Perception, Practices, and Barriers to Cervical Cancer Screening Among Women in Rural and Urban Slums of Eastern India: A Community-Based Cross-Sectional Study
Geeta C Acharya, Sumelika Das, Avnika Jasuja, Ipsita Debata

TL;DR
This study finds that only a small percentage of women in rural and urban slums in Eastern India have been screened for cervical cancer, with major barriers including mistrust in public health services and poor awareness of free government programs.
Contribution
The study provides novel insights into the low uptake of cervical cancer screening in underserved regions of India and identifies key barriers such as mistrust and lack of awareness.
Findings
Only 6.7% of surveyed women had undergone cervical cancer screening, all through private facilities.
94-96% of women were unaware of free government screening services.
Mistrust in public health services and accessibility issues were strongly linked to non-participation in screening.
Abstract
Background Despite being avoidable with prompt screening, one of the notable causes of death among Indian women is still cervical cancer. Awareness, access to screening, and perceptions of risk differ considerably, especially in rural and underserved urban populations. Objective The purpose of the study was to assess awareness, perceptions, screening practices, and perceived barriers related to screening of cervical cancer among women, between the ages of 30 and 65 years, living in rural and urban slum areas of Eastern India. Methods A descriptive cross-sectional study was carried out between November 2024 and February 2025 in the community under the field practice areas of a tertiary care hospital in Bhubaneswar, Odisha. A total of 400 women (200 each from rural and urban slums) were chosen by a two-stage random sampling method. Information was gathered using a predesigned,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
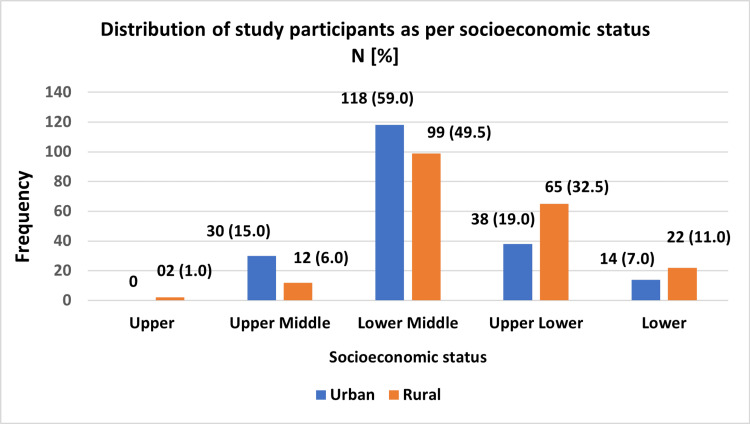 Figure 1
Figure 1| Variable | Category | Frequency (%) |
| Residence | Urban slum | 200 (50.0) |
| Rural | 200 (50.0) | |
| Age group (years) | 30–39 | 168 (42.0) |
| 40–49 | 142 (35.5) | |
| 50–65 | 90 (22.5) | |
| Marital status | Single | 63 (15.8) |
| Married | 325 (81.3) | |
| Widowed/Divorced | 12 (3.0) | |
| Education | Illiterate | 96 (24.0) |
| Primary | 118 (29.5) | |
| Secondary & above | 186 (46.5) |
| Domain | Item | Yes n (%) | No n (%) |
| Knowledge | Heard about cervical cancer | 124 (31.0) | 276 (69.0) |
| Aware of the affected age group | 51 (12.7) | 349 (87.3) | |
| Aware of the screening program | 36 (9) | 364 (91) | |
| Aware of screening locations | 53 (13.2) | 347 (86.8) | |
| Aware of human papillomavirus (HPV) vaccination | 22 (5.5) | 378 (94.5) | |
| Aware of signs and symptoms | 54 (13.5) | 346 (86.5) | |
| Practices | Use of contraception | 196 (49.0) | 204 (51.0) |
| Appropriate menstrual hygiene practices | 327 (81.8) | 73 (18.2) | |
| Ever undergone cervical cancer screening | 14 (3.5) | 386 (96.5) | |
| Encouraged for screening | 16 (4.0) | 384 (96.0) | |
