Avoidable emergency department admissions among nursing home residents – insights from a retrospective study
Julie Merche, Henri Thonon, François-Xavier Sibille, Julie Gabriel, Elise Simonin, Didier Schoevaerdts, Thérèse Van Durme, Marie de Saint-Hubert

TL;DR
This study finds that about 20% of emergency department admissions by nursing home residents in a Belgian hospital could have been avoided, often due to preventable issues like falls and catheter problems.
Contribution
The paper introduces a retrospective assessment tool to identify avoidable emergency admissions and quantifies their frequency in a specific hospital setting.
Findings
Approximately 22.6% of admissions were judged potentially avoidable by geriatricians.
Falls, catheter issues, and wounds were the most common causes of avoidable admissions.
The proposed tool had high specificity but moderate sensitivity in identifying avoidable admissions.
Abstract
To quantify avoidable admissions of nursing home residents in a Belgian hospital, identify associated factors, and propose a retrospective assessment tool. Between 14.1% and 22.6% of admissions were deemed potentially avoidable, depending on the assessment method. Falls, catheter issues, and wounds were common causes. Identifying common avoidable complaints and diagnoses may support the development of alternative care solutions in nursing homes. The online version contains supplementary material available at 10.1007/s41999-025-01264-2. The number of nursing home residents (NHRs) admitted to emergency departments (EDs) is steadily increasing. Some of these admissions have been identified as potentially avoidable. This study aims to quantify avoidable admissions at a Belgian hospital and identify factors associated with these admissions. A retrospective assessment tool is also…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
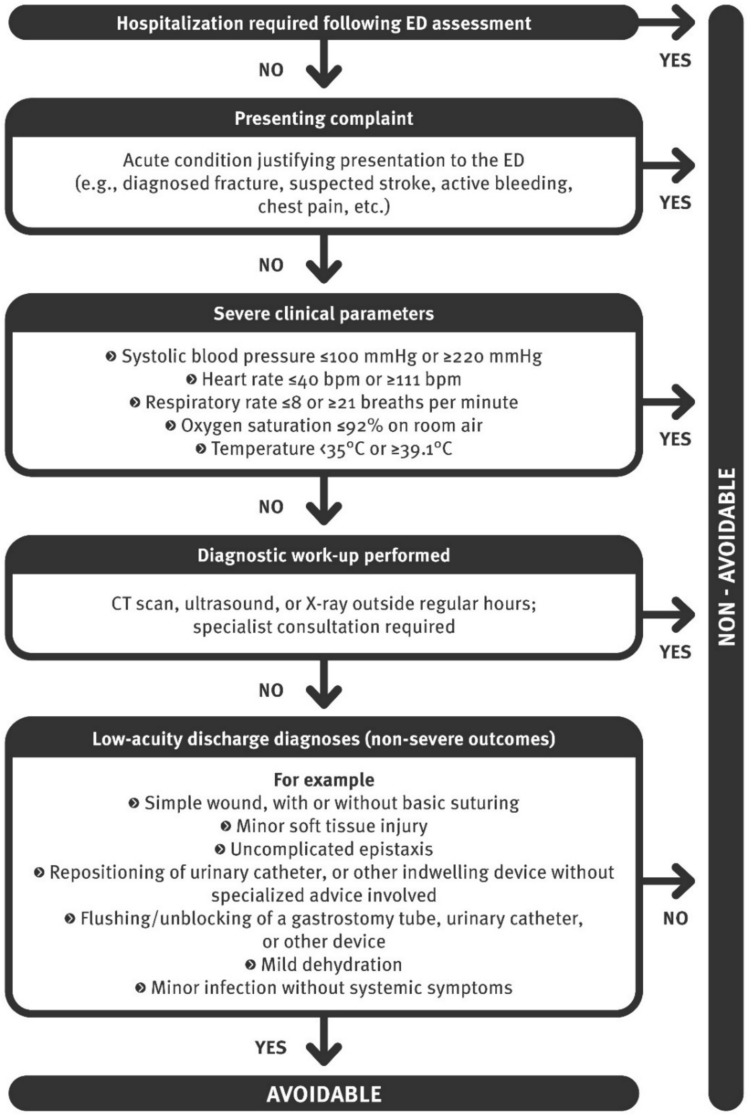 Figure 1
Figure 1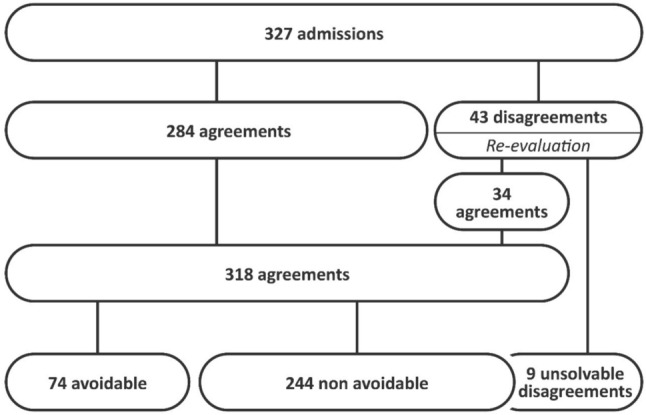 Figure 2
Figure 2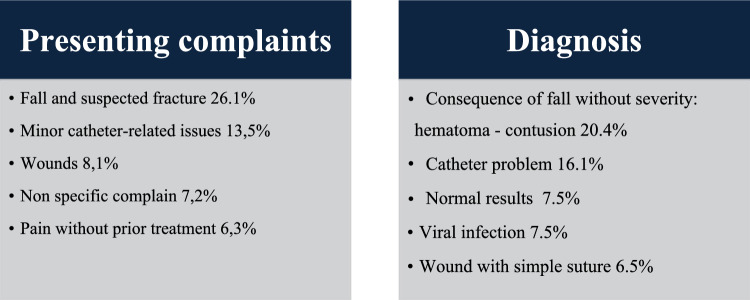 Figure 3
Figure 3- —http://dx.doi.org/10.13039/501100002661Fonds De La Recherche Scientifique - FNRS
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGeriatric Care and Nursing Homes · Emergency and Acute Care Studies · Frailty in Older Adults
Introduction
An increase in emergency department (ED) visits by nursing home residents (NHRs) has been documented in numerous countries [1–5]. For instance, one in four NHRs visits the ED every six months in Canada [6], while an annual rate of 18.9% has been reported in France [7]. These visits are associated with prolonged ED stays, an increased workload for healthcare providers, and rising costs [8]. This trend is multifactorial, driven by the complex healthcare needs of this population [9], care fragmentation, and inadequate primary care support [1, 3]. NHRs frequently present with severe clinical conditions and are at a high risk of hospitalization and mortality [5, 8, 10]. ED visits can pose particular challenges for this demographic due to an unsuitable environment, communication barriers, limited geriatric expertise among emergency healthcare providers, atypical disease presentations, and risks of misdiagnosis, iatrogenesis, health deterioration, and mortality [5, 8–12]. Although most ED admissions for NHRs are deemed necessary, their adverse consequences have prompted efforts to identify potentially avoidable admissions [10]. Reducing avoidable admissions could help mitigate health risks for NHRs and decrease overall healthcare costs [11, 13].
