Testing of Pre‐Operative Peripheral Nerve Blocks in Randomised Controlled Trials: A Scoping Review
Aurelien‐Xuan Rosendal Bahuet, Rasmus Linnebjerg Knudsen, Mathias Therkel Steensbæk, Sina Yousef, Rikke Helene Frølund Bjulf, Anne‐Sofie Linde Jellestad, Jonas Erasmus Egede Glahn, Sine Wichmann, Kai Henrik Wiborg Lange, Lars Hyldborg Lundstrøm, Anders Kehlet Nørskov

TL;DR
This review finds that many clinical trials on nerve blocks for surgery lack consistent reporting of testing methods and success criteria, making it hard to compare results and apply findings in practice.
Contribution
The study highlights a methodological gap in reporting peripheral nerve block testing in randomized trials, advocating for standardized reporting.
Findings
76% of trials reported testing nerve blocks, but 24% did not.
Only 58% of trials defined success criteria or reported success rates.
Most trials used sensory assessments, but only 73% used motor assessments.
Abstract
Peripheral nerve blocks are widely used for anaesthesia in upper and lower limb surgery, but the methods used to assess their success vary substantially. This scoping review examined contemporary research practises and the extent to which trials report on peripheral nerve block evaluation. A search was conducted on PubMed for randomised controlled trials published between 2014 and 2025 in anaesthesia journals, involving pre‐operative peripheral nerve blocks in adults undergoing limb surgery. Two independent authors screened and extracted data for each trial. Outcomes included the proportion of trials that reported block testing, described test methods, defined successful blocks, and reported success rates. Of 284 trials included, 215 (76%, 95% CI 71%–81%) reported testing blocks, and 210 (74%, 95% CI 69%–79%) described the test methods. Of the 215 trials reporting testing, 204 used…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
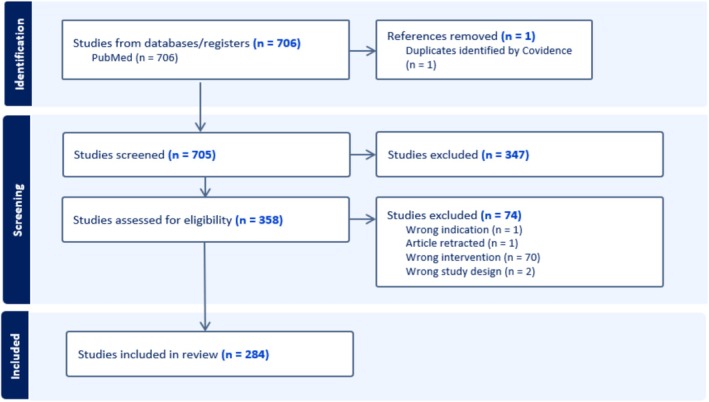 FIGURE 1
FIGURE 1|
Anesthesiology |
|
British Journal of Anaesthesia |
|
Anaesthesia |
|
Regional Anaesthesia and Pain Medicine |
|
Journal of Clinical Anaesthesia |
|
Best Practise & Research Clinical Anaesthesiology |
|
Anaesthesia & Analgesia |
|
European Journal of Anaesthesiology |
|
Korean Journal of Anesthesiology |
|
Anaesthesia Critical Care & Pain Medicine |
|
Canadian Journal of Anaesthesia |
|
Minerva Anestesiologica |
|
Journal of Anaesthesia |
|
BMC Anesthesiology |
|
Current Opinion in Anesthesiology |
|
Journal of Clinical Monitoring and Computing |
|
Acta Anaesthesiologica Scandinavica |
|
Anaesthesia and Intensive Care |
| Trials |
|
|---|---|
| Year of publication | |
| 2014–2019 | 175 (62) |
| 2020–2025 | 109 (38) |
| Publishing journal | |
| Anesthesiology | 18 (6) |
| British Journal of Anaesthesia | 14 (5) |
| Anaesthesia | 17 (6) |
| Regional Anaesthesia and Pain Medicine | 64 (23) |
| Journal of Clinical Anaesthesia | 16 (6) |
| Anaesthesia & Analgesia | 18 (6) |
| European Journal of Anaesthesiology | 22 (8) |
| Korean Journal of Anesthesiology | 15 (5) |
| Anaesthesia Critical Care & Pain Medicine | 4 (1) |
| Canadian Journal of Anaesthesia | 11 (4) |
| Minerva Anestesiologica | 15 (5) |
| Journal of Anaesthesia | 20 (7) |
| BMC Anesthesiology | 39 (14) |
| Journal of Clinical Monitoring and Computing | 2 (1) |
| Acta Anaesthesiologica Scandinavica | 7 (2) |
| Anaesthesia and Intensive Care | 2 (1) |
| Number of patients randomised | |
