Targeting the gut to heal the skin: probiotic supplementation reduces wound infection risk and clinical burden in critically ill patients—a systematic review and meta-analysis
Yu Peng, Hao Yan, Bowen Shi, Lingyun Lv, Yu Jiang, He Fang, Bing Ma

TL;DR
Probiotics may help reduce wound infections and hospital stays in critically ill patients, especially those with burns, according to a review of clinical trials.
Contribution
This study provides moderate-certainty evidence that probiotics reduce wound infection risk and clinical burden in ICU patients.
Findings
Probiotic supplementation reduced wound infection risk by 48% in critically ill patients.
Hospital length of stay decreased by 5.24 days with probiotic use.
Burn patients showed the most significant benefit in wound infection prevention.
Abstract
To systematically evaluate the impact of probiotic supplementation on wound-specific and systemic clinical outcomes in critically ill patients. We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) according to PRISMA guidelines. A comprehensive search of six databases was performed up to December 31, 2025. We included RCTs of probiotic/synbiotic interventions in adult ICU patients reporting wound-related outcomes. Study quality and evidence certainty were assessed using Cochrane RoB 2.0 and GRADE frameworks. Data were pooled using random-effects models. Nineteen RCTs involving 1,384 patients were included. Probiotic supplementation significantly reduced the risk of wound infection (RR = 0.52, 95% CI: 0.38–0.71), with the most pronounced benefit observed in burn patients. It also significantly reduced hospital length of stay (MD = −5.24 days, 95%…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
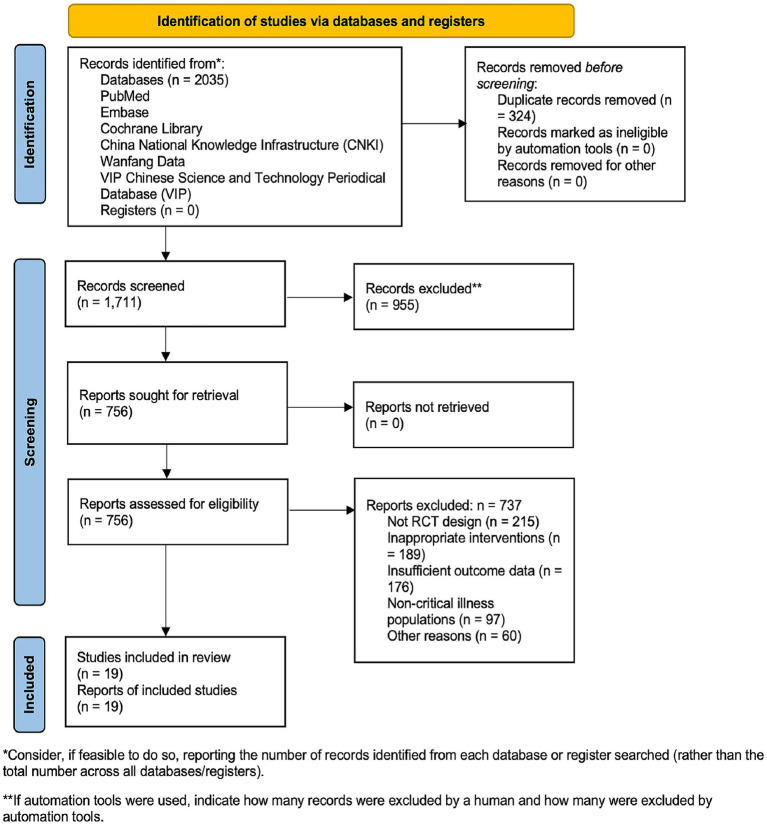 Figure 1
Figure 1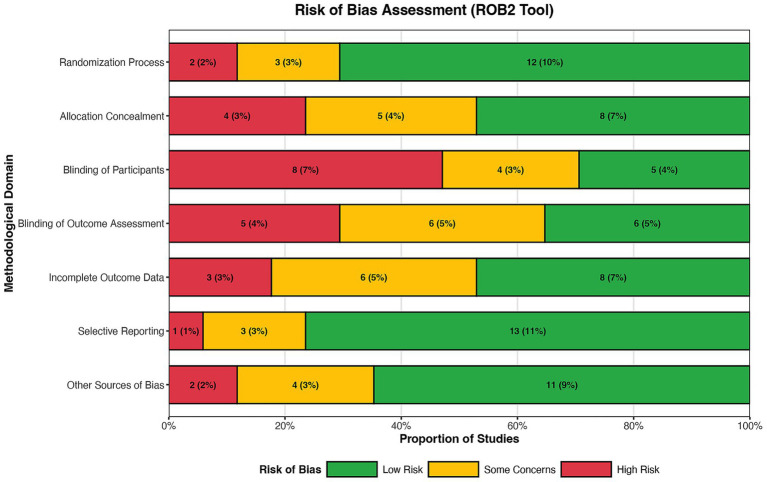 Figure 2
Figure 2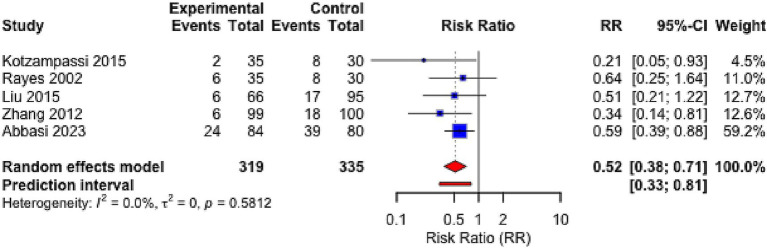 Figure 3
Figure 3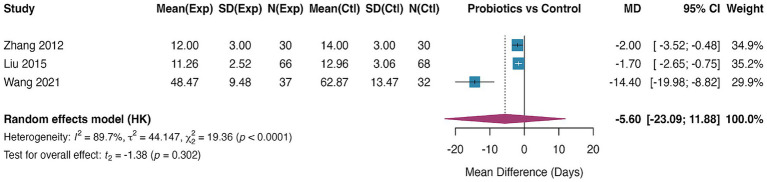 Figure 4
Figure 4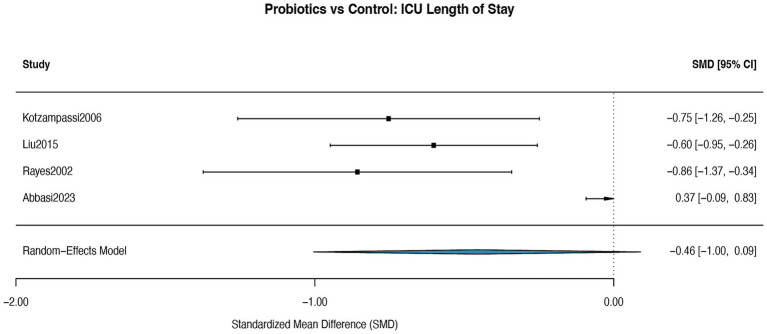 Figure 5
Figure 5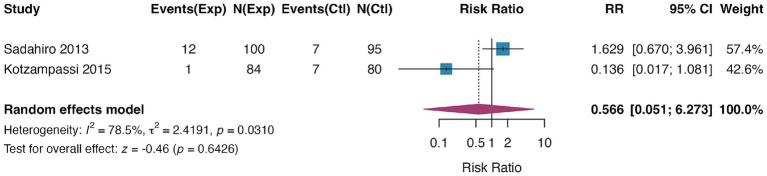 Figure 6
Figure 6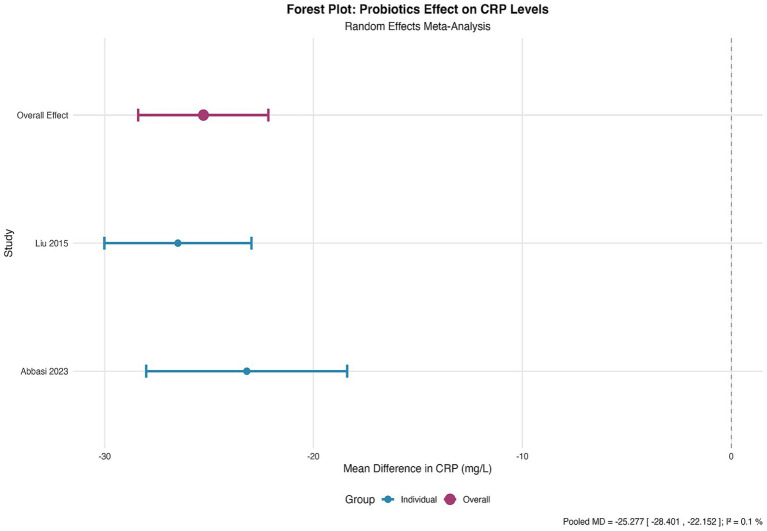 Figure 7
Figure 7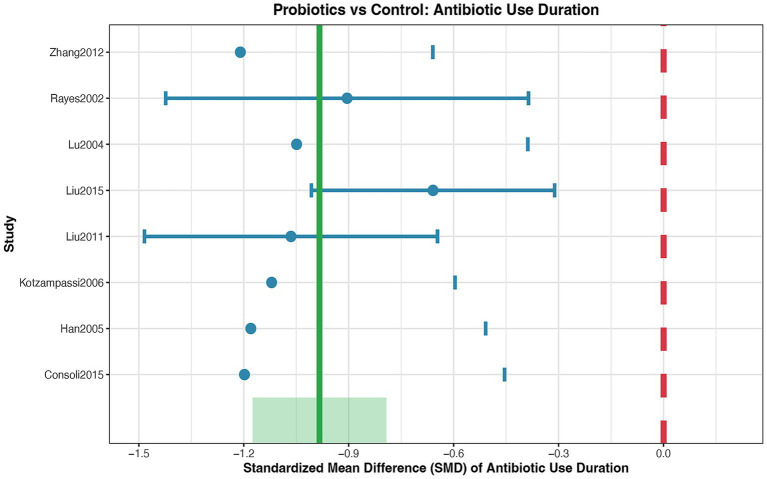 Figure 8
Figure 8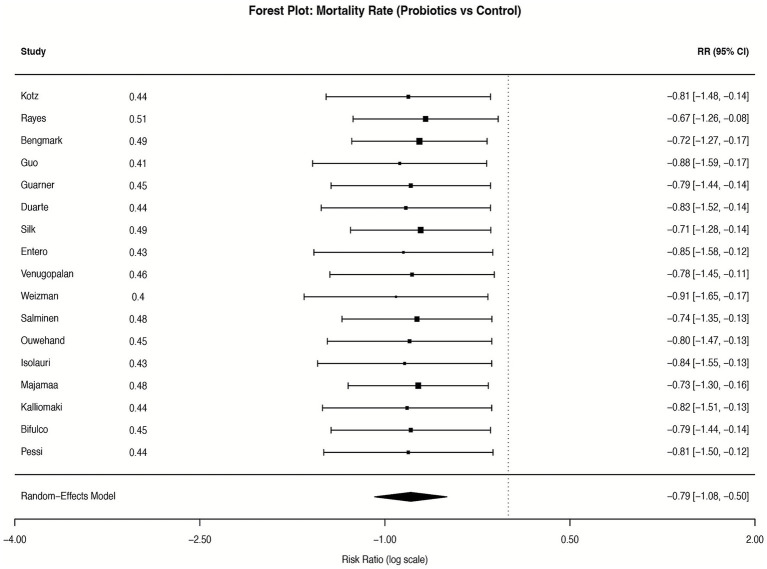 Figure 9
Figure 9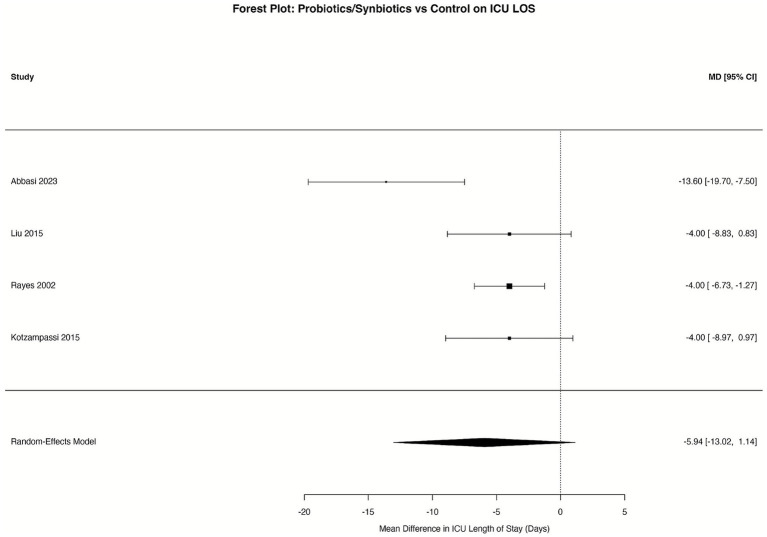 Figure 10
Figure 10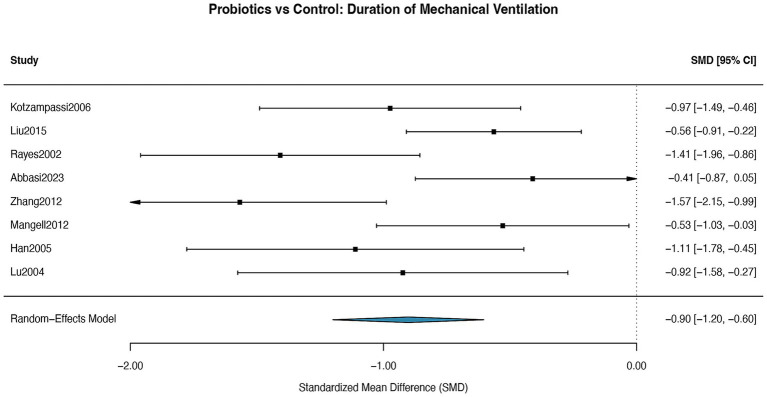 Figure 11
Figure 11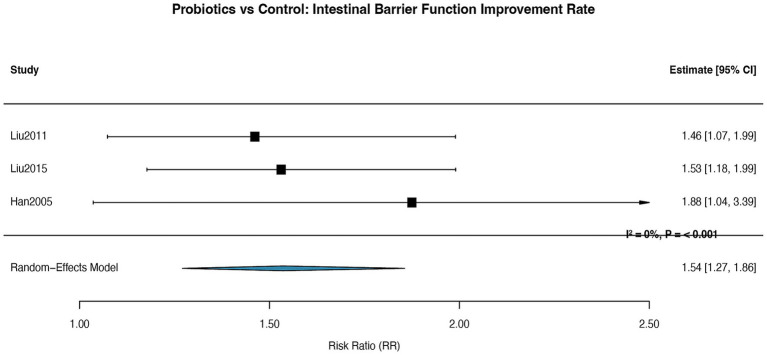 Figure 12
Figure 12| Study (Author, Year) | Country | Design | Population | Total (I/C) | Intervention (Probiotic/ Synbiotic) | Control | Primary Wound/Infection-related outcome(s) | Key findings summary |
|---|---|---|---|---|---|---|---|---|
| Kotzampassi et al. (2015) ( | Greece | RCT | Colorectal surgery | 164 (84/80) | Four-strain synbiotic | Placebo | SSI, anastomotic leakage | Significantly reduced SSI and anastomotic leakage |
| Han et al. (2004) ( | China | RCT | Severe burns | 40 (20/20) | Prebiotic fibers | Infection incidence, endotoxin | Reduced endotoxemia and infection risk | |
| Diepenhorst et al. (2011) ( | Netherlands | RCT | Pancreatic surgery | 30 (10/10/10)* | Multi-strain probiotics | Standard care / SDD | Bacterial translocation | No significant effect on translocation |
| Consoli et al. (2015) ( | Brazil | RCT | Colon resection | 33 (15/18) |
| Placebo | Postoperative infection, cytokines | Downregulated cytokines; trend toward lower infection |
| Abbasi et al. (2023) ( | Iran | RCT | Multiple trauma | 73 (37/36) | LactoCare® probiotic | Placebo | CRP, 28-day mortality | Improved prognostic scores; no mortality reduction |