It has been well established that no consensus currently exists regarding the definition of "avoidable" in this context [11, 13]. As such, various terms have been employed, including "avoidable," "preventable," and "inappropriate," often preceded by "potentially," highlighting the complexity of assessment [14]. Reported rates range from 4 to 55%, depending on the context, definition, study design (prospective or retrospective), and measurement tools [2, 11, 15–22]. Additionally, perspectives vary between NHRs, families, caregivers, clinicians, and policymakers [13, 23].
The decision-making process for transferring NHRs to the ED is complex and can lead to admissions being deemed avoidable due to a multitude of factors:
- Clinical context: The nonspecific nature of health changes in NHRs frequently complicates the presumptive diagnosis [12, 20]. However, certain reasons for transfer may be adequately managed without ED evaluation, either because they are not severe or, as suggested by some authors, because they do not require diagnostic tests [15, 16, 24]. For example, a basic wound requiring only wound care.
- NHR preferences and advance care planning: Hospital admissions may be avoidable if advance care planning’s have not been established or respected [5, 23, 25], are misaligned with the NHR’s overall condition [16], or cannot be implemented by the nursing home (NH) [26].
- Family pressures: Family dynamics are particularly relevant in end-of-life situations [23, 26].
- Nursing home context: Avoidable admissions are associated with factors such as the unavailability of general practitioners (GPs) or specialist consultations [17, 25, 26], staff turnover, staffing levels (which are debated), and staff training [11, 13, 26, 27]. Organizational and communication challenges within NH teams [7, 23, 26, 28] and limitations in diagnostic and treatment resources [13, 14, 16, 26] also contribute to this issue.
- Healthcare policies: Contributing factors include hospital- and ED-centric care models, a lack of alternative pathways facilitating direct hospital admissions, a safety culture characterized by fear of litigation, economic constraints, and limited geriatric expertise within NHs [3, 13, 20, 23, 26, 29].
To our knowledge, the quantification of avoidable ED admissions for NHRs in Belgium has not been previously documented. Most of studies have been conducted in the USA and Canada, with limited data available from European countries, despite significant differences in healthcare systems [25]. The primary objective of this study is to quantify the annual percentage of avoidable ED admissions for NHRs in a Belgian hospital. Additionally, we evaluate and assess the use of a rapid decision-making tool as a screening method for identifying avoidable admissions and propose actionable recommendations for healthcare providers and policymakers.
Methodology
Study setting
The CHU UCL Namur (936 beds, including 300 university care beds and 73,694 annual ED admissions) operates across three hospital sites in the Namur province [30]. This study was conducted at the Godinne site, a rural university hospital. It has been reported in France that rural NHs transfer NHRs to hospitals less frequently than urban NHs [7]. In Belgium, 5% of individuals aged over 65 reside in NHs [29]. The Belgian long-term care system comprises short-stay centres, assisted living residences, residential homes, and nursing homes [31]. In this study, the term nursing home is used as a generic designation for all facility types. The level of care covered by public health insurance is determined by care dependency level. Services are delivered by public, non-profit, and for-profit providers, under federal and regional governance [31]. NHRs can visit EDs without prior approval from their GP. They may arrive via personal transportation or private ambulances, both allowing choice of hospital but at the NHR’s expense. Alternatively, public emergency services (via the European emergency number 112) can dispatch an ambulance for a fixed fee, typically transporting the NHR to the nearest hospital. Depending on the situation, a physician-staffed or a nurse -staffed ambulance may also be sent. GPs in Belgium are self-employed and are legally obligated to participate in on-call duties [29].
Study design and eligibility criteria
Single-centre, descriptive, retrospective study based on data collected from the medical records of all ED admissions involving NHRs aged 70 years or older, between January 1 and December 31, 2022. This study received approval from the hospital's ethics committee in December 2022, with a waiver of informed consent, as data were exclusively obtained from medical records (NUB: B0392025000041).