| 1–50 | 73 (26) |
| 51–100 | 154 (54) |
| > 100 | 57 (20) |
| Trial location (continent and most frequent countries) | |
| Africa | 11 (4) |
| Egypt | 11 (4) |
| Asia | 102 (36) |
| China | 34 (12) |
| Japan | 9 (3) |
| South Korea | 28 (10) |
| Turkey | 9 (3) |
| Other | 22 (8) |
| Europe | 85 (30) |
| Belgium | 10 (4) |
| France | 15 (5) |
| Italy | 10 (4) |
| Switzerland | 14 (5) |
| Other | 36 (13) |
| North America | 81 (28) |
| Canada | 36 (13) |
| United States of America | 45 (16) |
| Oceania | 3 (1) |
| Australia | 3 (1) |
| South America | 10 (4) |
| Brazil | 1 (0) |
| Chile | 9 (3) |
| Block placement and most common block types | |
| Upper limb | 163 (57) |
| Interscalene brachial plexus block | 74 (26) |
| Supraclavicular brachial plexus block | 43 (15) |
| Infraclavicular brachial plexus block | 26 (9) |
| Axillary brachial plexus block | 27 (9) |
| Lower limb | 122 (43) |
| Femoral nerve block | 54 (19) |
| Saphenous nerve block | 47 (17) |
| Sciatic nerve block | 32 (11) |
| Popliteal sciatic nerve block | 31 (11) |
|
| |||
|---|---|---|---|
| Yes | No | Partial | |
| PNB tested | 215 (76, 71–81) | 55 (19, 15–24) | 14 (5, 2–7) |
| PNB test described | 210 (74, 69–79) | 60 (21, 16–26) | 14 (5, 2–7) |
| PNB success criteria defined | 164 (58, 52–63) | 112 (39, 34–45) | 8 (3, 1–5) |
| PNB success rate reported | 164 (58, 52–63) | 112 (39, 34–45) | 8 (3, 1–5) |
| Management of data from unsuccessful PNBs described | 128 (45, 39–51) | 149 (52, 47–58) | 7 (2, 1–5) |
| Subgroup | Sub‐group |
| PNB tested ( |
| ||
|---|---|---|---|---|---|---|
| Yes | No | Partial | ||||
| Publishing journal in the upper 50th percentile of impact factor | Yes | 184 | 137 (74, 68–80) | 37 (20, 14–26) | 10 (5, 2–9) |
|
| No | 100 | 78 (78, 70–86) | 18 (18, 10–26) | 4 (4, 0–8) | ||
| Published after 2019 | Yes | 109 | 79 (72, 64–81) | 25 (23, 15–31) | 5 (5, 1–9) |
|
| No | 175 | 136 (78, 72–84) | 30 (17, 12–23) | 9 (5, 2–8) | ||
| PNB as the sole anaesthetic for surgery | Yes | 76 | 64 (84, 76–92) | 8 (11, 4–17) | 4 (5, 0–10) |
|
| No | 208 | 151 (73, 67–79) | 47 (23, 17–28) | 10 (5, 2–8) | ||
| ‘Large’ trials (> 100 participants) | Yes | 57 | 47 (82, 73–92) | 8 (14, 5–23) | 2 (4, 0–8) |
|
| No | 227 | 168 (74, 68–80) | 47 (21, 15–26) | 12 (5, 2–8) | ||
| Prospective, publicly accessible protocol | Yes | 156 | 116 (74, 68–81) | 33 (21, 15–28) | 8 (5, 2–9) |
|
| No | 128 | 99 (77, 70–85) | 23 (18, 11–25) | 6 (5, 1–8) | ||
| Trials in which the PNB was the primary intervention or comparator | Yes | 256 | 199 (78, 73–83) | 44 (17, 13–22) | 13 (5, 2–8) |
|
| No | 28 | 16 (57, 39–75) | 11 (39, 21–57) | 1 (4, 0–10) | ||
| Subgroup | Sub‐group |
| PNB test described ( |
| ||
|---|---|---|---|---|---|---|
| Yes | No | Partial | ||||
| Publishing journal in the upper 50th percentile of impact factor | Yes | 184 | 135 (73, 67–80) | 39 (21, 15–27) | 10 (5, 2–9) |
|
| No | 100 | 75 (75, 67–83) | 21 (21, 13–29) | 4 (4, 0–8) | ||
| Published after 2019 | Yes | 109 | 78 (72, 63–80) | 26 (24, 16–32) | 5 (5, 1–9) |
|
| No | 175 | 132 (75, 69–82) | 34 (19, 14–25) | 9 (5, 2–8) | ||
| PNB as the sole anaesthetic for surgery | Yes | 76 | 63 (83, 74–91) | 9 (12, 5–19) | 4 (5, 0–10) |
|
| No | 208 | 147 (71, 64–76) | 51 (25, 19–30) | 10 (5, 2–8) | ||
| ‘Large’ trials (> 100 participants) | Yes | 57 | 47 (82, 73–92) | 8 (14, 5–23) | 2 (4, 0–8) |
|
| No | 227 | 163 (72, 66–78) | 52 (23, 17–28) | 12 (5, 2–8) | ||
