Postoperative Atrial Fibrillation Impacted by Completeness of Coronary Revascularization and Antiplatelet Regimen
Qin Jiang, Minghui Xie, Yalu Yu, Zhiai Tang, Jiaqi Xia, Shengshou Hu

TL;DR
This study shows that incomplete heart surgery and use of clopidogrel increase the risk of post-surgery heart rhythm problems.
Contribution
The study reveals that antiplatelet drug choice modifies the impact of revascularization completeness on postoperative atrial fibrillation.
Findings
Incomplete revascularization increased POAF risk by 70% compared to complete revascularization.
Clopidogrel users with incomplete revascularization had higher POAF rates than ticagrelor users.
Incomplete revascularization was linked to higher inflammation and longer hospital stays.
Abstract
Postoperative atrial fibrillation (POAF) is a common complication after off‐pump coronary artery bypass grafting (OPCABG) and contributes to increased morbidity and prolonged hospital stays. Both myocardial ischemia and systemic inflammation play a critical role in its pathogenesis, which is closely related to the intensity of coronary revascularization and antiplatelet treatment, respectively. This study investigated the impact of the interaction between completeness of coronary revascularization and antiplatelet regimen on POAF incidence. A total of 505 eligible patients, undergoing elective first‐time OPCABG surgery from May 2017 to May 2024, were reviewed and divided into the incomplete revascularization (IR) group (n = 143) and complete revascularization (CR) group (n = 362) according to the extent of coronary revascularization. The incidence of POAF within the first week…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
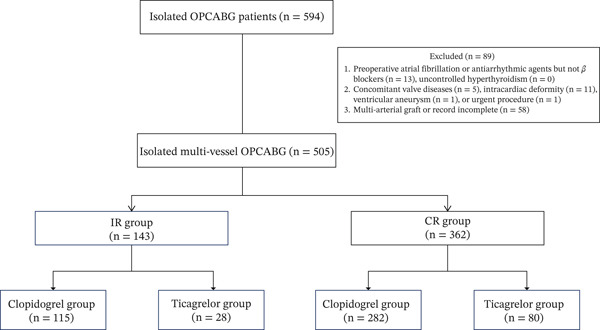 Figure 1
Figure 1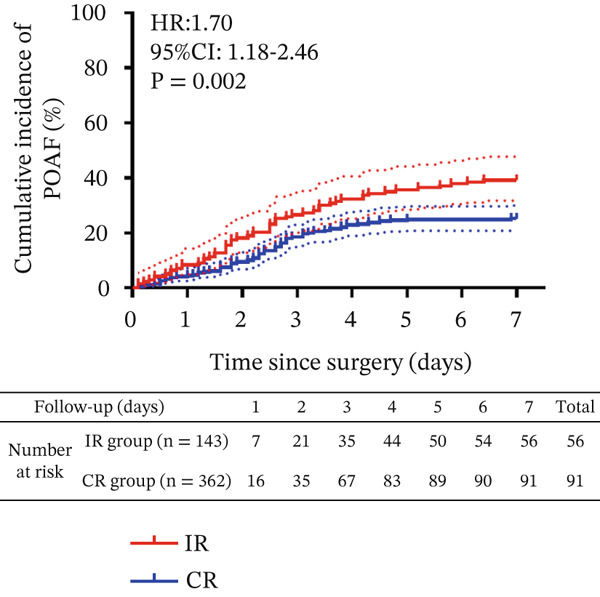 Figure 2
Figure 2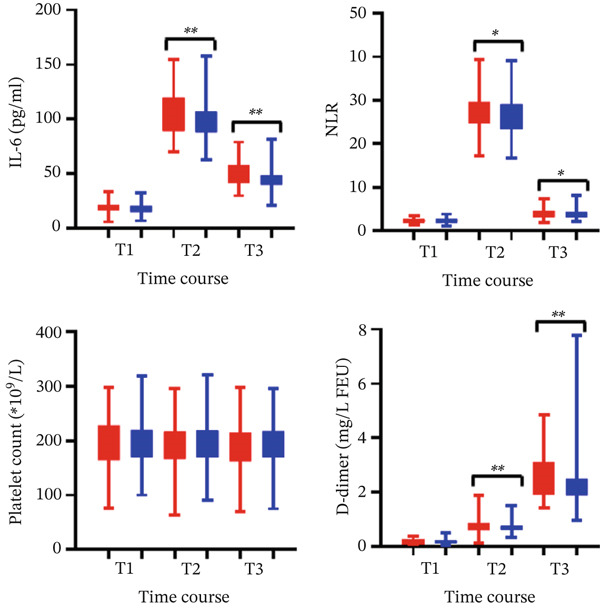 Figure 3
Figure 3| IR group ( | CR group ( |
| |
|---|---|---|---|
| Demographic characteristics | |||
| Age (years) | 56.7 ± 8.2 | 55.9 ± 7.8 | 0.343 |
| Male, no. (%) | 110 (76.9) | 292 (80.6) | 0.347 |
| BMI (kg/m2) | 23.7 ± 1.8 | 23.6 ± 2.0 | 0.767 |
| CYP2C19 metabolizer status | 0.553 | ||
| Wild type | 59 (41.3) | 139 (38.4) | |
| Loss‐of‐function type | 84 (58.7) | 223 (61.6) | |
| Clinical diseases, no. (%) | |||
| Previous MI | 20 (14.0) | 55 (15.2) | 0.783 |
| Previous PCI | 14 (9.8) | 32 (8.8) | 0.733 |
| Left main stenosis | 20 (14.0) | 58 (16.0) | 0.682 |
| Tobacco use, no. (%) | 0.883 | ||
| Never | 78 (54.5) | 203 (56.1) | |
| > 6 months ago | 42(29.4) | 107 (29.5) | |
| <6 months ago | 23(16.1) | 52 (14.4) | |
| Comorbidities profile, no. (%) | |||
