Current Breastfeeding Attitudes, Knowledge and Confidence of Obstetricians and Gynaecologists in Australia and New Zealand
Gabrielle Cher, Diana M. Bond, Natasha Nassar, Katy Hunt, Jane Svensson, Olga Aleshin, Antonia Shand

TL;DR
This study explores the attitudes, knowledge, and confidence of Australian and New Zealand obstetricians and gynaecologists regarding breastfeeding support.
Contribution
The study provides new insights into the current gaps in breastfeeding education and confidence among O&G specialists and trainees in Australia and New Zealand.
Findings
Only 37% of respondents felt confident in managing breastfeeding challenges.
Most respondents (60%) expressed a desire for more breastfeeding education.
Personal breastfeeding experience and extra training were linked to higher confidence and knowledge.
Abstract
There are limited data on what obstetricians and gynaecologists (O&G) know and think about supporting breastfeeding women. To investigate breastfeeding attitudes, knowledge and confidence of Australian and New Zealand O&G specialists and trainees in educating, assessing and managing breastfeeding women. An online REDCap survey was distributed via email in February 2023 to fellows and trainees of the Royal Australian New Zealand College of Obstetricians and Gynaecologists (RANZCOG). The survey included questions on demographic characteristics, knowledge, attitudes and confidence about breastfeeding. Of 312 (11%) respondents, 63% were > 40 years old, 78% female and two‐thirds had personally breastfed. Half had no formal breastfeeding education. Mean score related to attitude was 4.8/7 (71.1%) with higher scores associated with extra training (β = 0.44 (95% CI 0.04, 0.84)) and personal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
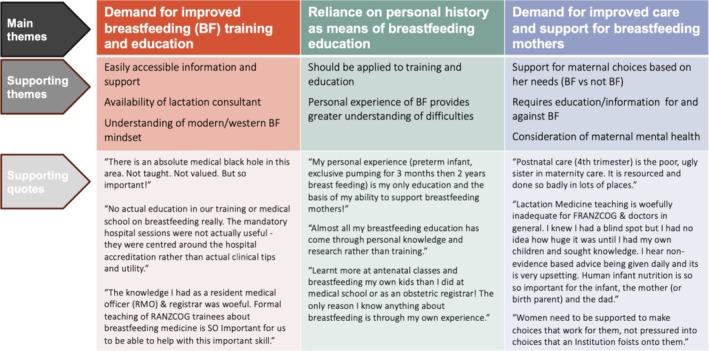 FIGURE 1
FIGURE 1| Demographic characteristics | Number | % |
|---|---|---|
| Age Group (years) ( | ||
| 20–39 | 109 | 36.1 |
| 40–59 | 147 | 48.7 |
| ≥ 60 | 46 | 15.2 |
| Sex ( | ||
| Female | 241 | 78.5 |
| Male | 66 | 21.5 |
| Country of medical training ( | ||
| Australia/New Zealand | 260 | 83.3 |
| Other | 52 | 16.7 |
| Trainee or FRANZCOG/Specialist ( | ||
| RANZCOG trainee | 79 | 25.3 |
| FRANZCOG/Specialist | 233 | 74.7 |
| Years in practice for specialist (years) ( | ||
| Less than 5 | 62 | 26.6 |
| 5–10 | 40 | 17.2 |
| More than 10 | 131 | 56.2 |
| Type of role ( | ||
| Obstetrics | 66 | 21.2 |
| Obstetrics and Gynaecology | 216 | 69.2 |
| Gynaecology | 21 | 6.7 |
| Other | 9 | 2.9 |
| Formal breastfeeding education or training ( | ||
| Yes | 150 | 48.1 |
| No | 155 | 49.7 |
| Don't know | 7 | 2.2 |
| Have sought additional training about breastfeeding ( | ||
| Yes | 66 | 21.2 |
| No | 246 | 78.8 |
| Breastfeeding history ( | ||
| Personally breastfed | 193 | 62.2 |
| Partner has breastfed | 57 | 18.1 |
| Never breastfed or had breastfeeding partner | 55 | 17.5 |
| Prefer not to say | 7 | 2.2 |
| Accredited Baby‐Friendly Health Initiative facility ( | ||
| Yes | 257 | 82.3 |
| No | 20 | 6.4 |
| Missing | 35 | 11.2 |
| Confidence ( | Agree | Neutral | Disagree |
|---|---|---|---|
| I play a role in breastfeeding promotion and education for my patients | 262 (83.4%) | 28 (8.9%) | 24 (7.6%) |
