Association Between Postpartum Depression Symptoms of Primiparas and Uterine Recovery, Sleep Quality and Postpartum Stress
Hui Gao, Xiao Yang

TL;DR
This study explores how postpartum depression in first-time mothers is linked to uterine recovery, sleep quality, and postpartum stress.
Contribution
The study identifies specific risk and protective factors for postpartum depression in primiparous women.
Findings
Poor sleep quality and high postpartum stress are significant risk factors for postpartum depression.
Adequate lochia volume and good pelvic floor muscle recovery act as protective factors against postpartum depression.
Lower education level and illness during pregnancy are also independent risk factors for postpartum depression.
Abstract
To investigate the relationship between postpartum depression (PPD) symptoms in primiparous women and uterine recovery, sleep quality and postpartum stress. This retrospective study enrolled 194 postpartum women who underwent 42-day postpartum examinations in our hospital from February 2024 to February 2025. General demographic information, uterine recovery (including uterine fundal height decline, lochia volume and pelvic floor muscle recovery), sleep quality (determined using the Pittsburgh Sleep Quality Index [PSQI]) and postnatal stress levels (measured using the Maternal Postpartum Stress Scale [MPSS]) were collected through the electronic medical record system. PPD was assessed using the Edinburgh Postnatal Depression Scale (EPDS). Mothers with an EPDS score ≥10 were classified into the PPD group, and those with <10 were classified into the non-PPD group. Univariate and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
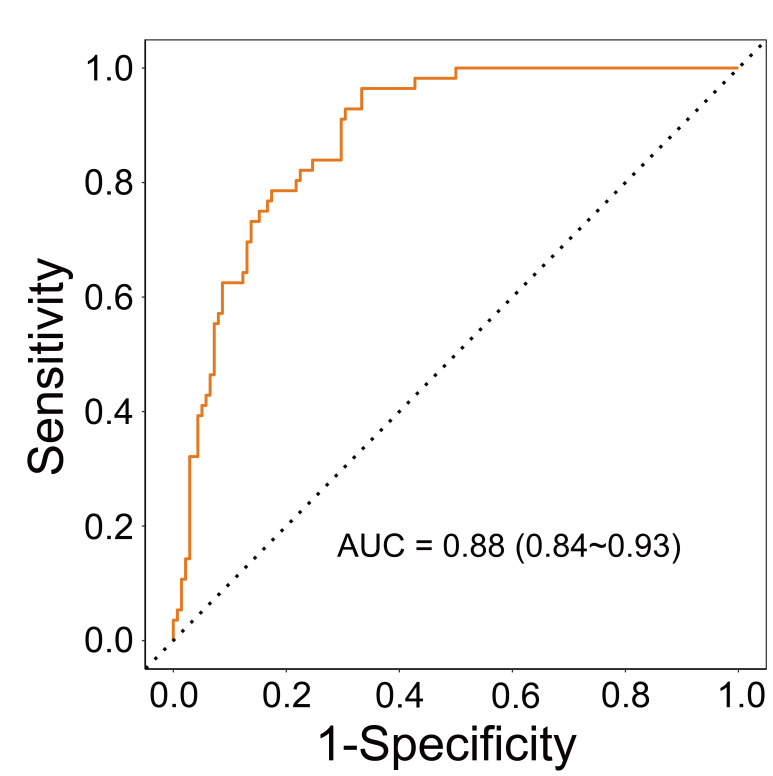 Fig. 1
Fig. 1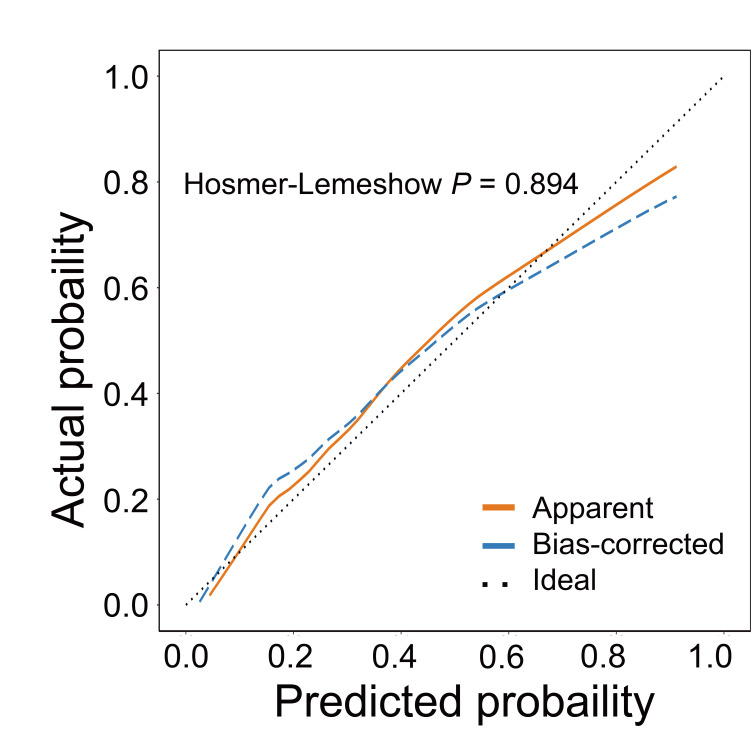 Fig. 2
Fig. 2| Variables | Total (n = 194) | Non-PPD group (n = 138) | PPD group (n = 56) | Statistic |
| |
| Age, n (%) | 0.390 | |||||
| 96 (49.48) | 71 (51.45) | 25 (44.64) | ||||
| 98 (50.52) | 67 (48.55) | 31 (55.36) | ||||
| Educational level, n (%) | 0.010 | |||||
| Specialist and above | 111 (57.22) | 87 (63.04) | 24 (42.86) | |||
| High school and below | 83 (42.78) | 51 (36.96) | 32 (57.14) | |||
| Marital relationship, n (%) | 0.017 | |||||
| Harmony | 141 (72.68) | 107 (77.54) | 34 (60.71) | |||
| Disharmony | 53 (27.32) | 31 (22.46) | 22 (39.29) | |||
| Monthly household income (CNY)a, n (%) | 0.226 | |||||
| 156 (80.41) | 114 (82.61) | 42 (75.00) | ||||
| 38 (19.59) | 24 (17.39) | 14 (25.00) | ||||
| Unintended pregnancy, n (%) | 0.375 | |||||
| No | 163 (84.02) | 118 (85.51) | 45 (80.36) | |||
| Yes | 31 (15.98) | 20 (14.49) | 11 (19.64) | |||
| Regular prenatal check-ups, n (%) | 0.022 | |||||
| No | 60 (30.93) | 36 (26.09) | 24 (42.86) | |||
| Yes | 134 (69.07) | 102 (73.91) | 32 (57.14) | |||
| Illness during pregnancy, n (%) | 0.007 | |||||
| No | 158 (81.44) | 119 (86.23) | 39 (69.64) | |||
| Yes | 36 (18.56) | 19 (13.77) | 17 (30.36) | |||