| Hypertension | 82 (57.3) | 203 (56.1) | 0.796 |
| Diabetes mellitus | 32 (22.4) | 87 (24.0) | 0.693 |
| Hypercholesterolemia | 39 (27.3) | 109 (30.1) | 0.588 |
| Triglyceride | 28 (19.6) | 68 (18.8) | 0.900 |
| OSAS | 21(14.7) | 42(11.6) | 0.345 |
| COPD | 24(16.8) | 47(13.0) | 0.268 |
| Subclinical hypothyroidism | 11(7.7) | 32(8.8) | 0.677 |
| Preoperative medications, no. (%) | |||
| Aspirin | 133 (93.0) | 343 (94.8) | 0.524 |
| Statins | 135 (94.4) | 339 (93.6) | 0.839 |
| Calcium channel antagonist | 45 (31.5) | 125 (34.5) | 0.532 |
| Nitrate ester | 88 (61.5) | 211 (58.3) | 0.547 |
| Beta‐blocker | 101 (70.7) | 266 (73.5) | 0.509 |
| Diuretics | 25 (17.5) | 66 (18.2) | 0.898 |
| Cardiac function | |||
| LAD (mm) | 35.4 ± 5.3 | 36.9 ± 5.9 | 0.007 |
| LVEDD (mm) | 51.7 ± 5.7 | 51.4 ± 6.2 | 0.683 |
| LVEF (%) | 53.6 ± 10.0 | 54.0 ± 10.4 | 0.678 |
| LVEF ≤ 35 | 11 (7.7) | 41 (11.3) | 0.258 |
| SYNTAX score | 28.6 ± 3.2 | 28.4 ± 3.3 | 0.595 |
| CHADS‐VASc score | 2.0 ± 1.1 | 1.8 ± 1.1 | 0.085 |
| HATCH score | 1.5 ± 1.2 | 1.3 ± 1.2 | 0.187 |
| IR group ( | CR group ( |
| |
|---|---|---|---|
| Intraoperative conditions | |||
| Operation time (min) | 298 ± 40 | 330 ± 44 | < 0.001 |
| IABP assistance support, no. (%) | 27 (18.9) | 70 (19.3) | 1.0 |
| Graft characteristics | |||
| Graft numbers ( | 2.7 ± 0.5 | 3.2 ± 0.6 | < 0.001 |
| Distal anastomosis number ( | 2.8 ± 0.4 | 3.8 ± 0.6 | < 0.001 |
| Transit‐time flow meter (mL/min) | |||
| LIMA | 34 ± 12 | 34 ± 12 | 0.930 |
| D1 | 59 ± 22 | 63 ± 24 | 0.114 |
| OM1/2 | 42 ± 12 | 47 ± 13 | 0.047 |
| RA/PDA/PLV | 36 ± 11 | 35 ± 10 | 0.384 |
| Postoperative medications, no. (%) | 0.630 | ||
| Clopidogrel | 115 (80.4) | 282 (77.9) | |
| Ticagrelor | 28 (19.6) | 80 (22.1) | |
| Antiplatelet time (h) | 16.7 ± 5.9 | 17.0 ± 5.7 | 0.572 |
| ICU recovery | |||
| Mechanical ventilation time (h) | 13.6 ± 10.6 | 13.3 ± 8.4 | 0.699 |
| Duration in ICU stay (d) | 1.6 ± 0.8 | 1.7 ± 0.9 | 0.257 |
| Re‐exploration, no. (%) | 3 (2.1) | 5 (1.4) | 0.693 |
| Chest drainage (mL) | 774 ± 120 | 777 ± 120 | 0.829 |
| 30‐day recovery | |||
| Death, no. (%) | 1 (0.7) | 2 (0.6) | 1.0 |
| Cognitive dysfunction, no. (%) | 16 (11.2) | 20 (5.5) | 0.034 |
| Ischemic stroke, no. (%) | 6 (4.2) | 3 (0.8) | 0.018 |
| Postoperative hospital stay (d) | 10.7 ± 1.8 | 10.3 ± 1.8 | 0.006 |
| IR group ( | CR group ( |
| |
|---|---|---|---|
| POAF incidence ( | 56 | 91 | 0.002 |
| Time to onset (d) | 2.5 ± 1.6 | 2.4 ± 1.3 | 0.677 |
| Percentage of monitoring time in POAF | 10.1% (4.8%, 16.5%) | 6.0% (2.3%, 9.5%) | 0.003 |
| Number of distinct POAF episodes | 9 (6, 14) | 6 (3, 9) | < 0.001 |