| Barriers | Screening procedure perceived as painful | 47 (11.8) | 353 (88.2) |
| Lack of family support | 29 (7.3) | 371 (92.7) | |
| Difficulty accessing health facilities | 127 (31.8) | 273 (68.3) | |
| Belief that disease develops after screening | 184 (46.0) | 216 (54.0) | |
| Mistrust in health centers | 124 (31.0) | 276 (69.0) | |
| Lack of awareness due to poor promotion | 307 (76.8) | 93 (23.3) | |
| Fear of stigma | 77 (19.3) | 323 (80.8) |
| Variable | Category | Total n (%) | Ever Screened n (%) | Never Screened n (%) | χ² | p-value | |
| Awareness of cervical cancer | Yes | 122 (30.5) | 22 (18.0) | 100 (82.0) | 35.50 | < 0.001 | |
| No | 278 (69.5) | 5 (1.8) | 273 (98.2) | ||||
| Age group | < 45 years | 207 (51.8) | 16 (59.2) | 191 (51.2) | 0.65 | 0.418 | |
| ≥ 45 years | 193 (48.2) | 11 (40.8) | 182 (48.8) | ||||
| Perceived barriers to screening* | Perceived screening as painful | Yes | 47 (11.8) | 1 (3.7) | 46 (12.3) | 1.80 | 0.178 |
| No | 353 (88.2) | 26 (96.3) | 327 (87.7) | ||||
| Difficulty accessing health centers | Yes | 127 (31.8) | 2 (7.4) | 125 (33.5) | 7.91 | 0.004 | |
| No | 273 (68.2) | 25 (92.6) | 248 (66.5) | ||||
| Fear of stigma | Yes | 77 (19.3) | 2 (7.4) | 75 (20.1) | 2.61 | 0.106 | |
| No | 323 (23.0) | 25 (92.6) | 298 (79.9) | ||||
| Mistrust in health centers | Yes | 124 (31.0) | 3 (11.1) | 121 (32.4) | 5.35 | 0.021 | |
| No | 276 (69.0) | 24 (88.9) | 252 (67.6) | ||||
| Anticipated out-of-pocket expense | Yes | 113 (28.3) | 4 (14.8) | 109 (29.2) | 0.11 | 0.018 | |
| No | 287 (71.7) | 23 (85.2) | 264 (70.8) | ||||
| Characteristic | Knowledge OR (95% CI) | p-value | Favourable Attitude OR (95% CI) | p-value | Practices (Ever Screened) OR (95% CI) | p-value |
| Age | 0.95 (0.91–1.00) | 0.043 | 1.00 (0.98–1.03) | 0.892 | 0.99 (0.95–1.04) | 0.744 |
| Education | 1.34 (1.01–1.76) | 0.041 | 0.96 (0.82–1.12) | 0.600 | 0.80 (0.60–1.05) | 0.112 |
| Socioeconomic status | 0.57 (0.36–0.91) | 0.018 | 0.82 (0.61–1.09) | 0.176 | 0.67 (0.40–1.15) | 0.148 |
| Mistrust in health centres | 0.36 (0.14–0.93) | 0.034 | 10.13 (5.94–17.25) | <0.001 | 0.72 (0.29–1.79) | 0.480 |
| Fear of stigma | 2.71 (1.21–6.08) | 0.015 | 1.19 (0.66–2.13) | 0.560 | 1.08 (0.39–3.01) | 0.880 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCervical Cancer and HPV Research · Global Cancer Incidence and Screening · Reproductive tract infections research
Introduction
One of the rare cancers that can be mostly avoided with prompt screening, early detection, and appropriate treatment is cervical cancer. It continues to be a major source of women’s mortality and morbidity globally, particularly in low- and middle-income countries (LMICs), despite the availability of efficient preventive strategies. Globally, approximately 604,000 women were affected with cervical cancer, and more than 342,000 fatalities were reported in 2020 alone [1]. The burden is particularly disproportionate in India, which is responsible for over 25% of cervical cancer fatalities worldwide, with over 120,000 new cases and approximately 77,000 deaths annually [2].