| I help facilitate immediate and uninterrupted skin‐to‐skin contact between newborn infants and mothers at all births | 279 (88.9%) | 20 (6.4%) | 15 (4.8%) |
| I support mothers in initiating and maintaining breastfeeding | 272 (86.6%) | 34 (10.8%) | 8 (2.5%) |
| I believe obstetricians should counsel mothers on the use and risks of feeding bottles, teats and pacifiers | 96 (30.6%) | 120 (38.2%) | 98 (31.2%) |
| I can identify if an infant is sucking/feeding well at the breast | 175 (55.7%) | 56 (17.8%) | 83 (26.4%) |
| I feel confident in managing breastfeeding‐related challenges | 115 (36.6%) | 78 (24.8%) | 121 (38.5%) |
| I am aware of the available services to refer my patients to for breastfeeding support and care | 301 (95.9%) | 7 (2.2%) | 6 (1.9%) |
| I would value more formal breastfeeding education or training | 188 (59.9%) | 64 (20.4%) | 62 (19.7%) |
| Attitudes and Beliefs about Breastfeeding ( | |||
| A mother instinctively knows how to breastfeed | 37 (11.4%) | 58 (17.8%) | 231 (70.9%) |
| Breastfeeding supports mother–infant bonding | 309 (94.8%) | 12 (3.7%) | 5 (1.5%) |
| Breastfeeding is more convenient than formula feeding | 258 (79.1%) | 55 (16.9%) | 13 (4.0%) |
| If a mother is struggling to breastfeed, she should be encouraged to use formula | 21 (6.4%) | 109 (33.4%) | 196 (60.1%) |
| Infant formula is as healthy for an infant as breastmilk | 22 (6.7%) | 39 (12.0%) | 265 (81.3%) |
| Formula feeding is the better choice if the mother plans to go out to work | 12 (3.7%) | 49 (15.0%) | 265 (81.3%) |
| The clinician should assist the mother to make a fully informed and appropriate decision about infant feeding | 310 (95.1%) | 14 (4.3%) | 2 (0.6%) |
| Breastfeeding beyond 12 months has no health benefits to the infant | 35 (10.7%) | 62 (19.0%) | 229 (70.3%) |
| I think breastfeeding problems are the domain of a midwife or lactation consultant, not a doctor | 37 (11.4%) | 61 (18.7%) | 228 (69.9%) |
| Attitudes and behaviours | Knowledge | Confidence | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| Mean (SD) | % correct (SD | MD |
| Mean (SD) | % correct (SD) | MD (95% CI) |
| Mean (SD) | % correct (SD) | MD (95% CI) |
| |
| Sex | |||||||||||||
| Male | 66 | 6.20 (1.69) | 68.89 (18.8) | −0.34 (−0.74, 0.07) | 0.10 | 7.89 (1.88) | 65.75 (15.7) | −1.48 (−1.92, −1.04) | < 0.001 | 4.53 (1.54) | 64.71 (22.0) | −0.30 (−0.71, 0.10) | 0.14 |
| Female | 241 | 6.53 (1.40) | 72.56 (15.5) | 9.37 (1.54) | 78.08 (12.8) | 4.83 (1.45) | 69.00 (20.7) | ||||||
| Age (years) | |||||||||||||
| 20–39 | 109 | 6.50 (1.49) | 72.22 (16.5) | 0.80 | 9.63 (1.39) | 80.25 (11.6) | < 0.001 | 4.56 (1.30) | 65.14 (18.6) | 0.02 | |||
| 40–59 | 147 | 6.37 (1.45) | 70.78 (16.1) | 8.95 (1.70) | 74.58 (14.2) | 4.73 (1.53) | 67.57 (21.9) | ||||||
| ≥ 60 | 46 | 6.43 (1.66) | 71.44 (18.4) | 8.26 (1.96) | 68.83 (16.3) | 5.3 (1.56) | 75.71 (22.3) | ||||||
| Country of training | |||||||||||||
| Australia/NZ | 260 | 6.42 (1.48) | 71.33 (16.4) | −0.14 (−0.58, 0.31) | 0.55 | 9.15 (1.70) | 76.25 (14.2) | 0.69 (0.18, 1.20) | 0.01 | 4.79 (1.45) | 68.43 (20.7) | 0.12 (−0.32, 0.56) | 0.59 |
| Other | 52 | 6.56 (1.58) | 72.89 (17.5) | 8.46 (1.80) | 70.50 (15.0) | 4.67 (1.59) | 66.71 (22.8) | ||||||
| Role | |||||||||||||
| Specialist | 233 | 6.42 (1.53) | 71.33 (17.0) | −0.08 (−0.46, 0.30) | 0.68 | 8.83 (1.80) | 73.58 (15.0) | −0.82 (−1.25, −0.38) | < 0.001 | 4.89 (1.50) | 69.86 (21.4) | 0.19 (0.08, 0.83) | 0.02 |