Data collection
Two authors (JG and JM) conducted the data collection. ED visits were pseudonymized. Data were manually extracted from ED reports and scanned documents, including letters from GPs or NHs, geriatric letters, hospitalization reports, and records from the belgian health network. Both authors cross-verified the coding and ensured there were no errors. The collected information encompassed sociodemographic data, frailty scores, geriatric scales, comorbidities (including chronic behavioural disorders, classified under “psychogeriatric patient”), and treatments (all medications listed in the Belgian Centre for Pharmacotherapeutic Information compendium, including "pro re nata"). NH characteristics (type, distance from the hospital, dementia units) were also documented. Furthermore, parameters related to ED stays were recorded (timing, mode of transport, decision-maker, length of stay, hospital admission, or discharge home), as well as presenting complaints for admission, in addition to diagnoses, examinations, and administered treatments. A distinction was made between "minor catheter-related issues" (e.g., flushing gastrostomy or cystocath, or urinary catheter placement) and "complex catheter-related issues", which necessitated device replacement by a specialist. Multiple admissions within the year for the same NHR were considered independent events for the assessment of avoidability. Costs were evaluated using the hospital billing service and ambulance cost calculations. Data collection adhered to a written protocol, and any discrepancies were resolved by consensus.
Outcomes measurement
Defining the avoidability of ED admissions remains a challenge due to the absence of a standardized definition [11]. The systematic review conducted by Renom-Guiteras et al. highlights the heterogeneity of assessment tools and the lack of a comprehensive instrument that incorporates all relevant factors, such as NHR characteristics and the preferences of both NHRs and their families [32]. Similarly, a recent systematic review by Makhmutov et al., which examined assessment tools for avoidable care transitions in older adults, reached a similar conclusion: existing instruments lack comprehensiveness, as they address only a limited number of perspectives [33]. Two primary approaches are commonly utilized:
- The first approach relies on the concept of "ambulatory care sensitive conditions" (ACSCs) and defines avoidable admissions as those resulting from a failure of preventive care [2, 6, 18, 21, 34, 35]. This list of conditions (e.g., heart failure, chronic obstructive pulmonary disease), has been established, and these diagnoses can be easily identified using International Classification of Diseases and Related Health Problems (ICD-10) codes, which can be automatically extracted from databases retrospectively [2, 34].
- The second approach focuses on admissions involving “low-acuity” visits that do not necessitate ED management and could instead be safely handled within the NH [6, 16, 17, 19, 36]. These visits typically encompass low-severity diagnoses (e.g., minor wounds, uncomplicated urinary tract infections, and mild dehydration) which exhibit low triage urgency and result in frequent discharges back to the NH [6, 9, 35]. Such admissions often reflect deficiencies in resources, medical expertise, or diagnostic capabilities within NHs. Their assessment is based on various methods, including chart reviews guided by explicit criteria, expert judgment regarding the necessary level of care, and/or structured tools such as numerical appropriateness scales, structured implicit review forms, or the Appropriateness Evaluation Protocol [2, 15–18, 20, 22, 37, 38].
We opted for the term "avoidable" rather than "inappropriate". Working retrospectively, not all perspectives or contextual factors could be collected. Indeed, it was thus less feasible to state about «failure of preventive care», which limits the appropriateness of using the term "inappropriate." [15]. We therefore focused on low-acuity visit more than on ACSCs.
Two approaches were employed in our analysis: (1) a retrospective assessment tool (Fig. 1) designed to determine the avoidability of ED admissions among NHRs, based on criteria derived from the literature and retrospectively available in medical records, developed by the authors. Additional file 1 presents these criteria. (2) an independent clinical judgment by two geriatricians with heterogeneous backgrounds: one senior physician who had led the literature review on the concept of avoidable hospital admissions, and one junior physician in her final year of geriatric training, conducting a master's thesis on the topic. They independently answered the question, “Was this admission avoidable?” without being influenced by the NHR 's outcome.Fig. 1. Retrospective assessment tool. ED, emergency department; CT, Computed tomography
The evaluations were conducted independently of the retrospective assessment tool and of each other. Disagreements were resolved through consensus, and the reproducibility of the judgments was analysed. This dual approach, combining an explicit tool with subjective clinical judgment, takes into account implicit and contextual factors [16, 32, 37].
Lastly, we calculated the costs based on the hospital billing records for each visit considered avoidable. The calculation of ambulance costs also took into account the distance travelled, and the pricing depending on whether the intervention involved the 112-emergency service or not.
Statistical analysis
Quantitative variables were presented as mean (SD – standard deviation) for normal distributions or as median (first and third quartile [Q1–Q3]) for non-normal distributions, as determined by the Shapiro–Wilk test. Categorical variables were analysed using the Chi-squared test of independence or Fisher's exact test. Quantitative variables were compared utilizing Student’s t-test or the Mann–Whitney U test, depending on the data distribution. The threshold for statistical significance was established at 5%. Inter-rater agreement was assessed using Cohen’s kappa coefficient. No records were excluded, even in the presence of missing data. All analyses were conducted using R software, version 4.3.1 (2023–06-16). Variables unrelated to the ED were analyzed using univariate binomial logistic regression to evaluate their potential in predicting the risk of avoidable admission. Variables demonstrating a significant association (p < 0.10) were subsequently included in the multivariate regression. A stepwise regression approach, incorporating both forward and backward selection, was employed to optimize the model’s Akaike Information Criterion and identify independent predictors of avoidable admission.