| Prospective, publicly accessible protocol | Yes | 156 | 116 (74, 68–81) | 32 (21, 14–27) | 8 (5, 2–9) |
|
| No | 128 | 94 (73, 66–81) | 28 (22, 15–29) | 6 (5, 1–8) | ||
| Trials in which the PNB was the primary intervention or comparator | Yes | 256 | 197 (77, 72–82) | 46 (18, 13–23) | 13 (5, 2–8) |
|
| No | 28 | 13 (46, 28–65) | 14 (50, 31–69) | 1 (4, 0–10) | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnesthesia and Pain Management · Intraoperative Neuromonitoring and Anesthetic Effects · Pain Management and Opioid Use
Introduction
1
Heterogeneity in outcome measurement is a commonly cited issue when performing systematic reviews [1]. When testing procedural interventions in randomised clinical trials (RCTs), it is imperative to ensure that the procedure is conducted and performed according to a set standard. Peripheral nerve blocks (PNBs), in which local anaesthetics are injected perineurally to anaesthetise a target area, are an increasingly commonly used anaesthetic procedural intervention [2]. Numerous clinical trials have investigated the effects of different local anaesthetics and doses, as well as adjuvants, in various PNBs [3, 4, 5, 6]. However, to ensure the validity of results, it is crucial that the blocks are systematically and preferably uniformly tested; success rates should also be reported and discussed, with unsuccessful procedures being accounted for when interpreting results [7]. Success rates of PNBs vary according to factors such as needle guidance technique, block type, operator experience, the type of local anaesthetic and the concentration, dose, and volume of local anaesthetic used; a Cochrane systematic review comparing ultrasound guidance to other methods of nerve localisation for PNBs reported block success rates ranging from 61% to 100% [8].
The success of a PNB can be defined in several ways, and previous research suggests there is significant variability in the way PNBs are tested, both in clinical practise and research [9]. Simple sensory and motor function assessments using graded scales remain the most used modalities, but other methods such as thermography or peripheral flow index may also be employed [9, 10]. Variations in testing methodology, such as the time of testing or the grading scale used, may complicate comparisons even between trials assessing PNBs using the same modality [11].
As the use of PNBs continues to increase, so too does the need for a robust and transparent evidence base that can inform clinical practise. Detailed descriptions of how PNBs are tested and deemed successful and the rates of successful blocks are therefore essential to allow valid comparisons between trials, to perform meta‐analysis of results and for clinical applicability of results. To our knowledge, no evidence exists on whether RCTs transparently describe the testing methods, definitions of success and success rates of PNBs.
Aim
2
This scoping review was carried out to explore existing literature and assess contemporary research practise in the field of peripheral nerve blocks [12]. It aimed to determine the proportion of RCTs published in the last decade involving PNBs in the pre‐operative anaesthetic management of upper and lower limb surgery that describe how PNBs are tested. We also aimed to explore the proportion of RCTs that had defined a successful block and that reported success rates of blocks.