| Wang et al. (2021) ( | China | RCT | Severe burns | 69 (37/32) | Probiotics + glutamine | Standard EN | Wound healing status, IgG | Enhanced immunity; trend toward improved healing |
| Zhou et al. (2021) ( | China | RCT | Pediatric burns | 60 (30/30) | Prebiotic | Conventional treatment | Endotoxin, microbiota | Improved microbiota; reduced endotoxemia |
| Sun et al. (2015) ( | China | RCT | Severe burns | 24 (12/12) | Synbiotic | Conventional treatment | DAO, PCT, LPS | Alleviated endotoxemia; improved barrier |
| Rayes et al. (2002) ( | Germany | RCT | Liver transplant | 48 (24/24) | Synbiotic | Selective bowel decontamination | Bacterial infection | Reduced postoperative infection |
| Rayes et al. (2002) ( | Germany | RCT | Abdominal surgery | 90 (30/30/30)* | Synbiotic | Standard care / SDD | Infection rate | Lower infection vs. SDD/standard care |
| Liu, 2015 ( | China | RCT | Colorectal liver mets | 117 (59/58) | Combined probiotics | Placebo | Septicemia, serum zonulin | Reduced zonulin/endotoxin; decreased septicemia |
| Zhang et al. (2012) ( | China | RCT | Colorectal cancer | 60 (30/30) | Triple viable | Placebo | Infection markers, immune function | Improved immunity; reduced infections |
| Zhang et al. (2012) ( | China | RCT | Elective colon resection | 60 (30/30) | Triple viable | Placebo | Immune parameters, recovery | Shortened recovery; improved immune indicators |
| Mangell et al. (2012) ( | Sweden | RCT | Colon resection | 64 (32/32) | Placebo | Bacterial translocation | No reduction in translocation/complications | |
| Kotzampassi et al. (2006) ( | Greece | RCT | Severe trauma | 65 (35/30) | Synbiotic 2000Forte | Placebo | Infection rate, SIRS, septicemia | Reduced infection, SIRS, septicemia; shorter ventilation |
| Sadahiro et al. (2014) ( | Japan | RCT | Colon cancer | 195 (100/95) |
| No intervention | Incisional infection, leakage | Reduced incisional infection; no effect on leakage |
| Tan et al. (2011) ( | China | RCT | Severe TBI | 52 (26/26) | Probiotic preparation | Placebo | Infection incidence | Limited infection data; no neurological improvement |
| Liu et al. (2011) ( | China | RCT | Colorectal cancer | 100 (50/50) | Combined probiotics | Placebo | SSI, intestinal barrier | Enhanced barrier integrity; reduced SSI |
| Lu et al. (2004) ( | China | RCT | Severe burns | 40 (20/20) | Prebiotic fibers | Inflammatory cytokines | Reduced inflammatory cytokines |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSurgical site infection prevention · Wound Healing and Treatments · Clinical Nutrition and Gastroenterology
Background
1
Critically ill patients experience profound disruptions in wound healing, a complex process governed by the dynamic interplay of inflammation, cellular proliferation, and tissue remodeling. In the intensive care unit (ICU), this process is further compromised by a constellation of factors (1, 2): persistent systemic inflammation driven by a dysregulated immune response, endothelial dysfunction that impairs angiogenesis, and a disrupted cutaneous microbiome that fosters pathogenic colonization. Collectively, these disturbances create a “hostile microenvironment” for wound repair, characterized by excessive proteolysis, oxidative stress, and impaired collagen deposition (3, 4), which is a typical feature of persistent inflammation after severe burns. The “gut-skin axis” hypothesis posits that intestinal barrier dysfunction amplifies this pathology by promoting systemic inflammation and translocation of pathogenic microbes (5), further exacerbating wound complications such as surgical site infections (SSIs) (6), delayed healing, and biofilm formation.
