Influencing Factors, Construction and Verification of a Nomogram Model for Adolescent Depression With Nonsuicidal Self-Injury Behaviour
Fanfan Lu, Meihua Li, Zhengmao Cai, Xinxin Huang

TL;DR
This study builds and validates a prediction model to identify adolescents with depression who are at risk of nonsuicidal self-injury, helping with early intervention.
Contribution
A novel nomogram model is developed and validated for predicting nonsuicidal self-injury in adolescents with depression.
Findings
The model identified factors like parental relationship, depression severity, and childhood trauma as significant predictors of NSSI behavior.
The nomogram model showed high accuracy in both training and verification sets with C-index values of 0.936 and 0.923, respectively.
The model's high sensitivity and specificity suggest strong potential for clinical application in early detection.
Abstract
Adolescent depression with nonsuicidal self-injury (NSSI) is a serious public health issue. NSSI involves intentional self-harm without suicidal intent and is common amongst depressed teens, leading to considerable psychological and physical risks. Early detection and intervention are essential to reduce these risks. To explore the influencing factors of adolescent depression with NSSI behaviour and construct a nomogram prediction model and verify its clinical application value. From January 2023 to April 2025, 136 cases of adolescent depression admitted to our hospital were selected. Patients were randomly divided into training (n = 95) and verification (n = 41) sets in a 7:3 ratio. Multivariate logistic regression was used to analyse the risk factors of NSSI behaviour in the training set, and a nomogram prediction model was constructed. Receiver operating characteristic (ROC) and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
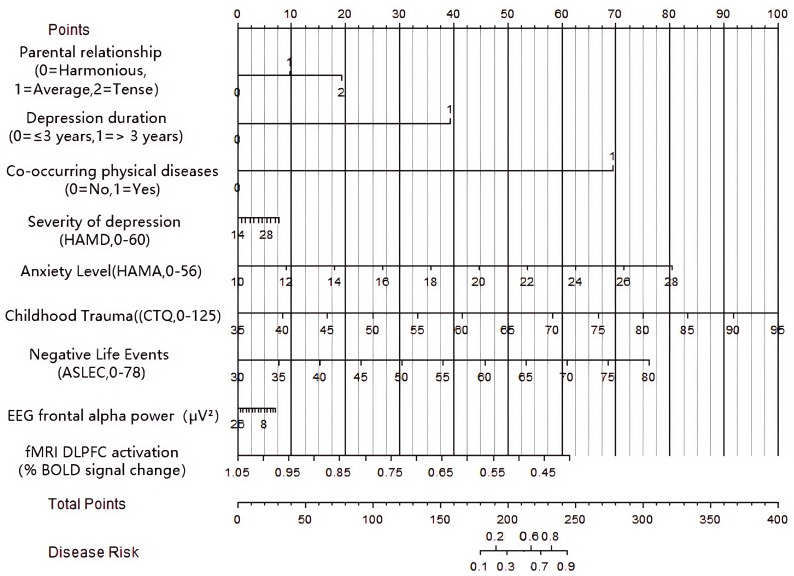 Fig. 1
Fig. 1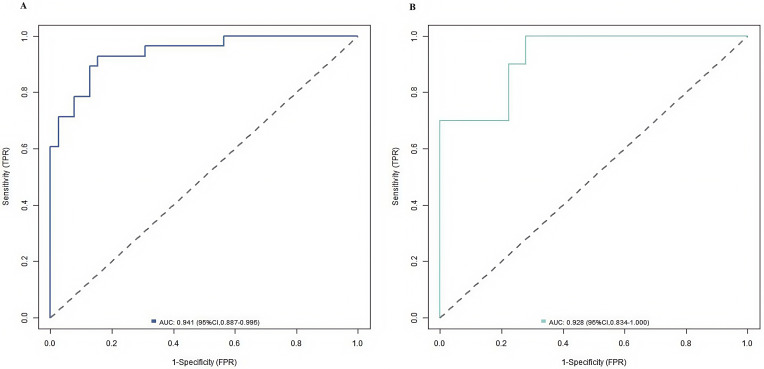 Fig. 2
Fig. 2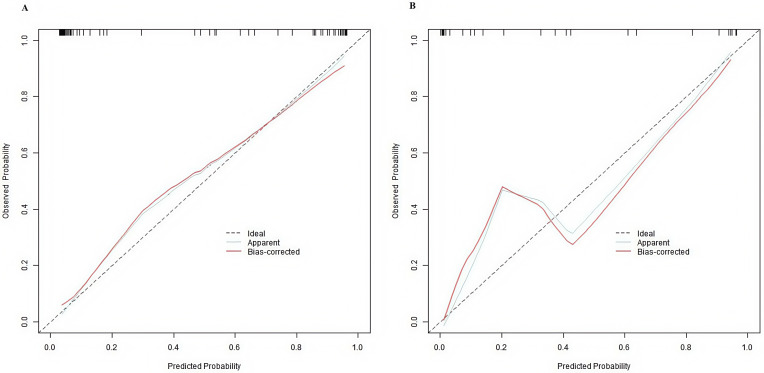 Fig. 3
Fig. 3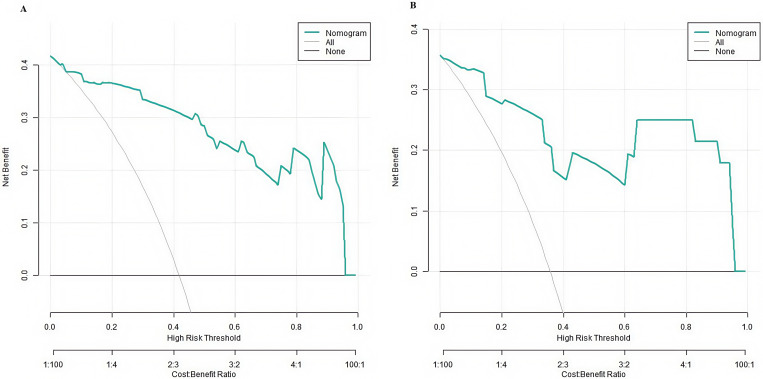 Fig. 4
Fig. 4| Index | Training set (n = 95) | Verification set (n = 41) |
|
| |
| Age ( | 15.32 | 15.03 | 0.883 | 0.378 | |
| Gender [n (%)] | Male | 45 (47.37) | 18 (43.90) | 0.138 | 0.709 |
| Female | 50 (52.63) | 23 (56.10) | |||
| Family type [n (%)] | Nuclear family | 60 (63.16) | 21 (51.22) | 2.107 | 0.550 |
| Single parent family | 15 (15.79) | 7 (17.07) | |||
| Reconstituted family | 10 (10.53) | 7 (17.07) | |||
| Other | 10 (10.53) | 6 (14.63) | |||
| Parental relationship [n (%)] | Harmonious | 40 (42.11) | 18 (43.90) | 0.116 | 0.943 |
| Average | 40 (42.11) | 16 (39.02) | |||
| Tense | 15 (15.79) | 7 (17.07) | |||
| Depression duration [n (%)] | 65 (68.42) | 31 (75.61) | 0.712 | 0.398 | |
| 30 (31.58) | 10 (24.39) | ||||
| Residence [n (%)] | Rural | 30 (31.58) | 12 (29.27) | 0.071 | 0.789 |
| Urban | 65 (68.42) | 29 (70.73) | |||
| Only child [n (%)] | Yes | 51 (53.68) | 19 (46.34) | 0.618 | 0.431 |
| No | 44 (46.32) | 22 (53.66) | |||
| Left behind experience [n (%)] | Yes | 20 (21.05) | 9 (21.95) | 0.013 | 0.906 |
| No | 75 (78.95) | 32 (78.05) | |||
| History of trauma [n (%)] | Yes | 16 (16.84) | 6 (14.63) | 0.103 | 0.748 |
| No | 79 (83.58) | 35 (85.37) | |||
| Co-occurring physical diseases [n (%)] | Yes | 27 (28.42) | 12 (29.27) | 0.010 | 0.919 |
| No | 68 (71.58) | 29 (70.73) | |||
| Severity of depression ( | 22.36 | 23.24 | 1.284 | 0.201 | |
| Anxiety level ( | 18.61 | 19.34 | 1.326 | 0.186 | |
| Childhood trauma ( | 68.95 | 69.03 | 0.047 | 0.962 | |
| Negative life events ( | 55.68 | 56.42 | 0.518 | 0.605 | |
| EEG frontal | 12.36 | 12.14 | 0.321 | 0.748 | |
| fMRI-DLPFC activation (% BOLD signal change) | 0.85 | 0.87 | 0.623 | 0.533 | |
| Incidence of NSSI [n (%)] | Yes | 38 (40.00) | 15 (36.59) | 0.140 | 0.707 |
