Born with two faces: sequential DLBCL, NOS and TFHL-AI with TET2 mutation – a case report
Qing Li, Shishuo Dai, Chenlu Yang, Weiping Liu, Yu Wu

TL;DR
A 74-year-old man developed two lymphomas in sequence, both sharing a TET2 mutation, highlighting challenges in diagnosis and treatment.
Contribution
This case report identifies shared TET2 mutations in sequential DLBCL and TFHL-AI, suggesting a common precursor or clonal evolution.
Findings
NGS revealed shared TET2 mutations in both DLBCL, NOS and TFHL-AI biopsies.
Combination therapy with chidamide and COEP achieved partial remission in TFHL-AI.
The patient's overall survival was 35 months, with disease progression after partial remission.
Abstract
Diffuse large B-cell lymphoma, not otherwise specified (DLBCL, NOS) and nodal T follicular helper cell lymphoma, angioimmunoblastic type (TFHL-AI) share significant histopathological and pathogenetic similarities. However, the mechanisms underlying these overlaps remain insufficiently explored in the literature. We report the case of a 74-year-old man who initially presented with progressive sore throat and was diagnosed with DLBCL, NOS based on a tonsillar biopsy. He achieved complete remission following six cycles of R-CHOP chemotherapy (rituximab, cyclophosphamide, vindesine, liposomal doxorubicin, and dexamethasone). However, the patient was lost to follow-up. About two years later, he re-presented with generalized pruritus and lymphadenopathy. A cervical lymph node biopsy confirmed TFHL-AI. He received four cycles of the histone deacetylase inhibitor (HDACi) chidamide combined with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
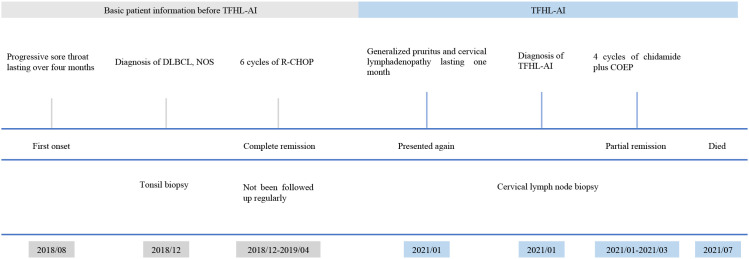 Figure 1
Figure 1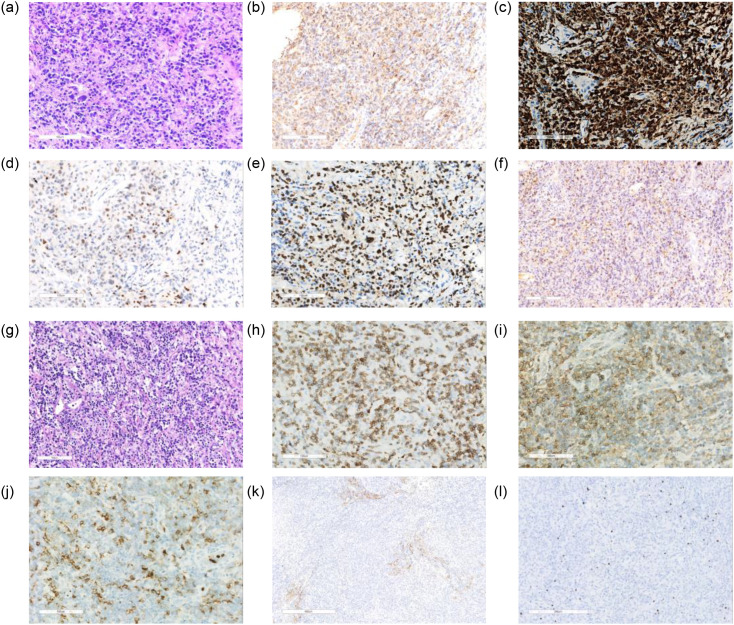 Figure 2
Figure 2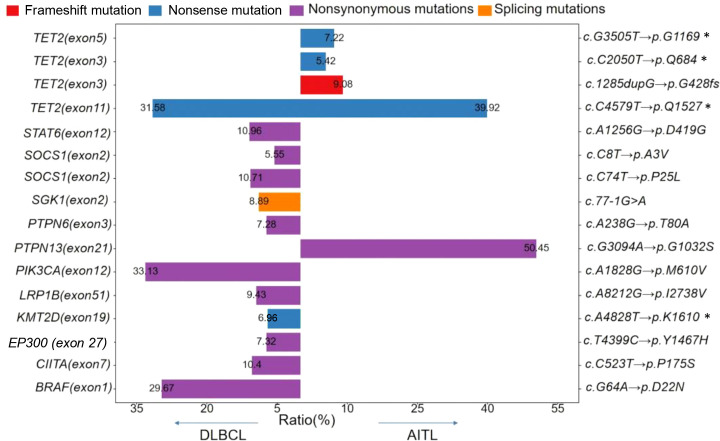 Figure 3
Figure 3| Age | Gender | Disease 1& treatment | Disease 2 & treatment | Clinical outcomes | References |
|---|---|---|---|---|---|
| 47 | M | TFHL-AI, CHOP | EBV+DLBCL, NOS, R-GDP | remission | ( |
| 78 | M | TFHL-AI, CHOP | EBV+DLBCL, NOS, lenalidomide & chidamide | dead | ( |
