Conversion Surgery for Alpha-Fetoprotein–Producing Esophagogastric Junction Cancer with Multiple Liver Metastases and Portal Vein Tumor Thrombus after Nivolumab Combination Chemotherapy: A Case Report and Literature Review
Masaaki Akai, Shoji Takagi, Tomohiro Toji, Yoshifumi Mitani, Mikoto Shimabara, Yuta Nobunaga, Toshihisa Matsumura, Masafumi Inoue

TL;DR
A rare case of esophagogastric junction cancer with liver metastases was successfully treated with a combination of chemotherapy and surgery, leading to long-term remission.
Contribution
This case report demonstrates the feasibility of conversion surgery after nivolumab-based chemotherapy for AFP-producing cancer with liver metastases.
Findings
Combination therapy with S-1, oxaliplatin, and nivolumab led to rapid disappearance of liver metastases and normalization of AFP levels.
Conversion surgery achieved a complete pathological response with no recurrence 12 months post-surgery.
The treatment approach may be effective for selected patients with AFP-producing esophagogastric junction cancer.
Abstract
Alpha-fetoprotein–producing gastric cancer (AFPGC) is a rare subtype of gastric cancer associated with poor prognosis due to early liver metastasis. There have been limited reports on conversion surgery following nivolumab combination chemotherapy in cases of AFPGC with liver metastasis. Here, we present a case of alpha-fetoprotein–producing esophagogastric junction cancer (AFP-EGJC) successfully treated with this treatment. The patient was a 31-year-old man. After liver tumors were incidentally detected, he was diagnosed with esophagogastric junction cancer (cT3N1M1) with multiple liver metastases and portal vein tumor thrombus. Combination therapy with S-1 (tegafur/gimeracil/oteracil), oxaliplatin, and nivolumab was initiated. The response was remarkable, with the rapid disappearance of liver metastases. Serum AFP was also abnormally high at 691.9 ng/mL, but it quickly normalized…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
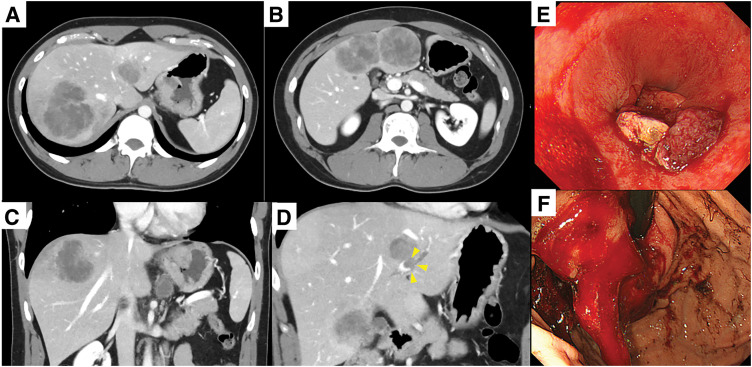 Fig. 1
Fig. 1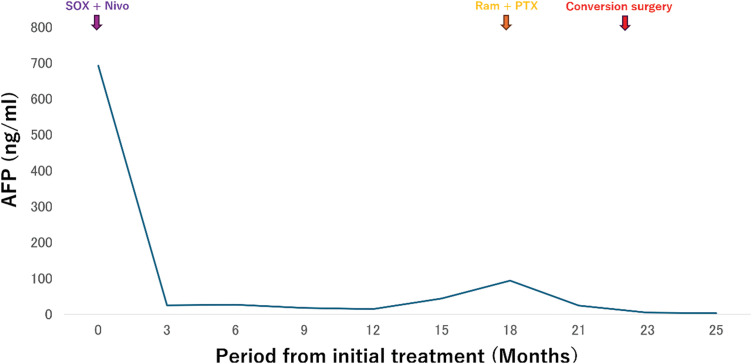 Fig. 2
Fig. 2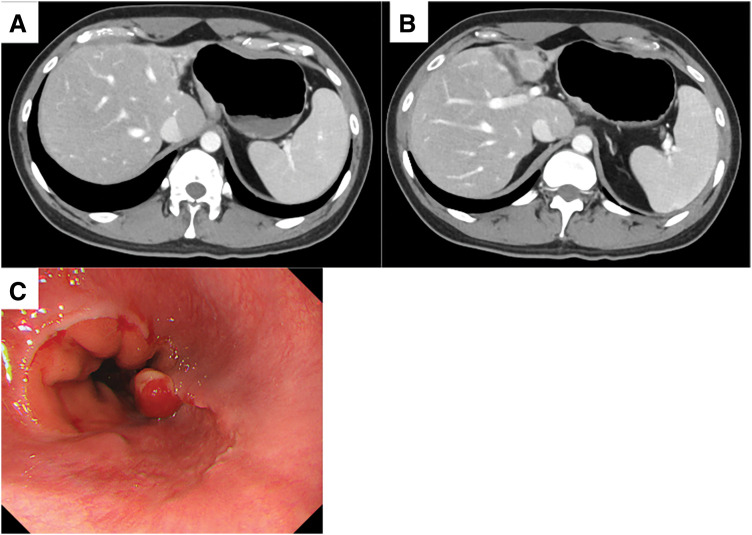 Fig. 3
Fig. 3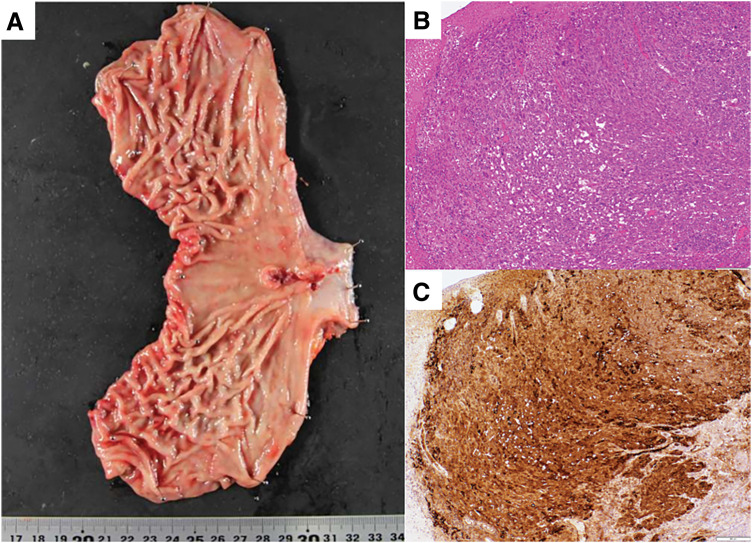 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal Cancer Research and Treatment · Gastric Cancer Management and Outcomes · Hepatocellular Carcinoma Treatment and Prognosis
Abbreviations
AFP alpha-fetoprotein AFP-EGJC alpha-fetoprotein–producing esophagogastric junction cancer AFPGC alpha-fetoprotein–producing gastric cancer CA19-9 carbohydrate antigen 19-9 CEA carcinoembryonic antigen CPS combined positive score CR complete response CS conversion surgery GC gastric cancer ICI immune checkpoint inhibitor Nivo nivolumab PD-L1 programmed death-ligand 1 SOX S-1 and oxaliplatin