| Trainee | 79 | 6.51 (1.38) | 72.33 (15.3) | 9.65 (1.37) | 80.42 (11.4) | 4.43 (1.35) | 63.29 (19.2) | ||||||
| Specific role | |||||||||||||
| Gynaecology (Gyn) | 21 | 6.95 (1.53) | 77.22 (17.0) | 0.19 | 9.05 (2.25) | 75.42 (18.8) | 0.41 | 4.81 (1.86) | 68.71 (26.6) | 0.97 | |||
| Obstetrics (Obs) | 66 | 6.26 (1.43) | 69.56 (15.9) | 9.35 (1.43) | 77.92 (11.9) | 4.80 (1.44) | 68.57 (20.6) | ||||||
| Obs and Gyn | 216 | 6.48 (1.50) | 72.00 (16.7) | 8.94 (1.77) | 74.50 (14.8) | 4.77 (1.43) | 68.14 (20.4) | ||||||
| Other | 9 | 5.89 (1.36) | 65.44 (15.1) | 9.11 (1.54) | 75.92 (12.8) | 4.56 (1.94) | 65.14 (27.7) | ||||||
| Formal BF training | |||||||||||||
| Yes | 150 | 6.51 (1.49) | 72.33 (16.6) | 0.12 (−0.21, 0.46) | 0.48 | 9.17 (1.65) | 76.42 (13.8) | 0.26 (−0.13, 0.65) | 0.19 | 4.83 (1.41) | 69.00 (20.1) | 0.10 (−0.24, 0.43) | 0.56 |
| No | 155 | 6.39 (1.48) | 71.00 (16.5) | 8.92 (1.80) | 74.33 (15.0) | 4.74 (1.55) | 67.71 (22.1) | ||||||
| Sought extra BF training | |||||||||||||
| Yes | 66 | 6.82 (1.47) | 75.78 (16.3) | 0.47 (0.69, 0.88) | 0.02 | 9.14 (1.80) | 76.17 (15.0) | 0.13 (−0.35, 0.60) | 0.59 | 5.47 (1.33) | 78.14 (19.0) | 0.88 (0.50, 1.27) | < 0.001 |
| No | 246 | 6.35 (1.48) | 70.56 (16.4) | 9.01 (1.72) | 75.08 (14.3) | 4.59 (1.45) | 65.57 (20.7) | ||||||
| BF History | |||||||||||||
| Personal | 193 | 6.69 (1.37) | 74.33 (15.2) | 0.003 | 9.48 (1.49) | 79.00 (12.4) | < 0.001 | 5.07 (1.31) | 72.43 (18.7) | < 0.001 | |||
| Partner | 57 | 6.12 (6.12) | 68.00 (19.4) | 7.91 (1.94) | 65.92 (16.2) | 4.68 (1.50) | 66.86 (21.4) | ||||||
| None | 55 | 6.05 (1.46) | 67.22 (16.2) | 8.76 (1.60) | 73.00 (13.3) | 3.89 (1.56) | 55.57 (22.3) | ||||||
| Accredited BHFI | |||||||||||||
| Yes | 257 | 6.48 (1.47) | 72.00 (16.3) | 0.23 (−0.45, 0.91) | 0.51 | 9.08 (1.79) | 75.67 (14.9) | 0.38 (−0.42, 1.19) | 0.35 | 4.86 (1.43) | 69.43 (20.4) | −0.39 (−1.05, 0.27) | 0.24 |
| No | 20 | 6.25 (1.65) | 69.44 (18.3) | 8.7 (1.46) | 72.50 (12.1) | 5.25 (1.65) | 75.00 (23.6) | ||||||
- —Royal Hospital for Women Foundation, Royal Hospital for Women Senior Staff Committee
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreastfeeding Practices and Influences · Child and Adolescent Health · Maternal Mental Health During Pregnancy and Postpartum
Introduction
1
Breastfeeding is well established in protecting infant and maternal health and stands as a critical public health matter [1, 2, 3]. Breastfeeding mothers' need education and support to breastfeed successfully [4]. Yet despite its well‐established benefits, only 39% of Australian mothers exclusively breastfeed to 3 months and 15% reach 5 months [5], which is less than the recommended duration of 6 months of exclusive breastfeeding [6]. The most cited reasons for not continuing breastfeeding in the Australian National Infant Feeding Survey (2010) were breastfeeding‐related challenges [5] that can be addressed and managed by trained professionals.