Materials and Methods
3
A protocol was developed in accordance with Joanna Briggs Institute (JBI) guidance [13]. It was made available on Open Science Framework prior to data collection and was published in April 2025 [14, 15]. The scoping review follows the JBI Manual for Evidence Synthesis and adheres to the Preferred Reporting Items for Systematic reviews and Meta‐Analyses extension for scoping reviews (PRISMA‐ScR) [12, 16].
Eligibility Criteria
3.1
Population
- Studies on adults (as defined by trialists) receiving a pre‐operative PNB as part of, or as the sole, anaesthetic management for upper or lower limb surgery. Truncal and fascial plane blocks were not included, as the lack of consensus on how these blocks can be assessed would have limited the meaningful assessment of this study's outcomes [17, 18, 19].
Concept
- PNBs of isolated nerve structures or nerve plexuses with an innervation area accessible for specific, non‐invasive testing of success. If combined with other forms of anaesthesia that would make testing unfeasible (e.g., spinal or general anaesthesia), the PNB was to be performed prior to this.
Context
- PubMed‐indexed RCTs published in peer‐reviewed journals of anaesthesia.
- Publication date between January 1st, 2014, and February 20th, 2025.
- Published in English.
Outcomes
3.2
- The proportion of RCTs stating that PNBs were tested.
- The proportion of RCTs describing how the PNBs were tested.
- The proportion of RCTs using sensory function to test PNBs.
- The proportion of RCTs using motor function to test PNBs.
- The proportion of RCTs defining PNB success criteria.
- The proportion of RCTs reporting PNB success rates.
- The success rate of PNBs is reported by trialists.
- The proportion of RCTs describing how data from unsuccessful PNBs were managed in the statistical analyses.
Information Sources and Search Strategy
3.3
In order to include specialty‐relevant trials with high quality methodology that would accurately answer the review's aims, the search was narrowed to journals listed under the ‘Anesthesiology’ category on Web of Science that primarily focus on perioperative or regional anaesthesia and publish in English [20]. This was determined using the journals' overview, aims and scope, and by screening publications from the past 24 months. A search string adapted to the PubMed database was developed with a medical librarian experienced in database literature searches. As all included journals were indexed on PubMed, the search was not carried out on other databases. The journals included in the search are listed in Table 1, and the search string is provided in Appendix A. The final search was executed on February 20th, 2025.
Source Selection and Data Charting Process
3.4
Each trial was independently screened by two different authors. Disagreements were resolved through discussion between the screening authors and, where necessary, the involvement of a third, senior author. Data extraction was also performed independently by two authors per trial, with consensus provided by the review's first author. Covidence, a systematic review software, was used for trial screening and data extraction [21].
Data Items
3.5
Data for each trial were collected regarding trial information (e.g., year of publication, publishing journal, trial size), anaesthetic management (e.g., type of PNB, surgery performed under PNB only or combined with other anaesthetic techniques) and outcomes as stated above.
An extraction form was made using Covidence's data extraction tool, shown in Appendix B. Two authors piloted the data extraction form on five randomly selected full‐text articles to ensure that the data collected effectively fulfilled the review's objectives. The clinical suitability of a testing method for a given PNB lies outside the scope of this review and was therefore not assessed.
Synthesis of Results
3.6
Data are presented in narrative form or using tables. Proportions are presented with corresponding 95% confidence intervals (CIs). Continuous variables are presented as means with corresponding standard deviations (SDs) for data with normal distributions, and with medians and interquartile ranges (IQRs) for non‐normally distributed data. Subgroup analyses were performed on the following two outcomes:
- The proportion of RCTs that state that PNBs were tested.
- The proportion of RCTs describing how the PNBs were tested.
Subgroup analyses, pre‐defined in the study protocol, were performed based on the following criteria:
- Publishing journal in the upper 50th percentile of Impact Factor, according to the Web of Science 2024 Journal Impact Factor (yes vs. no) [20].
- Published within the last 5 years (after 2019) (yes vs. no).
- PNB as the sole anaesthetic for surgery (yes vs. no).
- ‘Large’ trials (over 100 participants) (yes vs. no).
- Trials with a prospective, publicly accessible protocol (yes vs. no).
- Trials in which the PNB was the primary intervention or comparator (yes vs. no).