| Mode of delivery, n (%) | 0.112 | |||||
| Vaginal delivery | 83 (42.78) | 64 (46.38) | 19 (33.93) | |||
| Caesarean section | 111 (57.22) | 74 (53.62) | 37 (66.07) | |||
| Postpartum haemorrhage, n (%) | 0.369 | |||||
| No | 117 (60.31) | 86 (62.32) | 31 (55.36) | |||
| Yes | 77 (39.69) | 52 (37.68) | 25 (44.64) | |||
| Health status of newborns, n (%) | 0.017 | |||||
| Good health | 141 (72.68) | 107 (77.54) | 34 (60.71) | |||
| Poor health | 53 (27.32) | 31 (22.46) | 22 (39.29) | |||
| Neonatal gender, n (%) | 0.147 | |||||
| Female infant | 95 (48.97) | 63 (45.65) | 32 (57.14) | |||
| Male infant | 99 (51.03) | 75 (54.35) | 24 (42.86) | |||
| Feeding methods, n (%) | 0.159 | |||||
| Breastfeeding | 81 (41.75) | 62 (44.93) | 19 (33.93) | |||
| Artificial feeding | 113 (58.25) | 76 (55.07) | 37 (66.07) | |||
| PSQI score, M (Q1, Q3) | 7.00 (6.00, 9.00) | 7.00 (6.00, 9.00) | 9.00 (7.00, 11.00) | Z = –3.21 | 0.001 | |
| MPSS score, Mean | 16.25 | 15.37 | 18.41 | t = –3.61 | ||
| Grouping | n | Uterine fundal height decline (mm) | Lochia volume (mL) | ||
| 24 h postpartum | 48 h postpartum | 24 h postpartum | 48 h postpartum | ||
| PPD group | 56 | 8.12 | 11.47 | 204.35 | 44.31 |
| Non-PPD group | 138 | 8.37 | 11.82 | 214.62 | 49.24 |
| t value | 1.35 | 1.58 | 3.61 | 5.73 | |
| 0.180 | 0.115 | ||||
| Grouping | n | Muscle strength grade | ||
| Grade I | Grade II | |||
| PPD group | 56 | 11 | 29 | 16 |
| Non-PPD group | 138 | 12 | 48 | 78 |
| t value | 4.57 | 4.81 | 12.46 | |
| 0.033 | 0.028 | |||
| Variables |
| SE | Z |
| OR (95% CI) | Assignment | |
| Age | |||||||
| 1.00 (Reference) | 0 | ||||||
| 0.27 | 0.32 | 0.86 | 0.391 | 1.31 (0.70–2.45) | 1 | ||
| Educational level | |||||||
| Specialist and above | 1.00 (Reference) | 0 | |||||
| High school and below | 0.82 | 0.32 | 2.55 | 0.011 | 2.27 (1.21–4.28) | 1 | |
| Marital relationship | |||||||
| Harmony | 1.00 (Reference) | 0 | |||||
| Disharmony | 0.80 | 0.34 | 2.35 | 0.019 | 2.23 (1.14–4.36) | 1 | |
| Monthly household income (CNY)a | |||||||
| 1.00 (Reference) | 0 | ||||||
| 0.46 | 0.38 | 1.20 | 0.229 | 1.58 (0.75–3.35) | 1 | ||
| Unintended pregnancy | |||||||
| No | 1.00 (Reference) | 0 | |||||
| Yes | 0.37 | 0.41 | 0.88 | 0.377 | 1.44 (0.64–3.25) | 1 | |
| Regular prenatal check-ups | |||||||
| No | 1.00 (Reference) | 0 | |||||
| Yes | –0.75 | 0.33 | –2.27 | 0.023 | 0.47 (0.25–0.90) | 1 | |
| Illness during pregnancy | |||||||
| No | 1.00 (Reference) | 0 | |||||
| Yes | 1.00 | 0.38 | 2.63 | 0.008 | 2.73 (1.29–5.77) | 1 | |
| Mode of delivery | |||||||
| Vaginal delivery | 1.00 (Reference) | 0 | |||||
| Caesarean section | 0.52 | 0.33 | 1.58 | 0.114 | 1.68 (0.88–3.21) | 1 | |
| Postpartum haemorrhage | |||||||
| No | 1.00 (Reference) | 0 | |||||
| Yes | 0.29 | 0.32 | 0.90 | 0.370 | 1.33 (0.71–2.50) | 1 | |
| Health status of newborns | |||||||
| Good health | 1.00 (Reference) | 0 | |||||
| Poor health | 0.80 | 0.34 | 2.35 | 0.019 | 2.23 (1.14–4.36) | 1 | |
