Prognostic value of preoperative anorectal manometry parameters for anastomotic leakage after sphincter-preserving surgery for rectal cancer
Jin Gi Chang, Eon Bin Kim, Chan Wook Kim, Yong Sik Yoon, Jong Lyul Lee, In Ja Park, Seok-Byung Lim

TL;DR
High preoperative anal pressure measured by manometry predicts anastomotic leakage risk after rectal cancer surgery.
Contribution
Identifies preoperative anorectal manometry parameters as novel predictors of anastomotic leakage.
Findings
Higher maximum resting pressure correlates with increased anastomotic leakage risk.
Maximum resting pressure of 55.65 mm Hg is a predictive cutoff for leakage.
Shorter tumor distance from the anal verge also predicts leakage.
Abstract
Anastomotic leakage (AL) remains a serious complication following low anterior resection (LAR) for rectal cancer. Although several risk factors for AL have been identified, the role of preoperative anal sphincter function remains unexplored. We hypothesized that elevated maximum resting pressure (MRP) and maximum squeeze pressure (MSP), measured preoperatively via anorectal manometry (ARM), might increase AL risk by inducing functional outlet obstruction. This single-center retrospective cohort study included patients who underwent LAR without a diverting stoma between January 2010 and December 2015. We analyzed the associations between preoperative ARM parameters and early major AL events. Independent predictors of AL were also identified. Receiver operating characteristic curve analysis was performed to evaluate the predictive value of ARM parameters for AL. Among 1,396 patients,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