Chi‐square tests were used to compare subgroups.
Results
4
Our search identified 706 studies. Following removal of duplicates and abstract screening, 358 studies were assessed in full‐text screening, of which 284 were included (Figure 1).
Preferred reporting items for systematic reviews and meta‐analyses flow diagram. Latest search performed on February 20, 2025.
Study Characteristics
4.1
Trial characteristics are summarised in Table 2. The majority of trials included fewer than 100 patients (227/284, 80%), were published between 2014 and 2019 (175/284, 62%) and approximately half had a prospectively registered, publicly accessible protocol (156/284, 55%). Of the 284 included trials, 162 (57%) investigated upper limb blocks and 121 (43%) investigated lower limb blocks, with one trial including both [22]. Most included trials had a PNB as the primary intervention or comparator (256/284, 90%). Included trials are individually listed in Table S1.
Review Outcomes
4.2
Amongst the included trials, 215/284 (76%, 95% CI 71%–81%) stated that all PNBs performed in the trial were tested, with 210/284 trials (74%, 95% CI 69%–79%) describing the test methods (Table 3). Of the 215 trials stating that all PNBs were tested, 204 (95%, 95% CI 91%–97%) reported using sensory testing and 157 (73%, 95% CI 67%–79%) reported using motor testing, with 151 (70%, 95% CI 64%–76%) reporting both sensory and motor testing. Amongst the trials that reported testing, graded scales (e.g., assessing block quality using a scale with three or more ordered categories) or quantitative measurements such as maximum voluntary isometric contraction were used to assess sensory blocks in 128/204 trials (63%, 95% CI 56%–69%) and motor blocks in 122/157 trials (78%, 95% CI 71%–84%).
Success criteria (e.g., a certain threshold on a grading scale) for PNBs were specified in 164/284 (58%, 95% CI 52%–63%) of trials, and the same number of trials reported their success rates. Of note, four trials reported a success rate without defining criteria for a successful block [23, 24, 25, 26]. In studies reporting success rates, the median success rate of PNBs was 98% (range 15–100%, IQR 92%–100%). Under half (128/284, 45%, 95% CI 39%–51%) of included trials reported how data from unsuccessful blocks were managed in the statistical analyses.
Subgroup Analyses
4.3
Subgroup analyses are shown in Tables 4a and 4b. Trials in which the PNB was the primary intervention or comparator had statistically significantly higher rates of reporting PNB testing and describing how PNBs were tested than trials where the PNB was not the primary intervention or comparator. There were no significant differences in other subgroups, both regarding reporting PNB testing and describing how PNBs were tested.
Discussion
5
Reporting of Block Testing and Block Success
5.1
We identified 284 RCTs involving PNBs published in major anaesthesia journals between January 2014 and February 2025. Although 76% of trials reported testing of the performed PNBs, a substantial proportion did not. The observed variability in reporting reflects a previously recognised heterogeneity that exists in research on regional anaesthesia [7, 9, 27].
The number of trials reporting definitions of a successful block was lower than those reporting testing, with approximately two in five trials not reporting the criteria for a successful nerve block. Reporting whether blocks were tested and how successful blocks were defined are essential for assessment of results as well as trial comparability and reproducibility. Furthermore, clear descriptions of testing and success criteria are crucial to clinical implementation of results. Without transparency on these key components, interpretation of outcomes such as postoperative pain and opioid consumption may be futile. Proposed classification systems for failed PNBs may help to standardise reporting [28, 29].
In a 2022 Delphi study conducted to develop a core outcome set for regional anaesthesia and facilitate intertrial comparison, cold sensory testing 30 min after a block was selected as a core outcome [7]. Of the 42 trials published following the publication of this outcome set, 31% (13/42) did not report any form of sensory testing. Data on timing and modality of sensory testing were not recorded in this review, so the number of trials not adhering to this core outcome is likely higher.