| Mean ventricular rate at POAF episodes | 134 (118, 145) | 127 (116, 133) | 0.001 |
| Cumulative duration of all POAF episodes (h) | 17 (8, 28) | 10 (4, 16) | 0.003 |
| Number of prolonged episodes | 0.022 | ||
| Less or equal to 24 h | 39 | 78 | |
| > 24 h | 17 | 13 |
- —National Natural Science and Technology Foundation of China
- —Sichuan Provincial People’s Hospital
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtrial Fibrillation Management and Outcomes · Cardiac, Anesthesia and Surgical Outcomes · Antiplatelet Therapy and Cardiovascular Diseases
Summary
- • What Is Already Known on This Topic: Postoperative atrial fibrillation (POAF) is a frequent and potentially recurrent complication occurring within the first week after off‐pump coronary artery bypass grafting (OPCABG). Myocardial ischemia and inflammation are established pathogenic drivers of POAF, which significantly increase long‐term mortality and cerebrovascular risk after isolated surgical revascularization.
- • What This Study Adds: A total of 505 patients with three‐branch coronary stenosis undergoing elective first‐time OPCABG surgery were retrospectively reviewed and divided into incomplete revascularization (IR) group (n = 143), complete revascularization (CR) group (n = 362) according to the extent of coronary revascularization. IR was associated with significantly higher POAF incidence within 1 week after OPCABG, greater POAF burden, elevated proinflammatory cytokines, and heightened prothrombotic activity. Subgroup analysis revealed that ticagrelor‐based DAPT attenuated outcome differences between IR and CR groups—an effect absent with clopidogrel‐based DAPT.
- • How This Study Might Affect Research, Practice, or Policy: Antiplatelet regimen selection should consider revascularization completeness to optimize POAF prevention, prioritizing ticagrelor‐based DAPT over clopidogrel in incompletely revascularized patients.
1. Introduction
It is well‐established that off‐pump coronary artery bypass grafting (OPCABG), compared with on‐pump CABG, is associated with favorable short‐term outcomes [1] but a higher incidence of incomplete revascularization (IR) [2]. IR has been associated with increased long‐term mortality in patients with multivessel coronary artery disease undergoing single‐artery grafting with left internal mammary artery (LIMA) [3]. Antithrombotic management is pivotal in patients with atherosclerotic cardiovascular disease. Inadequate P2Y12 inhibition and heightened adenosine diphosphate‐mediated platelet aggregation under fixed‐dose regimens are linked to increased major adverse vascular events in patients with polyvascular atherothrombotic disease [4].