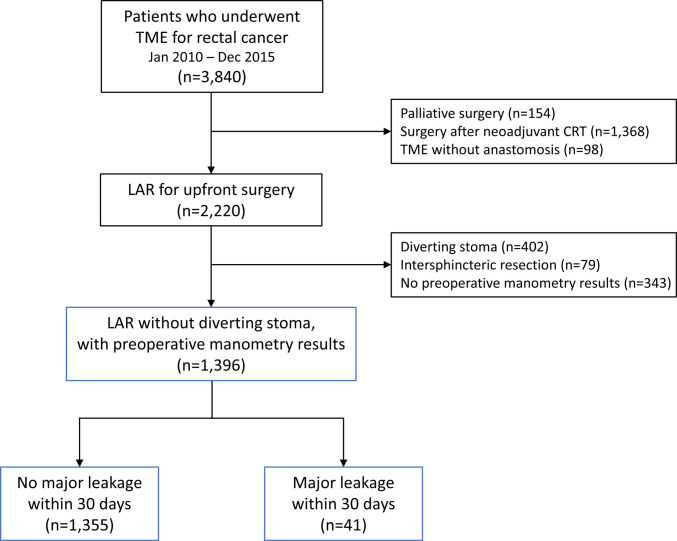 Figure 1
Figure 1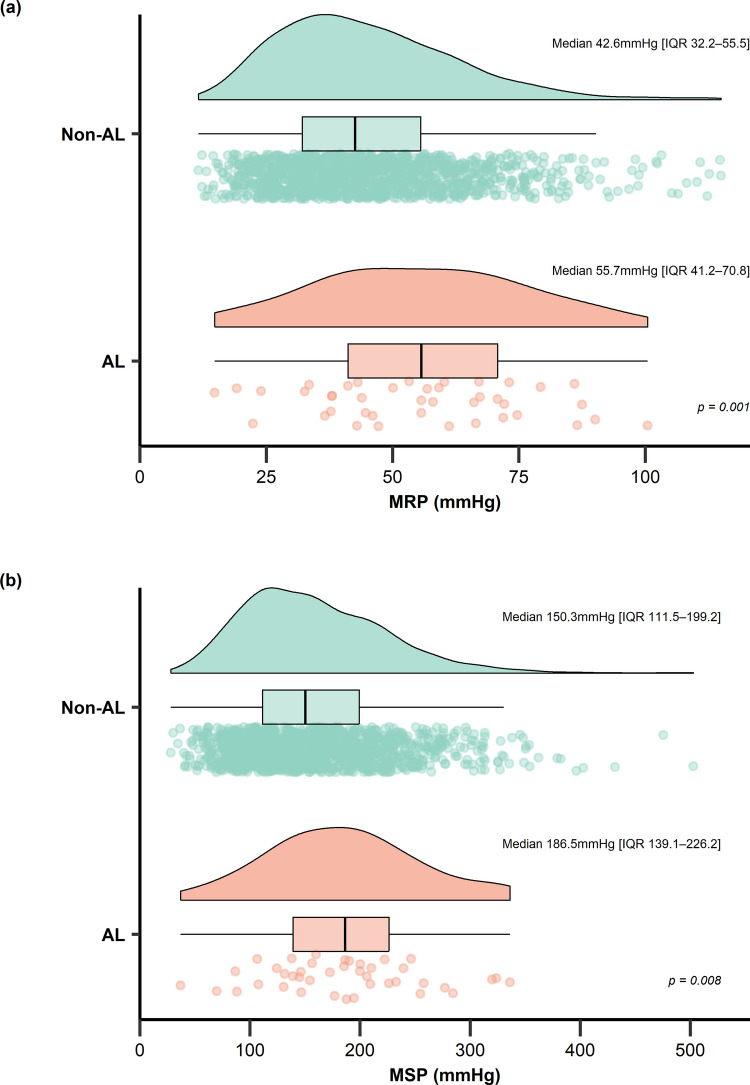 Figure 2
Figure 2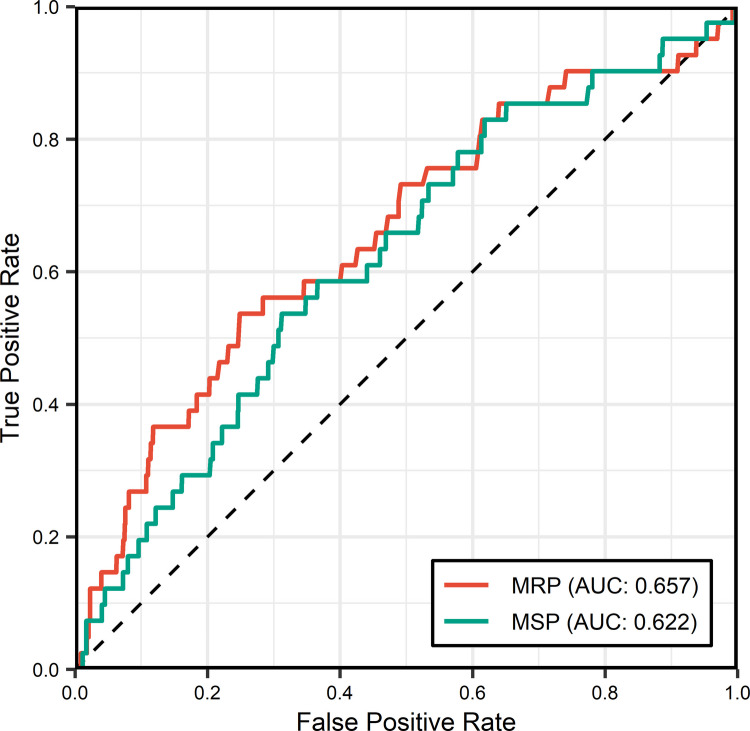 Figure 3
Figure 3- —National Research Foundation of Korea (NRF) grant funded by the Korea government, Ministry of Science and ICT (MSIT)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsColorectal Cancer Surgical Treatments · Anorectal Disease Treatments and Outcomes · Pelvic floor disorders treatments
Introduction
Rectal cancer is one of the most common gastrointestinal malignancies worldwide, with total mesorectal excision (TME) as the standard surgical approach for middle and lower rectal cancers [1, 2]. Despite advances in surgical techniques and perioperative care, anastomotic leakage (AL) remains one of the most feared complications following rectal cancer surgery, affecting both short-term morbidity and long-term outcomes [3, 4]. The incidence of AL after low anterior resection (LAR) has been reported to range from 4 to 20%, depending on the definitions applied and the method of detection [5–8]. Regardless of severity, AL is significantly associated with increased mortality, reoperation rates, and hospital costs [8]. Furthermore, it impairs long-term anorectal function and may compromise oncologic survival [9].