| Neonatal gender | |||||||
| Female infant | 1.00 (Reference) | 0 | |||||
| Male infant | –0.46 | 0.32 | –1.45 | 0.148 | 0.63 (0.34–1.18) | 1 | |
| Feeding methods | |||||||
| Breastfeeding | 1.00 (Reference) | 0 | |||||
| Artificial feeding | 0.46 | 0.33 | 1.40 | 0.161 | 1.59 (0.83–3.03) | 1 | |
| 24 h uterine fundal height decline | –0.18 | 0.13 | –1.34 | 0.180 | 0.84 (0.65–1.08) | ||
| 48 h uterine fundal height decline | –0.19 | 0.12 | –1.57 | 0.116 | 0.83 (0.66–1.05) | ||
| 24 h lochia volume | –0.03 | 0.01 | –3.37 | 0.97 (0.95–0.99) | |||
| 48 h lochia volume | –0.17 | 0.03 | –4.93 | 0.84 (0.79–0.90) | |||
| PSQI score | 0.18 | 0.06 | 3.15 | 0.002 | 1.20 (1.07–1.35) | ||
| MPSS score | 0.11 | 0.03 | 3.39 | 1.11 (1.05–1.19) | |||
| Pelvic floor muscle strength | |||||||
| Grade I | 1.00 (Reference) | 0 | |||||
| Grade II | –0.42 | 0.48 | –0.87 | 0.384 | 0.66 (0.26–1.69) | 1 | |
| –1.50 | 0.50 | –3.00 | 0.003 | 0.22 (0.08–0.60) | 2 | ||
| Variables |
| SE | Z |
| OR (95% CI) | VIF | |
| Educational level | |||||||
| Specialist and above | 1.00 (Reference) | ||||||
| High school and below | 0.84 | 0.41 | 2.07 | 0.039 | 2.33 (1.05–5.18) | 1.01 | |
| Illness during pregnancy | |||||||
| No | 1.00 (Reference) | ||||||
| Yes | 1.07 | 0.50 | 2.13 | 0.033 | 2.91 (1.09–7.78) | 1.03 | |
| 24 h lochia volume | –0.03 | 0.01 | –2.41 | 0.016 | 0.97 (0.95–0.99) | 1.02 | |
| 48 h lochia volume | –0.20 | 0.05 | –4.41 | 0.82 (0.75–0.89) | 1.03 | ||
| PSQI score | 0.19 | 0.07 | 2.48 | 0.013 | 1.20 (1.04–1.39) | 1.02 | |
| MPSS score | 0.11 | 0.04 | 2.79 | 0.005 | 1.11 (1.03–1.20) | 1.03 | |
| Pelvic floor muscle strength | |||||||
| Grade I | 1.00 (Reference) | ||||||
| Grade II | –0.02 | 0.59 | –0.03 | 0.973 | 0.98 (0.31–3.10) | ||
| –1.40 | 0.60 | –2.33 | 0.020 | 0.25 (0.08–0.80) | 1.01 | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal Mental Health During Pregnancy and Postpartum · Menstrual Health and Disorders · Sleep and related disorders
Introduction
Postpartum depression (PPD) refers to a common mental health disorder in women after childbirth [1]. This condition is characterised by persistent low mood, loss of interest and anxiety [2]. According to the global burden of disease estimate, the global incidence rate of PPD is approximately 17.22% [3]. PPD not only seriously affects maternal physical and mental health and the quality of life but may also have long-term adverse effects on infant growth and development, parent–child interaction and family functioning [4]. The risk of PPD in primiparous women requires extra attention due to factors, such as the lack of childcare experience and difficulties in adapting to role changes. With the adjustment of reproductive policy and the increase in social concern for women’s health, in-depth investigation of factors affecting PPD in primiparous women is of great clinical and public health significance for early prevention and intervention.