POAF is a frequent and potentially recurrent complication occurring within the first week after OPCABG during intensive medical care. It disrupts normal cardiac rhythm and promotes thrombus formation and stroke risk during long‐term follow‐up [5]. Patients with POAF experiencing a high arrhythmia burden face an elevated risk of stroke and other cardiovascular events compared to those with a low burden [6]. Currently, no single modifiable risk factor reliably predicts POAF occurrence; however, an emerging AI‐based bedside tool has been developed to predict POAF with good discrimination by leveraging existing patient characteristics [7]. Nevertheless, the potential influence of specific intraoperative factors such as the completeness of revascularization combined with the postoperative antiplatelet regimen on predisposing OPCABG patients to POAF remains inadequately investigated. Therefore, we conducted this retrospective cohort study to explore how the interaction between completeness of revascularization and postoperative antiplatelet therapy influences POAF incidence and burden.
2. Methods
2.1. Ethical Approval Statement
The Medical Ethics Review Board of Sichuan Provincial People’s Hospital granted institutional approval for this study (Approval No. 2021216; March 1st, 2021) and waived the requirement for written informed consent due to the retrospective, observational design.
2.2. Patients
For this association analysis, we screened electronic medical records of patients undergoing elective first‐time OPCABG between May 2017 and May 2024. Inclusion criteria comprised patients who (1) underwent elective first‐time OPCABG with three‐branch stenosis and (2) received a regular single arterial graft with LIMA anastomosis to the left anterior descending (LAD) artery. Exclusion criteria included the following: preexisting atrial fibrillation/atrial flutter, uncontrolled hyperthyroidism, or multiarterial revascularization [8]. The primary outcome was the cumulative incidence of POAF within the first postoperative week. Secondary outcomes included postoperative clinical metrics during hospitalization: POAF burden, inflammatory indices, and prothrombotic markers.
2.3. Surgical Procedure and Definition of IR
All off‐pump coronary artery bypass anastomoses were performed via median sternotomy by an experienced surgeon under a standardized induction and anesthesia protocol. Saphenous vein grafts were harvested using conventional techniques [9] for non‐LAD targets (right coronary artery [RCA] or circumflex artery [LCx] systems). Patient‐controlled analgesia and a flexible chest tube were utilized to mitigate postoperative pain. IR was defined as the absence of a graft to any major coronary territory (RCA or LCx system) or its major branch vessels with ≥ 70% stenosis, assessed via coronary angiography review on Neusoft PACS/RIS Workstation (Version 5.5; Neusoft Corp., Shenyang, China) [10]. CR was defined as graft placement to all major coronary territories (RCA and LCx systems) with significant (≥ 70%) stenosis. If a major branch within a system (e.g., obtuse marginal branch in LCx and posterior descending artery or posterolateral branch in RCA) had significant stenosis but was not grafted, revascularization was still considered complete if another major branch within the same system received more than one graft and provided adequate flow to the ischemic territory.
2.4. POAF Metrics
Continuous cardiac monitoring was maintained throughout hospitalization, including ICU and intermediate care stays. Standby 12‐lead electrocardiography (ECG) was available for confirmation [11]. POAF was defined as an ECG‐documented atrial rhythm with (1) absence of distinct P‐waves, (2) irregular R–R intervals, and (3) ventricular rate > 100 beats/min, persisting for ≥ 30 s [12]. POAF burden was quantified per patient as follows: (1) number of distinct POAF episodes; (2) cumulative duration of all POAF episodes (hours); and (3) percentage of monitoring time in POAF [13].
2.5. Inflammatory Biomarkers
All patients were routinely transferred to the intensive care unit (ICU) postoperatively for monitoring and endotracheal intubation for mechanical ventilation. Antiplatelet agents were administered orally after extubation when clinically appropriate or via nasogastric tube if intubated. Beta‐blocker and statin were conventionally prescribed for all indicated patients with dosages tailored to individual conditions. Serum cytokines and simplified surrogate indicators, including interleukin‐6 (IL‐6) and neutrophil–lymphocyte ratio (NLR), were measured at three time points: preoperatively and on postoperative Days 1 and 5 [14]. Standard laboratory parameters (platelet and D‐dimer as a fibrinolytic marker) were obtained from the electronic medical record system at identical time points [15].