| No | 57 (60.00) | 26 (63.41) | |||
| Index | NSSI group (n = 38) | Non-NSSI group (n = 57) |
|
| |
| Age ( | 15.03 | 15.10 | 0.229 | 0.819 | |
| Gender [n (%)] | Male | 17 (44.74) | 25 (43.86) | 0.007 | 0.932 |
| Female | 21 (55.26) | 32 (56.14) | |||
| Family type [n (%)] | Nuclear family | 17 (44.74) | 38 (66.67) | 4.543 | 0.208 |
| Single-parent family | 8 (21.05) | 7 (12.28) | |||
| Reconstituted family | 7 (18.42) | 6 (10.53) | |||
| Other | 6 (15.79) | 6 (10.53) | |||
| Parental relationship [n (%)] | Harmonious | 10 (26.32) | 30 (52.63) | 12.210 | 0.002 |
| Average | 12 (31.58) | 20 (35.09) | |||
| Tense | 16 (42.11) | 7 (12.28) | |||
| Depression duration [n (%)] | 18 (43.37) | 40 (70.18) | 4.987 | 0.025 | |
| 20 (52.63) | 17 (29.82) | ||||
| Residence [n (%)] | Rural | 14 (36.84) | 23 (40.35) | 0.118 | 0.731 |
| Urban | 24 (63.16) | 34 (59.65) | |||
| Only child [n (%)] | Yes | 19 (50.00) | 32 (56.14) | 0.345 | 0.556 |
| No | 19 (50.00) | 25 (43.86) | |||
| Left behind experience [n (%)] | Yes | 8 (21.05) | 14 (24.56) | 0.157 | 0.691 |
| No | 30 (78.95) | 43 (75.44) | |||
| History of trauma [n (%)] | Yes | 6 (15.79) | 11 (19.30) | 0.191 | 0.662 |
| No | 32 (84.21) | 46 (80.70) | |||
| Co-occurring physical diseases [n (%)] | Yes | 9 (23.68) | 4 (7.02) | 5.361 | 0.020 |
| No | 29 (76.32) | 53 (92.98) | |||
| Severity of depression ( | 24.64 | 22.20 | 2.690 | 0.008 | |
| Anxiety level ( | 19.15 | 17.54 | 2.268 | 0.025 | |
| Childhood trauma ( | 75.12 | 65.68 | 5.896 | 0.001 | |
| Negative life events ( | 58.75 | 50.36 | 4.934 | 0.001 | |
| EEG frontal | 10.24 | 12.80 | 2.822 | 0.005 | |
| fMRI-DLPFC activation (% BOLD signal change) | 0.71 | 0.81 | 3.786 | 0.001 | |
| Index | Meaning | Assignment/measurement scale |
| Parental relationship | State of parent interaction in the family | 0 = harmonious, 1 = average, 2 = tense |
| Depression duration | Duration of depression | 0 = |
| Co-occurring physical diseases | Are there any other physical diseases? | 0 = no, 1 = yes |
| Severity of depression | Severity of depressive symptoms | Continuous variable (HAMD score, ranging from 0 to 60) |
| Anxiety level | Severity of anxiety symptoms | Continuous variable (HAMA score, ranging from 0 to 56) |
| Childhood trauma | Severity of traumatic events experienced in childhood. | Continuous variable (CTQ score, ranging from 0 to 125 [ |
| Negative life events | Influence degree of negative life events | Continuous variable (ASLEC score, ranging from 0 to 78 [ |
| EEG frontal | Power of frontal lobe | Continuous variable (unit: µV2) |
| fMRI-DLPFC activation | Power of frontal lobe | Continuous variable (unit: % BOLD signal change) |
| NSSI occurrence | Is there any nonsuicidal self-injury behaviour? | None = 0, yes = 1 |
| Factor | B | Standard error | Wald |
| OR | 95% CI | Collinear statistics | |
| Tolerance | VIF | |||||||
| Parental relationship (average vs. harmonious), [n (%)] | 0.523 | 0.132 | 4.012 | 0.132 | 1.682 | 1.305–2.168 | 0.287 | 3.749 |
| Parental relationship (tense vs. harmonious), [n (%)] | 0.662 | 0.271 | 5.950 | 0.015 | 1.939 | 1.139–3.300 | ||
| Depression duration ( | 0.961 | 0.435 | 4.877 | 0.027 | 2.614 | 1.114–6.135 | 0.317 | 3.151 |
| Severity of depression (HAMD, | 0.137 | 0.052 | 6.875 | 0.009 | 1.147 | 1.035–1.270 | 0.676 | 1.478 |
| Anxiety level (HAMA, | 0.139 | 0.066 | 4.438 | 0.035 | 1.149 | 1.010–1.307 | 0.865 | 1.156 |
| Childhood trauma (CTQ, | 0.097 | 0.025 | 14.513 | 0.001 | 1.102 | 1.048–1.158 | 0.911 | 1.098 |
| Negative life events (ASLEC, | 0.132 | 0.033 | 15.565 | 0.001 | 1.141 | 1.069–1.218 | 0.895 | 1.117 |
| Co-occurring physical diseases (yes, [n (%)]) | 1.414 | 0.644 | 4.824 | 0.028 | 4.112 | 1.164–14.523 | 0.728 | 1.373 |
| EEG frontal | −0.142 | 0.053 | 7.214 | 0.007 | 0.868 | 0.782–0.962 | 0.927 | 1.079 |