Interpretation of Success Rates
5.2
The median success rate across included trials was 98%. By comparison, a 2009 study using data from more than 8000 PNBs administered in a clinical context reported a lower success rate of 89% [30]. A potential explanation for this discrepancy is that PNB administration in a research context does not necessarily reflect real‐life clinical practise. For example, a trial protocol may dictate that only experienced clinicians will administer PNBs for included patients, whereas in clinical contexts, PNBs may be administered by clinicians with a broader range of experience. The widespread adoption of ultrasound guidance in contemporary performance of PNBs may also lead to higher success rates [8]. Some degree of reporting bias may also explain the high success rate we found; in our review, a minority of trials reported how data from unsuccessful blocks were managed in statistical analyses. If patients with an unsuccessful block were excluded from trial analyses, this would clearly skew the reported success rate and trial results. Trials should therefore report how data from unsuccessful blocks are managed in the clinical trial setup, and how data from these cases were analysed, for example, using either intention‐to‐treat or per‐protocol analyses.
One included study reported a low success rate of 15%; the authors attributed this to low local anaesthetic volume and a short 15‐min interval between block placement and testing [31]. Whilst these specific details were not part of our data extraction, they illustrate how factors such as technique and timing can affect the reported success rates of PNBs, and hence the generalisability and clinical implications of the results. Drawing conclusions from RCTs comparing PNBs to other anaesthetic interventions may therefore not be possible if the success rate of the PNBs is unknown or skewed due to suboptimal timing or dosing. For example, postoperative pain is a frequently cited outcome in RCTs involving PNBs [32]. Interpretation of this outcome assumes that the administered PNBs provided analgesia as expected. This further highlights the importance of trials reporting how they test blocks, how they define a successful nerve block, the block's success rate and how unsuccessful blocks were handled in statistical analyses.
Trials Without PNBs as the Primary Intervention or Comparator
5.3
We included trials where participants received a PNB without this being the trial's primary intervention or comparator. For example, two trials assessed gabapentin and prolonged‐release oxycodone‐naloxone, respectively, for postoperative pain in patients undergoing total knee arthroplasty with femoral and sciatic nerve blocks in addition to spinal anaesthesia [33, 34]. In both trials, block success rate would directly influence outcomes, as a successful PNB would likely reduce postoperative pain, regardless of group allocation. Despite the PNB not being the primary focus of these trials, reporting of block testing, criteria for block success, and success rates remain essential for valid interpretation of trial results. However, this subgroup of trials had significantly lower reporting rates of PNB testing compared to the trials in which PNBs were the primary intervention or comparator.
Strengths and Limitations
5.4
This review has several strengths. It was conducted according to a pre‐defined, published protocol and adhered to established methodological frameworks and guidelines. Data screening and extraction for each trial were performed independently by two reviewers, reducing the risk of selection and extraction bias. By limiting the search to RCTs published in the last decade, the review provides an up‐to‐date overview of current research practises in the testing and reporting of peripheral nerve blocks. The large number of included studies further strengthens the robustness of the findings.
This review also has limitations. The search was limited to a single database (PubMed) and included only studies published in a select number of high impact factor peer‐reviewed journals of anaesthesia. These restrictions may have introduced selection bias and limited the generalisability of findings. However, the decision to focus the search on selected, specialty‐relevant journals was made to ensure that included trials would be of high methodological quality, thus preventing results from being skewed by trials published in less established journals, which may not have the same methodological standards. Furthermore, it was thought that potential issues with reporting of PNB testing in high impact factor journals highlighted by this review would be just as, if not more, prevalent in lower impact factor journals. All included journals were indexed on PubMed, which is why the search was not carried out on other databases. Although we recognise the selection bias introduced by the limited selection of journals, we believe that the risk of omission of high‐quality RCTs that would have changed the conclusion is minor. The exclusion of non‐English language trials may have resulted in the omission of relevant trials conducted in other languages. As is typical in scoping reviews, we did not assess the methodological quality of included studies, which means variations in study rigour were not accounted for in the analysis. Data collected regarding testing methodology was limited to whether testing was carried out using sensory or motor modalities and whether graded scales or quantifiable measures were used. This decision was made to provide consistency in the collected data and ensure the review's outcomes could be meaningfully answered, as collecting detailed information on factors such as specific test methodology, timing and conditions would have introduced substantial heterogeneity. However, this also limits the conclusions that can be drawn regarding the variability that exists in testing methodology. Additionally, whilst data extraction was conducted by two independent reviewers for each trial, consensus was reached by a single author, which may have introduced unintentional bias.