2.6. Statistical Analysis
Multivariable Cox regression analyses were performed to identify factors associated with POAF occurrence, with covariates selected based on clinical relevance and prior literature (age, sex, smoking status, obstructive sleep apnea syndrome [OSAS], and postoperative antiplatelet regimen, revascularization completeness, chronic obstructive pulmonary disease [COPD], subclinical hypothyroidism, coronary artery complexity, and anticoagulation guidance score). The cumulative incidence of POAF within the first postoperative week was analyzed using Kaplan–Meier curves with log‐rank testing. POAF burden metrics (episode count, cumulative duration, and time percentage) were analyzed using Mann–Whitney U tests (nonnormal distributions). Continuous variables are presented as mean ± standard deviation (SD) for normally distributed data or median with interquartile range (IQR) for nonnormally distributed data, assessed using the Kolmogorov–Smirnov test. Categorical variables are expressed as frequencies (percentage) and compared using χ ^2^ or Fisher’s exact tests as appropriate. All analyses were conducted using IBM SPSS Statistics (Version 25.0; Armonk, NY) and GraphPad Prism (Version 10.4.1; San Diego, CA), with statistical significance defined as two‐sided p < 0.05.
3. Results
After screening 594 patients against inclusion criteria, 89 were excluded. Ultimately, 505 patients were included in the final analysis and stratified into IR (n = 143, 28.3%) and CR (n = 362, 71.7%) groups (Figure 1). Baseline demographic characteristics and comorbidities were comparable between groups (Table 1). Significant intergroup differences were observed in mean number of grafts per patient (2.7 ± 0.5 vs. 3.2 ± 0.6, p < 0.001) and distal anastomoses per patient (2.8 ± 0.4 vs. 3.8 ± 0.6, p < 0.001). However, intraoperative transit‐time flow measurements demonstrated comparable graft patency between groups (Table 2).
The study protocol OPCABG, off‐pump coronary artery bypass grafting; IR, incomplete revascularization; CR, complete revascularization.
3.1. POAF incidence
Multivariate Cox regression analyses identified independent prognostic factors with statistical significance only including postoperative antiplatelet regimen, revascularization completeness, and COPD. Multivariable logistic regression revealed that IR was associated with a 3.54‐fold increased risk of POAF (adjusted odds ratio [aOR] = 1.599, 95% CI: 1.141–2.241) compared to CR. Similarly, a clopidogrel‐based regimen was associated with higher POAF risk (aOR = 2.077, 95% CI: 1.309–3.293) versus ticagrelor therapy, particularly among CYP2C19 loss‐of‐function allele carriers. While, COPD imposed a modest impact on POAF (COPD: 27/71 (38.0%) vs. without COPD: 120/434 (27.6%), p = 0.074). Cumulative incidence analysis demonstrated significantly higher POAF occurrence in IR patients (39.2%, 56/143) versus CR patients (25.4%, 92/362), with an overall hazard ratio of 1.70 (95% CI: 1.18–2.46; p = 0.002; Figure 2). Time to dual antiplatelet therapy (DAPT) initiation post‐OPCABG was comparable between regimens. Stratified analysis by antiplatelet regimen: clopidogrel group: POAF incidence 42.6% (IR) vs. 25.9% (CR) (p = 0.001); ticagrelor group: POAF incidence 25.0% (IR) vs 22.5% (CR) (p > 0.05). A significant interaction between revascularization status and antiplatelet regimen was observed (p interaction < 0.001).
Kaplan–Meier analysis of POAF incidence by revascularization completeness. The cumulative incidence of POAF was 39.2% in the incomplete revascularization (IR) group versus 25.1% in the complete revascularization (CR) group (hazard ratio [HR] for IR vs. CR: 1.70; 95% confidence interval [CI]: 1.18–2.46; p = 0.002). Dashed lines represent 95% CIs. Numbers at risk are shown below the x‐axis. Abbreviations: POAF, postoperative atrial fibrillation; HR, hazard ratio; CI, confidence interval; IR, incomplete revascularization; CR, complete revascularization.