The UNICEF Baby Friendly Initiative states that medical staff should have adequate knowledge, competence and skills to support breastfeeding and be provided the necessary training to do so [7]. Moreover, the American College of Obstetrics and Gynaecologists advises that obstetric care providers develop and maintain knowledge and skills in guiding, assessing and supporting breastfeeding mothers [2]. However, studies have found a lack of knowledge and confidence among different medical professional groups in supporting, assessing and managing breastfeeding women [8, 9]. A study in the United Kingdom found that medical schools were not adequately preparing students for breastfeeding assessment and knowledge and that 93% of medical students requested further breastfeeding education [10]. Dovetailing this, a 2022 Cochrane review indicated that doctors were not receiving adequate training to support and manage breastfeeding challenges [11]. In Canada, breastfeeding knowledge was investigated among paediatric trainees and found that most junior doctors lack the knowledge and training to manage breastfeeding difficulties [12]. Other American and Canadian studies demonstrate inadequate breastfeeding knowledge and standards among doctors providing obstetric care [13, 14]. In Australia, a study of General Practitioners found that nearly all the participants lacked formal breastfeeding training, and despite having positive attitudes towards breastfeeding, their knowledge and confidence in providing support and care to breastfeeding mothers was suboptimal [15]. Brodribb et al. [16] found that nearly 80% of Australian General Practitioners felt that they needed further breastfeeding education.
Obstetricians and gynaecologists have a critical role in maternity care, as breastfeeding advocates, educators and supporters. Evidence shows that implementing interventions to support breastfeeding can increase the rate, exclusivity and duration of breastfeeding [17]. O&G trainees and specialists, therefore, need knowledge and training to provide evidence‐based and appropriate care to mothers. Instituting formal breastfeeding education for physicians has been shown to not only improve breastfeeding knowledge among doctors but also ensure better patient outcomes [18, 19]. However, it is not known if formal breastfeeding education is currently provided to O&G doctors working in Australia and New Zealand and whether this impacts their confidence and ability to educate and manage breastfeeding women. This study aimed to investigate breastfeeding knowledge and attitudes about breastfeeding, and confidence in providing breastfeeding care and support to breastfeeding women among O&G doctors in Australia and New Zealand.
Materials and Methods
2
Data Collection
2.1
A link to an anonymous Research Electronic Data Capture (REDCap) questionnaire was distributed by email in February 2023 to specialist trainees, fellows and subspecialists of the Royal Australian New Zealand College of Obstetricians and Gynaecologists (RANZCOG) in Australia and New Zealand by the RANZCOG. Study data were collected and managed using REDCap electronic data capture tools hosted at the University of Sydney. REDCap is a secure, web‐based software platform designed to support data capture for research studies [20]. A single reminder email was sent after 2 weeks. The study investigators did not have access to the email addresses of the responders. RANZCOG trainees and specialists who stated that they were providing antenatal and postnatal care were included in this study.