Despite extensive research on risk factors for AL, the role of anal sphincter function—as measured via anorectal manometry (ARM)—remains largely unexplored. ARM objectively quantifies sphincter pressures [10]. The internal anal sphincter maintains the maximum resting pressure (MRP), preventing passive fecal spillage, while the external anal sphincter generates the maximum squeeze pressure (MSP) for voluntary control. Although ARM is well established for predicting postoperative functional outcomes such as fecal incontinence or LAR syndrome, its potential role in predicting AL has not yet been investigated [11].
We hypothesized that elevated anal sphincter pressure might increase intraluminal pressure at the anastomotic site, potentially compromising staple line integrity. Therefore, the present study aimed to evaluate whether preoperative ARM parameters are associated with AL after LAR.
Methods
Study design & patient selection
This single-center retrospective cohort study was conducted at Asan Medical Center. We screened consecutive patients who underwent TME with LAR for rectal cancer between January 2010 and December 2015. Preoperative workup included colonoscopy, abdominopelvic/chest CT, and rectal MRI. Liver MRI or PET-CT was performed to evaluate suspected metastases. Patients were included if they underwent elective LAR with primary double-stapling anastomosis below the peritoneal reflection. Exclusion criteria included palliative surgery, prior neoadjuvant chemoradiotherapy, TME without primary anastomosis (e.g., Hartmann’s procedure or abdominoperineal resection), construction of a diverting stoma, and incomplete preoperative anorectal manometry data. Additionally, patients who underwent intersphincteric resection were excluded to minimize confounding related to postoperative alterations in anal sphincter function.
Data collection and definitions
Clinical and pathological data were extracted from the patients’ electronic medical records. The collected clinicopathological variables included age, sex, diabetes mellitus, hypertension, body mass index (BMI), tumor distance from the anal verge, type of operation, surgical approach (open vs. minimally invasive surgery), T stage, N stage, and postoperative early major AL events. Early major AL was defined according to the International Study Group of Rectal Cancer (ISREC) grading system as grade C leakage occurring within 30 days after surgery [3]. Preoperative ARM parameters were obtained from manometry reports and included high-pressure zone length (HPZL), MRP, and MSP.
Surgical procedures
During the study period, all surgical procedures were performed by eight board-certified colorectal surgeons using open, laparoscopic, or robotic approaches. Patients underwent mechanical bowel preparation, with prophylactic antibiotics administered preoperatively and discontinued within 24 h postoperatively. LAR involved high or low ligation of the inferior mesenteric artery and total or tumor-specific mesorectal excision, followed by double-stapled anastomosis. The extent of mesorectal excision was determined based on tumor location; TME was performed for mid-to-low rectal cancers, whereas tumor-specific mesorectal excision was applied for upper rectal and rectosigmoid cancers. The creation of a protective diverting stoma was determined intraoperatively at the surgeon’s discretion, based on patient-related risk factors and intraoperative findings. Transanal decompression tubes were not used in this study cohort.
Anorectal manometry
Preoperative ARM was routinely performed for candidates of sphincter-preserving surgery, typically within one month before the surgery. The test was performed using a Microcapillary Infusion System (J.S. Biomedicals Inc., USA) via the distilled water infusion method. A 5-mm-diameter catheter equipped with eight radially oriented pressure channels—positioned 5 cm from the catheter tip—was used, with distilled water perfused at a constant rate of 0.5 mL/channel/min. Data were recorded and analyzed using LGI Polygram software (Synetics Liberty System, USA) to calculate key parameters, including vector volume, sphincter pressures, and HPZL. Patients were placed in the left lateral decubitus position. Following zero-point calibration at the anal verge, the catheter was inserted such that the pressure channels were positioned 6 cm above the anal verge. Resting and squeeze pressures were alternately measured in triplicate using a rapid pull-through technique at a constant speed of 1 cm/s. MRP and MSP were calculated, with the latter defined as the mean of the peak pressures recorded during voluntary squeeze maneuvers. Subsequently, stationary pull-through testing was conducted at 1-cm intervals. Rectal sensory parameters, including minimal sensory volume and maximal tolerance volume, was assessed using a balloon catheter inflated incrementally by 60 mL. The reference normal ranges were as follows: HPZL, 2.0–3.5 cm; MRP, 40–70 mm Hg; and MSP, 100–180 mm Hg.