3.2. Inflammatory and Prothrombotic Profiles
Significantly higher IL‐6 levels were observed in the IR group versus CR group at postoperative 1 day (104 ± 20 vs. 98 ± 16 pg/mL, p < 0.001) and 5 days (49 ± 11 vs. 45 ± 9 pg/mL, p < 0.001). Similarly, NLR was elevated in IR patients at postoperative 1 day (27.3 ± 3.7 vs. 26.3 ± 4.1, p = 0.013), and 5 days (4.0 ± 1.1 vs. 3.8 ± 1.1, p = 0.043). Platelet counts showed no significant intergroup differences at any measurement point. D‐dimer levels—reflecting prothrombotic activity—increased progressively in both cohorts but remained significantly higher in the IR group at postoperative 1 day (0.8 ± 0.3 mg/L FEU vs. 0.7 ± 0.2 mg/L FEU, p = 0.001), at postoperative 5 days (2.6 ± 0.7 mg/L FEU vs. 2.3 ± 0.7 mg/L FEU, p < 0.001; Figure 3).
Serial measurements of inflammatory and prothrombotic markers in two groups. Levels of interleukin‐6 (IL‐6), neutrophil–lymphocyte ratio (NLR), platelet count, and D‐dimer (mg/L FEU) were measured preoperatively (T1) and on postoperative Day 1 (T2) and Day 5 (T3). Data presented as box plots (boxes: interquartile range; horizontal line: median; whiskers: range). ∗ p < 0.05 and ∗∗ p < 0.01 for IR vs. CR at each timepoint. Notes: Red bar: incomplete revascularization; blue bar: complete revascularization.
3.3. Postoperative Outcomes
Length of hospital stay was significantly longer in the IR group versus CR group (10.7 ± 1.8 vs. 10.3 ± 1.8 days; p = 0.006; Table 2). During POAF episodes, the median ventricular rate was significantly higher in IR patients (134 [118, 145] vs. 127 [116, 133] bpm; p = 0.001). POAF burden metrics consistently demonstrated greater severity in the IR group: monitoring time in POAF: 10.1% [4.8%–16.5%] versus 6.0% [2.3%–9.5%] (p = 0.003); prolonged episodes (> 24 h): 30.4% versus 14.3% (p = 0.022; Table 3).
4. Discussion
This retrospective cohort study demonstrates two principal findings: (1) IR independently increased POAF risk after OPCABG compared to CR, manifesting as higher POAF burden, amplified inflammatory response, and enhanced prothrombotic activity and (2) the POAF risk disparity between IR and CR was confined to clopidogrel‐treated patients with no significant difference observed under ticagrelor therapy, indicating a critical drug–revascularization interaction particularly pronounced in CYP2C19 loss‐of‐function allele carriers.
Personalized management by multidisciplinary critical care teams is essential given its unpredictable nature and challenges in POAF prevention [16]. Both myocardial ischemia and inflammation are established pathogenic drivers of POAF [17] with peak burden occurring on postoperative Days 2–3 [18], which significantly increases long‐term mortality and cerebrovascular risk after isolated surgical revascularization [19]. Thus, elucidating the impact of modifiable perioperative factors such as particularly revascularization completeness and antiplatelet regimen selection on POAF occurrence and severity is clinically imperative for optimizing OPCABG outcomes.
CR remains the surgical gold standard for optimizing long‐term outcomes and cardiac function in CABG [20]. In patients with multivessel disease, grafting ≥ 1 distal anastomosis per major coronary branch significantly improves survival and reduces cardiac mortality [21]. While IR of nondominant branches may not impact major adverse events, CR of all angiographically significant lesions (≥ 70% stenosis) demonstrably lowers adverse event rates [22]. However, CR achievement is frequently constrained by diffuse disease, technical limitations, and patient comorbidities [23]. Notably, contemporary data suggest IR rates are increasing over time [24]. Despite advantages in select populations like hybrid revascularization [25], OPCABG faces inherent technical challenges: hemodynamic instability during heart positioning, limited visualization of inferior/posterolateral territories, and restricted anastomotic access during beating heart surgery. Thus, mitigating the long‐term sequelae of unavoidable IR, particularly its association with heightened inflammation, POAF risk, and thrombotic burden represents a critical unmet need in surgical coronary revascularization.