Results
Population and NHs description
In 2022, a total of 16,476 visits to the ED were recorded, of which 4,057 involved patients aged over 70 years (24.6%). Among these, 327 visits were attributed to NHRs, accounting for 8.1% of ED visits in the > 70 age group. The 327 admissions involved 246 NHRs, with 20.7% presenting multiple times throughout the year (See Additional file 2). The characteristics of the study population are summarized in Table 1. The median age was 86 years [81–90], and 67.9% of the population were women. The NHRs exhibited a high level of frailty: a median Clinical Frailty Scale score of 7 [6, 7] and a median Katz index of 15 [11–20]. Additionally, 57.3% required assistive devices for mobility, 19.0% were bedridden, and the median Charlson Comorbidity Index was 7 [6–8]. Furthermore, 55.7% of the NHRs had moderate to severe major neurocognitive disorders, 25.7% presented with behavioural disorders. Polypharmacy was prevalent, with a median of 11 medications [8–14]. NHRs were admitted from 51 NHs, of which 11 (21.6%) were public, 19 (37.3%) were private for-profit facilities, and 21 (41.2%) were non-profit associations. Among these facilities, 82.3% offered multiple services (assisted living residences, residential homes, and nursing homes), while 11.8% provided only beds under the status of residential homes, and 5.9% were classified solely as assisted living residences. Eleven NHs (21.6%) had a dedicated protected unit for NHRs with cognitive impairment. The median distance between the NHs and the hospital was 28 km [17.1–41.9], which corresponded to a median travel time of 32 min [20.5–40.5].Table 1population and nursing homes characteristicsNon-avoidable^a^(N = 253)Avoidable^a^(N = 74)All N = 327p-valueAge, y86 [81–91]87 [81–89]86 [81–90]0.987Women178 (70.4%)44 (59.5%)222 (67.9%)0.104ISAR4 [3, 4]4 [3, 4]4 [3, 4]0.904 Missing37 (14.3%)20 (27.0%)57 (17.4%)ISAR at 0 or 1: low risk0 (0.0%)1 (1.9%)1 (0.4%)0.200ISAR greater than or equal to 2: at risk216 (100.0%)53 (98.2%)269 (99.6%)Clinical Frailty Score7 [6, 7]7 [6, 7]7 [6, 7]0.941 Missing103131 to 4: Very Fit to vulnerable0 (0%)0 (0%)0 (0%)0.6785: Mildly Frail9 (3.7%)1 (1.4%)10 (3.2%)6: Moderately Frail71 (29.2%)24 (33.8%)95 (30.3%)7: Severely frail156 (64.2%)43 (60.6%)199 (63.4%)8: Very severely Frail6 (2.5%)3 (4.2%)9 (2.9%)9: Terminally1 (0.4%)0 (0.0%)1 (0.3%)Katz Score (/24)15 [11–20]15 [12.2–20]15 [11–20]0.459 Missing60 (23.7%)20 (27.0%)80 (24.5%)Mobility0.766 Bedridden49 (19.8%)11 (15.9%)60 (19.0%) Dependant on assistive device140 (56.7%)41 (59.4%)181 (57.3%) Independent58 (23.5%)17 (24.7%)75 (23.7%) Missing6511Number of medications on the treatment list11 [8–14]11 [7–13]11 [8–14]0.340Central nervous system acting drugs (number)2 [1–3]2 [1, 2]2 [1–3]0.075Charlson (/37)7 [6–8]7 [6–9]7 [6–8]0.619** Age0.963 70–79 years61 (24.1%)17 (23.0%)78 (23.9%) ≥ 80 years192 (75.9%)57 (77.0%)249 (76.2%) Myocardial infarction** > 0.999 Yes68 (26.9%)20 (27.0%)88 (26.9%)** Congestive Heart Failure0.651 Yes88 (34.8%)23 (31.1%)111 (33.9%) Peripheral vascular disease0.241 Yes47 (18.6%)19 (25.7%)66 (20.2%) Cerebrovascular Accident or Transient Ischemic Attack0.703 Yes74 (29.3%)24 (32.4%)98 (30.0%) Dementia0.855 Yes142 (56.1%)40 (54.1%)182 (55.7%) Chronic Obstructive Pulmonary Disease0.410 Yes69 (27.3%)16 (21.6%)85 (26.0%) Connective tissue disease** > 0.999 Yes10 (3.9%)3 (4.1%)13 (4.0%)** Peptic ulcer disease0.895 Yes88 (34.8%)27 (36.5%)115 (35.2%) Liver disease0.636 Mild7 (2.8%)3 (4.1%)10 (3.1%) Moderate to severe7 (2.8%)3 (4.1%)10 (3.1%) Diabetes mellitus0.176 Uncomplicated22 (8.7%)8 (10.8%)30 (9.2%) End-organ damage26 (10.3%)13 (17.6%)39 (11.9%) Hemiplegia0.693 Yes23 (9.1%)5 (6.8%)28 (8.6%) Moderate to severe chronic kidney disease0.357 Yes7 (2.8%)0 (0.0%)7 (2.1%) Solid tumor0.299 Localized19 (7.5%)10 (13.5%)29 (8.9%) Metastatic14 (5.5%)4 (5.4%)18 (5.6%) Leukaemia** > 0.999 Yes5 (1.9%)1 (1.4%)6 (1.8%)** Lymphoma0.717 Yes8 (3.2%)3 (4.1%)11 (3.4%) AIDS** Yes000Psychogeriatric patient65 (25.7%)19 (25.7%)84 (25.7%) > 0.999Nursing homes characteristicsPrivate for-profit facilities98 (38.7%)36 (48.7%)134 (41.0%)0.164Non-profit associations120 (47.4%)30 (40.5%)150 (45.9%)0.361Public39 (15.4%)10 (13.5%)49 (15.0%)0.827Total number of beds144 [124–170]150 [92.5–182]144 [124–170]0.852Alzheimer specific unit91 (36.0%)30 (40.5%)121 (37.0%)0.562Distance from ED, km11.5 [3–22.3]11.1 [3.0–22.3]11.5 [3.0–22.3]0.626Distance from ED, min15 [6–25]14 [6–25]15 [6–25]0.638ISAR, Identification of Seniors At Risk; AIDS, Acquired immunodeficiency syndrome; NH, nursing home; ED, emergency departmentValue are mean ± SD, n (%) or median [p25-p75]^a^Avoidable or not based on the assessment of two geriatricians. The analyses were conducted both by considering uncertain cases as non-avoidable and by treating them as a separate group. The observed differences remained statistically significant when categorizing admissions as avoidable or not based on the retrospective assessment tool
ED admission description