| fMRI DLPFC activation (% BOLD signal change) | −4.261 | 1.731 | 6.058 | 0.014 | 0.014 | 0.001–0.420 | 0.961 | 1.041 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSuicide and Self-Harm Studies · Personality Disorders and Psychopathology · Mental Health Research Topics
Introduction
Adolescence is a critical stage of human development. However, the incidence of adolescent depression, which poses a serious threat to the physical and mental health of adolescents, is increasing annually [1]. Adolescent depression with nonsuicidal self-injury (NSSI) behaviour has aroused widespread concern. NSSI behaviour refers to the intentional and repetitive injury, such as cutting, biting, scratching or hitting, to one’s body tissue without the intent to commit suicide [2]. This behaviour, which is common in patients with adolescent depression, not only exacerbates their suffering and healthcare burden but also elevates the risk of suicide, thereby dealing a heavy blow to families and society. This kind of behaviour is common in patients with adolescent depression, and its occurrence is closely related to risk factors under various theoretical frameworks. For example, family environment theory points out that tension between parents can destroy the emotional support system of adolescents, and previous studies have shown that family conflicts are significantly related to NSSI [3]. Traumatic stress theory holds that childhood trauma affects an individual’s ability to cope with stress by changing the development of the emotional regulation centre of the brain [4]. Life event theory states that negative life events can aggravate depressive symptoms and reduce psychological resilience. this effect then becomes the direct cause of NSSI [5]. According to emotional disorder theory, the degree of depression and anxiety directly reflects the disorder of an individual’s emotional regulation, and the comorbid state of high depression and anxiety is the core predictor of NSSI [6]. At present, the research on forecasting models has developed from single-factor analysis to multidimensional integration. For example, Șipoș et al. [5] built a machine learning–based risk model of adolescent NSSI. However, they only included psychosocial factors and did not combine clinical indicators. These models generally have the problems of high sample heterogeneity and insufficient clinical operability. In particular, they lack specific prediction tools for adolescent depression groups. New evidence shows that NSSI affects 12%–20% of teenagers around the world, and the prevalence rate of patients with depression is as high as 40%. NSSI behaviour not only leads to direct physical injuries, such as infections and scarring, but also causes long-term psychological problems, such as enhanced suicidal ideation and emotional adjustment disorder [7].
Although NSSI in depressed adolescents is a major public health challenge, doubling the risk of suicide attempts and imposing heavy burdens on families and society, the specific pathogenic pathway between adolescent depression and NSSI remains unclear. Existing studies mostly focus on isolated risk factors, such as family conflict and trauma, and lack a comprehensive predictive framework [8, 9]. This study aims to explore the influencing factors of NSSI in adolescents with depression and construct a validated nomogram prediction model. As a visual tool, this model integrates multidimensional risk factors (including psychosocial characteristics, clinical indicators and neuroimaging data) to provide clinicians with intuitive risk prediction results, filling the gap in NSSI prediction tools for adolescents with depression. It offers a quantitative basis for early intervention, ultimately contributing to the enhanced protection and promotion of adolescent mental health and reduced adverse outcomes.