Future Implications
5.5
Future trials in regional anaesthesia should include clear descriptions of how PNBs are tested and how successful blocks are defined. Consistent use of systematic structures, such as core outcome sets or classification systems for failed PNBs, may help standardise reporting in RCTs, facilitating intertrial comparison and the clinical application of trial findings.
Conclusions
6
This scoping review investigated contemporary practise in testing methodology reported in RCTs involving PNBs from major anaesthetic journals. Although most trials do report testing PNBs, about one in four did not. Furthermore, approximately two in five trials did not define what constituted a successful block or report rates of success. Lack of consistent and transparent test methodology poses challenges when comparing trials and performing meta‐analyses, and in translating trial findings into clinical practise. Consistent use of systematic reporting is advised.
Author Contributions
All authors meet the recommendations for authorship defined by The International Committee of Medical Journal Editors. A.‐X.R.B., K.W.L., L.H.L., and A.K.N. conceived the study concept and design. A.‐X.R.B., R.L.K., M.T.S., S.Y., R.H.F.B., J.E.G., and S.W. conducted title, abstract, and full‐text screening and data extraction. A.‐X.R.B. carried out data analysis and wrote the first draft of this manuscript with support from A.‐S.L.J. L.H.L. and A.K.N. provided project supervision. All authors read and approved the final manuscript.
Funding
The authors have nothing to report.
Ethics Statement
Ethics approval was not required for this scoping review.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Table S1: Details of included studies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1J. B. Schroll , R. Moustgaard , and P. C. Gotzsche , “Dealing With Substantial Heterogeneity in Cochrane Reviews. Cross‐Sectional Study,” BMC Medical Research Methodology 11 (2011): 22, 10.1186/1471-2288-11-22.21349195 PMC 3056846 · doi ↗ · pubmed ↗
- 2D. F. Johnston and L. R. Turbitt , “Defining Success in Regional Anaesthesia,” Anaesthesia 76, no. 1 (2021): 40–52, 10.1111/anae.15275.33426663 · doi ↗ · pubmed ↗
- 3J. Li , H. Wang , B. Dong , J. Ma , and X. Wu , “Adding Dexmedetomidine to Ropivacaine for Femoral Nerve Block Inhibits Local Inflammatory Response,” Minerva Anestesiologica 83 (2017): 590–597, 10.23736/S 0375-9393.17.11430-6.28106354 · doi ↗ · pubmed ↗
- 4M. Lopez , M. Calvo , A. Sancho , N. Brogly , E. Guasch , and F. Gilsanz , “Effective Volumes of 1.5% Mepivacaine With Different Sodium Concentration for Ultrasound Guided Popliteal Block,” Journal of Clinical Anesthesia 37 (2017): 139–144, 10.1016/j.jclinane.2016.12.009.28235506 · doi ↗ · pubmed ↗
- 5D. Holland , R. J. J. Amadeo , S. Wolfe , et al., “Effect of Dexamethasone Dose and Route on the Duration of Interscalene Brachial Plexus Block for Outpatient Arthroscopic Shoulder Surgery: A Randomized Controlled Trial,” Canadian Journal of Anesthesia 65 (2018): 34–45, 10.1007/s 12630-017-0989-7.29127558 · doi ↗ · pubmed ↗
- 6J. M. Flaherty , A. A. Berg , A. Harrison , et al., “Comparing Liposomal Bupivacaine Plus Bupivacaine to Bupivacaine Alone in Interscalene Blocks for Rotator Cuff Repair Surgery: A Randomized Clinical Trial,” Regional Anesthesia and Pain Medicine 47 (2022): 309–312, 10.1136/rapm-2021-103349.35190468 · doi ↗ · pubmed ↗
- 7J. Hill , T. Ashken , S. West , et al., “Core Outcome Set for Peripheral Regional Anesthesia Research: A Systematic Review and Delphi Study,” Regional Anesthesia and Pain Medicine 47 (2022): 691–697, 10.1136/rapm-2022-103751.35863787 · doi ↗ · pubmed ↗
- 8S. R. Lewis , A. Price , K. J. Walker , K. Mc Grattan , and A. F. Smith , “Ultrasound Guidance for Upper and Lower Limb Blocks,” Cochrane Database of Systematic Reviews 2015 (2015): CD 006459, 10.1002/14651858.CD 006459.pub 3.26361135 PMC 6465072 · doi ↗ · pubmed ↗