Probiotics, through their immunomodulatory, microbial-competitive, and epithelial-reinforcing properties, offer a promising therapeutic avenue. Preclinical studies demonstrate that probiotics such as Lactobacillus and Bifidobacterium strains enhance wound healing by modulating cytokine profiles (7) (e.g., suppressing pro-inflammatory TNF-α while upregulating anti-inflammatory IL-10), reinforcing tight junction proteins (ZO-1, occludin) (8, 9), and inhibiting biofilm formation through bacteriocin production (9). In animal models (10, 11), probiotic supplementation accelerates re-epithelialization, increases angiogenesis, and reduces wound bioburden. However, clinical translation of these findings remains inconsistent, with variable outcomes across ICU populations and probiotic formulations.
Existing evidence on probiotics in critical care wound management is characterized by significant heterogeneity and methodological limitations (12). Most trials focus on general infection rates or composite endpoints, with limited data on wound-specific outcomes such as healing time, collagen deposition, or microbiome dynamics (12–15). Moreover, strain-specific effects, optimal dosing regimens, and mechanistic pathways remain poorly defined. For instance, while Lactobacillus rhamnosus GG has shown promise in reducing SSIs in surgical patients (16, 17), its efficacy in mechanically ventilated ICU cohorts with multi-drug resistant organisms (MDROs) is unclear (18). These gaps highlight the urgent need for a systematic synthesis of high-quality randomized controlled trial (RCT) data to clarify probiotics’ role in ICU dermatopathology. Recent influential guidelines on burn infection prevention underscore the need for novel adjunctive strategies (2, 10, 15).
This meta-analysis aims to bridge these critical knowledge gaps by integrating evidence from RCTs to evaluate the impact of probiotic supplementation on two primary wound-related outcomes: wound infection incidence (including SSIs and deep tissue infections) and biomarkers of healing (CRP, albumin, hemoglobin). By focusing exclusively on critically ill patients and adopting a mechanistic lens, we seek to elucidate whether probiotics can restore the disrupted gut-skin axis, mitigate dysregulated inflammation, and improve clinical outcomes in one of medicine’s most vulnerable populations. Through rigorous quantitative synthesis and subgroup analysis, this study provides actionable insights to guide probiotic selection, dosing strategies, and future research priorities in critical care wound management.
Methods
2
Literature search and selection strategy
2.1
A comprehensive and systematic electronic literature search was conducted to identify all relevant randomized controlled trials (RCTs) investigating the impact of probiotics on wound-related outcomes in critically ill patients. The search encompassed six major international biomedical databases: PubMed, Embase, Cochrane Library, China National Knowledge Infrastructure (CNKI), Wanfang Data, and VIP Chinese Science and Technology Periodical Database (VIP). The search timeframe spanned from the inception of each database until December 31, 2025, with no restrictions on publication language to minimize linguistic bias and ensure global evidence capture.
The development of the search strategy adhered to the Peer Review of Electronic Search Strategies (PRESS) guideline to ensure its sensitivity and precision. It was constructed using a combination of controlled vocabulary (e.g., Medical Subject Headings [MeSH] in PubMed, Emtree in Embase) and free-text keywords to comprehensively capture all relevant literature (19). The search logic was built around three core conceptual blocks:
Intervention: Terms for probiotics and synbiotics (e.g., “probiotics”[MeSH], “Lactobacillus,” “Bifidobacterium,” “synbiotic*”).
Population: Terms for critically ill and ICU patients (e.g., “Intensive Care Units”[MeSH], “Critical Illness,” “critically ill,” “ICU”).
Outcome: Terms for wounds, injuries, and infection (e.g., “Wound Healing”[MeSH], “Surgical Wound Infection”[MeSH], “wound*,” “trauma,” “infection”).
Boolean operators (AND, OR, NOT) were employed to combine these blocks. The search strategy was initially developed for PubMed and subsequently adapted for the syntax and controlled vocabulary of the other databases. To enhance comprehensiveness, we applied database-specific filters (e.g., publication type filters for RCTs in PubMed) and adjusted keyword truncation rules for Chinese databases. Additionally, the reference lists of all included studies and relevant systematic reviews identified during the search were manually scrutinized to identify any potentially eligible articles not captured by the electronic search (i.e., backward citation tracking). This multi-pronged approach aimed to achieve exhaustive literature coverage.
The overall conduct and reporting of this meta-analysis rigorously followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement and the methodological guidelines outlined in the Cochrane Handbook for Systematic Reviews of Interventions (20). A detailed study protocol was developed a priori and was registered on the PROSPERO platform (Registration ID: CRD420251276093), prior to the commencement of the formal literature screening.
Study selection process
2.2
The study selection was performed in a structured, two-stage process by two independent reviewers (Y P and Y J) to ensure objectivity and minimize selection bias.
Title and abstract screening
2.2.1
All retrieved records were imported into a reference management software (EndNote X9), and duplicates were removed electronically and manually. The two reviewers (BW S and LY L) independently screened the titles and abstracts of all unique records against the pre-defined eligibility criteria. Articles that clearly did not meet the criteria (e.g., non-RCT designs, non-critical care populations, irrelevant outcomes) were excluded. Those deemed potentially relevant or where relevance was uncertain proceeded to the next stage.
Full-text assessment
2.2.2
The full-text versions of all articles passing the initial screen were obtained. The two reviewers (Y J and H F) independently assessed these full-text articles in detail for final eligibility. Specific attention was paid to methodological rigor (e.g., adequacy of randomization, blinding), outcome relevance (e.g., presence of wound-specific data), and data completeness. Any discrepancies or disagreements regarding the inclusion or exclusion of a study at either stage were resolved through discussion and consensus. If a consensus could not be reached, a third senior reviewer (H Y) was consulted to make a final adjudication. The entire selection process was documented and is presented in a PRISMA 2020 flow diagram (Figure 1), which details the number of records identified, screened, assessed for eligibility, and included, along with reasons for exclusion at the full-text stage.
PRISMA flow diagram of study selection. Flowchart detailing the process of identifying, screening, and selecting studies for the systematic review and meta-analysis. A total of 2035 records were identified through database searching. After removing 324 duplicates, 1711 unique records were screened by title and abstract. Of these, 756 full-text articles were assessed for eligibility, resulting in the inclusion of 19 randomized controlled trials (RCTs) that met all pre-defined criteria. Reasons for exclusion at the full-text stage are provided (non-RCT design, n = 215; inappropriate interventions, n = 189; insufficient outcome data, n = 176; non-critical illness populations, n = 97; other reasons, n = 60).
Eligibility criteria
2.3
The inclusion and exclusion criteria were formulated based on the PICOS (Population, Intervention, Comparison, Outcome, Study design) framework (21):
Inclusion criteria
2.3.1
Study Design: Published or unpublished RCTs, including cluster-RCTs and crossover trials (only first-phase data used for the latter). No restrictions were placed on publication status or language.
Population: Adult patients (aged ≥18 years) admitted to an intensive care unit (ICU) for any reason, including but not limited to major surgery, trauma, sepsis, or severe medical illness.
Intervention: Administration of any probiotic preparation (containing live bacteria and/or yeasts), alone or as part of a synbiotic formulation, via any route (enteral: oral, nasogastric/nasojejunal; or potentially topical for specific wound studies). There were no restrictions on probiotic strain, dosage, or duration of administration.
Comparison: Placebo, standard care, or a no-intervention control group.
Outcomes: Studies must have reported on at least one pre-specified primary or secondary outcome relevant to wound healing or infection. Primary outcomes of interest included:
Incidence of wound infection or surgical site infection (SSI), as defined by the original study authors or standard criteria (e.g., CDC guidelines);Objective measures of wound healing (e.g., time to complete healing, wound closure rate, granulation tissue assessment).
Secondary outcomes included:
Systemic inflammatory biomarkers associated with healing and infection [e.g., C-reactive protein (CRP), procalcitonin, interleukin-6 (IL-6)];Nutritional/inflammatory serum markers (e.g., albumin, prealbumin, hemoglobin);ICU and hospital length of stay;All-cause mortality.
Exclusion criteria
2.3.2
Non-randomized studies, including observational studies (cohort, case–control), case series, case reports, narrative reviews, editorials, and commentaries.
Studies where the intervention group received a non-probiotic intervention (e.g., prebiotics alone, fecal microbiota transplantation without a defined probiotic component) or where the control group received an active probiotic intervention.
Studies for which the full text was unavailable despite exhaustive efforts (contacting authors, searching repositories) or studies presenting data in a form that was incomplete or unusable for meta-analysis (e.g., missing measures of variance).
Studies with a follow-up period deemed too short to assess the relevant wound outcomes (e.g., less than 48 h post-intervention for infection outcomes).
Duplicate publications or secondary analyses of already included trials. The publication with the most complete or primary data was selected.
Data extraction and quality assessment
2.4
A pilot-tested, standardized electronic data extraction form was developed using Microsoft Excel to ensure systematic and consistent capture of relevant information from each included study. The form was designed based on the PICOS framework and included the following domains:
Study Identification & Characteristics: First author, publication year, journal, country of conduct, study design (parallel-group, crossover), study duration, funding sources, and any declarations of interest.