INTRODUCTION
As GC is the fourth leading cause of cancer deaths worldwide and the fifth most frequently diagnosed cancer, it presents a significant global health problem.^1)^ The 5-year overall survival rate of patients with Stage IV GC is only 7%.^2)^ In recent years, immunotherapy, particularly ICIs, has garnered attention as a promising treatment strategy for GC. Recent clinical trials, the CheckMate649^3)^ and ATTRACTION-4^4)^ studies, demonstrated the efficacy of nivolumab-based combination chemotherapy as a first-line regimen for advanced or metastatic HER2-negative gastric adenocarcinoma. In Japan, the GC guidelines have recommended this regimen since November 2021.^5)^ CS has also attracted attention as a treatment for Stage IV GC, and some reports indicate that R0 resection can lead to longer survival.^6)^
AFP is an oncofetal protein.^7)^ Elevated serum AFP levels in adults are used as a clinical biomarker for hepatocellular carcinoma or yolk sac tumors.^8,9)^ AFPGC is a rare type of GC; the reported incidence of GC is 1.3%–15%.^10)^ AFPGC has a poor prognosis and is characterized by higher rates of venous invasion, lymphatic invasion, and metachronous or synchronous liver metastases than other GCs.^11–13)^
There have been limited reports on CS following nivolumab combination chemotherapy in cases of AFPGC with liver metastasis. Here, we present a patient with AFP-EGJC who underwent this treatment.
CASE PRESENTATION
A 31-year-old man with no significant medical history was incidentally noted to have liver tumors. Upper gastrointestinal endoscopy revealed advanced esophagogastric junction cancer (macroscopic type 2; esophageal invasion: 1.5 cm; gastric invasion: 4 cm) (Fig. 1). A biopsy confirmed poorly differentiated adenocarcinoma that was HER2-negative and AFP-positive. The PD-L1 CPS of this tumor was more than 5. Blood tests revealed a CEA level of 8.1 ng/mL, CA19-9 level of 58 U/mL, and an AFP level of 691.9 ng/mL. Contrast-enhanced CT revealed multiple liver metastases in both lobes with a portal vein tumor thrombus. The primary tumor appeared as a contrast-enhancing thickening of the gastric wall without serosal invasion. One enlarged lymph node was detected along the lesser curvature of the stomach. Based on these findings, the patient was diagnosed with AFP-EGJC, classified as clinical Stage IVB (cT3N1M1). Diagnostic laparoscopy was not performed at the initial presentation because multiple liver metastases were evident, and priority was given to prompt initiation of systemic therapy.