The characteristics of ED visits are outlined in Table 2. Regarding transport, 88.6% arrived by ambulance, comprising 49.5% using emergency medical services, 21.7% arriving by private ambulance, and 17.4% through physician-staffed ambulance. In the cohort, 52.9% were referred by their GP (either via telephone or following a consultation). The primary presenting complaints for admission included falls and suspected fractures (21.0%), respiratory symptoms (9.3%), and confusion (8.1%). The most common diagnoses were fractures or functional decline (15.1%), delirium (7.2%), and pneumonia (6.2%). Additional diagnostic tests were performed in 92.4% of cases. Among the NHRs, 23 (7.0%) had a care plan classified as palliative, of whom 21 had underwent at least one diagnostic test. The median duration of stay in the ED was 304 min [233–411], and 43.1% of NHRs returned to their NH following the ED visit.Table 2. Characteristics of ED visitsNon-avoidable^a^(N = 253)Avoidable^a^(N = 74)All N = 327 p-valueDay of admission0.08Weekend, public holiday or overnight89 (35.2%)18 (24.3%)107 (32.7%)Business day164 (64.8%)56 (75.7%)220 (67.3%) Monday32 (12.7%)16 (21.6%)48 (14.7%)0.083 Tuesday30 (11.9%)8 (10.8%)38 (11.6%)0.967 Wednesday21 (8.3%)7 (9.5%)28 (8.6%)0.938 Thursday31 (12.3%)15 (20.3%)46 (14.1%)0.120 Friday49 (19.4%)10 (13.5%)59 (18.0%)0.327Length of stay in the ED, min324 [249–424]245 [146–302]304 [233–411]** < 0.001Mode of transportation**Private ambulance49 (19.4%)22 (29.7%)71 (21.7%)0.011Emergency medical service (112)127 (50.2%)35 (47.3%)162 (49.5%)Physician-staffed ambulance (112)52 (20.6%)5 (6.8%)57 (17.4%)Personal transportation25 (9.9%)12 (16.2%)37 (11.3%)**Who refers the patient to the ED?**0.709Patient or relatives4 (1.6%)2 (2.7%)6 (1.8%)NH113 (44.7%)35 (47.3%)148 (45.3%)GP or on-call GP136 (53.8%)37 (50,0%)173 (52.9%)Transition of care letter from the NH203 (80.2%)48 (64.9%)251 (76.8%)**0.009Referral letter from the GP106 (41.9%)30 (40.5%)136 (41.6%)0.941Pre-existing and established palliative care plan before admission17 (6.7%)6 (8.1%)23 (7.0%)0.879Assessment conducted in the emergency department248 (98.0%)54 (73.0%)302 (92.4%) < 0.001Blood test233 (92.1%)44 (59.5%)277 (84.7%) < 0.001Arterial blood gas analysis90 (35.6%)2 (2.7%)92 (28.1%) < 0.001Blood cultures75 (29.6%)4 (5.4%)79 (24.2%) < 0.001Urine culture sediment117 (46.3%)15 (20.3%)132 (40.4%) < 0.001COVID-19 swab82 (32.4%)6 (8.1%)88 (26.9%) < 0.001X-ray172 (68.0%)30 (40.5%)202 (61.8%) < 0.001CT scan, ultrasound, MRI134 (53.0%)20 (27.0%)154 (47.1%) < 0.001Electrocardiogram184 (72.7%)22 (29.7%)206 (63.0%) < 0.001Specialist consultation required223 (88.1%)23 (31.1%)246 (75.2%) < 0.001Treatment administered in the ED** Oral65 (25.7%)20 (27.0%)85 (26.0%)0.936 Intravenous174 (68.8%)13 (17.6%)187 (57.2%)** < 0.001** Aerosols24 (9.5%)1 (1.4%)25 (7.7%)0.039 Oxygen therapy57 (22.5%)2 (2.7%)59 (18.0%)** < 0.001Wound suturing5 (2.0%)5 (6.8%)10 (3.1%)0.051Patient spent the night in the ED28 (11.1%)6 (8.1%)34 (10.4%)0.605Patient died during the ED stay2 (0.8%)0 (0.0%)2 (0.6%) > 0.999Discharge destination from the ED < 0.001Hospitalization177 (70.0%)7 (9.5%)184 (56.3%)Nursing home74 (29.3%)67 (90.5%)141 (43.1%)Death2 (0.8%)0 (0.0%)2 (0.6%)Patient refuses hospitalization4 (1.6%)4 (5.4%)8 (2.5%)0.081Hospitalization within 10 days prior**16 (6.32%)11 (14.86%)27 (8.26%)0.035ED, emergency departement; NH, nursing home; GP, general practionner; COVID-19, coronavirus disease; CT-scan, Computed tomography; MRI, Magnetic resonance imagingValue are mean ± SD, n (%) or median [p25-p75]Values in bold indicate statistically significant p-values (p < 0.05)^a^Avoidable or not based on the assessment of two geriatricians. The analyses were conducted both by considering uncertain cases as non-avoidable and by treating them as a separate group. The observed differences remained statistically significant when categorizing admissions as avoidable or not based on the retrospective assessment tool
Avoidable admissions
According to the clinical judgment of two geriatricians, 22.6% of admissions were deemed avoidable, with an inter-rater agreement of 86.9% (substantial agreement, Cohen’s kappa: 0.66). Disagreements in clinical judgment were noted for 43 cases (13.2%), of which consensus was reached for 34 cases following review (79.1%), while 9 cases remained unresolved due to insufficient detail/information (Fig. 2). These unresolved cases were subsequently classified as non-avoidable. The retrospective assessment tool yielded a more conservative avoidability rate of 14.1%. This tool analysis demonstrated a specificity of 98.4% and a sensitivity of 56.8%, with an Area Under the Curve (AUC) of 0.776 (95% CI: 0.71–0.89). High positive and negative predictive values were obtained at 91.3% and 88.6% respectively.Fig. 2. Agreement – disagreement: flow chart. At first review, the two geriatricians agreed on 284 cases and disagreed on 43. After re-evaluation, 9 disagreements remained. These 9 cases were considered non-avoidable for the purpose of analysis
No significant differences were observed in population characteristics based on whether the admissions were deemed avoidable or not. We were unable to demonstrate any association between NH characteristics and the avoidability of admissions (Table 1).