Materials and Methods
Materials
A total of 136 patients with adolescent depression were selected from January 2023 to April 2025. All patients met the diagnostic criteria for major depressive disorder as defined by the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) and provided voluntary informed consent. Subsequently, using a screening for non-suicidal self-injury (NSSI) behavior (defined as 5 episodes of self-injury in the past year), the patients were divided into two groups: the NSSI group (n = 53, with definite self-injury behavior) and the control group (n = 83, without self-injury behavior) [5]. Sample size estimation was based on the principle of the number of variables required by the logistic regression model in previous literature (each independent variable needs at least 10–15 samples). This study hypothesized seven potential risk factors (including parental relationships, prolonged depression, physical comorbidities, severe depressive and anxiety symptoms, childhood trauma, and negative life events) and the expected sample size needed 70–105 samples. In consideration of a shedding rate of 20%, 136 cases were finally included. Inclusion criteria included the following: (1) aged between 12–18 years. (2) met the diagnostic criteria for depression in the DSM-5 [10]. and (3) patients and their families were informed and agreed to cooperate with the investigation. Exclusion criteria encompassed the following: (1) co-occurring other mental disorders or physical diseases. (2) history of suicidal behaviour. (3) inability to complete the questionnaires because of intellectual disabilities (such as mild or severe intellectual disability and autism spectrum disorder). and (4) participation in a study and evaluation of the influence of or suffering from serious physical diseases (such as malignant tumours and organ failure). This research strictly followed the ethical guidelines of the Helsinki Declaration. All data were anonymised (identifiers, such as name and ID number, were deleted and replaced with research IDs), and only researchers were authorised to access the data. The patient and their legal guardian signed the informed consent form, which was approved by the affiliated kangning hospital of wenzhou medical university ethics committee (approval number: YJ-2025-11-02).
Both groups excluded those who had attempted suicide. Patients were randomly divided into the training (n = 95) and validation (n = 41) sets in a 7:3 ratio. The sample size met the requirement of 10–15 samples per independent variable (seven factors), ensuring statistical power. Internal validation was performed to assess model stability.
Methods
Data Collection
Demographic data included gender, age, ethnicity, family type, parental relationship, place of residence, only-child status and history of being left behind.
Clinical features comprised age of onset, duration of illness, history of trauma, presence of co-occurring physical illness, severity of depression and level of anxiety. The severity of depression was assessed by employing the Hamilton Depression Rating Scale (HAMD) [11], and the level of anxiety was assessed by using the Hamilton Anxiety Scale (HAMA) [12].
Psychosocial factors encompassed childhood trauma, negative life events, family relationships and social support. Childhood trauma was assessed by using the Childhood Trauma Questionnaire (CTQ) [4], and negative life events were assessed with the Adolescent Life Events Scale (ASLEC) [13].
Neurobiological measures were acquired as follows: 64-channel Electroencephalogram (EEG) (Brain Products GmbH, Gilching, Germany): Resting-state brain activity was recorded at a sampling rate of 1000 Hz with Ag/AgCl electrodes placed in accordance with the International 10–20 System. EEG frontal power was measured bilaterally, and the average value was used for analysis (unit: µV^2^). 3T frontal power, functional Magnetic Resonance Imaging (fMRI) (model: MAGNETOM Prisma, Siemens Healthineers, Erlangen, Germany): During functional scanning, participants completed an emotional face processing task (presenting angry/happy neutral faces). Blood-oxygen-level-dependent (BOLD) signals were acquired by using a T2*-weighted echo planar imaging sequence (TR/TE = 2000/30 ms, 64 64 matrix, 33 axial slices). Amygdala and dorsolateral prefrontal cortex (DLPFC) (Unit: % BOLD signal change) activation was analysed by using SPM12 (Version 12. Wellcome Trust Centre for Neuroimaging, London, UK).
HAMD
The HAMD is a classic tool for evaluating the severity of depressive symptoms. It is widely used in psychiatric clinical and scientific research fields. Although it was originally developed for adults, previous studies have verified its applicability in adolescents and proved its good internal consistency (Cronbach’s = 0.82–0.89) and convergence effectiveness with child-specific scales, such as the Child Depression Scale [11]. Its items are diverse, covering a wide range of dimensions, such as low mood (frequency of despair), loss of interest (diminished enthusiasm), sleep disorders (difficulty falling asleep and sleep quality), appetite changes (fluctuations in appetite and weight) and suicidal ideation (presence and intensity). On the basis of a standardised process, symptoms are scored on a 0–4 scale, with total scores ranging from 0 to 60. Mild depression (8–17 points) has slight symptoms and slightly disturbed functioning. moderate depression (18–24 points) has considerable functional impairment, making daily tasks difficult. and severe depression ( 25 points) has severely impaired functioning, almost losing self-care ability, with a dramatically increased risk of suicide.
HAMA
HAMA is a key tool for measuring anxiety levels. It precisely dissects somatic and psychic anxiety [12]. Cross-cultural validation studies amongst Asian teenagers reported acceptable reliability (intraclass correlation coefficient = 0.78–0.85) and structural validity, although the wording of the project (such as ‘work difficulty’) was suitable for the background of teenagers. Somatic anxiety includes muscle tension (location, frequency and intensity), such as shoulder pain episodes. cardiovascular symptoms (palpitation frequency and severity). respiratory symptoms (shortness of breath). and gastrointestinal symptoms (frequency of nausea and abdominal pain). Psychic anxiety focuses on anxious mood (duration and intensity of worry and fear), tension (restlessness and irritability) and panic attacks (presence and characteristics). Scores are aggregated on a 0–4 scale, with a total score ranging from 0 to 56. Typically, mild anxiety (7–13 points) involves occasional anxiety experiences without remarkable life disruption. moderate anxiety (14–20 points) involves frequent anxiety symptoms, with some functional impairment. and severe anxiety (21 points and above) is generalised, with near-paralysis in various aspects of life, urgently needing intervention for relief.