The assessment of uterine recovery typically encompasses multiple dimensions [5]. Uterine fundal height descent denotes a classical and straightforward clinical measure for tracking the pace of uterine involution; a slow descent may indicate subinvolution, which is associated with discomfort and potential infection [6]. Lochia volume, particularly in the immediate postpartum period, serves as a critical indicator of endometrial shedding and regeneration. Abnormally scant or prolonged lochia can signal retained products of conception or infection, both of which are sources of physical pain and psychological distress [7]. Furthermore, the childbirth process poses a major trauma to the pelvic floor. Pelvic floor muscle strength is increasingly recognised as a key component of postpartum recovery, as its impairment is directly linked to urinary incontinence and sexual dysfunction, which severely affect a woman’s quality of life, self-esteem and psychological well-being [8]. A close association exists between postnatal physical discomfort and negative emotions, and the discomfort caused by poor uterine recovery may interfere with a woman’s daily life and increase her psychological stress, which in turn may induce depressive symptoms [9]. The quality of sleep is another key factor that affects the physical and mental health of postpartum women [10]. Factors such as fluctuating hormone levels after childbirth, the need for breastfeeding and nighttime care for newborns make sleep disruption a common problem for postpartum women [11]. Sleep disorders are an important risk factor for PPD [12]. Postnatal stress refers to the psychological pressure that arises in the postpartum period due to a variety of factors, such as changes in maternal roles, adjustments in family relationships and childcare responsibilities [13]. Postpartum stress serves as an important psychosocial factor in the development of PPD [14]. However, systematic research on the quantitative relationship between indicators of uterine recovery, sleep quality and postpartum stress and PPD is still lacking, and the underlying mechanisms of action have not been fully clarified.
This study aimed to further explore the factors influencing PPD and its related mechanisms by investigating postpartum depressive symptoms in primiparous women and their association with uterine recovery, sleep quality and postpartum stress. Through this study, we expect to provide new bases and ideas for the early identification and intervention of PPD and provide scientific support for the improvement of maternal physical and mental health and mother–infant relationship. Meanwhile, this work will also provide reference for clinicians in postnatal health care, helping them to focus more on the physical and mental health of mothers, identify and deal with PPD in a timely manner and improve the quality of life of mothers and the well-being of their families.
Materials and Methods
Study Population
We conducted a retrospective study that included parturients who underwent 42-day postpartum check-ups from February 2024 to February 2025 at the obstetrics clinic of the West China Second University Hospital, Sichuan University. A total of 194 study participants were finally included. The study received approval from the Medical Research Ethics Committee of the West China Second University Hospital, Sichuan University (Ethics Approval Number: 2025-068) and strictly adhered to the medical ethical principles of the Declaration of Helsinki. All patients gave informed consent.
Sample Size Calculation
According to a cross-sectional study of the Chinese population, 20.2% of postpartum women have symptoms of PPD [15]. Therefore, this study adopted 20% as the estimated value for the expected prevalence of PPD to ensure a sufficient sample size representing the disease burden in the target population. Another meta-analysis involving 12,614 pregnant women indicated that sleep disorders were significantly associated with the risk of PPD, with a combined effect size of odds ratio (OR) = 2.36 [16]. The required sample size was calculated using G*Power (version 3.1.9.7; Heinrich-Heine-Universität Düsseldorf; Düsseldorf, Germany). The significance level ( ) was set at 0.05 and the test power (1- ) at 0.80. The calculation results show that the total sample size should be at least 155 cases. A total of 194 patient data were analysed in this study, which met the sample size requirements.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: (1) singleton pregnancy and first delivery; (2) aged 18–40 years old; (3) visiting the obstetrics outpatient clinic of our hospital for routine checkups on time 42 days after delivery; (4) having normal communication skills and being able to understand and complete the questionnaire independently.
The exclusion criteria included the following: (1) psychiatric disorders (e.g., depression, anxiety disorders, schizophrenia, etc.) diagnosed before pregnancy; (2) serious postnatal complications (e.g., postpartum haemorrhage, puerperal infections, eclampsia, etc.) and are still under therapeutic observation; (3) serious hearing, visual or speech disorders and inability to fill in the scale.