Recognizing the preventable aspect of cervical cancer, public health initiatives in India, including the National Cancer Control Programme and the more recent National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS), have emphasized early screening using Visual Inspection with Acetic Acid (VIA) and Papanicolaou (Pap) smear testing, especially in primary healthcare level [3]. The World Health Organization advises routine cervical cancer screening starting at age 30 because, particularly in low-resource settings, the risk of persistent human papillomavirus infection and development to precancerous lesions increases significantly after this age [4]. Until the age of 65, screening is typically recommended; after that, the value diminishes for women who have undergone sufficient prior screening. The 30- to 65-year-old age group is the most suitable target demographic for cervical cancer screening, according to evidence from India, which balances screening yield, cost-effectiveness, and invasive disease prevention [5].
Despite this, screening coverage remains unacceptably low. National Family Health Survey-5 data reported that fewer than 2% of women from India, aged between 30 and 49 years, have ever had a cervical screening [3]. Although recent programmatic data suggest an expansion of screening through Ayushman Arogya Mandirs using VIA, with over 100 million women screened by mid-2025, this coverage remains uneven and does not adequately reflect uptake among socioeconomically disadvantaged populations [6].
Multiple barriers contribute to low screening uptake in India, including limited knowledge and awareness, sociocultural stigma, fear of pain or diagnosis, misconceptions regarding screening procedures, and poor accessibility to healthcare facilities. These barriers are particularly pronounced among women residing in rural areas and urban slums [7]. These communities often face the double burden of poverty and poor health infrastructure, leaving a gap between policy intent and ground reality. Consequently, a substantial gap persists between the accessibility and use of cervical cancer screening services at the community level.
In this context, the study was undertaken to assess the awareness, perceptions, and practices related to cervical cancer screening and to determine the perceived barriers to screening among women aged 30 - 65 years residing in rural and urban slum areas of Eastern India.
Materials and methods
Study design and setting
This cross-sectional study was conducted in the community between November 2024 and February 2025 at selected urban slums and rural villages under the field practice areas of the Urban Health and Training Centre (UHTC) and Rural Health and Training Centre (RHTC), respectively. Both centers run under the Community Medicine Department of a tertiary medical college and teaching hospital in Bhubaneswar, Odisha, India.
Study population and eligibility criteria
The study participants were women between the ages of 30 and 65 who had been residing in the selected areas for a minimum of six months. Women suffering from terminal health conditions and women diagnosed with psychiatric or convulsive disorders were excluded from the study.
Sample size
The sample size was determined using the formula \begin{document} n = \frac{4pq}{l^2} \end{document} , where p represents prevalence, q = 1-p, and l denotes allowable error. Assuming a prevalence of 50% to ensure maximum variability and an allowable error of 5%, the estimated sample size was 400 participants. This included 200 women, each from urban slums and rural villages.
Sampling technique
The study participants were chosen using a two-stage sampling process. In the first stage, five urban slums and five rural villages were chosen by simple random sampling from the list of eligible areas under the UHTC and RHTC, respectively. In the second stage, 40 eligible women were enrolled from each selected slum or village using a spatial random walk method.
The direction of household visits was determined by the bottle-spinning technique from a central point in each area, a field-friendly method that ensured the randomization of entry points. Data collection began at the first household in the indicated direction, and investigators proceeded sequentially to adjacent households. One eligible woman was interviewed per household. Locked houses and non-consenting participants were excluded without replacement. The process continued until the required sample size of 40 women per area was achieved, yielding a total of 400 participants.
Data collection tool and procedure
Data were collected by a predesigned questionnaire (Appendix 1), adapted from published literature and standard national guidelines [3,5,6,7]. To ensure content relevance, clarity, and contextual appropriateness, the questionnaire items were examined by subject matter experts in public health and community medicine. It was devised in English and translated into the local language, Odia, for field use. The questionnaire was back-translated to ensure conceptual and linguistic accuracy. To evaluate feasibility and clarity, a pilot test was carried out in a similar population from other urban slums and rural areas. Data from the pilot test were excluded from the final study, and no modifications were needed after the pilot.
Individual questionnaire items with binary (Yes/No) or categorical response options were used to evaluate knowledge, screening practices, and perceived barriers. No summative or aggregate scores were computed for knowledge, attitudes, or perceived barriers; each item was examined separately. The questionnaire included the following domains: Socio-demographic characteristics included residence, housing type, age, marital status, age at menarche, obstetric history, family history of cancer, menstrual history, education, occupation, and socioeconomic status. Knowledge regarding cervical cancer and screening included questions regarding awareness about cancer, signs and symptoms, the affected age group, the screening program, screening locations, and vaccination. Cervical cancer screening practices included questions on contraceptive use, menstrual hygiene practices, history of cervical cancer screening, type of screening procedure undergone, and source of encouragement or referral. Perceived barriers and attitude towards screening were assessed using questions addressing beliefs and attitudes regarding screening (e.g., fear of pain, embarrassment, stigma, mistrust, accessibility issues, misconceptions).