CTQ
CTQ is designed to assess the severity of childhood trauma across five dimensions: emotional abuse (frequent verbal humiliation), physical abuse (details of physical punishment and beating), sexual abuse (frequency and nature of contact), emotional neglect (indifference to emotional needs) and physical neglect (degree of inadequate care). It consists of 28 items scored on a five-point Likert scale (total score range: 25–125) [4]. High scores indicate severe experiences of childhood trauma. In this study, CTQ scores were evaluated on the basis of the total score: a score below 40 indicates mild trauma, that between 40 and 79 specifies moderate trauma and that of 80 or above reflects severe trauma.
ASLEC
ASLEC evaluates negative life events on a 0–6 scale (total score range: 0–78) [13]. It systematically evaluates the impact of negative life events across multiple domains, including academics (e.g., exam failure and heavy academic pressure), interpersonal relationships (e.g., conflicts, bullying and strained relationships), family (e.g., crises or changes) and health (e.g., serious or chronic illnesses). Each event is rated on a 0–6 scale to assess its occurrence and the degree of psychological and life impact on the adolescent. High total scores reflect a strongly negative influence. Total scores below 35 indicate mild impact, typically presenting as temporary emotional fluctuations that can be self-regulated. scores between 35 and 65 suggest moderate impact, with noticeable emotional and behavioural changes and partial functional impairment requiring long recovery. and scores above 65 indicate severe impact, potentially leading to stress-related disorders and requiring professional intervention to restore psychological balance. The scale is useful for identifying high-risk adolescents and providing targeted guidance for psychological support.
Statistical Analysis
SPSS 26.0 (IBM, Armonk, New York, USA) software was used for data analysis. The Kolmogorov–Smirnov test was conducted to test normality. Measurement data conforming to the normal distribution were expressed as means with standard deviations ( s), and the independent samples t-test was employed for comparison between groups. Data with nonnormal distribution were analysed after logarithmic transformation or expressed as medians (interquartile interval), and the Mann–Whitney U test was employed for comparison between groups. Categorical variables were presented as frequencies and percentages, with group differences assessed through the ^2^ test. Univariate and multivariate logistic regression analyses were conducted to identify factors influencing depression amongst adolescents with NSSI behaviour. R software (version 3.5.2, R Foundation, Vienna, Austria) was employed to standardise continuous variables (depression severity, anxiety, trauma, life events, EEG wave power and functional Magnetic Resonance Imaging-Dorsolateral Prefrontal Cortex (fMRI-DLPFC) activation) to z-scores, and a nomogram model based on regression coefficient allocation point values was constructed by utilising the lrm function. Model performance was evaluated by utilising the C-index, calibration curve (Hosmer–Lemeshow test) and decision curve analysis (DCA) with the help of Receiver Operating Characteristic (ROC) and the decision curve package. Two-sided *p * 0.05 was considered statistically significant.
Results
Comparison of the Incidence and Clinical Characteristics of NSSI
Behaviour Between the Training and Verification Sets
In the training set of 95 patients, 38 (40.00%) exhibited NSSI behaviour, whereas in the validation set of 41 patients, 15 (36.59%) showed this behaviour. No significant differences were found in incidence and clinical characteristics between the training and verification sets (*p * 0.05), as shown in Table 1.
Table 1.: Comparison of clinical characteristics between the training and verification sets.
Associated Factor Analysis for NSSI in the Training Set
As shown in Table 2, the results of univariate analysis revealed that non-NSSI patients and patients with NSSI differed significantly in terms of parental relationship, depression duration, co-occurring physical diseases, depression severity, anxiety level, childhood trauma, EEG frontal power, fMRI-DLPFC activation and negative life events (*p * 0.05). Further multivariate logistic regression analysis was conducted with NSSI occurrence as the dependent variable (0 = no, 1 = yes) and factors with *p * 0.05 from the univariate analysis as covariates (Table 3, Ref. [4, 13]). The results of multivariate logistic regression analysis are shown in Table 4.
Table 4.: Multivariate logistic regression analysis for NSSI occurrence in the training set.
Establishment of the NSSI Prediction Model
Continuous variables (depression severity, childhood trauma and negative life events) in the training set were tested for linear correlations on the basis of previous research evidence (such as those reported by Irniger C et al. [4]) and clinical professional cognition to judge the relationship between variables and the probability of NSSI. The results revealed an approximate linear correlation between continuous variables and NSSI risk (*p * 0.05), and nonlinear transformation was not needed. On the basis of this result, the multivariate logistic regression analysis showed that tension with parents, long depression course, physical illness, high depression degree, high anxiety degree, childhood trauma, EEG frontal power, fMRI-DLPFC activation and negative life events are the related factors of NSSI behaviour. For classified variables, the predictive contribution score was calculated in accordance with the coefficient of logistic regression: the value of each classification level was converted into the corresponding score (score = value/minimum value 100). For example, the score of ‘nervousness’ ( = 0.662) in the parent–child relationship variable was (0.662/0.132) 100 50. The score of ‘average’ ( = 0.421) was (0.421/0.132) 100 32. Furthermore, to accurately estimate the predictive contribution of each category, we used effects coding (or contrast coding) instead of simple dummy coding (0–1). In this model, the ‘harmony’ category was designated as the reference group and assigned a value of 0 for comparison. This approach ensures that the coefficient for each other category represents its deviation from the overall mean, providing a more interpretable measure of its unique effect. Finally, the nomogram prediction model was constructed on the basis of the above score distribution. This method ensures that the length of the score axis of each variable in the nomogram is proportional to the coefficient, and the positive/negative direction of the coefficient is reflected by the direction of the score axis (the right is a positive coefficient and the left is a negative coefficient). The model was constructed on the basis of the above standardised score distribution. The total score was used to predict the probability of NSSI, and a high total score is indicative of high prediction accuracy. Each related factor in the model was assigned points, and the total score of predicting NSSI was calculated and reflected by the probability of predicting NSSI. A high total score indicates the high accuracy of predicting NSSI in patients with adolescent depression (Fig. 1).