Data Collection
Data collection was completed by uniformly trained clinicians. The data on research subjects were extracted by the researchers from the hospital’s electronic medical record system; the information included maternal age, education level, couple relationship, monthly household income, whether the pregnancy was unplanned, regularity of antenatal check-ups, presence of pregnancy diseases, mode of delivery, postpartum haemorrhage, newborn’s health status, newborn’s gender and mode of feeding. The height of the uterine fundus descent and amount of lochia at 24 and 48 h after delivery were also collected. The health status of the newborn was assessed at the 42-day postpartum check-up: (1) Good health: A newborn who was full-term (gestational age 37 weeks), with a birth weight appropriate for gestational age and without any diagnosed major congenital anomalies, severe neonatal diseases (such as severe neonatal asphyxia, sepsis or need for neonatal intensive care unit admission) or ongoing significant medical concerns at the time of the check-up. (2) Poor health: A newborn who was preterm (gestational age 37 weeks), had low birth weight, and/or was diagnosed with any major congenital anomaly, severe neonatal disease or presented with any significant ongoing medical issue requiring follow-up or treatment. In addition, maternal pelvic muscle recovery was assessed by the obstetrician at the 42-day outpatient visit on the basis of the modified Oxford scale grading system [17]. This system grades pelvic floor muscle strength on a 6-point scale (0 to 5) as follows: 0 = no contraction; 1 = flicker (a minor muscle twitch); 2 = weak contraction (partial muscle compression without resistance); 3 = moderate contraction (complete muscle compression with slight resistance); 4 = good contraction (complete compression against moderate resistance); 5 = strong contraction (complete compression against strong resistance). A high grade indicates desirable recovery of pelvic floor muscle strength [18].
Survey Methodology
All the clinicians and researchers who participated in the questionnaire survey received professional training, with emphasis on the use of gentle, neutral and noncritical language when asking questions and avoidance of direct or sensitive questions that may cause discomfort to the parturients. In regard to sensitive issues related to postpartum stress, we adopted a step-by-step guiding approach, starting with general problems and gradually transitioning to specific ones, which provided new mothers with sufficient time to adapt and think. If during the investigation, the parturient showed emotional fluctuations or discomfort, the investigators were to immediately suspend the investigation, provide necessary psychological support and refer the patient to a professional psychological counsellor if necessary. At the beginning of the questionnaire, we clearly informed the parturients of the anonymity and confidentiality of the survey to ensure that they could answer the questions with peace of mind and reduce the psychological pressure caused by concerns about privacy leakage.
Survey Scale
This hospital prioritises the mental wellbeing of maternity patients. Routine mental health questionnaires were administered to all maternity patients. The survey results were routinely incorporated into individual medical records, and the information from the scales were extracted for this research.
The presence of postpartum depressive symptoms was assessed using the Edinburgh Postnatal Depression Scale (EPDS) [19]. The EPDS is a widely used and validated screening tool for the identification of women at high risk for PPD in research and clinical settings, particularly in obstetric populations [19]. Although a formal clinical diagnosis of major depressive disorder requires a comprehensive evaluation based on standardised diagnostic criteria (e.g., Diagnostic and Statistical Manual of Mental Illnesses-5), a cutoff score of 10 on the EPDS has good sensitivity and specificity for identifying probable cases of PPD in community and obstetric samples [20, 21]. The EPDS scale consists of 10 items and adopts a 4-level scoring standard (0–3 points), with a score range of 0–30 points. The higher the EPDS score is, the greater the possibility of the patient having depressive symptoms. Those with EPDS scores 10 points were allotted into the non-PPD group, and those with scores 10 points were included in the PPD group. In this study, the Cronbach’s alpha coefficient of the EPDS scale was 0.89.
The postpartum sleep status of the research subjects was evaluated using the Pittsburgh sleep quality index (PSQI) [22]. The PSQI scale consists of 19 self-rated questions used to generate scores across seven components: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication and daytime dysfunction. The PSQI scale adopts a four-level scoring standard (0–3 points), with a score range of 0–21 points. The higher the PSQI score, the poorer the sleep quality. In this study, the Cronbach’s alpha coefficient of the PSQI scale was 0.81.
The postpartum stress level was evaluated using the Maternal Postpartum Stress Scale (MPSS) [23]. The MPSS scale consists of 22 items covering four dimensions: personal needs, infant care, physical changes and sexual behaviour. The MPSS scale adopts a 5-level scoring standard (0–4 points), with a total score ranging from 0 to 88 points. The higher the total score of MPSS, the higher the postpartum stress level. In this study, the MPSS scale had a Cronbach’s alpha coefficient of 0.87.