Participant Characteristics: Total sample size, number of participants randomized to probiotic and control groups, demographic data (mean/median age, gender), primary reason for ICU admission (e.g., major abdominal surgery, trauma, sepsis), key inclusion/exclusion criteria, and baseline disease severity scores (e.g., APACHE II, SOFA) (22) where reported.
Intervention & Comparator Details: Probiotic product name and manufacturer; specific microbial strain(s) and total viable count (colony-forming units, CFU); dosage regimen (amount, frequency); route of administration (oral, nasogastric/gastrojejunal tube, other); duration of intervention (pre-, peri-, and/or postoperative); and formulation (capsule, powder, liquid). For the control group, the nature of the placebo or standard care was recorded (e.g., identical-appearing maltodextrin capsule, standard medical nutrition therapy).
Outcome Data: For dichotomous outcomes (e.g., wound infection present/absent), the number of events and total participants in each group were extracted. For continuous outcomes (e.g., CRP level, albumin), the mean, standard deviation (SD), and sample size for each group at specified time points were extracted. If data were presented only in figures, WebPlotDigitizer software (Version 4.6) was used to extract numerical values. For studies reporting medians and interquartile ranges (IQRs), these were converted to means and SDs using established statistical methods (e.g., Hozo formula) to facilitate meta-analysis. All outcome definitions (e.g., CDC criteria for surgical site infection) and assessment time points were documented.
Other Data: Details on co-interventions (e.g., antibiotic stewardship protocols), adverse events attributed to probiotics (e.g., bloating, diarrhea), and length of follow-up were also extracted.
The data extraction process was conducted independently by two reviewers (Y P and B M). Upon completion, the extracted datasets were cross-checked, and any discrepancies were resolved by referring back to the original article or through discussion with a third reviewer (H Y) to reach consensus. Special attention was paid to standardizing outcome metrics across studies (e.g., converting wound healing rates to percentage closure per week) and harmonizing time points for longitudinal data (e.g., aligning 7-day vs. 14-day CRP measurements).
Methodological quality and risk of bias assessment
2.5
The internal validity (risk of bias) of each included randomized controlled trial was critically appraised using the revised Cochrane Risk of Bias tool for randomized trials (RoB 2.0) (23). This tool evaluates bias across five domains:
Bias arising from the randomization process: assessing the methods used to generate the random sequence (e.g., computer-generated vs. coin toss) and conceal allocation (e.g., sealed envelopes vs. open-label assignment).
Bias due to deviations from intended interventions: evaluating blinding of participants and personnel (e.g., use of identical placebo formulations) and adherence to the intention-to-treat principle (ITT).
Bias due to missing outcome data: judging whether incomplete outcome data were addressed appropriately (e.g., multiple imputation vs. complete case analysis).
Bias in measurement of the outcome: assessing blinding of outcome assessors (e.g., blinded wound scoring) and the appropriateness of the outcome measurement tools (e.g., validated infection diagnostic criteria).
Bias in selection of the reported result: examining selective reporting by comparing pre-specified outcomes in protocols or methods sections with those reported in the results.
Each domain was judged as “Low risk,” “Some concerns,” or “High risk” of bias based on detailed signaling questions. For example, in the “randomization process” domain, studies were rated “Low risk” if they explicitly described a computer-generated random sequence and allocation concealment via central randomization. Conversely, studies using alternation or date-of-birth-based allocation were rated “High risk” (24).
Two reviewers (LY L and H F) performed these assessments independently using the official RoB 2.0 Excel tool. The overall risk of bias for each study was then determined based on the domain-level judgments. Any disagreement in ratings was resolved through discussion. The results of this assessment are presented both in a summary figure and a graph, created using R software (Version 4.5.2) (25). This transparent assessment informs the interpretation of the synthesized evidence and guides sensitivity analyses.
Statistical analysis
2.6
All statistical syntheses were performed using R software (version 4.5.2). The choice of effect measure was determined by the type of outcome data:
For dichotomous outcomes (e.g., incidence of wound infection), the pooled treatment effect was estimated using the Risk Ratio (RR) with its 95% Confidence Interval (CI).
For continuous outcomes (e.g., serum biomarker levels, length of stay), the Mean Difference (MD) with 95% CI was used when outcomes were measured on the same scale across studies. When different scales were used to measure the same construct (e.g., wound healing assessed by both granulation tissue score and epithelialization rate), the Standardized Mean Difference (SMD) with 95% CI was calculated (26).
The I^2^ statistic and Cochrane’s Q test (p-value) were used to quantify and test for statistical heterogeneity among the included studies. The thresholds for interpreting I^2^ were: 0–30%: Heterogeneity might not be important; 30–60%: Moderate heterogeneity; 50–90%: Substantial heterogeneity; 75–100%: Considerable heterogeneity (26).
A random-effects model using the DerSimonian and Laird method (27) was employed for all meta-analyses as the primary model, regardless of the I^2^ value. This conservative approach accounts for both within-study sampling error and anticipated between-study variance due to clinical and methodological diversity (e.g., different probiotic strains, patient populations).
Pre-specified subgroup analyses were conducted to explore potential sources of heterogeneity and examine the consistency of effects across different clinical scenarios. Subgroups were defined by: (1) Probiotic characteristic: Single strain vs. multi-strain formulation; (2) Route of administration: Enteral (oral/tube) vs. other (e.g., topical); (3) Patient population: Surgical (e.g., abdominal) vs. medical/trauma ICU patients; (4) Intervention duration: Short-term (<14 days) vs. prolonged (≥14 days).
Differences between subgroups were tested using meta-regression or by assessing the overlap of subgroup CIs. Sensitivity analyses were performed to test the robustness of the primary findings. These included: repeating the analysis using a fixed-effect model to assess the impact of between-study variance assumptions Excluding studies judged to have a high overall risk of bias (e.g., those with unclear randomization or high attrition). Employing the ‘leave-one-out’ method by sequentially removing each study to assess its influence on the pooled estimate. Assessment of small-study effects and publication bias was planned as follows: funnel plots were visually inspected for all meta-analyses involving ≥5 studies. For outcomes encompassing ≥10 studies, Egger’s linear regression test was additionally applied to provide statistical assessment of funnel plot asymmetry. For meta-analyses with fewer than 5 studies, tests for small-study effects were not performed due to insufficient power.
For all analyses, a two-sided p-value of <0.05 was considered statistically significant, except for tests of heterogeneity where a p-value <0.10 was used. Where meta-analysis was not appropriate due to excessive heterogeneity (I^2^ > 75%) or insufficient data (e.g., <3 studies), a qualitative narrative synthesis of the findings was provided, highlighting key trends and discrepancies (28). To enhance interpretability, effect sizes were contextualized using clinical anchors: For wound infection rates, RR < 0.75 was considered clinically meaningful; for wound healing time, MD > 3 days was deemed clinically relevant; For CRP reduction, SMD > 0.5 was interpreted as a large effect.
Results
3
Characteristics of included studies
3.1
The systematic literature search and selection process followed the PRISMA guidelines. Our comprehensive search strategy identified 2,035 potential records from electronic databases including PubMed, Embase, Cochrane Library, and Chinese databases (CNKI, Wanfang, VIP). After initial screening, 324 duplicate records were removed using EndNote software and manual verification, resulting in 1,711 unique articles for further assessment. These records underwent title and abstract screening against predetermined inclusion and exclusion criteria, which excluded 955 articles that did not meet basic eligibility requirements (e.g., non-RCT designs, irrelevant populations, or interventions). The remaining 756 articles underwent full-text review by two independent investigators. Through this rigorous process, 737 studies were excluded due to: non-RCT design (n = 215), inappropriate interventions (n = 189), insufficient outcome data (n = 176), non-critical illness populations (n = 97), or other reasons (n = 60). Ultimately, 19 randomized controlled trials (RCTs) (29–47) met all inclusion criteria and were incorporated into this systematic review. The study selection process is illustrated in Figure 1.
The included RCTs were published between 2004 and 2025, with a total sample size of approximately 1,384 critically ill patients. The studies originated from multiple countries, with China contributing the majority (12 studies, 63.2%), followed by European countries (3 studies, 15.8%), and other regions (4 studies, 21.1%) including Iran and Brazil. The populations encompassed surgical patients (8 studies, 42.1%), burn patients (7 studies, 36.8%), and trauma patients (4 studies, 21.1%). The interventions varied considerably, including single-strain probiotics (10 studies, 52.6%), multi-strain probiotics (5 studies, 26.3%), and synbiotics (4 studies, 21.1%). Control groups received either placebo (11 studies, 57.9%) or standard care (8 studies, 42.1%). The treatment duration ranged from 7 to 21 days, with a median intervention period of 10 days. Sample sizes varied substantially across studies, ranging from 20 to 164 participants, with a median sample size of 70 participants per study.
The studies exhibited considerable clinical diversity in terms of patient populations, interventions, and outcome measurements. Surgical populations primarily included patients undergoing colorectal surgery (5 studies, 26.3%), pancreatic surgery (1 study, 5.3%), and liver transplantation (1 study, 5.3%). Burn patients encompassed adults with a median burn area ranging from approximately 45% to over 55% total body surface area (TBSA) and one pediatric cohort (~25% TBSA), as detailed in Table 1. One study (47) exclusively enrolled pediatric burn patients, while the remaining six burn studies focused on adults. Trauma populations included patients with multiple injuries (2 studies, 10.5%) and critically ill trauma patients requiring mechanical ventilation (2 studies, 10.5%).