Nomogram prediction model for NSSI occurrence in patients with adolescent depression. NOTE: NSSI, nonsuicidal self-injury; VIF, Variance Inflation Factor; HAMD, Hamilton Depression Rating Scale; CTQ, Childhood Trauma Questionnaire; ASLEC, Adolescent Self-Rating Life Events Checklist; EEG, Electroencephalography; fMRI-DLPFC, functional Magnetic Resonance Imaging-Dorsolateral Prefrontal Cortex.
Evaluation and Verification of the NSSI Prediction Model
The nomogram model showed good calibration and fit on the training and verification sets (C-index values of 0.936 [95% CI: 0.887–0.995] and 0.923 [95% CI: 0.834–1.000]. average absolute errors between predicted and actual values of 0.092 and 0.105. and Hosmer–Lemeshow test p values of 0.452 and 0.523). ROC curves indicated that the area under the curve of the nomogram model in predicting NSSI behaviour in patients with adolescent depression in the training and verification sets were 0.941 (95% CI: 0.887–0.995) and 0.928 (95% CI: 0.834–1.000), respectively, with the sensitivity of 0.929 and 0.846, respectively, and specificity of 1.000 and 0.667, respectively. Fig. 2 shows ROC curves, and Fig. 3 presents calibration curves.
Receiver operating characteristic(ROC) curve of the prediction model for NSSI in patients with adolescent depression ((A) is the training set, and (B) is the verification set).
Calibration curves of the prediction model for NSSI in adolescents with depression ((A) is the training set, and (B) is the verification set).
DCA for the Nomogram Prediction Model
The results of DCA showed that the clinical applicability of the nomogram model differed on different data sets. On the training set (Fig. 4A), the model showed significant net benefits in the threshold probability range of 0.15–0.85. However, on the verification set (Fig. 4B), the effective threshold range reduced to 0.20–0.75. This reduction may reflect the influence of sample fluctuation on the stability of the model. Notably, when the threshold probability exceeded 0.75, the net benefit of the ‘no intervention’ strategy was better than that predicted by the model. This finding suggested that clinicians should be cautious in applying the model results when evaluating high-risk patients. On the whole, the prediction model had the best clinical guidance value for patients in the middle-risk range (20%–75%). However, for high-risk patients (threshold 0.75), other clinical indicators for comprehensive evaluation should be combined to ensure the accuracy and safety of decision-making (Fig. 4).
Decision curve analysis (DCA) of the prediction model for NSSI in patients with adolescent depression ((A) is the training set, and (B) is the verification set).
Discussion
In this study on adolescent depression with NSSI behaviour, multivariate logistic regression analysis identified tense parental relationships, long depression duration, co-occurring physical disease, high depression severity, high anxiety levels, childhood trauma and negative life events as the factors associated with NSSI behaviour. These factors reveal the complex causes of adolescents’ self-injury behaviour in the face of depression from different angles and are of great importance for deeply understanding the psychopathological mechanism of this special group and formulating accurate intervention strategies.
This study found that tense parental relationships (OR = 1.939) are a core risk
factor for NSSI. This factor exhibits a more pronounced effect than family
environment in ordinary adolescents observed by Liang et al. [3]. In the
community samples of Liang et al. [3], the OR value of family conflict for
NSSI was 1.52. The risk weight observed in depressed patients in the present
study is higher than that observed by Liang et al. [3], suggesting that
the pathological state of depression may exacerbate the negative impact of family
tension through emotional dysregulation mechanisms. This study is the first to
verify the independent predictive value of parental relationship tension in
depression groups and to supplement the specific evidence of family factors in
clinical samples. Long depression duration is also a crucial risk factor. With
the prolongation of the course of depression, the psychological resilience of
patients is constantly challenged, and many aspects, such as emotional
regulation, cognitive function and social ability, are continuously damaged.