| 56 | M | TFHL-AI, CHOP | EBV+DLBCL, NOS, PD-1 inhibitor & GDP regimen | PR | ( |
| 65 | M | TFHL-AI, CHOP | DLBCL, NOS, CHOP-R | PR | ( |
| 68 | M | TFHL-AI, CHOP | EBV DLBCL, NOS, COP-R | remission | ( |
| 36 | F | TFHL-AI, FED & AHSCT | DLBCL, NOS, CHOP-R & ASCT | CR | ( |
| 68 | F | TFHL-AI, CVP | EBV+ DLBCL, NOS, ICE | dead | ( |
| 64 | M | TFHL-AI, IHOP | DLBCL, NOS, CHOP-R | PR | ( |
| 83 | M | EBV+DLBCL, NOS, R‐miniCHOP | TFHL-AI, chidamide and prednisolon | OS 15 months | ( |
| 73 | M | DLBCL, NOS, R-CHPVD | TFHL-AI, GLA | OS 8 months | ( |
| 72 | F | DLBCL, NOS, BR | TFHL-AI, no treat | NA | ( |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLymphoma Diagnosis and Treatment · Chronic Lymphocytic Leukemia Research · CNS Lymphoma Diagnosis and Treatment
Introduction
Diffuse large B-cell lymphoma, not otherwise specified (DLBCL, NOS) is a lymphoid malignancy in adults characterized by significant clinical and genetic heterogeneity (1). Nodal T follicular helper cell lymphoma, angioimmunoblastic type (TFHL-AI), a subtype of mature T-cell lymphoma, is associated with poor prognosis. Key mutations frequently observed in TFHL-AI include RHOA, TET2, DNMT3A, and IDH2 (2). Although cases of DLBCL, NOS developing after TFHL-AI, and vice versa, have been reported (3, 4), this study performed deep sequencing of biopsy tissue samples from two disease states to explore the potential links between DLBCL, NOS and TFHL-AI.
Case description
In August 2018, a 74-year-old man developed a sore throat that progressively worsened. However, he did not seek medical attention at Sichuan Cancer Hospital until December 2018. Prior to this, his sore throat persisted despite symptomatic treatment at a community hospital. The patient denied fever, night sweats, or weight loss, and had no significant medical history or family history of genetic diseases. Physical examination revealed bilateral tonsillar enlargement. In December 2018, a tonsil biopsy was performed and sent to the Department of Pathology at West China Hospital, Sichuan University, for further analysis.