Face-to-face interviews were conducted by trained female field investigators and medical interns under faculty supervision to ensure participant comfort, cultural sensitivity, and data reliability.
Statistical analysis
Data were analyzed using IBM SPSS Statistics for Windows, version 21.0 (IBM Corp., Armonk, NY, USA). The results were summarized using descriptive statistics, such as frequencies, percentages, means, and standard deviations. To find independent predictors of cervical cancer screening behavior, binary logistic regression analysis was used. Every variable was considered categorical. Responses were coded as binary variables (Yes = 1, No = 0) for regression analysis. There was no conversion of summed or continuous scores into binary variables. Statistical significance was defined as a p-value of less than 0.05.
Ethical considerations
The Institutional Ethics Committee of Kalinga Institute of Medical Sciences, Bhubaneswar, granted ethical approval (KIIT/KIMS/IEC/2280/2025). Every participant provided written informed consent. Participants were made aware that participation in the study was entirely optional and that their responses would only be used for academic purposes, and privacy and confidentiality were upheld throughout.
Results
The study included 400 women in total, with equal representation from both urban slum areas and rural villages (200 participants each). The study participants’ average age was 39.09 ± 8.93 years. Table 1 depicts the sociodemographic details of the study participants.
Based on the Modified BG Prasad Socioeconomic Scale 2024 [8], 139 (34.75%) participants belonged to the lower socioeconomic category, as depicted in Figure 1.
Distribution of study participants according to socioeconomic status as per the Modified BG Prasad Scale (2024)Modified BG Prasad scale (2024) [8].
An overview of study participants' knowledge, practices, and perceived barriers for cervical cancer screening is provided in Table 2. All variables are presented as frequencies and percentages after being categorically analyzed. On assessing the knowledge, a substantial proportion of participants, 276 (69%), reported that they had never heard of cervical cancer. Awareness of free government-provided cervical cancer screening services was remarkably low, with 192/200 (96%) of urban slum residents and 189/200 (94.5%) of rural women being unaware of such services, resulting in an overall unawareness rate of 95.25%.
Among the screened participants, the majority were younger than 45 years, 16/27 (59.2%), and this age group showed a higher likelihood of screening uptake, although not significant (p = 0.418). For most of these women, the screening was initiated following a recommendation from a healthcare provider, which influenced 16/27 (59.3%) of screened women to undergo the procedure.
Among participants who had never been screened for cervical cancer, several barriers were identified, many of which showed statistical significance with non-utilization of screening services. Difficulty in accessing health centers (χ2 = 7.91, p = 0.004), mistrust in health centers (χ2 = 5.35, p = 0.021), and anticipated out-of-pocket expense (χ² = 0.11, p = 0.018) were found to be significant barriers to cervical cancer screening uptake among women from both rural and urban areas, as depicted in Table 3.
*Table 3: Knowledge, attitudes, practices, and perceived barriers related to cervical cancer screening and their association with screening uptake (n = 400)Values expressed as a number (%).Statistical test: Chi-square test of independence comparing each variable with cervical cancer screening uptake (ever screened vs never screened); p < 0.05 is considered statistically significant.Multiple responses permitted for perceived barriers.
As depicted in Table 4, binary logistic regression analysis demonstrated that socio-demographic variables like age, level of education, and socio-economic status showed statistically significant associations with screening knowledge (p = 0.043, p = 0.041, and p = 0.018, respectively). Mistrust in health centers was also significantly associated with both knowledge and favorable attitudes towards screening (p = 0.034, p < 0.001, respectively).
Table 4: Association of selected characteristics with knowledge, attitude, and cervical cancer screening practicesReference categories: Higher socioeconomic status; no mistrust in health centers; higher education levels. Statistical test: Binary logistic regression; p < 0.05 is considered statistically significant.Abbreviations: OR, odds ratio; CI, confidence interval.
