. pylori eradication. If proven beneficial, such interventions could be particularly valuable in populations with limited access to healthcare resources, where eradication failure rates remain high.
Conclusions
In conclusion, this systematic review and meta-analysis resulted in a significant inverse association between serum vitamin D levels and H. pylori infection, with implications for pathogenesis, eradication success, and public health interventions. However, we could not confirm causality; our findings provide a strong base for further research into vitamin D’s role in gastric immunity and its utility as a modifiable risk factor in managing *H. pylori *infection.
Integrating epidemiological evidence with molecular findings could facilitate future research in developing more targeted and effective strategies for the prevention and treatment of H. pylori infection.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Helicobacter pylori: a contemporary perspective on pathogenesis, diagnosis and treatment strategies Microorganisms Ali A Al Hussaini KI 222122024 https://doi.org/10.3390/microorganisms 120102223827620710.3390/microorganisms 12010222 PMC 10818838 · doi ↗ · pubmed ↗
- 2Helicobacter pylori (H. pylori) and cancer 7 2025 32013 https://www.cancer.gov/about-cancer/causes-prevention/risk/infectious-agents/h-pylori-fact-sheet
- 3Epidemiology, diagnosis and risk factors of Helicobacter pylori infection Helicobacter pylori in Human Diseases Kotilea K Bontems P Touati E 1733 Cham, Switzerland Springer 2019 https://doi.org/10.1007/5584_2019_35710.1007/5584_2019_35731016621 · doi ↗ · pubmed ↗
- 4Worldwide prevalence and risk factors of Helicobacter pylori infection in children Children (Basel) Borka Balas R MelițLE Mărginean CO 135992022 https://doi.org/10.3390/children 90913593613866910.3390/children 9091359 PMC 9498111 · doi ↗ · pubmed ↗
- 5Vitamin D and immune regulation: antibacaterial, antiviral, anti-inflammatory JBMR Plus L Bishop E Ismailova A Dimeloe S Hewison M White JH 052021 https://doi.org/10.1002/jbm 4.1040510.1002/jbm 4.10405 PMC 746127932904944 · doi ↗ · pubmed ↗
- 6The role of vitamin D receptors in gastric epithelial homeostasis Biology Theses Ismail Ali I 2018 https://scholarworks.uaeu.ac.ae/bio_theses/3
- 7Vitamin D receptor regulates liver regeneration after partial hepatectomy in male mice Endocrinology Elangovan H Stokes RA Keane J 771652024 https://doi.org/10.1210/endocr/bqae 07710.1210/endocr/bqae 077PMC 1125020938963813 · doi ↗ · pubmed ↗
- 8Mechanisms underlying the effect of vitamin D on the immune system Proc Nutr Soc Cantorna MT 286289692010 https://doi.org/10.1017/S 00296651100017222051552010.1017/S 0029665110001722 PMC 3138329 · doi ↗ · pubmed ↗