The patient’s complete blood count, coagulation markers, liver and kidney function parameters, electrolytes, cardiac ultrasound, and electrocardiography were all within normal limits. Serum Epstein–Barr virus (EBV) DNA level was 6.29 × 10^1^ copies/mL. Positron emission tomography/computed tomography (PET/CT) revealed abnormal FDG uptake in multiple regions: bilateral oropharyngeal lateral walls, left posterior nasopharyngeal wall, bilateral submandibular glands, bilateral cervical paravascular regions, and left posterior cervical triangle. The Deauville score was 5. A diagnosis of DLBCL, NOS was established. From December 2018 to April 2019, the patient underwent six cycles of R-CHOP chemotherapy (rituximab, cyclophosphamide, vindesine, liposomal doxorubicin, and dexamethasone), achieving complete remission as confirmed by PET/CT (Deauville score 2). However, the patient was not followed up regularly thereafter.
In January 2021, about two years after being diagnosed with DLBCL, the patient developed systemic itching and cervical lymph node enlargement that lasted for one month. A physical examination revealed palpable cervical lymph nodes, and a biopsy confirmed TFHL-AI. PET/CT (positron emission tomography/computed tomography) showed hypermetabolic lymph nodes in the cervical, thoracic, and abdominal regions, while bone marrow biopsy was negative. Serum EBV DNA was elevated (1.25 × 10^4^ copies/mL). Given that the patient was diagnosed with post-DLBCL TFHL-AI, NOS and extensive disease, the patient received four courses of treatment with chidamide combined with COEP regimen (cyclophosphamide, vincristine, etoposide and prednisone) from January to March 2021. After 4 cycles, the patient achieved partial remission, with EBV DNA decreasing to 2.30 × 10² copies/mL. However, due to disease progression, the patient died in July 2021, 6 months after being diagnosed with TFHL-AI, with an overall survival of 35 months. A summary of the clinical course is shown in Figure 1.
A summary of the patient’s clinical course.
Tonsil biopsy revealed diffuse infiltration of large atypical lymphoid cells with focal necrosis (Figure 2a). Immunohistochemical staining showed that the atypical cells were positive for CD20 (Figure 2b), CD79a (Figure 2c), MUM-1 (Figure 2d), BCL-6 (data not shown), and Ki-67 (MIB-1, ~80%; Figure 2e). EBV infection was confirmed by EBER1/2 ISH (~20%; Figure 2f). The cells were negative for CD30, CD56, GB, TIA-1, and BCL-2. Although approximately 20% of EBER-positive tumor cells were detected, this case was not suitable for diagnosis as EBV-positive DLBCL, NOS according to the WHO-HAEM5 and ICC (2022) criteria (requiring >80% EBER-positive tumor cells) (5). Therefore, we diagnosed this case as DLBCL, NOS. Gene rearrangement analysis demonstrated monoclonal IGK and IGH rearrangements. According to the Hans algorithm, the DLBCL was classified as non-germinal center B-cell-like (non-GCB) subtype.
Histopathological, immunohistochemical, and ISH findings at DLBCL, NOS and TFHL-AI (a–f) (a) Hematoxylin and eosin (H&E) staining shows diffuse infiltration of large atypical lymphoid cells with vesicular nuclei, prominent nucleoli, and focal areas of necrosis (original magnification ×100); (b) Positive for CD20; (c) Positive for CD79a; (d) Positive for MUM-1; (e) Positive for Ki-67 (MIB-1, ~80%); f ISH for EBER1/2 reveals strong nuclear positivity in tumor cells, confirming EBV association (EBER-ISH, ×100, +, ~20%). All images were taken from the same tonsillar biopsy specimen. (g–l) Histopathological, immunohistochemical, and ISH findings at diagnosis of TFHL-AI (g) Hematoxylin and eosin staining showed partially naked follicles, expanded interfollicular zones, and prominent vascular proliferation; (h) Positive for CD3; (i) Positive for CD4; (j) Partial positivity for CD10; (k) CD21 highlights follicular dendritic cell meshworks; (l) EBER1/2 ISH showing nuclear positivity in scattered lymphocytes.