Overall, the study reported low uptake of cervical cancer screening, poor awareness of available services, and the presence of deeply rooted practical and psychosocial barriers that hinder women from accessing potentially life-saving services. Gaps in communication, trust, and service delivery within the public health system are further highlighted by screened women's exclusive use of private healthcare facilities. To boost screening adoption, community-level knowledge must be strengthened, public health services must be trusted, and screening programs must be made more accessible and of higher quality.
Discussion
The present study emphasizes the persistently poor uptake of screening for cervical cancer in India, particularly among socioeconomically disadvantaged women, underscoring a substantial public health gap. The observed screening prevalence of 6.7% is alarmingly low and aligns with findings reported by Srivastava et al. (2022), who reported a prevalence of 3.9% among women in Delhi and Haryana [9]. Collectively, these findings suggest that despite national recommendations and the inclusion of screening for cervical cancer offered by the National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases, and Stroke (NPCDCS), population-level screening coverage remains far from adequate.
A particularly concerning finding in the present study is that all women who had undergone screening accessed services exclusively through private healthcare facilities, with no reported utilization of government screening services. This reflects a substantial gap in awareness regarding the availability of free cervical cancer screening in public health centers, as well as a lack of trust in government healthcare services. Similar patterns have been reported in other Indian studies, where perceived poor quality of care, breaches in privacy concerns, and negative attitude of healthcare providers have been identified as deterrents to the use of public-sector screening services.
The barriers identified in this study, including financial concerns, fear, stigma, distance to health facilities, and lack of information, are consistent with findings from multiple Indian settings. Studies by Ramaiah and Jayarama (2018) [10] and Naik et al. (2017) [11] reported poor awareness and sociocultural resistance to gynaecological examinations in rural Karnataka and urban Maharashtra, respectively. Olubodun et al. (2019) [12] further emphasized that fear and embarrassment acted as major deterrents to screening uptake. In Gujarat, Murugan et al. (2024) [13] reported that fewer than 10% of rural women had ever been screened, citing stigma, fatalistic beliefs, gender inequities, and low prioritization of women’s health as key barriers. These findings suggest that low screening uptake is influenced not only by service availability but also by sociocultural norms and deficits in trust within the health system.
International evidence reflects similar challenges across low- and middle-income countries. Studies from Ghana [14], Zimbabwe [15], and Iran [16] have consistently identified cultural taboos, misinformation, and fear of diagnosis as key predictors of non-screening behaviour, indicating that barriers to cervical cancer screening share common structural and sociocultural determinants across diverse settings.
An important finding of the present study was that health worker contact emerged as a significant motivating factor for screening uptake. Evidence from India [17,18] and Botswana [19] similarly demonstrates that interpersonal communication and community-based education delivered by frontline health workers can improve awareness and acceptance of screening for cervical cancer. This emphasizes the potential role that Accredited Social Health Activists (ASHAs), Auxiliary Nurse Midwives (ANMs), and other community health workers can play in bolstering screening programs via focused teaching and trust-building measures.
Socioeconomic factors, including low levels of education, limited income, and unemployment, were also linked to poor screening uptake in the present study. These findings were consistent with earlier studies by Lin (2008) [20], Wu (2003) [21], and Ba et al. (2021) [22], which demonstrated strong associations between socioeconomic disadvantage and reduced utilization of preventive health services.
Emerging strategies such as HPV self-sampling kits and mobile outreach services may help address several of the identified barriers. Evidence from India and other LMICs suggests that self-sampling approaches, as proposed by Bhatia et al. (2021) [23], may be particularly acceptable to women who are hesitant to undergo facility-based pelvic examinations. Integrating such approaches with strengthened community engagement and improved public health infrastructure and delivery could enhance cervical cancer screening coverage in underserved populations.
Recommendations
The results of the study indicate that increasing community-level knowledge through culturally relevant health education given in local languages is necessary to improve cervical cancer screening uptake in low-resource settings. Frontline healthcare professionals, such as Anganwadi workers and Accredited Social Health Activists (ASHAs), can be crucial in educating the public, dispelling myths, and encouraging women to use screening programs. It may be possible to increase awareness and normalize preventative gynecological care by incorporating cervical cancer screening messages into already-existing maternity and reproductive health platforms, such as Village Health and Nutrition Days.