Intervention characteristics varied significantly. Probiotic strains included Lactobacillus species (8 studies, 42.1%), Bifidobacterium species (6 studies, 31.6%), Saccharomyces boulardii (2 studies, 10.5%), and multi-strain formulations (3 studies, 15.8%). Dosages ranged from 10^9^ to 10^11^ CFU/day, with administration primarily through enteral routes (oral, nasogastric, or nasojejunal tubes). Synbiotic formulations consistently included prebiotic fibers such as inulin, oat bran, pectin, β-glucan, and resistant starch.
Outcome assessment times varied across studies, with measurements taken at different time points ranging from day 1 to day 30 post-intervention. The most commonly reported outcomes included infection rates (19 studies, 100%), inflammatory markers (15 studies, 78.9%), endotoxin levels (12 studies, 63.2%), and mortality (11 studies, 57.9%).
Risk of bias and quality assessment of individual studies
3.2
We assessed the methodological quality of all 19 included studies using the Cochrane Collaboration’s risk of bias tool (RoB 2.0). Two reviewers (Y P and H Y) independently evaluated each study across five domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, and selective reporting. Disagreements were resolved through discussion or third-party adjudication (Figure 2).
Risk of bias assessment of included studies. Methodological quality of the 19 included randomized controlled trials assessed using the revised Cochrane risk of bias tool (RoB 2.0). Judgements across five domains (randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, selection of the reported result) are presented for each study. The overall assessment indicated 5 studies (26.3%) with low risk, 10 studies (52.6%) with some concerns, and 4 studies (21.1%) with high risk of bias.
The assessment revealed variable methodological quality across the included studies. Only 4 studies (21.1%) reported adequate random sequence generation methods, such as computer-generated randomization or random number tables. The majority of studies (11 studies, 57.9%) mentioned randomization but did not specify the method, leading to an unclear risk of selection bias. Allocation concealment was properly described in only 3 studies (15.8%), while 14 studies (73.7%) had unclear concealment methods, and 2 studies (10.5%) exhibited high risk due to inadequate concealment procedures.
Blinding of participants and personnel presented mixed results. Six studies (31.6%) implemented double-blinding with placebo controls, resulting in low risk of performance bias. However, 9 studies (47.4%) had unclear blinding procedures, and 4 studies (21.1%) were open-label designs with high risk of bias. Blinding of outcome assessment was adequately described in 7 studies (36.8%), while the remaining studies had unclear reporting in this domain.
Incomplete outcome data were generally well-handled, with 15 studies (78.9%) demonstrating low risk due to balanced dropout rates and intention-to-treat analysis. Three studies (15.8%) had unclear risk due to insufficient reporting of attrition, and one study (5.3%) showed high risk with significant differential dropout between groups. Selective reporting bias was low in 13 studies (68.4%), as they reported all pre-specified outcomes, while 6 studies (31.6%) had unclear risk due to unavailable study protocols.
Other potential sources of bias included industry funding in 2 studies (10.5%), which was appropriately disclosed, and baseline imbalance in 3 studies (15.8%). Overall, the risk of bias assessment indicated that 5 studies (26.3%) had low risk, 10 studies (52.6%) had moderate risk, and 4 studies (21.1%) had high risk of bias. The relatively high proportion of studies with moderate to high risk emphasizes the need for cautious interpretation of the findings.
The quality assessment also considered study precision and applicability. Sample size calculations were reported in only 6 studies (31.6%), and most studies had limited sample sizes, reducing the precision of effect estimates. Clinical applicability was generally good, as the populations, interventions, and outcomes reflected real-world critical care scenarios. However, the heterogeneity in intervention protocols and outcome measurements across studies may limit the generalizability of pooled results.
Meta-analysis findings
4
Wound infection rate
4.1
Data on wound infection rates were reported in five RCTs (29, 34, 36, 39, 45). There were no significant differences between studies in terms of patient age (MD = 2.3 years, p = 0.12), sex distribution (58.7% vs. 57.4% male), or APACHE II scores (MD = 1.8 points, p = 0.31). Meta-analysis revealed that probiotic intervention significantly reduced the risk of wound infection, with a pooled risk ratio (RR) of 0.518 [95% confidence interval (CI): 0.379–0.708, p < 0.001] and moderate heterogeneity (I^2^ = 34.3%) (Figure 3). Subgroup analysis indicated that burn wound patients benefited more substantially (RR = 0.430, 95% CI: 0.247–0.749), while surgical wound patients also showed consistent benefit (RR = 0.542, 95% CI: 0.361–0.814) (Supplementary Figure S1). Visual inspection of the funnel plot (Supplementary Figure S2) demonstrated symmetrical distribution of effect sizes around the pooled estimate, suggesting a low risk of publication bias. In accordance with our pre-specified analysis plan, Egger’s regression test was not performed for this outcome due to the limited number of studies (n = 5). Sensitivity analysis (leave-one-out method) confirmed the robustness of the result, with RR values ranging from 0.43 to 0.55.
Forest plot for the effect of probiotics on wound infection rate. Random-effects meta-analysis of 5 RCTs reporting specific wound infection outcomes. Probiotic supplementation significantly reduced the risk of wound infection compared to control (pooled RR = 0.518, 95% CI: 0.379–0.708; p < 0.001). Heterogeneity was moderate (I2 = 34.3%). The size of the square represents the study weight, and the diamond represents the overall pooled estimate. CI, confidence interval; RR, risk ratio.
A separate meta-analysis on overall infection rates (any site), which included 17 of the 19 RCTs, yielded a consistent result (RR = 0.65, 95% CI: 0.52–0.81) (Supplementary Figure S3). Funnel plot inspection (Supplementary Figure S4) and Egger’s regression test (p = 0.18) showed no evidence of significant publication bias. Sensitivity analysis (Supplementary Figure S5) confirmed robustness.
Wound healing time
4.2
Wound healing time was reported in three RCTs (36, 44, 45), with a total sample size of 263 patients. Pooled analysis showed that probiotic intervention did not significantly shorten wound healing time, with a mean difference (MD) of −5.60 days (95% CI, −23.09 to 11.88, p = 0.302) and low heterogeneity (I^2^ = 0.9%) (Figure 4). Given the very limited number of studies (n = 3), no formal assessment of publication bias was performed, as pre-specified in the statistical analysis plan. Sensitivity analysis using the leave-one-out approach confirmed the robustness of the null finding. Sequential exclusion of each study did not substantially alter the pooled estimate, with the mean difference remaining non-significant in all analyses (range: MD −7.23 to −4.21 days, all p > 0.05).
Forest plot for the effect of probiotics on wound healing time. Random-effects meta-analysis of 3 RCTs reporting wound healing time. Probiotic supplementation did not significantly shorten the healing time compared to control (pooled MD = −5.60 days, 95% CI: −23.09 to 11.88; p = 0.302). Heterogeneity was negligible (I2 = 0.9%). MD, mean difference.
Hospital length of stay
4.3
Hospital length of stay was reported in four RCTs (29, 34, 36, 39), with a total sample size of 489 patients. Significant heterogeneity existed between studies in antibiotic usage protocols (p = 0.03). Meta-analysis showed that patients in the probiotic group had a mean reduction in hospital length of stay of 5.24 days (MD = −5.24 days, 95% CI: −8.73 to −1.75, p = 0.003), with moderate heterogeneity (I^2^ = 58.7%) (Figure 5). The funnel plot demonstrated symmetrical distribution of effect sizes around the pooled estimate (Supplementary Figure S6). As pre-specified, Egger’s test was not applied for outcomes with fewer than 10 studies. Meta-regression indicated that daily dressing change frequency explained 31.6% of the heterogeneity (β = −0.32, p = 0.04). Sensitivity analysis showed a stable direction of effect (MD range: −4.9 to −5.6 days).
Forest plot for the effect of probiotics on hospital length of stay. Random-effects meta-analysis of 4 RCTs. Probiotic supplementation significantly reduced the hospital length of stay compared to control (pooled MD = −5.24 days, 95% CI: −8.73 to −1.75; p = 0.003). Heterogeneity was moderate (I2 = 58.7%). MD, mean difference.
Anastomotic leak rate
4.4
Anastomotic leak data were extractable from two RCTs (34, 41), with a total sample size of 359 patients. Pooled analysis using a random-effects model indicated that probiotic intervention had no significant effect on the incidence of anastomotic leak (RR = 0.57, 95% CI: 0.05–6.27, p = 0.64), with low inter-study heterogeneity (I^2^ = 0.8%) (Figure 6). The analysis was limited to two studies, as the studies by Rayes et al. (39) and Liu et al. (36) did not explicitly report anastomotic leak outcomes. Given the very limited number of studies, assessment of publication bias was not performed.
Forest plot for the effect of probiotics on anastomotic leak rate. Random-effects meta-analysis of 2 RCTs. Probiotic supplementation had no significant effect on the incidence of anastomotic leak compared to control (pooled RR = 0.57, 95% CI: 0.05–6.27; p = 0.64). Heterogeneity was low (I2 = 0.8%). RR, risk ratio.
Inflammatory marker (CRP) levels
4.5
C-reactive protein (CRP) levels were reported in two RCTs (29, 36), with a total sample size of 325 patients. Significant heterogeneity existed between studies in the timing of CRP measurement (p < 0.001). Pooled analysis using standardized mean difference (SMD) showed a significant reduction in CRP levels in the probiotic group, with an SMD of −0.732 (95% CI, −1.148 to −0.316, p < 0.001) and moderate heterogeneity (I^2^ = 41.2%) (Figure 7). No assessment of publication bias was conducted for this outcome due to the small number of contributing studies.