Avoidable admissions were associated with shorter ED stays, the absence of diagnostic tests, and a higher frequency of discharges back to the NH. No significant differences were observed regarding the timing of admission (weekdays vs. nights/holidays) or the referring individual. However, a large part of avoidable admissions were transported by ambulance (83.8%), with 64.5% of them arriving under the regulation of the 112 european emergency number. Avoidable admissions were less likely to include a transfer letter from the NH. The most frequent presenting complaints and diagnoses for avoidable admissions are summarized in Fig. 3. Prominent presenting complaints include falls, minor catheter-related issues, and wounds.Fig. 3. Presenting complaints and Diagnoses in Avoidable Cases
Costs
The total cost of the 74 avoidable admissions, calculated based on hospital billing (including examinations and monitoring fees), amounted to €14,624.81. The median cost per avoidable admission was €136.94 [€96.59–€209.04], with a range from €45.26 to €888.63. The costs related to ambulance transportation amounted to €8,615.77. This amounts to a total of €23,240.58, of which nearly 40% corresponds to transportation costs, borne by the patient.
Predictors of avoidable admission
The variables significantly associated with avoidable ED admissions according to clinical judgment, independent of emergency department-related factors, are summarized in Table 3. In the univariate analysis, the timing of admission, mode of transport, and presence of an explanatory letter from NH influenced the likelihood of avoidable admission. Additionally, recent hospitalization within the previous 10 days, refusal of hospitalization, and an increased number of central nervous system-acting drugs were also linked to avoidability. Among the most common presenting complaints for transferring NHRs, falls with suspected fractures, catheter-related issues, wounds, and pain without prior treatment attempts were all associated with avoidable ED admissions. In the multivariate analysis, five variables emerged as independent predictors of avoidable admissions: hospitalization within 10 days prior, pain without truing a treatment, falls with suspected fractures, admission on Mondays, and ambulance transport. The area under the operating curve ROC (receiver operating characteristic) of the multivariate model is 0.794 [95% CI: 0.697–0.892].Table 3. Univariate and multivariate analysis of avoidable admissionUnivariate regressionMultivariate regressionOR95% CIP valueOR95% CIP valueMinor catheter-related issues9.9483.929–25.189 < 0.001Wound4.7051.806–12.2570.002Transition of care letter from the NH0.4550.257–0.8030.007Physician-staffed ambulance0.280.108–0.730.009Number of Central nervous system acting drugs, by 10.8160.663–1.0040.054Admission on weekend, public holiday or overnight0.5820.323–1.050.072Patient refuses hospitalization3.5570.868–14.5850.078Hospitalization within 10 days prior2.5861.143–5.8510.0236.1131.125–33.2160.036Pain without prior treatment6.0651.99–18.4840.0024.8250.85–27.3980.076Fall and suspected fracture3.1331.561–6.2880.0013.5121.149–10.7320.027Admission on Mondays1.9050.979–3.7090.0583.1830.963–10.5240.058Private ambulance transport1.7610.978–3.1710.0592.9920.999–8.9620.05NH, nursing home
Discussion
This study presents the first quantitative evaluation of potentially avoidable ED admissions among NHRs in Belgium. Using a dual-assessment approach–combining structured clinical judgment and a retrospective assessment tool–we found that approximately 22.6% of ED visits could be considered avoidable, with a more conservative estimate of 14.1% derived from the retrospective assessment tool (consistent with its stringent criteria). These results fall within the range reported in international literature (4% to 55%) and underscore the influence of methodological variability, inconsistent definitions, healthcare system structures, and differing perspectives [2, 11, 13, 15–23]. More specifically, our rate of avoidable admissions aligns within the range reported in other studies utilizing the definition of low-acuity visits, i.e., transfers that could have been managed within the NH [6, 9, 15, 17, 22, 38].
Our choice of the term "avoidable" rather than "inappropriate" reflects the retrospective nature of our analysis and acknowledges the multifactorial, context-dependent decision-making process surrounding ED transfers. This aligns with existing literature that highlights the complexity and subjectivity of avoidability assessments, especially when multiple stakeholders are involved [13, 32, 33].
Avoidable admissions in our cohort were characterized by less severe clinical presentations, shorter ED stays, fewer diagnostic procedures, and a higher likelihood of discharge back to the NH. The most frequent presenting complaints included falls and suspected fractures, minor catheter-related issues, wounds, non specific complain and pain without prior treatment – conditions that could likely have been managed on-site given adequate resources and clinical support. These findings reinforce concerns raised in earlier studies regarding the limitations in diagnostic capacity, staff expertise, and clinical decision-making confidence within NHs [6, 9, 36].