Study outcomes
The primary outcome was the association between preoperative ARM parameters (i.e., HPZL, MRP, and MSP) and the incidence of early major AL. Secondary outcomes included identifying independent risk factors (from clinicopathological and preoperative ARM parameters) for AL and assessing the predictive performance of preoperative ARM parameters.
Statistical analysis
Continuous variables were presented as mean ± standard deviation (SD) or median with interquartile range (IQR), as appropriate. Categorical variables were expressed as frequencies and percentages. Between-group comparisons were performed using Student’s t test or the Mann–Whitney U test for continuous data, and Pearson’s chi-square test or Fisher’s exact test for categorical data. Logistic regression analyses were conducted to identify independent risk factors for AL. Variables with clinical significance, including key manometric parameters, were entered into the multivariable model. The predictive performance of preoperative ARM parameter was evaluated using receiver operating characteristic (ROC) curve analysis. The area under the ROC curve (AUC) and its 95% confidence interval (CI) were calculated. The optimal cutoff value was determined using the Youden index, and the corresponding sensitivity and specificity were reported. A two-sided p value < 0.05 was considered statistically significant. All statistical analyses were performed using R software (version 4.5.1; R Foundation for Statistical Computing, Vienna, Austria).
Results
Clinicopathological characteristics
Of the 3,840 patients who underwent LAR for rectal cancer, 1,396 were enrolled (Fig. 1). Among this cohort, early major AL occurred in 41 patients (2.9%). The median time to AL diagnosis was 6 days (IQR, 3–13 days). Table 1 summarizes baseline clinicopathological characteristics. Patients who developed AL were younger (57.1 ± 11.7 vs. 60.9 ± 10.5 years, p = 0.024) and had a significantly shorter tumor distance from the anal verge (7.7 ± 2.4 vs. 9.1 ± 2.7 cm, p = 0.002), compared with patients without AL. There were no significant differences in sex, comorbidities, or tumor stage between the groups.Fig. 1. Patient selection flow diagram; TME, total mesorectal excision; CRT, chemoradiotherapy; LAR, low anterior resectionTable 1Clinicopathological characteristicsVariablesTotal (n = 1,396)Non-AL (n = 1,355)AL (n = 41)pSex0.369 Female, no. (%)554 (39.7)541 (97.7)13 (2.3) Male, no. (%)842 (60.3)814 (96.7)28 (3.3)Age (years), mean (SD)60.8 (10.5)60.9 (10.5)57.1 (11.7)0.024Diabetes mellitus, no. (%)183 (13.1)180 (98.4)3 (1.6)0.379Hypertension, no. (%)485 (34.7)471 (97.1)14 (2.9)1.000BMI (kg/m2), mean (SD)23.8 (3.0)23.8 (3.0)23.0 (3.2)0.111Tumor distance from AV (cm), mean (SD)9.0 (2.7)9.1 (2.7)7.7 (2.4)0.002Approach type0.794 Open, no. (%)704 (50.4)682 (96.9)22 (3.1) MIS, no. (%)692 (49.6)673 (97.3)19 (2.7)T stage0.647 T0-T2, no. (%)507 (36.3)494 (97.4)13 (2.6) T3-T4, no. (%)889 (63.7)861 (96.9)28 (3.1)N stage1.000 N0, no. (%)828 (59.3)804 (97.1)24 (2.9) N +, no. (%)568 (40.7)551 (97.0)17 (3.0)AL anastomotic leakage, AV anal verge, BMI body mass index, MIS minimally invasive surgery, SD standard deviation
Preoperative ARM parameters
When preoperative ARM parameters were compared by AL status, median HPZL did not differ significantly between the groups (Table 2); however, both median MRP and MSP were significantly higher in the patients with AL (p = 0.001 and 0.008, respectively). As illustrated in Fig. 2, both MRP and MSP showed right-shifted distributions in the AL group compared with the non-AL group. Table 2. Comparison of preoperative anorectal manometry parameters by anastomotic leakage statusParametersTotal (n = 1,396)Non-AL (n = 1,355)AL (n = 41)pHPZL (cm)2.2 (1.8–2.7)2.2 (1.8–2.7)2.3 (2.0–2.6)0.461MRP (mm Hg)42.8 (32.3–56.2)42.6 (32.2–55.5)55.7 (41.2–70.8)0.001MSP (mm Hg)151.1 (111.9–200.2)150.3 (111.5–199.2)186.5 (139.1–226.2)0.008AL anastomotic leakage, HPZL high-pressure zone length, MRP maximum resting pressure, MSP maximum squeeze pressure*Data are presented as median (interquartile range)Fig. 2. Raincloud and box plots of preoperative anorectal manometric parameters by early anastomotic leakage (AL) status. a Maximum resting pressure (MRP). b Maximum squeeze pressure (MSP); IQR, interquartile range