Statistical Analysis
Data were analysed using SPSS (Version 27.0; IBM Corp.; Armonk, NY, USA) statistical software. Measurements are expressed as mean standard deviation ( s), where normal distribution was confirmed by the Shapiro–Wilk test, and comparisons between groups were achieved using independent sample t-test. Non-normally distributed data were expressed as medians, and the Mann–Whitney U test was used for between-group comparisons. Count data were expressed as the number of cases (percentage) [n (%)], and comparisons between groups were performed using the ^2^ test or Fisher’s exact probability method (when the theoretical frequency was 5). Independent risk factors were assessed using multifactorial logistic regression analysis, and (ORs) and their 95% confidence intervals (CIs) were calculated. Variables with *p * 0.05 in univariate logistic regression were included in the multivariate logistic regression model. Multivariate logistic regression analysis was performed using the stepwise regression method (screening criterion: *p * 0.05). The variance inflation factor (VIF) was used to evaluate the collinearity among variables in the multivariate logistic regression model. VIF 5 was considered to indicate no collinearity among variables. The receiver operating characteristic (ROC) curve and its area under the curve (AUC) were used to assess the discrimination of the logistic model, and the calibration curve and Hosmer–Lemeshow test were used to evaluate the calibration. All the tests were bilateral, and *p * 0.05 was considered statistically significant.
Results
General Information of the Participants
A total of 194 primiparous women, 56 in the PPD group and 138 in the non-PPD group, were included in this study. No significant difference was observed in the distribution of the two groups in terms of age, monthly household income, unplanned pregnancy, mode of delivery, postpartum haemorrhage, sex of the newborns and feeding methods (*p * 0.05) (Table 1). In the PPD group, the proportion of those with high school or lower education, disharmony with husband, no regular prenatal checkups and the presence of illnesses during pregnancy were significantly higher than that in the non-PPD group. In addition, the PPD group had a higher proportion of newborns with poor health. The PPD group also displayed significantly higher PSQI (9.00 vs. 7.00, p = 0.001) and MPSS (18.41 vs. 15.37, *p * 0.001) scores than the non-PPD group.
Table 1.: Comparison of general information between PPD and non-PPD groups.
Comparison of Uterine Recovery Effects
No significant difference was noticed in the height of uterine fundal descent
between the PPD and non-PPD groups at 24 and 48 h postpartum (*p *
0.05) (Table 2). However, the lochia volume in the PPD group was significantly
less than that in the non-PPD group at 24 (*p *
0.001) and 48 h
(*p *
0.001) postpartum.
Comparison of Pelvic Floor Muscle Strength Recovery
At 6 weeks postpartum, the PPD group exhibited a poorer pelvic floor muscle strength recovery, as evidenced by significantly higher proportions of grades I (p = 0.033) and II (p = 0.028) muscle strength than in the non-PPD group, whereas the proportion of those with muscle strength grade III (*p * 0.001) was significantly lower (Table 3).
Univariate Logistic Regression Analysis of PPD
Univariate and subsequent multivariate logistic regression analyses were
performed to identify factors independently associated with PPD. The dependent
variable was the presence of PPD, defined as an EPDS score 10.
Independent variables included all demographic, obstetric and postnatal
characteristics listed in Table 1 and uterine recovery parameters (uterine fundal
height decline and lochia volume) and pelvic floor muscle strength. Univariate
logistic regression analysis showed that high school and below literacy
(p = 0.011), disharmony with husband (p = 0.019), illness
during pregnancy (p = 0.008), newborns in poor health (p =
0.019) and higher PSQI (p = 0.002) and MPSS scores (*p *
0.001) were significantly associated with a high risk of PPD (Table 4). In
addition, having regular prenatal check-ups (p = 0.023), high lochia
volume at 24 (p = 0.001) and 48 h (*p *
0.001) and pelvic
floor muscle strength grade III (p = 0.003) were associated with
a reduced risk of PPD reduction.
Multivariate Logistic Regression Analysis of PPD
Multivariate logistic regression analysis showed that high school and below literacy (OR = 2.33, 95% CI: 1.05 to 5.18, p = 0.039), illness during pregnancy (OR = 2.91, 95% CI: 1.09 to 7.78, p = 0.033), and high PSQI (OR = 1.20, 95% CI: 1.04 to 1.39, p = 0.013) and MPSS scores (OR = 1.11, 95% CI: 1.03 to 1.20, p = 0.005) were independent risk factors for PPD (Table 5). By contrast, a higher lochia volume at 24 (OR = 0.97, 95% CI: 0.95 to 0.99, p = 0.016) and 48 h (OR = 0.82, 95% CI: 0.75 to 0.89, *p * 0.001) and pelvic floor muscle strength grade III (OR = 0.25, 95% CI: 0.08 to 0.80, p = 0.020) served as protective factors.
Evaluation of Multifactor Models
The VIF values of all variables in the multivariate logistic regression model were less than 5, which indicates that no collinearity was observed among the variables (Table 5). Fig. 1 shows the ROC curve based on the multivariate logistic regression model. The AUC of the multivariate logistic regression model was 0.88, which implies that this model has a high discriminatory capability for the PPD population. Fig. 2 illustrates the calibration curve of this model. No significant difference was recorded between the observed and predicted values of this model, which indicates that the model had a good fit.