IL‐6, a cytokine rapidly synthesized following coronary artery bypass grafting, orchestrates key inflammatory pathways that potentiate atherosclerotic progression. Through stimulation of endothelial activation, vascular smooth muscle proliferation, and leukocyte recruitment, IL‐6 mediates plaque destabilization and perioperative myocardial injury [26]. Simultaneously, OPCABG induces significant activation of the coagulation cascade and compensatory fibrinolysis. Notably, this prothrombotic state persists despite therapeutic heparinization in completely revascularized patients, suggesting intrinsic limitations in pharmacologic reversal of surgically triggered thrombosis [27].
Platelets are central mediators of thromboinflammation. Clinical evidence demonstrates ticagrelor’s superior net clinical benefit over other P2Y_12_ inhibitors across indications, particularly in acute coronary syndromes, high thrombotic risk profiles, and extended secondary prevention [28]. Mechanistically, ticagrelor inhibits equilibrative nucleoside transporter‐1, increasing extracellular adenosine concentrations. This potentiates adenosine’s cardioprotective effects through coronary vasodilation, anti‐inflammatory modulation, and platelet inhibition [29]. Critically, potent P2Y_12_ inhibition with ticagrelor reduces major adverse cardiovascular events in high‐risk acute myocardial infarction and cardiogenic shock patients without increasing severe bleeding risk, excluding those aged > 75 years or requiring VA‐ECMO support [30].
Patients on the clopidogrel but not ticagrelor with IR demonstrated significantly higher POAF burden and prolonged hospitalization compared to CR. This result was similar to the scenario of percutaneous coronary intervention treatment on oral clopidogrel regimen that clinical factors (such as age and acute coronary syndrome) may be more decisive than CYP2C19 genotype on the accidence rate of major adverse cardiac event [31]. Thus, these findings underscore the critical need for multidisciplinary collaboration (surgeons, intensivists, and nursing teams) to implement precision antiplatelet strategies that mitigate IR‐related risks. It was advised for IR patients to prioritize ticagrelor over clopidogrel for POAF prophylaxis in IR patients, particularly CYP2C19 LOF carriers, initiate early DAPT upon hemodynamic stabilization post‐OPCABG, and protocolize POAF screening during peak burden days. This optimized approach addresses the clinical and economic burdens of prolonged hospitalization [32] while improving outcomes for patients with residual stenosis. For unavoidable IR cases, targeted antiplatelet management represents a feasible strategy to counterbalance anatomic limitations.
5. Study Limitations
This analysis inherits limitations inherent to retrospective studies, including potential documentation heterogeneity in POAF detection. Despite adopting standardized criteria (ECG‐confirmed AF ≥ 30 s [33]), variations in monitoring protocols across clinicians and shifts may have resulted in under‐ascertainment of transient arrhythmias. We defined completeness of revascularization anatomically (grafting vessels with ≥ 70% stenosis) rather than functionally [34]. While anatomic assessment remains the surgical gold standard [23], this approach may overlook territories with functionally significant ischemia in moderately stenotic lesions (40%–70%), potentially attenuating observed CR benefits. Prothrombotic states were assessed via D‐dimer rather than viscoelastic testing, which could have provided mechanistic insights into platelet–fibrin interactions and hypercoagulable phenotypes not captured by conventional assays [35].
6. Conclusions
This real‐world analysis demonstrates that IR significantly increases POAF risk after OPCABG, particularly in clopidogrel‐treated patients where POAF incidence nearly doubled. Crucially, this risk was abrogated by ticagrelor therapy, indicating that precision antiplatelet selection mitigates IR‐related arrhythmogenicity. These findings illuminate the thromboinflammatory pathogenesis of POAF and support protocolized ticagrelor use as a preventive strategy in IR patients, especially CYP2C19 loss‐of‐function carriers.
Author Contributions
Q.J. and Y.Y. performed the research and wrote the manuscript. Q.J. and S.H. designed the research. Q. J. and Z.T. analyzed the data. M.X. and J.X. contributed new analytical tools.