Cervical lymph node biopsy showed partially naked follicles, expanded interfollicular zones, and prominent vascular proliferation (Figure 2g). Tumor cells were positive for CD3, CD4, and partially for CD10 (Figures 2h–j). CD21 highlighted follicular dendritic cell meshworks (Figure 2k). EBER1/2 ISH revealed dispersed nuclear positivity, mainly in small lymphocytes with occasional large positive cells (Figure 2l). Ki-67 was ~60%. Tumor cells were negative for CD20, CXCL13, CD8, and CD15. They expressed PD-1, CD43, and CD30 (restricted to interfollicular large cells). PAX-5 showed weak focal staining (images not shown). Clonal TCRγ rearrangement was detected. No evidence of monoclonal IGH rearrangement was detected. No RHOA (G17V) or IDH2 (R172) mutations were found by Sanger sequencing.
At the time of DLBCL, NOS diagnosis, a TET2 nonsense mutation, c.C4579T (p.Q1527*), was identified by next-generation sequencing (NGS) in a tonsillar specimen. The same mutation was later detected in a lymph node specimen obtained at the time of TFHL-AI diagnosis. Notably, three additional TET2 variants with lower variant allele frequencies (VAFs) were identified exclusively in the TFHL-AI sample. Among the genes covered by both sequencing panels, TET2 was found to be mutated in both lymphoma types. The VAF of the shared TET2 mutation was 31.58% in the DLBCL, NOS sample and 39.92% in the TFHL-AI sample (Figure 3).
Mutational landscape of our reported case at the time of diagnosis of DLBCL, NOS and TFHL-AI The color represents the type of mutation, the left ordinate represents the mutation gene and mutation site, and the right vertical coordinate represents the change of nucleotides and amino acids. The abscissa represents the frequency of mutations. Genes covered by both sequencing panels include TET2, SOCS1, LRP1B, KMT2D, EP300, and CIITA. Mutations in genes not shared between panels—such as STAT6, SGK1, PTPN6, PIK3CA, BRAF (DLBCL only) and PTPN13 (AITL only)—are not directly comparable.
Discussion
While TET2 mutations are rare in DLBCL, NOS, they are more common in TFHL-AI. The role of TET2 mutations in the progression from DLBCL to TFHL-AI remains unclear and requires further research. TFHL-AI may develop from age-related clonal hematopoiesis (ACH), where TET2 mutations in ACH-derived germinal center B cells induce clonal evolution. These mutated B cells can function as microenvironmental cells, promoting TFHL-AI tumorigenesis (6). Studies indicate that 10%–60% of polyclonal B cells in TFHL-AI lymph nodes harbor the same TET2 mutation found in corresponding T-cell lymphoma clones (7). Furthermore, TET2-mutated premalignant cells can differentiate into both T-lineage tumor cells and B cells (7, 8). Determining the role of TET2 in epigenetic regulation is crucial for understanding the complex, multilineage tumorigenesis of TFHL-AI and offers new directions for research and therapeutic strategies (9).
In this context, our case likely reflects the divergent evolution of a mutated hematopoietic precursor into both B- and T-cell lymphoproliferative disorders. This paradigm has been previously described in TFHL-AI and associated myeloid neoplasms, and is further supported by recent studies such as Lewis et al. (10), which demonstrated a molecular and clonal link between TFHL-AI and B-cell proliferations. While DLBCL, NOS with secondary TFHL-AI is rarely reported, B-cell LPDs in the context of TFHL-AI are increasingly recognized, supporting a shared clonal origin and parallel evolution driven by TET2-mutated B cells within a TFH-rich microenvironment.
Although the initial biopsy did not meet the criteria for TFHL-AI, the presence of an underlying TFH-cell clone cannot be ruled out. Similar cases have been reported, including DLBCL later reclassified as TFHL-AI (11) and composite lymphomas with distinct DLBCL and TFHL-AI components (12). These highlight the risk of misdiagnosis when only one lineage is identified and emphasize the importance of evaluating TFH markers and T-cell clonality for accurate diagnosis and appropriate treatment. However, we acknowledge that T-cell clonality analysis was not performed on the initial biopsy, which represents a limitation in our evaluation.