Multivariate analysis identified five independent predictors of avoidable admissions: hospitalization within 10 days prior, pain without truing a treatment, falls with suspected fractures, admission on Mondays, and ambulance transport. These variables reflect both systemic and organizational weaknesses. For example, Monday admissions may stem from delayed decisions over the weekend, while recent hospitalizations suggest possible premature discharges or inadequate post-discharge planning. The frequent use of ambulance transport for low-acuity conditions also highlights the need to revisit triage protocols and develop alternative care pathways.
Interestingly, structural features of NHs–such as facility type, profit status, specialized Alzheimer’s units, and distance from the hospital–were not associated with avoidable admissions. Prior literature has noted that Alzheimer’s units and public facility status can influence transfer rates [17, 18]. The distance from the hospital also showed no clear relationship with avoidability, consistent with mixed findings in existing studies [18]. Our results align with past studies suggesting that such transfers are more influenced by internal practices, care culture, and staff capacity than by institutional characteristics [11, 13, 23, 26].
From an economic standpoint, the avoidable admissions in this study resulted in direct hospital costs and transportation cost exceeding €23,000 annually–excluding indirect costs. Cost evaluation remains challenging, as not all procedures performed during avoidable admissions are unnecessary. Some NHRs may still require diagnostic evaluations outside the ED, and ambulance use may be unavoidable in certain clinical contexts. While modest on a per-facility basis, this figure underestimates the broader societal impact when scaled to the national level. These findings highlight the potential for significant cost savings and improved care outcomes through better management of NHRs prior to ED admission [8, 11, 13].
The study population displayed high levels of frailty, multimorbidity, cognitive impairment, and polypharmacy, consistent with previous literature [9, 18, 39]. However, no specific NHR -level characteristics were independently predictive of avoidability. While factors like age, dementia, and indwelling devices use have been associated with ED transfers, they are insufficient for identifying avoidable admissions [4, 34, 40]. Our findings instead point to situational and organizational factors as key drivers.
Most ED visits, including avoidable ones, occurred during working hours, with a peak on Fridays, as observed by others [3, 10, 16, 18, 36, 40]. This contradicts the assumption that inappropriate transfers mainly occur during weekends or nights due to reduced staffing [29] and suggests that system-level improvements–such as enhanced access to diagnostics and treatment during working hours–could reduce ED admission [3, 8, 36]. NHRs are mainly transported by ambulance, and medically-assisted transport is less frequently avoidable–a finding also reported by other authors [2, 3, 8, 10, 18, 40].
Notably, half of the transfers occurred without prior GP consultation, often based on NH staff decisions. Although clinical assessments by GPs are known to reduce avoidable transfers [19, 41], such assessments were not consistently documented in our cohort. This has been reported reflecting either the need for a prompt decision [18] or challenges in reaching the GP [40]. We did not assess the involvement of NHRs or families in the decision-making process, though literature suggests that such involvement is often minimal [42]. Finally, consistent with the findings from other studies, we did not observe a significant difference in the appropriateness of admissions based on the decision-maker [18].
Among the 327 visits, 43.1% of NHRs were discharged back to their NHs, and nearly half of these visits were considered avoidable. Nevertheless, an ED avoidable admission may still result in hospitalization, especially when clinical uncertainty, fear of under-treatment, or medicolegal concerns drive decisions [11, 16, 29].
In 92.4% of cases, diagnostic tests were performed–even in 73.0% of avoidable cases. However, the performance of an additional examination does not necessarily justify an ED admission [36], particularly in cases involving routine blood tests that could be conducted during office hours by the GP. In Belgium, patients can access basic X-rays and blood tests without going through the ED. Therefore, we concluded that the need for a simple examination available during working hours does not, by itself, warrant ED admission. Advanced imaging (CT-scans (Computed tomography) and ultrasounds), can also be accessed rapidly through an emergency referral by the GP; however, this process entails taking time to initiate the request and may involve a delay in availability. Our findings also underscore the challenges related to accompanying NHRs to medical examinations. In many cases, ED admissions could have been managed on an outpatient basis with the presence of someone to accompany the NHR. The use of the ED sometimes reflects a lack of logistical support for scheduled diagnostic procedures, leading to hospital admission for practical rather than clinical reasons. Nonetheless, some examinations performed during avoidable visits reflect concerns regarding litigation and an overly stringent application of the duty of care [3]. For instance, 27.0% of avoidable admissions involved advanced imaging. These findings are consistent with previous studies, particularly concerning cranial CT-scans performed on NHRs who were subsequently discharged [24].
Falls were the most frequent presenting complaint for admission–including among avoidable visits–highlighting their clinical and organizational complexity in NHs. Although most falls are minor [24, 36], some result in serious injuries requiring emergency care (e.g., fractures, cranial trauma) [43]. It is well known that the absence of clear history, heteroanamnesis, or NHR communication can complicate triage decisions [43, 44]. Within our cohort, falls classified as avoidable admissions were often associated with basic assessments (such as X-rays and blood tests), prompting questions regarding the necessity of ED admission. Effective fall management requires a combination of preventive strategies (e.g. medication reviews, environmental adaptations), decision-making algorithms to support NH caregivers, access to radiology services, and enhanced monitoring capabilities within NHs [16, 24, 36]. In Norway, for instance, mobile imaging services prevented up to 70% of transfers [45], although logistical barriers such as staffing and prescribing authority remain concerning [46].
Catheter-related issues were the second leading cause of avoidable transfers–a known risk factor for unnecessary ED use [4, 34, 35, 47]. Many of these issues involved minor procedures (e.g., flushing or replacement) that could be performed in NHs at the condition of better staff training and material provision [40].