Contrast-enhanced CT and upper gastrointestinal endoscopy image before therapy. (A, B) Multiple liver metastases with a maximum diameter of 7.5 cm. (C) Primary esophagogastric junction cancer and lymph node metastasis. (D) Portal vein tumor thrombus (arrowheads). (E, F) Advanced esophagogastric junction cancer (macroscopic type 2; esophageal invasion: 1.5 cm; gastric invasion: 4 cm).
The patient was started on a regimen of S-1, oxaliplatin, and nivolumab (SOX + Nivo) as first-line chemotherapy. The tumor demonstrated a remarkable response, and a CT scan taken 3 months after treatment initiation showed a significant reduction in liver metastases. One year after starting therapy, the liver metastases achieved CR, with no detectable lesions on CT. Serum AFP levels also declined significantly, reaching 14 ng/mL after 1 year (Figs. 2 and 3). However, 15 months after treatment initiation, serum AFP levels increased, and progression was observed only in the primary lesion, with no recurrence of liver metastases. Second-line chemotherapy with nab-paclitaxel and ramucirumab was initiated. After 1 course, the tumor showed slight shrinkage, and curative resection via a transhiatal approach was considered feasible. Twenty-two months after initial treatment, the patient underwent laparoscopic proximal gastrectomy as CS. At the time of CS, the abdominal cavity was carefully inspected at the beginning of the procedure, and the absence of macroscopic peritoneal dissemination was confirmed before proceeding with tumor resection. The postoperative course was uneventful, and the patient was discharged on POD 9. Pathological examination confirmed ypStage IB (ypT2N0M0). The pathological response to chemotherapy was classified as Grade 1b, and immunohistochemistry showed diffuse AFP positivity (Fig. 4). After surgery, serum AFP levels returned to within the normal range. The patient remains alive and disease-free without adjuvant chemotherapy 12 months postoperatively.
Therapeutic course and serum level of AFP.AFP, alpha-fetoprotein; Ram + PTX, ramucirumab and nab-paclitaxel; SOX + Nivo, S-1, oxaliplatin, and nivolumab
Contrast-enhanced CT and upper gastrointestinal endoscopy image before conversion surgery. (A, B) Multiple liver metastases and the portal vein tumor thrombus disappeared, and gastric wall thickening and lymph node swelling also disappeared. (C) Upper gastrointestinal endoscopy revealed areas of scarring due to treatment and elevated lesions suggestive of residual cancer.
Resected specimen. (A) Macroscopic picture. (B) HE-stained image at ×40 magnification. Scale bar = 200 μm. (C) AFP immunostaining at ×40 magnification. Scale bar = 200 μm.AFP, alpha-fetoprotein; HE, hematoxylin and eosin
DISCUSSION
AFPGC is known to have a poor prognosis.^11–13)^ Esophagogastric junction cancer has a worse prognosis than GC.^14)^ Therefore, AFP-EGJC is considered to have an especially unfavorable prognosis. In this case, SOX + Nivo therapy was remarkably effective against an aggressive AFP-EGJC with multiple liver metastases, ultimately enabling curative resection via CS.
Numerous studies have reported the poor prognosis of AFPGC. According to a literature review by Ota et al.,^15)^ the median overall survival time was 14–72 months, and the 5-year survival rate was 8.3%–66%. Another review focusing on AFPGC in Japan reported that while high serum AFP levels were commonly seen in cases with liver metastases, AFP itself was not an independent prognostic factor.^16)^ Furthermore, it has been suggested that elevated AFP levels may correlate with reduced effectiveness of ICIs, as AFP may suppress antitumor immunity.^17)^
In the present case, although the initial AFP level was markedly elevated, it decreased dramatically in response to therapy. This suggests that a rapid decline in serum AFP levels may serve as an indicator of strong treatment response.
While several reports have demonstrated the effectiveness of chemotherapy in AFPGC,^18,19)^ reports on the efficacy of ICIs remain limited.^15,20,21)^ Most previously reported cases involving ICIs were in the context of recurrent tumors or gastric remnant cancer. To our knowledge, no prior cases have reported CS after first-line ICI-based therapy for AFP-EGJC.
When discussing CS for Stage IV GC, the Yoshida classification^22)^ provides a useful framework for patient selection. According to this classification, Stage IV disease is categorized based on resectability and response to systemic therapy, and CS is mainly considered for patients classified as Category 2, in whom initially unresectable disease becomes marginally resectable after chemotherapy.