Risk factors for early AL
Univariable logistic regression analysis revealed that age, preoperative MRP, preoperative MSP, and tumor distance from the anal verge were significantly associated with AL (Table 3). In multivariable analysis with these variables, higher preoperative MRP (odds ratio [OR], 1.021; 95% CI, 1.004–1.039; p = 0.017) and shorter tumor distance from the anal verge (OR, 0.815; 95% CI, 0.718–0.925; p = 0.002) were identified as independent risk factors for AL. Table 3. Univariable and multivariable logistic regression analyses for early anastomotic leakageUnivariableMultivariableVariablesOR95% CIpOR95% CIpAge0.9670.939–0.9960.0250.9890.956–1.0220.505Male (vs. Female)1.4310.735–2.7880.292Diabetes mellitus0.5150.157–1.6870.273Hypertension0.9730.505–1.8740.935BMI0.9150.820–1.0200.110MRP1.0281.013–1.044<0.0011.0211.004–1.0390.017MSP1.0061.001–1.010.0101.0030.999–1.0080.158T3-T4 (vs. T0-T2)1.2360.634–2.4080.534N + (vs. N0)1.0340.550–1.9420.918Tumor distance from AV0.8160.719–0.9260.0020.8150.718–0.9250.002MIS (vs. open surgery)0.8750.469–1.6320.675AV anal verge, BMI body mass index, CI confidence interval, MIS minimally invasive surgery, MRP maximum resting pressure, MSP maximum squeeze pressure, OR odds ratio
Predictive performance of preoperative MRP and MSP
ROC curve analysis was performed to evaluate the predictive performance of preoperative MRP and MSP for early major AL (Fig. 3). For MRP, the AUC was 0.657 (95% CI, 0.565–0.749), with an optimal cutoff value of 55.65 mm Hg yielding a sensitivity of 53.7% and a specificity of 75.1% for predicting major AL. For MSP, the AUC was 0.622 (95% CI, 0.538–0.710), with an optimal cutoff value of 185.45 mm Hg yielding a sensitivity of 53.7% and a specificity of 68.8% for predicting major AL.Fig. 3. Receiver operating characteristic curve of preoperative maximum resting pressure (MRP) and maximum squeeze pressure (MSP) for predicting anastomotic leakage; AUC, area under the curve
Clinicopathological characteristics stratified by MRP
Patients were categorized into low (< 55.65 mmHg) and high (≥ 55.65 mmHg) MRP groups based on the cutoff value derived from ROC curve analysis (Table 4). The high MRP group was significantly younger (54.9 vs. 62.8 years, p < 0.001) and had a higher mean BMI (24.2 vs. 23.6 kg/m^2^, p = 0.002) compared to the low MRP group. The prevalence of comorbidities, including diabetes mellitus and hypertension, was significantly lower in the high MRP group. Tumor-related characteristics, including distance from the anal verge (9.2 vs. 9.0 cm, p = 0.267) and tumor stage, did not differ significantly between the two groups. The high MRP group exhibited a significantly higher incidence of early AL (6.1% vs. 1.8%, p < 0.001). Table 4. Clinicopathological characteristics stratified by the MRP cutoff value of 55.65 mmHgVariablesLow MRP group (n = 1,037)High MRP group (n = 359)pSex0.262 Female, no. (%)421 (40.6)133 (37.0) Male, no. (%)616 (59.4)226 (63.0)Age (years), mean (SD)62.8 (9.9)54.9 (10.0)< 0.001Diabetes mellitus, no. (%)161 (15.5)22 (6.1)< 0.001Hypertension, no. (%)386 (37.2)99 (27.6)0.001BMI (kg/m2), mean (SD)23.6 (2.9)24.2 (3.2)0.002Tumor distance from AV (cm), mean (SD)9.0 (2.6)9.2 (2.8)0.267Approach type< 0.001 Open, no. (%)555 (53.5)149 (41.5) MIS, no. (%)482 (46.5)210 (58.5)T stage0.787 T0-T2, no. (%)374 (36.1)133 (37.0) T3-T4, no. (%)663 (63.9)226 (63.0)N stage0.762 N0, no. (%)618 (59.6)210 (58.5) N +, no. (%)419 (40.4)149 (41.5)Early AL, no. (%)19 (1.8)22 (6.1)< 0.001AL anastomotic leakage, AV anal verge, BMI body mass index, MIS minimally invasive surgery, MRP maximum resting pressure, SD standard deviation