Funding
This study was supported by the Sichuan Provincial People’s Hospital, SY2022017, and National Natural Science and Technology Foundation of China, 81800274.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dąbrowski E. J. , Kurasz A. , Pasierski M. , Pannone L. , Kołodziejczak M. M. , Raffa G. M. , Matteucci M. , Mariani S. , de Piero M. E. , la Meir M. , Maesen B. , Meani P. , Mc Carthy P. , Cox J. L. , Lorusso R. , Kuźma Ł. , Rankin S. J. , Suwalski P. , Kowalewski M. , and Thoracic Research Centre , Surgical Coronary Revascularization in Patients With Underlying Atrial Fibrillation: State-of-the-Art Review, Mayo Clinic Proceedings. (2024) 99, no. 6, 955–970, · doi ↗ · pubmed ↗
- 2Razavi A. A. , Malas J. , Salam A. , Emerson D. A. , and Bowdish M. E. , Off-Pump Coronary Artery Bypass Grafting Is Overutilized, Seminars in Thoracic and Cardiovascular Surgery. (2025) 37, no. 1, 43–47, 10.1053/j.semtcvs.2024.12.001, 39730082.39730082 PMC 12077573 · doi ↗ · pubmed ↗
- 3Aboul-Hassan S. S. , Awad A. K. , Stankowski T. , Perek B. , Marczak J. , Rodzki M. , Jemielity M. , Moskal L. , Sá M. P. , Torregrossa G. , Gaudino M. , and Cichon R. , Impact of Incomplete Revascularization on Long-Term Survival Based on Revascularization Strategy, Annals of Thoracic Surgery. (2024) 118, no. 3, 605–614, 10.1016/j.athoracsur.2024.04.032, 38777249.38777249 · doi ↗ · pubmed ↗
- 4Chaudhary R. and Neal M. D. , Invited Commentary: Platelet and Clot Characteristics to Guide Antithrombotic Management in Patients With Polyvascular Disease, Journal of the American College of Surgeons. (2023) 236, no. 3, 504–505, 10.1097/XCS.0000000000000493, 36729750.36729750 · doi ↗ · pubmed ↗
- 5Benedetto U. , Gaudino M. F. , Dimagli A. , Gerry S. , Gray A. , Lees B. , Flather M. , Taggart D. P. , and Investigators A. R. T. , Postoperative Atrial Fibrillation and Long-Term Risk of Stroke After Isolated Coronary Artery Bypass Graft Surgery, Circulation. (2020) 142, no. 14, 1320–1329, 10.1161/CIRCULATIONAHA.120.046940, 33017213.33017213 PMC 7845484 · doi ↗ · pubmed ↗
- 6Linz D. , Andrade J. G. , Arbelo E. , Boriani G. , Breithardt G. , Camm A. J. , Caso V. , Nielsen J. C. , De Melis M. , De Potter T. , Dichtl W. , Diederichsen S. Z. , Dobrev D. , Doll N. , Duncker D. , Dworatzek E. , Eckardt L. , Eisert C. , Fabritz L. , Farkowski M. , Filgueiras-Rama D. , Goette A. , Guasch E. , Hack G. , Hatem S. , Haeusler K. G. , Healey J. S. , Heidbuechel H. , Hijazi Z. , Hofmeister L. H. , Hove-Madsen L. , Hueb · doi ↗ · pubmed ↗
- 7Ma H. , Chen D. , Lv W. , Liao Q. , Li J. , Zhu Q. , Zhang Y. , Deng L. , Liu X. , Wu Q. , Liu X. , and Yang Q. , Performance of an AI Prediction Tool for New-Onset Atrial Fibrillation After Coronary Artery Bypass Grafting, E Clinical Medicine. (2025) 81, 103131, 10.1016/j.eclinm.2025.103131.40093989 PMC 11908608 · doi ↗ · pubmed ↗
- 8Jiang Q. , Huang K. , Lin S. , Wang D. , Tang Z. , and Hu S. , Impact of Multiarterial Versus Single Arterial Coronary Bypass Graft Surgery on Postoperative Atrial Fibrillation, American Journal of Cardiology. (2025) 234, 30–37, 10.1016/j.amjcard.2024.10.004, 39447720.39447720 · doi ↗ · pubmed ↗