ROC curve based on the logistic regression model. Abbreviation: ROC, receiver operating characteristic; AUC, area under the curve.
Calibration curve based on the logistic regression model.
Discussion
PPD is a common mental disorder in the postpartum period, and it seriously affects maternal physical and mental health and the mother–infant relationship [1]. This study analysed the association of PPD with uterine recovery, sleep quality and postpartum stress through a retrospective analysis of 194 primiparous women. The results show that the depressed group differed significantly from the nondepressed group in terms of literacy, couple relationship, regularity of antenatal checkups, the presence of illnesses during pregnancy and health status of the newborn and had higher scores on the PSQI and MPSS. Meanwhile, the depressed group had less lochia volume and poorer recovery of pelvic floor muscle strength. Logistic regression analysis showed that sleep quality, postnatal stress, uterine recovery indicators (lochia volume and pelvic floor muscle strength) and sociodemographic factors independently influenced postnatal depression.
Firstly, the results of the study show that some demographic characteristics were significantly associated with PPD. In this work, the risk of PPD among primiparous women with a high school education or less was 2.33 times higher than that among those with a specialist education or above. Jimènez-Barragan et al. [24] also reported through a prospective study that educational level is one of the risk factors for depression during pregnancy. This condition may be related to the limited access of mothers with low educational attainment to scientific childcare knowledge and their weaker psychological adjustment ability. The low-education group is more likely to be frustrated by neonatal care problems, and they are less aware of PPDand lack the awareness to actively seek professional help [25]. The risk of depression among parturients with disharmonious marital relationships is significantly increased, which suggests that having a family support system is crucial for postpartum mental health. Fang et al. [26] also stated through a study of 151 parturients that marital disharmony is an independent risk factor for PPD, which is consistent with the results of this study. A close and harmonious marital relationship can provide emotional support and relieve the parenting pressure of new mothers. However, tense relationships may lead to emotional isolation of new mothers and intensify negative emotions [27]. In addition, a history of illness during pregnancy is significantly associated with PPD, which may be caused by illnesses during pregnancy that increased the mother’s concern for her own health and that of the foetus, leading to prenatal anxiety that carries over into the postpartum period [28]. Mothers with poor neonatal health are at high risk of PPD, which may be associated with infant and child health problems that increase the burden of care on the mother and trigger anxiety [26]. Regular antenatal check-ups are a protective factor, probably because they help mothers to obtain timely health guidance and reduce unknown fears about labour and the postnatal period, reflecting the importance of perinatal care in mental health interventions.
In the present study, although no significant difference was observed in the height of uterine fundal descent between the depressed and non-depressed groups, the former had significantly less lochia volume and a lower proportion of pelvic floor muscle strength grade III at 24 and 48 h postpartum. A reduced lochia volume may reflect poor uterine contraction or delayed endothelial repair. We speculate that this physiological abnormality can be linked to mental health through several potential pathways: firstly, by directly contributing to physical discomfort, which may correlate with reduced maternal quality of life; secondly, through its potential association with inflammatory processes, as pro-inflammatory cytokines (e.g., interleukin-6, tumour necrosis factor-alpha) correlate with depressive states [29, 30]. However, the cross-sectional nature of our data cannot rule out the possibility of reverse causality, whereby PPD symptoms may influence physical recovery. In addition, the risk of PPD is high in women with poor recovery of pelvic floor muscle strength (grade I or II). Impaired pelvic floor muscle function may lead to urinary incontinence or sexual dysfunction, which further aggravates the psychological burden [8, 31]. By contrast, the protective effect of pelvic floor muscle strength grade III may be associated with high maternal satisfaction with recovery, which helps to enhance postnatal self-confidence and emotional stability of mothers.
PSQI and MPSS scores were significantly higher in the depressed group than in the non-depressed group, and multifactorial analyses showed both to be independent risk factors. Baattaiah et al. [32] reported through a cross-sectional study the significantly positive correlation of PSQI score with the EPDS score, which means that mothers with poor sleep quality has a high risk of developing PPD. Postpartum sleep disturbances may be related to factors, such as changes in hormone levels, the need to breastfeed at night and care of the newborn, which together contribute to disrupted maternal sleep and reduced sleep quality [33]. Chronic sleep deprivation has been theorised to interfere with normal brain function and emotion regulation, which can increase the vulnerability to depression [29, 30]. Nevertheless, pre-existing depressive symptoms contribute to the poor sleep quality observed. Postnatal stress may arise from role changes, adjustments in family relationships and childcare responsibilities [34]. These stresses, if not effectively relieved, may further aggravate the maternal psychological burden and lead to depression [35].