It is equally necessary to address psychological and structural impediments. While consistent service delivery and better communication regarding free screening services may lessen mistrust in public health facilities, strategies like the introduction of human papillomavirus self-sampling approaches may help overcome embarrassment and reluctance toward facility-based screening. In an effort to increase awareness, trust, and screening uptake, community health workers participated in targeted health education sessions after the study's findings were shared, and talks with local health authorities were started to organize recurring screening camps and improve referral connections.
Limitations
As a cross-sectional study, the information was captured at a single point in time, and therefore, does not allow causal inferences between knowledge, attitudes, and cervical cancer screening practices. Recall bias or social desirability bias could have also arisen from the use of self-reported data, especially for sensitive issues related to reproductive health. However, the use of a representative sample and a comparative urban-rural approach strengthened the relevance of our findings. Additionally, interviews conducted in participants’ homes may have influenced responses in joint or extended family settings. The study did not include male partners or family decision-makers, whose influence may affect women’s healthcare-seeking behaviour; this warrants future qualitative research.
Conclusions
This community-based study demonstrates that screening uptake for cervical cancer among women in urban slums and rural areas of Eastern India remains low. Fewer than one in fifteen women had ever undergone cervical cancer screening, and nearly three-fourths of participants lacked awareness regarding the availability of free screening services at government health facilities. Structural and psychosocial barriers, including mistrust in public health services, limited accessibility, and concerns related to stigma or embarrassment, were commonly reported. Despite the availability of cost-free screening under national programs, utilization was limited to private healthcare facilities, underscoring gaps in public health communication and trust. Strengthening community-level awareness through frontline health workers, improving accessibility, and enhancing trust in public sector services are essential to enhance screening uptake and to support progress toward cervical cancer prevention goals.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global Strategy to Accelerate the Elimination of Cervical Cancer as a Public Health Problem 10 2025 World Health Organization Geneva World Health Organization 2020 https://www.who.int/publications/i/item/9789240014107
- 2Cervical Cancer GLOBOCAN 9 2025 International Gynecologic Cancer Society 2022 Lyon International Gynecological Cancer Society Lyon, France: IARC 2025 https://igcs.org/cervical/?gad_source=1&gad_campaignid=20388608083&gbraid=0AAAA Ap O Xby T Vyl T 8l T Xfdm 54Bht WC Hi YN&gclid=Cjw KC Ai Ava LL Bh BF Eiw AYCN Tfw Kg Tz MO 8T 9x AEZC 4r 45AI-w RCOO Zaaky S 7z B Ep PE Lb T_w 7R Uuiujho Cl HUQ Av D_Bw E
- 3Status of cancer screening in India: an alarm signal from the National Family Health Survey (NFHS-5)J Family Med Prim Care Gopika MG Prabhu PR Thulaseedharan JV 730373071120223699298910.4103/jfmpc.jfmpc_1140_22PMC 10041275 · doi ↗ · pubmed ↗
- 4New recommendations for screening and treatment to prevent cervical cancer | World Health Organization 9 2025 Accessed October 8, 2025.Published July 6, 20212021 https://www.who.int/news/item/06-07-2021-new-recommendations-for-screening-and-treatment-to-prevent-cervical-cancer
- 5Cervical cancer screening: is the age group 30-65 years optimum for screening in low-resource settings?J Obstet Gynaecol India Gupta R Sharda A Kumar D Fulzele R Dwivedi R Gupta S 5305367120213460276510.1007/s 13224-021-01479-w PMC 8440710 · doi ↗ · pubmed ↗
- 6Ministry of Health and Family Welfare, Government of India. 10.18 crore women screened for cervical cancer under Ayushman Arogya Mandirs and NHM 9 2025 2025 https://www.mohfw.gov.in/?q=en/pressrelease-279
- 7An epidemiological study of cervical and breast screening in India: district-level analysis BMC Womens Health Monica Monica Mishra R 2252020203302833610.1186/s 12905-020-01083-6PMC 7542863 · doi ↗ · pubmed ↗
- 8Socioeconomic status assessment in India: history and updates for 2024 Int J Community Med Public Health Javalkar SR Shalini H Davalagi SB Vidya GS 13691377112024