Advance care planning was rarely documented in our cohort, despite its known role in reducing inappropriate care transitions [11, 19, 34]. Additionally, we observed a non-significant trend toward a higher frequency of hospitalization refusals in the avoidable admissions group. In Belgium, advance care planning is often incomplete or misaligned with NHR wishes [29], contributing to transfers that may not reflect care preferences. While palliative care plans were present in some cases, they do not necessarily include "do not hospitalize" directives and therefore did not always lead to classification as avoidable. Indeed, hospital admission is not always preferred in cases of imminent death, but nevertheless is not prohibited when symptoms are difficult to manage [16]
A major strength of our study lies in its methodology: data were rigorously collected and cross-validated by two authors, with high inter-rater agreement. The novel retrospective assessment tool, designed for simplicity and reproducibility, offers a practical tool for identifying avoidable admissions in real-time. We did not utilize the Structured Implicit Review tool, which requires unavailable retrospective data [16], nor the Appropriateness Evaluation Protocol (AEP), which tends to overestimate avoidable admissions [18]. Our goal is to provide a conservative, user-friendly tool that informs policymakers on strategies to reduce avoidable admissions, thereby minimizing the risk of misclassifying an admission as avoidable, which could restrict ED access for NHRs or compromise care [5, 14]. We did not investigate ambulatory care-sensitive conditions, which are often linked to severe outcomes, high hospitalization rates, and increased mortality [6]. Reducing avoidability to a single diagnosis oversimplifies transfer decisions [14, 23], which must consider severity, NHR needs, and NH capabilities [13, 14, 39]. The retrospective assessment tool is designed to quickly identify avoidable admissions without claiming to be exhaustive. Significant variability in avoidability assessments has been reported when different caregiver profiles are involved [20, 22, 48]. For instance, NH staff often estimate a lower number of transfers as avoidable [23]. Finally, the study provides the first quantification of this issue in Belgium.
However, several limitations must be acknowledged. The main limitation lies in the retrospective assessment of avoidability, combined with the single-center design and a limited patient sample. Indeed, the retrospective design limits our ability to capture contextual or psychosocial elements of the decision-making process. Our study included only NHRs who ultimately reached the ED, excluding potential under-referrals. Additionally, the lack of NH-level data prevented deeper insight into organizational practices and staff decision-making frameworks–an issue common to many clinician-led studies [14, 40]. Finally, while clinical judgment was used to enrich our analysis, it remains subjective and may vary across professional profiles [20, 22, 48].
Perspective
The findings of this study underscore several actionable strategies that may help reduce avoidable ED transfers among NHRs.
Firstly, improving access to outpatient diagnostic services, such as radiological imaging and routine blood testing, could enable more timely on-site management of common conditions–particularly those related to falls–thus reducing the need for ED attendance [20, 48].
Secondly, enhanced training for NH staff in procedures such as intra-veinous therapy, catheter management and basic wound care may empower them to manage low-acuity conditions without requiring hospital transfer [11, 20, 36, 48]. Some studies have explored hospital-at-home models in NHs. Kunkel et al. found that timely intravenous therapy reduced ED admissions [50]. In De Stampa et al., NH residence was associated with a lower 30-day readmission risk after hospital-at-home care involving notably intravenous therapy [51]. Expanding staff competencies in this way may contribute to safer and more autonomous care within the facility.
Thirdly, clinical evaluation by a GP prior to transfer should be encouraged wherever feasible, as this is associated with a lower likelihood of avoidable admissions [20, 29, 41]. Early assessment may aid in distinguishing between cases that require ED admission and those that could be managed within the NH.
Fourthly, advance care planning should be systematically promoted and documented to ensure that medical decisions are aligned with NHRs' individual preferences and care goals. The proactive establishment of advance care plannings has the potential to prevent transfers that do not reflect NHRs’ wishes, particularly in the context of multimorbidity or end-of-life care [9, 29].
Moreover, the establishment of geriatric outreach services or in-home consultations may provide valuable support in managing clinically complex, yet non-urgent, situations that might otherwise prompt an ED referral [29, 41]. Dai et al. reported a 36.1% reduction in hospital admissions after implementing an acute geriatric outreach service delivering hospital-level interventions [49].
Finally, the development of direct admission pathways to geriatric or others wards, bypassing the ED, could reduce the risks associated with ED stays while ensuring that necessary hospital care is provided efficiently and appropriately [52, 53].
Nevertheless, it is essential to recognise that NHs are, first and foremost, places of residence rather than medical institutions. Any proposed expansion of healthcare services within these settings must be carefully balanced against the need to preserve NHRs' autonomy, comfort, and quality of life [16]. Interventions should therefore be evaluated not only in terms of clinical efficacy but also with regard to their resource implications and acceptability to both staff and NHRs [10].
Conclusion
This study has quantified and provided valuable insights into the issue of avoidable ED admissions in Belgium. It also presents a specific tool for identifying and quantifying retrospectively avoidable admissions. The lack of significant differences in resident characteristics between avoidable and non-avoidable admissions suggests that system-level factors may play a more decisive role. In this perspective, concrete avenues for improvement are proposed, aiming to better target interventions.These initiatives must be carefully designed to enhance care quality without compromising NHR safety.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (DOCX 48 KB)Supplementary file2 (DOCX 74 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rapport annuel [https://www.chuuclnamur.be/wp-content/uploads/2023/11/com-213-01-01-web.pdf]
- 2Van den Bosch K, Willemé P, Geerts J, Breda J, Peeters S, Van De Sande S et al: Soins résidentiels pour les personnes âgées en Belgique: projections 2011 – 2025. In: KCE Reports. Bruxelles: Centre Fédéral d’Expertise des Soins de Santé (KCE); 2011. 10.57598/R 167B