Based on our findings, we propose a more integrated and proactive clinical approach. Firstly, for early identification of high-risk primiparas, routine postpartum care at the 42-day check-up should be expanded to include not only physical examination but also brief, standardised screenings for PPD (e.g., using the EPDS), sleep quality (e.g., using 1–2 key questions from the PSQI scale) and postpartum stress. Crucially, clinicians should be alerted that women presenting with objective signs of suboptimal physiological recovery—specifically, a history of scanty lochia in the immediate postpartum period or poor pelvic floor muscle strength (below Grade III) at the examination—constitute a key high-risk subgroup warranting closer psychological assessment. Secondly, regarding the timing of intervention, our results underscore the importance of the entire early postpartum period. Although the 42-day check-up is a critical window for formal screening, awareness and supportive interventions should begin earlier. Before discharge, mothers—especially those with lower education or a history of pregnancy illness—can receive preemptive education on normative recovery and mental health. Following discharge, community health workers can conduct proactive follow-ups within the first two weeks to assess sleep challenges and stress levels to provide initial support and facilitate referral if needed. This stepped-care model, which integrates physiological indicators with psychosocial screening across the postpartum continuum, can considerably improve the precision and effectiveness of PPD prevention.
This study encountered some limitations. Firstly, its retrospective, cross-sectional design precluded causal inference; thus, we cannot determine whether poor uterine recovery precipitates PPD, or vice versa. Secondly, the sample was modest and recruited from a single tertiary centre, which might have introduced selection bias and limit external validity. Thirdly, we examined the main effects only and did not test potential interactions (e.g., sleep quality postpartum stress) that can reveal synergistic pathways to PPD. Fourthly, survivorship bias is possible: women with severe depressive symptoms are less likely to attend the 42-day visit, which potentially underestimates PPD prevalence and attenuating risk estimates. Fifthly, uterine involution was assessed clinically (fundal height and lochia volume) rather than by transvaginal ultrasound, which might have reduced sensitivity in detecting subtle subinvolution. Finally, unmeasured confounders—such as inflammatory cytokines or sex-steroid fluctuations—may residualise observed associations. Future prospective, multicentre cohorts incorporating objective imaging and biomarkers are needed to clarify the temporal sequence and biological mechanisms linking physiological recovery with postpartum mental health.
Conclusions
This study identified psychosocial–physiological risk factors (lower education, illness during pregnancy, poor sleep quality and high postpartum stress) and physiological protective factors (adequate early lochia volume and good pelvic floor muscle recovery) for PPD in primiparous women. The findings underscore the multifactorial nature of PPD and highlight the critical importance of an integrated approach to postpartum care that addresses mental health and physical recovery. Future research should focus on verifying these associations longitudinally and exploring their underlying mechanisms to inform effective prevention and treatment strategies.
Availability of Data and Materials
The datasets generated and analyzed during the current study are not publicly available due to patient privacy and confidentiality considerations but are available from the corresponding author on reasonable request. Requests for data access should be directed to the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dennis CL Singla DR Brown HK Savel K Clark CT Grigoriadis S et al Postpartum Depression: A Clinical Review of Impact and Current Treatment Solutions Drugs 20248464565910.1007/s 40265-024-02038-z 38811474 · doi ↗ · pubmed ↗
- 2Miller LJ Postpartum depression JAMA 200228776276510.1001/jama.287.6.76211851544 · doi ↗ · pubmed ↗
- 3Wang Z Liu J Shuai H Cai Z Fu X Liu Y et al Mapping global prevalence of depression among postpartum women Translational Psychiatry 20211154310.1038/s 41398-021-01663-634671011 PMC 8528847 · doi ↗ · pubmed ↗
- 4Suryawanshi O 4th Pajai S A Comprehensive Review on Postpartum Depression Cureus 202214 e 3274510.7759/cureus.3274536686097 PMC 9851410 · doi ↗ · pubmed ↗
- 5Li X Musoba PM Zhou X Lai S Yang W Wang LN et al Recovery of uterine and ovarian function in patients with complete placenta previa after caesarean delivery: A retrospective study Medicine 2021100 e 2419610.1097/MD.000000000002419633466195 PMC 7808485 · doi ↗ · pubmed ↗
- 6Giouleka S Tsakiridis I Kostakis N Boureka E Mamopoulos A Kalogiannidis I et al Postnatal Care: A Comparative Review of Guidelines Obstetrical & Gynecological Survey 20247910512110.1097/OGX.000000000000122438377454 · doi ↗ · pubmed ↗
- 7Muganyizi PS Kimario GF Rwegoshora FJ Paul PP Makins A Impact of immediate postpartum insertion of T Cu 380A on the quantity and duration of lochia discharges in Tanzania Contraception and Reproductive Medicine 2021610.1186/s 40834-020-00145-2PMC 778396933397504 · doi ↗ · pubmed ↗
- 8De Lancey JOL Masteling M Pipitone F La Cross J Mastrovito S Ashton-Miller JA Pelvic floor injury during vaginal birth is life-altering and preventable: what can we do about it? American Journal of Obstetrics and Gynecology 2024230279294.e 210.1016/j.ajog.2023.11.125338168908 PMC 11177602 · doi ↗ · pubmed ↗