In the present case, the patient would be classified as Category 2, as multiple liver metastases initially rendered the disease unresectable, but CR of the metastatic lesions and tumor shrinkage following systemic therapy enabled complete resection. This case supports the concept that CS may be considered in carefully selected patients; however, its indication, optimal timing, and long-term benefit remain to be clarified.
GC with liver metastasis is generally associated with poor prognosis, and systemic chemotherapy is considered the standard treatment. However, several studies have suggested that selected patients with liver-limited metastases may benefit from surgical intervention when a favorable response to chemotherapy is achieved.^23,24)^ In recent years, ICI-based combination chemotherapy has improved response rates in advanced GC, potentially increasing opportunities for CS in carefully selected patients. Although ICIs have improved response rates in advanced GC, their impact on the indications and long-term outcomes of CS remains to be fully elucidated.
In the present case, distant metastases were confined to the liver and achieved CR with nivolumab-based chemotherapy, which enabled curative resection. Nevertheless, such outcomes are exceptional, and the optimal indications, treatment strategies, and long-term prognosis for GC with liver metastasis remain to be clarified through further clinical experience and prospective studies.
The optimal timing of CS in such cases remains controversial. In our patient, CS was initially considered when the first-line SOX + Nivo therapy had achieved its maximum effect, but surgery was postponed due to a lack of consent. Several months later, progression of the primary tumor was observed, raising concern that further delay might lead to a loss of operability. Although the liver metastases remained in CR, the possibility of occult regrowth could not be completely excluded. If the liver lesions had relapsed, CS would have been limited to a debulking procedure, potentially compromising prognosis. After the initiation of second-line nab-paclitaxel plus ramucirumab, the primary tumor showed a favorable response and decreased in size, enabling resection via a transhiatal approach alone. At the same time, the liver metastases continued to show a sustained CR without progression. Based on these findings and the risk of further progression of the primary tumor, we judged that proceeding with CS at this early time point would maximize the chance of curative resection. Nevertheless, the optimal duration and sequencing of systemic therapy before CS remain controversial and require further investigation.
Pathological findings after CS revealed that there was no metastasis, even in the lymph nodes that had been enlarged before treatment. Based on the achievement of complete radical resection at CS, postoperative chemotherapy was discontinued. The patient remains alive and disease-free without adjuvant chemotherapy 12 months postoperatively. Although this favorable outcome was observed in a single case, further accumulation of cases is required to clarify appropriate patient selection and the optimal timing of CS.
CONCLUSIONS
We presented a case of AFP-EGJC with multiple liver metastases that was successfully managed with first-line nivolumab-based combination chemotherapy followed by CS. This treatment strategy may be feasible in selected patients; however, further accumulation of similar cases is required.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ilic M, Ilic I. Epidemiology of stomach cancer. World J Gastroenterol 2022; 28: 1187–203.35431510 10.3748/wjg.v 28.i 12.1187 PMC 8968487 · doi ↗ · pubmed ↗
- 2American Cancer Society. Stomach cancer early detection, diagnosis, and staging. 2025.
- 3Janjigian YY, Shitara K, Moehler M, et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (Check Mate 649): a randomised, open-label, phase 3 trial. Lancet 2021; 398: 27–40.34102137 10.1016/S 0140-6736(21)00797-2PMC 8436782 · doi ↗ · pubmed ↗
- 4Kang YK, Chen LT, Ryu MH, et al. Nivolumab plus chemotherapy versus placebo plus chemotherapy in patients with HER 2-negative, untreated, unresectable advanced or recurrent gastric or gastro-oesophageal junction cancer (ATTRACTION-4): a randomised, multicentre, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol 2022; 23: 234–47.35030335 10.1016/S 1470-2045(21)00692-6 · doi ↗ · pubmed ↗
- 5Japanese Gastric Cancer Association. Japanese Gastric Cancer Treatment Guidelines 2021 (6th edition). Gastric Cancer 2023; 26: 1–25.36342574 10.1007/s 10120-022-01331-8PMC 9813208 · doi ↗ · pubmed ↗
- 6Takeno A, Motoori M, Kishi K, et al. Prognostic factors of conversion surgery for stage IV gastric cancer: a multi-institutional retrospective analysis. Ann Gastroenterol Surg 2024; 8: 431–42.38707233 10.1002/ags 3.12778 PMC 11066490 · doi ↗ · pubmed ↗
- 7Soltani K. Alpha-fetoprotein: a review. J Invest Dermatol 1979; 72: 211–3.88486 10.1111/1523-1747.ep 12530749 · doi ↗ · pubmed ↗
- 8Tatarinov Iu S. Detection of embryo-specific alpha-globulin in the blood serum of a patient with primary liver cancer (in Russian). Vopr Med Khim 1964; 10: 90–1.14207501 · pubmed ↗