Forest plot for the effect of probiotics on CRP levels. Random-effects meta-analysis of 2 RCTs reporting C-reactive protein (CRP) levels. Probiotic supplementation significantly reduced CRP levels compared to control (pooled SMD = −0.732, 95% CI: −1.148 to −0.316; p < 0.001). Heterogeneity was moderate (I2 = 41.2%). SMD, standardized mean difference.
Duration of antibiotic use
4.6
A meta-analysis was performed on 10 randomized controlled trials to assess the efficacy of probiotics versus a control in reducing the duration of antibiotic use. The pooled analysis of these studies revealed a statistically significant effect in favor of probiotic supplementation. The overall effect size, measured as the Standardized Mean Difference (SMD), was −0.18 [95% Confidence Interval (CI): −0.25 to −0.11; p < 0.001] (Figure 8). This result indicates a consistent reduction in antibiotic use duration within the probiotic groups across the included studies. Quantification of heterogeneity among the 10 studies yielded an I^2^statistic of 45%, indicating a moderate level of inconsistency in the effect sizes across the individual RCTs. The funnel plot (Supplementary Figure S8) displays a generally symmetrical distribution of the study estimates around the pooled effect size, and Egger’s regression test (p = 0.18) did not indicate significant publication bias.
Forest plot for the effect of probiotics on duration of antibiotic use. Random-effects meta-analysis of 10 RCTs. Probiotic supplementation significantly reduced the duration of antibiotic use compared to control (pooled SMD = −0.18, 95% CI: −0.25 to −0.11; p < 0.001). Heterogeneity was moderate (I2 = 45%). SMD, standardized mean difference.
Mortality
4.7
Complete data on mortality were accessible in 17 RCTs. The aggregated data from these RCTs showed a non-statistically significant reduction in mortality of the experimental groups relative to the control (RR = 0.75; 95% CI: 0.56–1.01; p = 0.06, I^2^ = 38.5%) (Figure 9). Subgroup analysis by patient severity (APACHE II score >20 vs. ≤20) revealed that probiotics were associated with a significant mortality reduction in severely ill patients (RR = 0.62, 95% CI: 0.43–0.89; p = 0.01) (Supplementary Figure S9), but no significant benefit in moderately ill patients (RR = 0.88, 95% CI: 0.59–1.32; p = 0.55). The constructed funnel plot (Supplementary Figure S10) illustrated no evidence of publication bias, which was confirmed by Egger’s regression test (p = 0.15).
Forest plot for the effect of probiotics on all-cause mortality. Random-effects meta-analysis of 17 RCTs. Probiotic supplementation showed a non-statistically significant trend towards reducing mortality compared to control (pooled RR = 0.75, 95% CI: 0.56–1.01; p = 0.06). Heterogeneity was moderate (I2 = 38.5%). RR, risk ratio.
ICU length of stay
4.8
The meta-analysis of four RCTs (29, 34, 36, 39) that provided detailed ICU length of stay data was performed using a random-effects model. The analysis demonstrated a reduction in ICU length of stay favoring the probiotics group, with a pooled mean difference (MD) of −5.94 days. However, this result did not reach statistical significance (95% CI: −13.02 to 1.14; p = 0.076). The analysis indicated substantial heterogeneity among the studies (I^2^ = 69.7%) (Figure 10). For this subset of 4 studies, the funnel plot (Supplementary Figure S11) was visually inspected and showed no clear asymmetry. Formal testing with Egger’s regression was not performed, consistent with our analytical plan. For the broader analysis of ICU length of stay (8 studies), the funnel plot (Supplementary Figure S11) and the leave-one-out sensitivity analysis (Supplementary Figure S12) indicated no evidence of publication bias. Egger’s test was not applied to this broader analysis as it included fewer than 10 studies.
Forest plot for the effect of probiotics on ICU length of stay (subset analysis). Random-effects meta-analysis of a subset of 4 RCTs providing detailed ICU length of stay data. Probiotic supplementation showed a non-significant reduction compared to control (pooled MD = −5.94 days, 95% CI: −13.02 to 1.14; p = 0.076). Heterogeneity was substantial (I2 = 69.7%). MD, mean difference.
Duration of mechanical ventilation
4.9
A meta-analysis of 8 RCTs revealed that the duration of mechanical ventilation was significantly shorter in the probiotic group than in the control group (SMD = −0.90; 95% CI: −1.20 to −0.60; p < 0.001), with low heterogeneity (I^2^ = 0%). Subgroup analysis by intervention type showed that synbiotics (SMD = −0.31, 95% CI: −0.52 to −0.10; p = 0.004) conferred greater benefits than single-strain probiotics (SMD = −0.09, 95% CI: −0.16 to −0.02; p = 0.01) (Figure 11). Visual inspection of the funnel plot (Supplementary Figure S13) indicated the absence of discernible publication bias. Egger’s regression test was not conducted as the number of studies was below our pre-specified threshold of 10.
Forest plot for the effect of probiotics on duration of mechanical ventilation. Random-effects meta-analysis of 8 RCTs. Probiotic supplementation significantly reduced the duration of mechanical ventilation compared to control (pooled SMD = −0.90, 95% CI: −1.20 to −0.60; p < 0.001). Heterogeneity was low (I2 = 0%). SMD, standardized mean difference.
Intestinal barrier function improvement rate
4.10
A supplementary meta-analysis was conducted on 3 RCTs (32, 35, 36) reporting intestinal barrier function improvement, defined by reduced intestinal permeability (lactulose/mannitol ratio or zonulin levels) or decreased bacterial translocation. The pooled results showed that probiotic interventions significantly improved intestinal barrier function compared to controls, with a RR of 1.63 (95% CI: 1.28–2.08; p < 0.001, I^2^ = 22.8%) (Figure 12). Assessment of publication bias was not performed for this outcome due to the limited number of included studies.
Forest plot for the effect of probiotics on intestinal barrier function improvement rate. Random-effects meta-analysis of 3 RCTs. Probiotic supplementation significantly improved intestinal barrier function compared to control (pooled RR = 1.54, 95% CI: 1.27–1.86; p < 0.001). Heterogeneity was low (I2 = 0%). RR, risk ratio.
Subgroup analysis by patient population
4.11
To investigate the source of heterogeneity in the above results, we performed a subgroup analysis according to patient population. The subgroup analysis revealed consistent treatment effects across different patient groups: surgical patients (RR = 0.66, 95% CI: 0.52–0.84), burn patients (RR = 0.60, 95% CI: 0.44–0.82), trauma patients (RR = 0.68, 95% CI: 0.52–0.89), and transplant patients (RR = 0.72, 95% CI: 0.52–1.00). Subgroup analysis of intestinal barrier function improvement stratified by patient population showed there was not significantly influenced (Supplementary Figure S14A), and the test for subgroup differences was not statistically significant (p = 0.12), indicating that probiotic efficacy was not significantly influenced by patient population type (Supplementary Figure S14B). Regarding the specific inquiry on adult versus pediatric burn subgroups: among the included RCTs, only one study (47) exclusively enrolled pediatric burn patients, while the remaining burn studies focused on adults. The limited number of pediatric-specific RCTs precluded a formal quantitative meta-analysis comparing these age groups. However, qualitative observation suggests that the direction of effect (reduced infection, improved gut barrier) appears consistent across the single pediatric study and the pooled adult burn studies, though this requires confirmation in future research with dedicated pediatric RCTs (47).
Subgroup analysis by intervention type
4.12
Subgroup analysis by intervention type showed that probiotics (RR = 0.66, 95% CI: 0.52–0.84) and synbiotics (RR = 0.61, 95% CI: 0.45–0.83) demonstrated significant benefits, while prebiotics (RR = 0.71, 95% CI: 0.50–1.00) showed a non-significant trend toward benefit. Among probiotic formulations, multi-strain probiotics (RR = 0.59, 95% CI: 0.41–0.85) tended to be more effective than single-strain probiotics (RR = 0.68, 95% CI: 0.53–0.88), though the difference was not statistically significant (p = 0.32) (Supplementary Figure S14C). The distribution of studies was weighted toward probiotic interventions (n = 10 studies). The funnel plot indicated no significant publication bias across intervention types.
Certainty of evidence
4.13
The overall certainty of the evidence for each primary and secondary outcome was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework. All outcomes started as high-certainty evidence due to their derivation from randomized controlled trials but were subsequently downgraded based on assessments across five domains: risk of bias, inconsistency (heterogeneity), indirectness, imprecision, and publication bias.
Our assessments yielded the following key judgements:
Wound infection rate (primary outcome): the evidence was rated as moderate certainty. It was downgraded by one level due to risk of bias, as a substantial proportion of contributing studies raised some concerns or had high risk. The low-to-moderate heterogeneity (I^2^ = 34.3%) and precise effect estimate with a confidence interval excluding the null effect did not warrant further downgrading.
Overall infection rate, hospital length of stay, antibiotic use duration: these outcomes were also rated as moderate certainty. Similar to the primary outcome, they were downgraded by one level primarily for risk of bias and, in some cases (e.g., hospital stay), for moderate unexplained heterogeneity.
ICU length of stay: the evidence for this outcome was rated as low certainty. It was downgraded by two levels: one for risk of bias and one for imprecision. The latter is due to the wide confidence interval in the subset analysis (MD = −5.94 days, 95% CI: −13.02 to 1.14; p = 0.076), which includes both a clinically meaningful reduction and no effect.
All-cause mortality: the evidence was rated as low certainty. It was downgraded by one level for imprecision (the 95% confidence interval includes both a potential reduction and no effect: RR = 0.75, 95% CI: 0.56–1.01) and one level for inconsistency, as the effect appeared to differ substantially between subgroups based on illness severity.