Regarding the correlation between depression duration and NSSI, Nagy et
al. [14] noted a correlation between chronic depression and self-injury but did
not quantify the specific influence of depression duration. In the present study,
logistic regression showed that the OR value for disease course 3 years was
2.614, which is significantly higher than that (OR = 1.89) in Nagy et
al. [14] meta-analysis. This difference is possibly due to the strict
restriction to ‘depression with NSSI’ samples and the inclusion of neuroimaging
indicators reflecting long-term brain function changes. Kang et al. [15] studied the family transmission of suicide and self-injury in low-income groups
but did not discuss disease duration separately. The present study confirmed that
the exhaustion of psychological resilience from long-term depression is an
independent driver of NSSI, providing quantitative evidence for the cumulative
effect of chronic depressive states, thus filling the gap in the research on the
quantitative relationship between disease duration and self-injury. For
adolescents with depression, co-occurring physical diseases are like adding
insult to injury. Physical disease itself not only brings physical discomfort and
limited function, but also increases the psychological burden, such as anxiety
about the prognosis of the disease, pain during treatment and social isolation
that may be caused by physical reasons, of patients. In contrast to those in the
study of Fernando et al. [16], concomitant somatic diseases (OR = 4.112)
show a very high risk weight in this study. Although this study focused on the
influence of mental illness and somatic diseases on suicide, it did not analyse
NSSI behaviour alone [16]. This study revealed the superposition effect of
somatic diseases and depression in adolescents for the first time, and it
reported an OR value that is considerably higher than that reported by Blessing
et al. [17] for NSSI. This difference indicates that the impairment of
physical function may promote self-injury through the two pathways of physical
pain and psychological despair [17]. This discovery breaks through the limitation
of previous studies focusing on psychosocial factors and brings the dimension of
physical health into the NSSI prediction framework. High depression severity and
anxiety levels are closely related and mutually influential, forming significant
risk factors for NSSI. A high degree of depression means that patients are deeply
immersed in negative emotions and cognitive states, such as depression, loss of
interest, self-blame and self-guilt, and experience a strong sense of pain and
helplessness. Meanwhile, a high degree of anxiety places them in a constant state
of tension, anxiety and worry and fills them with fear for the future [6]. In
terms of psychological mechanisms, NSSI in adolescent depression may be driven by
a reciprocal pathway of emotion regulation difficulties and negative
self-cognition. Emotion regulation dysfunction, such as impaired
prefrontal–limbic network connectivity (e.g., reduced DLPFC control over the
amygdala) [18] leads to failed emotional suppression, prompting individuals to
use self-injury as an alternative regulatory strategy, as supported by the
negative correlation between EEG frontal power and NSSI ( =
-0.142, p = 0.007) indicating disrupted frontal lobe emotional
modulation. Meanwhile, a negative self-cognition schema, with childhood
trauma–induced self-blame cognitions (CTQ score = 0.097, p
0.001) interacting with current depressive symptoms, forms a self-worth
degradation cycle, where individuals with high self-blame tendencies may
interpret negative life events (ASLEC score = 0.132, *p *
0.001) as self-validation of worthlessness, triggering self-injury as a form of
emotional release or self-punishment [19, 20]. In summary, the pathway of emotion
dysregulation negative cognition coping deficit
underscores the complex psychological mechanisms underlying NSSI. these
mechanisms are reflected in the model’s risk factors (e.g., anxiety, trauma and
life events) [6, 18, 19]. Irniger C et al. [4] discussed the mediating
effect of childhood trauma on NSSI through positive and negative coping styles
but did not combine neuroimaging indicators. In this study, the total score of
CTQ (OR = 1.102) and the wave power of EEG frontal lobe were
integrated synchronously. Trauma load could increase the risk of NSSI by
regulating the emotional regulation network of the frontal lobe, thus revealing
the pathological chain of trauma–neural mechanism–self–injury more deeply than
the analysis of a single psychological scale. When adolescents later develop
depression, their childhood traumatic experiences are easily reactivated,
accounting for their lack of effective coping abilities when facing current
psychological pressure. Traumatic emotions that were not properly handled in the
past are intertwined with the pain caused by the current depression, greatly
increasing the possibility of expressing inner pain through self-injury
behaviour. Negative life events are another crucial factor [20]. These negative
life events, whether they are major academic setbacks (such as exam failure and
pressure to enter a high-ranking school), interpersonal conflicts (conflicts with
classmates, teachers or family members), or family changes (such as the death of
relatives and divorce of parents) exert a considerable psychological effect on
adolescents, especially those who are already suffering from depression. Their
already fragile psychological resilience can be overwhelmed by these additional
stresses, prompting self-injury as a way to cope with inner pain and unresolved
pressures [5]. This research demonstrates distinct innovations over recent
studies. De Luca et al. [2] conducted a systematic review and Bayesian
meta-analysis on NSSI amongst community adolescents, focusing on incidence
trends, whereas the present study targeted depressed adolescents and innovatively
integrated 64-channel EEG (frontal -wave power) and 3T fMRI (DLPFC
activation) into the NSSI risk prediction model [2]. By contrast, Guo et
al. [21] only used single-mode fMRI to analyse prefrontal functional
connectivity in patients with adolescent depression. This study, for the first
time, constructed a multidimensional psychological–neural–clinical prediction
model by integrating multimodal neuroimaging data (64-channel EEG and 3T fMRI),
psychological scales (CTQ and ASLEC) and clinical risk factors (parental
relationship tension and childhood trauma). It results show that the multimodal
system significantly outperforms single-mode studies in terms of prediction
efficacy, verifying the independent predictive value of seven factors (e.g.,
parental tension with OR = 1.939 and childhood trauma with OR = 1.102). This work
provides a comprehensive tool for the risk stratification of adolescent
depression with NSSI.
On the basis of the above-mentioned factors associated with NSSI behaviour, this study further constructed a nomogram prediction model. The model demonstrated good calibration and fit on the training and verification sets, with C-index values of 0.936 and 0.923, average absolute errors between predicted and actual values of 0.092 and 0.105 and Hosmer–Lemeshow test p values of 0.452 and 0.523. These results show that the model has high accuracy and reliability in predicting NSSI behaviour in adolescents with depression.
The nomogram prediction model has broad prospects and potential for clinical application. Through this model, medical staff can accurately assess the risk of NSSI behaviour in patients with adolescent depression to formulate personalised treatment programmes and intervention measures. For patients predicted to be at high risk by the model, medical staff can formulate personalised and enhanced psychological intervention programmes in accordance with specific conditions [22]. For example, for patients with childhood trauma, trauma-focused cognitive behavioural therapy can help them deal with negative emotions and cognitive biases caused by past trauma. For patients who are at high risk because of tense parental relationships, family therapy can be provided, the family communication mode can be improved, family conflicts can be alleviated and the family support function can be enhanced. These personalised treatment programmes help meet the psychological needs of patients and promote the recovery of their mental health. On the basis of the prediction results of the model, medical staff can increase the follow-up frequency of high-risk patients and pay close attention to changes in their psychological state [23]. Through regular evaluation and monitoring, medical staff can identify the risk factors that may induce self-injury behaviour in time and take corresponding treatment measures quickly. For example, for patients with negative mood swings or cognitive impairment, the treatment plan can be adjusted in time, and psychological counselling and drug treatment can be strengthened to reduce the risk of self-injury behaviour.