PTCLs are aggressive malignancies with poor prognosis, low remission rates, and frequent relapses. Despite ongoing research, the outlook for TFHL-AI remains poor (13, 14). The 2022 NCCN guidelines recommends dose-adjusted EPOCH (etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin) as one of the first-line treatments, but its effectiveness is limited. Epigenetic drugs, which are currently investigated in clinical trials and recommended as second-line treatments (15), have shown potential for improving PTCLs outcomes (16). Chidamide, a selective HDAC inhibitor, has a unique mechanism of action. In a study of 383 patients with relapsed/refractory PTCLs, chidamide-based regimens showed encouraging results (17). Based on this, our patient was treated with chidamide plus COEP, which appeared to prolong survival. Notably, patients with TFHL-AI secondary to DLBCL typically survive only 2–3 months after TFHL-AI diagnosis (4, 18, 19).
We conducted a thorough literature review (Table 1) and found numerous reports of patients with TFHL-AI developing DLBCL, NOS after treatment (3, 20–26). In contrast, only three case reports describe the development of TFHL-AI following a prior diagnosis of DLBCL, and none included NGS analysis of tumor specimens before or after disease progression (4, 18, 19). These cases showed poor outcomes despite various treatments, highlighting the aggressive nature of such progression.
In summary, this case highlights a potential clonal relationship between DLBCL, NOS and TFHL-AI driven by shared TET2 mutations. The poor prognosis and diagnostic challenges highlight the need for thorough evaluation. Chidamide-based chemotherapy may offer a potential treatment option.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chapuy B Stewart C Dunford AJ Kim J Kamburov A Redd RA . Molecular subtypes of diffuse large B cell lymphoma are associated with distinct pathogenic mechanisms and outcomes. Nat Med. (2018) 24:679–90. doi: 10.1038/s 41591-018-0016-8, PMID: 29713087 PMC 6613387 · doi ↗ · pubmed ↗
- 2Zhang Y Lee D Brimer T Hussaini M Sokol L . Genomics of peripheral T-cell lymphoma and its implications for personalized medicine. Front Oncol. (2020) 10:898. doi: 10.3389/fonc.2020.00898, PMID: 32637355 PMC 7317006 · doi ↗ · pubmed ↗
- 3Poon F Ieremia E Collins G Matin RN . Epstein-barr virus-induced cutaneous diffuse large B-cell lymphoma in a patient with angioimmunoblastic T-cell lymphoma. Am J Dermatopathol. (2019) 41:927–30. doi: 10.1097/DAD.0000000000001371, PMID: 31599749 · doi ↗ · pubmed ↗
- 4Wang C Gong Y Jiang Q Liang X Chen R . Epstein-Barr Virus Positive Diffuse Large B-Cell Lymphoma Transformed into Angioimmunoblastic T-Cell Lymphoma after Treatment. Clin Case Rep. (2021) 9:e 04083. doi: 10.1002/ccr 3.4083, PMID: 34084501 PMC 8142414 · doi ↗ · pubmed ↗
- 5Falini B Martino G Lazzi S . A comparison of the international consensus and 5th world health organization classifications of mature B-cell lymphomas. Leukemia. (2023) 37:18–34. doi: 10.1038/s 41375-022-01764-1, PMID: 36460764 PMC 9883170 · doi ↗ · pubmed ↗
- 6Fujisawa M Nguyen TB Abe Y Suehara Y Fukumoto K Suma S . Clonal germinal center B cells function as a niche for T-cell lymphoma. Blood. (2022) 140:1937–50. doi: 10.1182/blood.2022015451, PMID: 35921527 PMC 10653021 · doi ↗ · pubmed ↗
- 7Schwartz FH Cai Q Fellmann E Hartmann S Mayranpaa MI Karjalainen-Lindsberg ML . Tet 2 mutations in B cells of patients affected by angioimmunoblastic T-cell lymphoma. J Pathol. (2017) 242:129–33. doi: 10.1002/path.4898, PMID: 28337768 · doi ↗ · pubmed ↗
- 8Nguyen TB Sakata-Yanagimoto M Asabe Y Matsubara D Kano J Yoshida K . Identification of cell-type-specific mutations in nodal T-cell lymphomas. Blood Cancer J. (2017) 7:e 516. doi: 10.1038/bcj.2016.122, PMID: 28157189 PMC 5301031 · doi ↗ · pubmed ↗