The survey included four sections: Attitudes and beliefs regarding breastfeeding, knowledge of breastfeeding, confidence in providing breastfeeding support and demographic information (Appendix 1). There were nine questions in Section 1 regarding attitudes and beliefs and responses were on a 5‐point Likert‐type scale (strongly disagree, disagree, neither agree nor disagree, agree, strongly agree). The 12 knowledge‐based questions in Section 2 covered breastfeeding physiology and basic sciences, benefits of breastfeeding, common breastfeeding issues and maternal conditions and their effect on breastfeeding. The questions included were developed from the literature review conducted in the process of this research project. Responses for the knowledge section were on a 4‐point Likert‐type scale (disagree, neither agree nor disagree, agree and don't know). Section 3 contained eight confidence‐based questions similarly using the 5‐point Likert‐type scale as Section 1. Negatively worded items were reverse scored. Higher scores indicated more positive attitudes in Section 1, correct answers in Section 2, and a higher level of confidence in Section 3. Section 4 contained demographic information, including whether formal breastfeeding education or training had been received during medical school or as part of mandatory hospital training. Breastfeeding history was determined by the participant as: (1) those that had personally breastfed themselves; (2) having a partner who had breastfed; or (3) never breastfed or been a partner to a breastfeeding woman. There was also a free text box at the conclusion of the survey to include any additional comments the participant wished to add.
The survey was based on previous surveys and questions developed by midwives, obstetricians and researchers and was piloted by lactation consultants, midwives and doctors who care for breastfeeding mothers. The pilot survey took approximately 3–6 min to complete. Ethics approval was obtained from the South Eastern Sydney Local Health District Human Research Ethics Committee (ETH12255).
Statistical Analysis
2.2
Frequency and percentage tabulation of the demographic characteristics of survey participants were calculated using descriptive statistics. Mean scores for knowledge, attitudes and behaviours were compared across demographic characteristics using independent sample t‐test analyses and ANOVA. Univariate and multivariate regression analyses were used to assess association between main factors of interest and each outcome of attitude, knowledge and confidence scores. Only factors with p value < 0.2 on univariate analyses were then included in the multivariate analyses to assess the overall impact on outcomes. Data were analysed using SPSS Version 28 (IBM SPSS Statistics, 2021 IBM Corp., Armonk, NY, USA) and p value < 0.05 was considered statistically significant.
Comments related to open‐ended questions were thematically analysed by two researchers who independently coded the data into emergent themes using the study objectives. Themes were then clustered into overarching themes, compared and discussed with a third researcher until consensus was reached. Quotations directly relating to the main themes were identified.
Results
3
A total of 326 participants responded, with 312 completed surveys, yielding an estimated response rate of 11% [21]. The majority of the participants were above 40 years of age (63%), specialists (75%) and female (78%). Fifty per cent of participants had no formal breastfeeding education or training, and 81% had a breastfeeding history, having either personally breastfed (63%) or had a breastfeeding partner (18%). Demographic characteristics of the survey participants are summarised in Table 1.
Attitudes and behaviours towards breastfeeding are presented in Table 2. Attitudes towards breastfeeding were largely positive, with an overall mean attitude score of 6.4/9 (71.1%). Around two‐thirds (70%) disagreed with the statement that breastfeeding problems are the domain of a midwife or lactation consultant. One‐third (33%) were neutral about whether a mother should be encouraged to use formula if struggling to breastfeed.
Overall knowledge was good with a mean score of 9.0/12 (75%). However, knowledge about discarding breast milk after radiological procedures and antibiotic side effects was low (correct responses 45% and 20% respectively) (Table S1).
The overall mean confidence score was 4.8/7 (68.6%). Most respondents (87%) said that they personally supported women in initiating and maintaining breastfeeding and that they helped facilitate skin‐toto‐skin contact between newborn infants and mothers at all births (89%). Only one in three respondents (37%) stated that they felt confident in managing breastfeeding challenges, and around half (55%) said that they could tell if an infant was sucking well at the breast (Table 2).