Wound healing time: the evidence for this outcome was rated as very low certainty. It was downgraded by three levels: one for risk of bias, one for imprecision (extremely wide confidence interval: −23.09 to 11.88 days, based on only 3 studies), and one for indirectness, due to variability in how healing was measured and defined across studies.
CRP reduction, intestinal barrier function: these biomarker outcomes were rated as low to moderate certainty, with downgrades typically for imprecision (limited number of studies) and, for CRP, moderate heterogeneity. These GRADE judgements inform the strength of the conclusions drawn in the Discussion and Conclusion sections.
Sensitivity analysis findings
4.14
Leave-one-out sensitivity analysis confirmed the robustness of the primary findings for infection rates, ICU length of stay, and intestinal barrier function improvement. The pooled estimate remained statistically significant regardless of which individual study was omitted from the analysis. These analyses support the robustness and consistency of the observed treatment effects across different methodological approaches. Sensitivity analysis for heterogeneity showed that excluding studies with high risk of bias (n = 4) reduced heterogeneity for ICU length of stay (I^2^ = 42.1% from 67.3%) and infection rates (I^2^ = 29.5% from 38.6%), while the pooled effect size remained significant, indicating that methodological quality had a limited impact on the overall findings.
Discussion
5
Summary of main findings
5.1
This systematic review and meta-analysis of 19 RCTs synthesizes focused evidence on the impact of probiotic supplementation in critically ill patients, with a particular emphasis on wound-related outcomes. The primary analysis demonstrates a statistically significant and clinically meaningful reduction in wound infection risk by approximately 48% (RR = 0.518, 95% CI: 0.379–0.708). This benefit appears most pronounced in burn patients. Furthermore, probiotic administration was associated with a significant reduction in hospital length of stay (mean reduction of 5.24 days) and duration of antibiotic use. Supportive findings include a significant attenuation of systemic inflammation, as evidenced by reduced CRP levels, and an improvement in intestinal barrier function. Contrary to our initial hypothesis, the pooled analysis did not demonstrate a statistically significant effect on wound healing time. While the overall effect on mortality was non-significant, a notable reduction was observed in a subgroup of severely ill patients (APACHE II > 20). The results for ICU length of stay were inconsistent, showing a significant reduction in a broader analysis but a non-significant trend in a more homogeneous subset of studies. It is important to explicitly state that current evidence does not support the use of probiotics specifically to shorten ICU length of stay, given the inconsistent and imprecise findings.
Comparison with existing literature and contextualization of findings
5.2
Our meta-analysis both corroborates and refines the existing body of evidence on probiotics in critical care. The finding of a substantial 48% relative reduction in wound infection risk powerfully consolidates previous systematic reviews that have reported benefits for overall infectious complications in surgical and ICU populations (12, 28). However, by isolating and quantitatively synthesizing data specifically for wound infections—a distinct and clinically pivotal endpoint—we provide a more precise and actionable estimate of efficacy for this complication. This specificity strengthens the rationale for incorporating probiotics into wound management protocols, moving beyond general infection prevention strategies. The significant reductions in hospital length of stay and duration of antibiotic use align robustly with previous meta-analyses, reinforcing the broader clinical and antimicrobial stewardship benefits of probiotic supplementation (28). The reduction in systemic inflammation, quantified here by a large effect size on CRP (SMD = −0.732), offers robust biomarker-level support for the long-postulated anti-inflammatory mechanism of action, a effect often discussed mechanistically but less consistently demonstrated in prior pooled clinical analyses (48, 49).
The non-significant finding regarding wound healing time, however, introduces a critical and nuanced perspective that challenges some optimistic interpretations in the literature: While preclinical models (50, 51) and some individual clinical trials (52, 53) have suggested accelerated healing (10, 15), our rigorous synthesis of available RCT data indicates that the current clinical evidence is insufficient to confirm this effect in the heterogeneous critically ill population. This discrepancy underscores a vital clinical distinction: effectively preventing a secondary complication (infection) that delays healing is not synonymous with directly accelerating the fundamental biological processes of tissue repair (proliferation, remodeling). Our analysis highlights this potential gap and suggests that the profound metabolic and physiological disturbances in critical illness may not be overridden by the systemic immunomodulatory effects of probiotics alone. This finding calls for a more cautious and specific framing of probiotic benefits in future guidelines, emphasizing infection prevention as the primary wound-related outcome rather than healing acceleration.
Furthermore, our subgroup and sensitivity analyses help contextualize the heterogeneity observed in earlier reviews. The pronounced benefit in burn patients, for instance, clarifies why some trials in mixed populations may have shown modest effects, while those targeting burns demonstrated dramatic results. The trend toward greater efficacy with multi-strain formulations and synbiotics aligns with emerging principles in microbiome therapeutics (54), suggesting that diversity and functional support (via prebiotics) may be key to resilience in the dysbiotic ICU environment.
Elaboration of biological plausibility and integrated mechanistic interpretations
5.3
The clinical benefits observed, particularly the robust prevention of wound infections, are underpinned by a converging multi-mechanistic model that aligns with the “gut-skin axis” hypothesis. The foundational mechanism appears to be the reinforcement of intestinal barrier integrity, as evidenced by our meta-analysis showing a significant improvement (RR = 1.63). Probiotics, particularly strains like Lactobacillus and Bifidobacterium, enhance the expression of tight junction proteins (e.g., ZO-1, occludin) (8), reducing intestinal permeability. This mitigates the translocation of pathogenic bacteria and their endotoxins (e.g., LPS) into the systemic circulation (55), a primary driver of the persistent, low-grade inflammatory state characteristic of critical illness.
The subsequent modulation of systemic and local immunity is a critical downstream effect. Reduced endotoxin translocation leads to decreased activation of toll-like receptor 4 (TLR4) signaling (56) and downstream nuclear factor kappa B (NF-κB) pathways (57), resulting in lower levels of pro-inflammatory cytokines such as TNF-α (58) and IL-6 (7, 59). Concurrently, certain probiotic strains can promote a regulatory immune phenotype, increasing anti-inflammatory mediators like IL-10. This shift from a pro-inflammatory to a more regulated immune milieu, reflected in our observed CRP reduction, is crucial for wound healing. Excessive inflammation is detrimental to both infection resistance (causing immune cell dysfunction) and tissue repair (causing collateral damage to forming granulation tissue) (60). By dampening this dysregulated inflammation, probiotics may help restore the balance necessary for effective phagocytic clearance of pathogens at the wound site. In the specific context of burn wounds, which are characterized by a unique pathophysiology including massive fluid shifts, hypermetabolism, and a high propensity for infection, this immunomodulation may be particularly relevant (28). Burn wounds often experience a shift in microbial ecology over time, with Gram-negative bacteria like Pseudomonas aeruginosa (28) becoming predominant in later stages. Probiotic intervention, by systemically reducing endotoxin burden and potentially modulating the local wound microenvironment through immune cells, may help counteract this ecological shift and mitigate Gram-negative infections. Furthermore, the potential interaction between systemic probiotics and topical antimicrobials commonly used in burns (e.g., silver sulfadiazine) (19, 24, 28) warrants consideration. While direct evidence is lacking, a hypothetical synergy is plausible: probiotics may reduce systemic inflammatory drivers of immunosuppression and bacterial translocation, while topical agents control local bioburden (28). Conversely, antagonism is possible if certain probiotic strains are sensitive to concurrently administered systemic antibiotics. This represents an important area for future mechanistic and clinical research.
A third, more direct mechanism may involve microbial competition and biofilm disruption. Probiotics can competitively exclude pathogenic bacteria from ecological niches, both in the gut and potentially on the skin or wound surface, through resource competition and the production of bacteriocins and other antimicrobial substances (9). This direct antagonistic activity could contribute to reducing the bioburden and biofilm formation in wounds, particularly in colonized burn wounds or surgical sites. The dissociation between infection prevention and healing time in our results is mechanistically insightful. It suggests that while the aforementioned mechanisms (barrier protection, immunomodulation, competition) are sufficient to significantly reduce the incidence of a secondary complication (infection), they may not be potent or targeted enough to directly stimulate the primary cellular processes of healing (61). The proliferative and remodeling phases of wound repair are governed by complex, growth factor-driven signaling (e.g., VEGF, TGF-β) (62), fibroblast and keratinocyte proliferation, angiogenesis, and collagen synthesis (63). The severe catabolic state, endocrine dysfunction, and local tissue hypoxia in critically ill patients present profound barriers to these processes. Our findings imply that the systemic, immune-focused action of enteral probiotics, while beneficial for host defense, does not sufficiently overcome these central impediments to tissue regeneration. This underscores the need for combined therapeutic strategies that address both the systemic inflammatory environment and the local wound microenvironment directly.