Family environment has an important influence on adolescents’ mental health. Medical staff can communicate and cooperate with patients’ families in depth. help them realise the importance of the family environment to patients. and guide them to improve family functions actively and create a warm, harmonious and supportive family atmosphere. By improving the family support system, patients’ psychological resilience can be enhanced and the possibility of seeking relief through self-injury behaviour can be reduced. The model is also helpful to the rational distribution of medical resources. By focusing professional resources on patients assessed as high risk, it ensures that these patients receive adequate, professional interventions and treatments. This approach not only improves the utilisation efficiency of medical resources, but also ensures the quality of mental health services for the whole group of adolescent patients with depression and achieves the goal of precise medical care and intervention [24].
Although this study has made achievements in constructing and verifying the nomogram prediction model, it still has some limitations. Its samples originated from a single medical centre, and its sample size is limited (n = 136). Geographical representation is insufficient. Although the training and verification sets were divided and verified internally, they may affect the stability of the model. This study did not involve potential factors, such as social support and coping style, nor did it analyse the behaviour type and frequency of NSSI in layers. Given that its cross-sectional design lacks longitudinal data, clarifying causal relationships and dynamic evolution is difficult. Although the inclusion of neuroimaging indicators is valuable, selection bias may exist, and neural markers and dynamic evolution are not discussed. Future research can expand the sample size, conduct multicentre research and adopt a longitudinal design. Moreover, they can incorporate tools, such as the Multidimensional Perceived Social Support Scale and Coping Style Scale, to quantify potential protective factors and record treatment exposure variables. In addition, they can study the behaviour classification of NSSI and explore the gene–environment–nerve interaction mechanism by combining molecular genetics and epigenetics. Furthermore, future work can analyse the interaction between neuroimaging and clinical factors, as well as carry out external verification in wide clinical scenarios, such as different regions and varying levels of medical institutions [25].
Conclusion
This study identified factors associated with NSSI in adolescent depression—parental tension, long depression duration, co-occurring physical diseases, high depression/anxiety severity, childhood trauma, EEG frontal power, fMRI DLPFC activation and negative life events—and constructed a nomogram model with good predictive efficacy. By integrating psychological–neural–clinical indicators, the model serves as a visual tool for early NSSI risk assessment. Future directions include multicentre validation with diverse samples, longitudinal studies to explore causal dynamics, incorporation of protective factors (such as social support) and clinical implementation for personalised intervention planning.
Availability of Data and Materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zwolińska W Dmitrzak-Węglarz M SłopieńA Biomarkers in Child and Adolescent Depression Child Psychiatry and Human Development 20235426628110.1007/s 10578-021-01246-y 34590201 PMC 9867683 · doi ↗ · pubmed ↗
- 2De Luca L Pastore M Palladino BE Reime B Warth P Menesini E The development of Non-Suicidal Self-Injury (NSSI) during adolescence: A systematic review and Bayesian meta-analysis Journal of Affective Disorders 202333964865910.1016/j.jad.2023.07.09137479039 · doi ↗ · pubmed ↗
- 3Liang K Zhao L Lei Y Zou K Ji S Wang R et al Nonsuicidal self-injury behaviour in a city of China and its association with family environment, media use and psychopathology Comprehensive Psychiatry 202211515231110.1016/j.comppsych.2022.15231135395465 · doi ↗ · pubmed ↗
- 4Irniger C Vetter J Weidt S Seifritz E Holtforth MG Krähenmann R From past to present: the connection of traumatic childhood experiences, recent stressful life events, and treatment expectations in depression European Journal of Psychotraumatology 202516251862510.1080/20008066.2025.251862540600914 PMC 12224735 · doi ↗ · pubmed ↗
- 5ȘipoșR Văidean T Predescu E Risk Factors and Clinical Predictors of Suicidal Behaviors and Non-Suicidal Self-Injury Among Pediatric Psychiatry Emergency Admissions Pre- and Post-Pandemic: A Retrospective Cohort Study Children (Basel, Switzerland) 2025128110.3390/children 1201008139857912 PMC 11764410 · doi ↗ · pubmed ↗
- 6Hansen ER Kruckow S Ewing SWF Nordentoft M Thomsen KR Tolstrup JS Adolescent substance use patterns and subsequent risk of mental and behavioural disorders, substance use, and suicidal behaviour: a cohort study The Lancet. Public Health 202510 e 578e 58710.1016/S 2468-2667(25)00115-X 40602857 · doi ↗ · pubmed ↗
- 7Pérez Arqueros V Ibáñez-Beroiz B Goñi-Sarriés A Galbete Jiménez A Efficacy of psychotherapeutic interventions for non-suicidal self-injury in adolescent population: Systematic review and meta-analysis Spanish Journal of Psychiatry and Mental Health 20231611912610.1016/j.rpsm.2022.10.00137689523 · doi ↗ · pubmed ↗
- 8Goldbach JT Schrager SM Wood JK O’Brien RP Dunlap SL Rhoades H Development and validation of the Transgender Adolescent Stress Survey-Minority Stress (TASS-MS) Frontiers in Psychology 202415144869310.3389/fpsyg.2024.144869339698391 PMC 11653417 · doi ↗ · pubmed ↗