Those who sought extra training and had personally breastfed were more likely to have higher attitude scores (p = 0.02 and p = 0.003 respectively) (Table 3). These two factors remained significant even after adjusting for sex, role, extra training and breastfeeding history: Extra training (β = 0.44 (95% CI 0.04, 0.84) p = 0.03) and personal breastfeeding (β = 0.37 (95% CI 0.15, 0.60) p = 0.001) (Table S2).
Participants with higher knowledge scores were more likely to be female, younger in age, trainees and those with a personal breastfeeding history (p < 0.001) (Table 3). After adjusting for factors of interest, knowledge scores remained higher for females (β = 0.58 (95% CI 0.10, 1.07) p = 0.02) and those who had personally breastfed (β = 0.45 (95% CI 0.21, 0.69) p < 0.001).
Compared with trainees, specialists had higher scores in confidence (4.9/7 vs. 4.4/7, p = 0.02) despite having lower overall scores in knowledge (8.8/12 vs. 9.7/12, p = < 0.001) (Table 3). After adjusting for sex, age, role, extra training and breastfeeding history, increased age (β = 0.39 (95% CI 0.64, 0.71) p = 0.002), extra training (β = 0.84 (95% CI 0.46, 1.21) p < 0.001) and personal breastfeeding (β = 0.52 (95% CI 0.31, 0.73) p < 0.001) were the most important factors associated with increased confidence (Table S2). Participants with a personal breastfeeding history scored higher in all three sections when compared with those without. Those who stated that they would value further education were more likely to be less than 40 years old, still in training, and not have formal breastfeeding training (All p = < 0.01) (Table 3).
Qualitative Results
3.1
An optional comment was completed by 13% of respondents (n = 39), the majority (77%) of whom were FRANZCOG/specialists (Figure 1). Comments were grouped into the following themes: (1) demand for improved breastfeeding training and education, (2) reliance on personal history as a means of breastfeeding education and (3) demand for improved care and support for breastfeeding mothers. The majority of comments were about reliance on personal history as a means of breastfeeding education and were strongly encouraging of the need for further breastfeeding education and training.
Free‐text comments by respondents classified by theme.
Discussion
4
To our knowledge, this is the first study to investigate the breastfeeding knowledge, confidence and attitudes among O&G trainees and specialists in Australia and New Zealand. This study found that many participants lacked confidence about breastfeeding and that the majority (60%) of doctors in O&G wanted more formal and improved education and training. Although knowledge was generally high, there were some areas of inadequate breastfeeding knowledge.
The positive attitude scores in this study were similar to previous studies investigating other groups of healthcare professionals [14, 22]. However, the knowledge section in this study's survey was more heterogenous. The questions specifically relevant to O&G doctors, such as maternal antibiotic side effects, breastfeeding restrictions post radiological contrast, appropriate advice for women with low milk supply and choice of antibiotics for mastitis, were less likely to be answered correctly. Findings from previous research investigating general practitioners in Australia and the UK suggest that the doctor's level of knowledge had a greater impact on their confidence than their attitudes towards breastfeeding [22, 23]. However, this study showed that the doctors' level of training had a greater impact on their confidence than their level of knowledge.
Similar to previous studies, we found personal breastfeeding history was the greatest predictor of higher confidence and, as demonstrated in the free‐text comments, it was highlighted as the most useful and beneficial source of breastfeeding education [16, 23, 24]. Those with a personal breastfeeding history also demonstrated higher knowledge and attitude scores. This is similar to a study by Brodribb et al., who found more positive breastfeeding attitudes and higher knowledge scores in doctors with a substantial breastfeeding history, which they defined as having more than 26‐week cumulative personal breastfeeding experience (self or partner) [22, 25, 26]. Personal experience, however, is not an adequate nor appropriate resource to rely on in providing evidence‐based information and support to patients.