Discussion
This retrospective cohort study demonstrated that preoperative MRP measured via ARM was an independent predictor of early major AL. This finding supports our hypothesis that elevated anal resting pressure may increase the risk of AL through a mechanism of functional outlet obstruction. During the early postoperative period, when anastomotic healing remains incomplete, high anal sphincter tone may impede the passage of stool and gas, leading to increased intraluminal pressure proximal to the anastomosis and elevated mechanical stress on the suture line. This proposed mechanism is consistent with evidence from other gastrointestinal surgical settings, where outlet obstruction or elevated intraluminal pressure has been implicated in anastomotic failure. For example, in esophageal surgery, delayed gastric emptying and pyloric dysfunction increase intragastric pressure and are associated with higher rates of esophagogastric AL [12]. In addition, previous studies have shown that transanal tube placement reduces the incidence of AL by decreasing intraluminal pressure at the anastomotic site [13–15]. Collectively, these observations reinforce our proposed pathophysiological model, wherein elevated preoperative anal resting pressure predisposes patients to AL through functional outlet obstruction, particularly during the critical early postoperative phase of anastomotic healing.
To our knowledge, this is the first study to investigate the pathophysiological impact of preoperative ARM parameters on anastomotic integrity following rectal cancer surgery. Previous applications of manometry in colorectal surgery have focused primarily on predicting postoperative functional outcomes—particularly fecal incontinence and LAR syndrome—rather than surgical complications [11, 16, 17]. Several studies have demonstrated that lower preoperative MRP or MSP values are associated with worse postoperative continence after intersphincteric resection or very LAR [17, 18]. However, the potential role of sphincter pressure in the mechanism of anastomotic failure has not been previously explored. Our finding that elevated preoperative MRP is significantly associated with AL represents a conceptually distinct clinical implication. While low sphincter pressures indicate functional weakness that may compromise continence, increased resting pressure may act as a functional outlet obstruction, leading to elevated proximal intraluminal pressure. This pressure gradient is particularly relevant during the immediate postoperative period, when the anastomosis has minimal tensile strength and is therefore highly vulnerable to mechanical disruption [19].
Various factors contribute to the risk of AL. [20]. While male sex, high BMI, and comorbidities are well-known predictors, tumor height remains one of the most robust factors [21–23]. A low anastomosis is associated with a significantly increased risk of AL, largely owing to greater technical complexity and compromised anastomotic perfusion [24–26]. Our findings are concordant with these previous reports. In this study, a shorter tumor distance from the anal verge was associated with a higher incidence of AL, demonstrating a pattern consistent with prior literature indicating increased risk of anastomotic complications in more distal tumors. In multivariable analysis, shorter tumor distance from the anal verge remained an independent risk factor after adjustment for established covariates. This result further reinforces the well-recognized association between shorter tumor distance from the anal verge and an increased risk of AL.