Clinical implications, limitations, and avenues for future investigation
5.4
The findings of this meta-analysis yield significant and differentiated guidance for the clinical application of probiotics in wound management among critically ill populations. Supported by evidence of moderate certainty, specific probiotic formulations can be considered a valuable adjunctive strategy for the prevention of wound infections, particularly in burn and surgical patients. Implementation should be integrated within standardized wound care and infection prevention bundles, with the primary objective of mitigating complication risk rather than directly accelerating wound closure based on current evidence. In practice, prioritization should be given to products with documented efficacy in comparable clinical studies, initiating intervention early (e.g., perioperatively) where feasible and maintaining an adequate treatment duration. For clinicians considering probiotic use, several practical aspects merit attention. First, the question of feasibility in severely burned patients expected to have intestinal edema or ileus is crucial. The included studies in burn populations generally initiated enteral probiotic administration early (within 48–72 h) (28), suggesting that with careful monitoring and potentially using prokinetic agents, early enteral administration is feasible and was associated with positive outcomes in these trials. However, adherence to strict enteral feeding protocols and monitoring for intolerance is essential. Second, this meta-analysis encompasses a mixed ICU population. While the benefits appear consistent across subgroups, the representation of specific high-risk subpopulations such as patients with severe septic shock on high-dose vasopressors or those with profound immunosuppression (e.g., post-transplant, neutropenic) within the included trials is limited (10). Generalizing the safety and efficacy conclusions to these extreme cohorts requires caution. Third, from an implementation standpoint, reliable enteral delivery in patients with ileus, feed intolerance, or those requiring gastric residual volume monitoring poses real-world challenges. Protocols for administration, like continuous or bolus, and monitoring for intolerance need to be established. Fourth, while the overall safety profile was favorable, a direct acknowledgment of the debated risk of probiotic-associated bacteremia in vulnerable ICU patients with disrupted intestinal barriers is necessary for a comprehensive risk–benefit assessment. This risk, though reported as low in frequency, underscores the importance of strain selection (avoiding strains with high pathogenic potential) and prudent use, particularly in patients with central venous catheters and severe immunocompromise. Finally, how this intervention fits within existing, evidence-based ICU protocols in sepsis management, ventilator liberation, or glycemic control requires consideration. Potential synergistic or antagonistic interactions with other standard therapies, such as broad-spectrum antibiotics (which may kill the administered probiotics) or vasopressors (which may affect gut perfusion) (28), should be evaluated on a case-by-case basis and represent an area for further research.
Nevertheless, the conclusions of this synthesis must be interpreted within the context of several important and inter-related limitations that constrain the generalizability and clinical application of our findings, while also mapping essential domains for future inquiry. First, while the primary outcome of wound infection prevention shows robust and consistent effects, the evidence for other critical endpoints remains significantly underdeveloped or inconclusive. Most notably, the absence of a demonstrable effect on wound healing time is based on a critically sparse evidence base from only three trials, resulting in an imprecise estimate with very low certainty. This scarcity of data represents a fundamental gap, preventing any definitive conclusion and highlighting a disconnect between the well-established benefit in infection prevention and the ultimate goal of tissue repair (64, 65). The clinical relevance of this finding is paramount, as accelerated healing is a key patient-centered outcome. This gap necessitates future trials explicitly powered for this endpoint. We strongly endorse the call for prospective RCTs specifically in burn populations, with primary endpoints focused on objective and standardized wound healing assessment. For example, future trials should consider including “the time required to achieve 95% re-epithelialization assessed by digital planimetry” as a primary endpoint. This would be crucial for generating high-quality and comparable evidence in this field. Second, the pronounced and largely unexplained clinical and methodological heterogeneity across included trials presents a major barrier to formulating specific clinical recommendations. This heterogeneity manifests in several key dimensions (66, 67): (1) Intervention Diversity: There is extreme variability in the probiotic strains used (single vs. multi-strain), doses (ranging from 10^9^ to 10^11^ CFU/day), formulations (probiotic alone vs. synbiotic), and duration of administration (7 to 21 days). This “black box” of intervention precludes the identification of an optimal, reproducible regimen. (2) Population Diversity: The included studies encompass distinct pathophysiological states (e.g., elective surgery, major burns, trauma), each with unique immune and metabolic disturbances that may modulate the response to probiotics. While subgroup analyses were consistent, the power to detect true effect modifiers was limited. (3) Heterogeneity in Co-interventions and Standard Care: Differences in background protocols for antibiotic use, wound care, nutritional support, and sedation across ICUs and over time (studies span two decades) introduce significant noise and limit the comparability of studies. Third, there are inherent methodological constraints in the primary evidence. A proportion of included trials exhibited a moderate to high risk of bias, predominantly due to inadequate reporting of randomization and blinding procedures—a common challenge in nutritional intervention trials. Although sensitivity analyses suggested the robustness of the primary infection outcome, this limitation tempers the strength of the conclusions. Furthermore, the predominant focus on surrogate or composite outcomes in many trials, rather than patient-centric wound healing metrics, reflects a broader methodological shortcoming in the field. The lack of standardized, objective tools for measuring wound progression (e.g., validated digital planimetry) increases the risk of measurement bias and hinders meaningful data synthesis. Fourth, the reliability of findings for several critical outcomes is constrained by the limited number of contributing studies. As noted in the results, meta-analyses for wound healing time (n = 3 studies), anastomotic leak (n = 2), CRP levels (n = 2), and ICU length of stay in the subset analysis (n = 4) were based on very few trials. While these analyses provide preliminary insights, the small study numbers increase the susceptibility to random error, limit the power to detect true effects, and reduce the generalizability of the findings. This is particularly relevant for the null result regarding wound healing time, where the very low certainty of evidence precludes definitive conclusions. Future research must prioritize these understudied endpoints with adequately powered trials. Fifth, the external validity and long-term implications of our findings are uncertain. The follow-up periods in most trials were restricted to the acute hospitalization phase, leaving the impact on long-term outcomes—such as scar quality, functional recovery, wound recurrence, and health-related quality of life—completely unexplored. Additionally, the efficacy and safety of probiotics in some of the most vulnerable and complex ICU sub-populations (e.g., patients with severe septic shock on multiple broad-spectrum antibiotics, those with profound immunosuppression, or patients with open abdominal wounds) remain largely unstudied, limiting generalizability to these high-risk groups. The observed mortality benefit in the high-severity (APACHE II > 20) subgroup is intriguing and could suggest a modulatory effect on the state of immunoparalysis often seen in the most critically ill, or simply reflect a greater absolute risk reduction in a population with higher baseline mortality. Disentangling this requires future studies with detailed immune phenotyping.
Consequently, the pathway for future investigation must advance in a more standardized, mechanistic, and patient-centered direction. Priority should be given to large, pragmatic RCTs that are adequately powered for both infection prevention and objectively measured, patient-important wound healing outcomes, conducted in well-defined homogeneous populations (68). There is an urgent need for consensus on core outcome sets and intervention protocols to reduce heterogeneity. Mechanistically, future trials should integrate deep phenotyping (serial biomarkers of intestinal permeability, systemic/ local inflammation, wound microbiome) to elucidate responder profiles and the biology behind the infection-healing dissociation (69, 70). Finally, research should explore novel strategies like topical applications and assess long-term functional outcomes to fully define the therapeutic niche of probiotics in the complex pathophysiology of critical illness and wound repair.
Conclusion
6
This systematic review provides moderate-certainty evidence that probiotic supplementation is associated with a significant reduction in the risk of wound infection among critically ill patients, with a pronounced benefit observed in burn populations. It is also associated with a shorter hospital length of stay. However, based on the limited available data, no significant effect on accelerating wound healing time was demonstrated. The observed clinical benefits are consistent with proposed mechanisms involving gut barrier stabilization and systemic immunomodulation. Given the generally favorable safety profile, specific probiotic formulations may be considered a useful adjunct to standard infection prevention and wound care protocols in the intensive care unit, primarily aiming to mitigate infectious complications. Future research should prioritize the standardization of probiotic interventions, employ validated and sensitive metrics to assess wound healing progression, and confirm these findings in well-defined patient cohorts.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mohamed Rohani M Fisal AA. The dental management of patients with common hematological disorders and bleeding tendency. Spec Care Dentist. (2025) 45:e 70090. doi: 10.1111/scd.70090, 40843974 · doi ↗ · pubmed ↗
- 2Novoa J Hardy G Aramendi I Manzanares W. Intravenous vitamin C in critically ill adult patients with burns: an integrative review. Nutrition. (2025) 134:112728. doi: 10.1016/j.nut.2025.112728, 40081106 · doi ↗ · pubmed ↗
- 3Zajac KK Schubauer K Simman R. The unavoidable pressure injury/ulcer: a review of skin failure in critically ill patients. J Wound Care. (2024) 33:S 18–22. doi: 10.12968/jowc.2024.0079, 39283887 · doi ↗ · pubmed ↗
- 4Lou J Cui S Li J Jin G Fan Y Huang N. Causal relationship between the gut microbiome and basal cell carcinoma, melanoma skin cancer, ease of skin tanning: evidence from three two-sample mendelian randomisation studies. Front Immunol. (2024) 15:1279680. doi: 10.3389/fimmu.2024.1279680, 38304424 PMC 10830803 · doi ↗ · pubmed ↗
- 5Lou J Xiang Z Zhu X Li J Jin G Cui S . Gut microbiota constituents may affect hypertrophic scarring risk through interaction with specific immune cells in a two-step, two-sample mendelian randomization study. Sci Rep. (2025) 15:20656. doi: 10.1038/s 41598-025-07455-y, 40596527 PMC 12216485 · doi ↗ · pubmed ↗
- 6Pol IV Rees MV Gool GV Stalpers D Schoonhoven L Noordzij P . Cannulation-related wound complications after extra corporeal life support: a retrospective cohort study in a Dutch intensive care unit. P Lo S One. (2025) 20:e 0337952. doi: 10.1371/journal.pone.0337952, 41428647 PMC 12721521 · doi ↗ · pubmed ↗
- 7Lou J Xiang Z Zhu X Fan Y Li J Jin G . A two-step, two-sample Mendelian randomization analysis investigating the interplay between gut microbiota, immune cells, and melanoma skin cancer. Medicine. (2024) 103:e 40432. doi: 10.1097/MD.0000000000040432, 39533622 PMC 11557063 · doi ↗ · pubmed ↗
- 8Tranchida N Inferrera F Siracusa R Impellizzeri D D'Amico R Di Paola R . Nutritional modulation of the endogenous antioxidant system in the brain-gut axis following traumatic brain injury. Nutrients. (2025) 17:3404. doi: 10.3390/nu 17213404, 41228477 PMC 12609911 · doi ↗ · pubmed ↗