This study's findings are similar to other Australian and international studies [16, 26, 27] investigating the breastfeeding knowledge and confidence among other health professionals, including breast surgeons, paediatricians and general practitioners. These studies report that the majority of doctors do not think they have adequate breastfeeding education and would value further training. In our study, participants wanting more breastfeeding education were more likely to be younger, trainees and those who did not have formal breastfeeding education. Inadequate knowledge may contribute to limited support and suboptimal management of breastfeeding mothers. A previous study by Finneran and Murphy [28] found that general practitioners who had formal training in breastfeeding were more likely to promote it to their patients. Research shows that improving physician education in breastfeeding improves maternal and newborn breastfeeding outcomes [18, 19]. This study suggests a potential need for the development of educational resources uniquely designed for O&G specialists and trainees.
Strengths of this study included the survey, including specialists and trainees from a wide geographical area of two countries. Given the high percentage of respondents with a breastfeeding history (81%), the participants included in this study may have had a greater interest in breastfeeding than nonrespondents. Alternatively, as suggested by the free‐text comments, participants with a personal breastfeeding history might have valued the importance of improving breastfeeding education, given their own lack of support or difficulties in breastfeeding as mothers and/or partners of breastfeeding mothers. Nonetheless, findings indicating higher knowledge scores among participants with a personal breastfeeding history suggest that even lower knowledge levels might prevail among nonrespondents who chose not to engage with this study. Limitations of the study include the low response rate (11%), which was not dissimilar to other surveys conducted among members of the RANZCOG [29] or an Australian study surveying breastfeeding knowledge among GPs [22]. The higher percentage of female respondents in this study is representative of the gender ratio within the college, with 83% of trainees being female [21]. Another limitation of this study was the small number of knowledge questions, which was thought to be necessary to make the study feasible for distribution and completion. A larger knowledge section may have produced a more comprehensive reflection of participant knowledge strengths and deficits. Quantifying what formal breastfeeding training participants have had would have yielded a more comprehensive understanding of the background education and training of this study's participants.
Overall confidence about breastfeeding in RANZCOG specialists and trainees was moderate, with poor confidence in managing breastfeeding challenges. The majority of respondents wanted more breastfeeding education and training. Breastfeeding is a critical public health matter with maternal and infant benefits and long‐term impacts. Given the low breastfeeding rates in Australia and New Zealand, addressing strategies to improve breastfeeding support is an important issue that could have a direct impact on maternal and infant care. The findings from this study can be utilised to develop and inform educational programs and guidelines, specifically catered towards O&G doctors and trainees to improve knowledge and confidence about breastfeeding and its impact on women's and infants' health. Regular training and updates should be implemented as part of ongoing clinical practice guidelines.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Data S1. Supporting Information.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A. Brown , “Breastfeeding as a Public Health Responsibility: A Review of the Evidence,” Journal of Human Nutrition and Dietetics 30, no. 6 (2017): 759–770.28744924 10.1111/jhn.12496 · doi ↗ · pubmed ↗
- 2American College of Obstetricians and Gynecologists (ACOG) , “Optimizing Support for Breastfeeding as Part of Obstetric Practice. Committee Opinion No. 658,” (2016).
- 3Centers for Disease Control and Prevention , “Breastfeeding: Why it Matters,” (2023), https://www.cdc.gov/breastfeeding/about‐breastfeeding/why‐it‐matters.html.
- 4J. Willumsen , “Breastfeeding Education for Increased Breastfeeding Duration,” (2013), https://www.who.int/elena/bbc/breastfeeding_education/en/.
- 5Australian Institute of Health and Welfare, (AIHW) , “2010 Australian National Infant Feeding Survey: Indicator Results,” (2012).
- 6NHMRC (National Health and Medical Research Council) , “Infant Feeding Guidelines: Information for Health Workers, NHMRC, Australian Government,” (2015).
- 7Baby Friendly Hospital Initiative (BFHI) Australia , BFHI Handbook for Maternity Facilities (BFHI, Australia, 2020).
- 8W. Brodribb , T. Fallon , C. Jackson , and D. Hegney , “Attitudes to Infant Feeding Decision‐Making–a Mixed‐Methods Study of Australian Medical Students and GP Registrars,” Breastfeeding Review 18, no. 1 (2010): 5–13.20443434 · pubmed ↗