Contrary to general expectations, traditional risk factors such as male sex, BMI, and diabetes mellitus were not identified as independent predictors of AL in our series. This finding likely resulted from the exclusion of two potent confounders: neoadjuvant chemoradiotherapy and diverting stoma formation. Neoadjuvant chemoradiotherapy, in particular, has been reported to potentially alter sphincter tone [27, 28] and, although controversial, may independently influence AL risk [29, 30]. By excluding patients who received neoadjuvant treatment, we aimed to isolate the independent effect of baseline sphincter pressure on anastomotic outcomes. The exclusion of these factors also yielded a lower overall leakage rate (2.9%) compared with that reported in unselected clinical series (4–13%) [6, 7]. While this limits direct generalizability to routine clinical practice, it represents a methodological strength by minimizing confounding and allowing a more precise assessment of the independent contribution of anal sphincter pressure to AL risk. In this context, it is important to recognize that anal sphincter pressures vary by patient demographics; thus, the effects of sex and age on AL risk may be partially mediated through baseline pressure. Previous studies have shown that MRP is higher in males and declines with advancing age [31, 32]. These physiological patterns may suggest a new explanation for the consistently higher incidence of AL observed in male patients. Similarly, the age-dependent decline in sphincter pressure may help explain why patients who developed AL in this study were younger than those without AL. These demographic patterns are further supported by the comparison of characteristics stratified by the MRP cutoff. The high MRP group was significantly younger and had fewer comorbidities, consistent with the known negative correlation between age and sphincter pressure. Notably, although the tumor distance from the anal verge was comparable between the two groups, the incidence of AL was significantly higher in patients with high MRP (6.1% vs. 1.8%). This finding suggests that elevated anal tone appears to be a distinct risk factor, exerting a mechanical impact on the anastomosis independent of tumor location.
Although elevated MSP was hypothesized as a potential risk factor and showed a significant association with AL in univariable analysis (p = 0.010), it failed to demonstrate independent significance in the multivariable model (p = 0.158). This distinction is likely due to the physiological difference between the two ARM parameters. While high MRP may exert continuous intraluminal pressure and sustain physical stress on the anastomotic line, MSP reflects only voluntary, intermittent contractions, which may have a limited impact on AL [33, 34]. Furthermore, the correlation between MRP and MSP may have influenced this result. Prior studies reported that both MRP and MSP were significantly higher in male and younger patients [31, 32]. In addition, patients with sarcopenia have shown concomitant reductions in both MRP and MSP [35]. Accordingly, the higher MSP observed among patients who developed AL may represent a secondary effect driven by its correlation with MRP, rather than indicating that MSP itself is an independent predictor of AL.
The findings of this study have important clinical implications for surgical decision-making in rectal cancer. Preoperative ARM can serve as a supplementary screening tool for preoperative risk stratification. Surgeons may incorporate high preoperative MRP as a complementary tool when determining individualized AL-preventing strategies for each patient. Construction of a diverting stoma can be selectively considered to minimize the consequences of potential AL. When stoma creation is not feasible or is declined by the patient, alternative protective strategies are recommended—for example, transanal drainage tube placement to reduce intraluminal pressure [13–15] or staple line reinforcement techniques, such as circumferential oversewing, to mechanically strengthen the anastomosis [36–38].
This study has several limitations. First, selection bias exists owing to the exclusion of patients with diverting stomas and those receiving neoadjuvant chemoradiotherapy. This limits the generalizability of our findings to high-risk or irradiated populations and may lead to an underestimation of the true incidence of AL. Additionally, the exclusive focus on ISREC Grade C leakage precludes the assessment of risk factors associated with Grade A or B leakage. Second, the proposed mechanism of functional outlet obstruction remains inferential, as we did not directly measure postoperative intraluminal pressures. Third, other relevant surgical factors, such as the number of linear stapler firings, anastomotic level, tension, and objective assessments of anastomotic perfusion were not analyzed. Moreover, the potential influence of mechanical anal dilatation before transanal stapler insertion on sphincter function was not evaluated. Finally, the modest AUC indicates that MRP has limited discriminative ability as a standalone predictor and should therefore be interpreted within the context of a multivariable risk assessment. Future research should focus on external validation in prospective, multicenter cohorts to confirm generalizability. In addition, mechanistic studies incorporating postoperative intraluminal pressure measurements could help clarify whether functional outlet obstruction contributes to AL risk. Furthermore, integrating MRP into comprehensive risk prediction models may improve clinical utility and inform the use of selective interventions, such as diverting stomas or alternative techniques.
Conclusion
Our findings demonstrated that elevated preoperative MRP is independently associated with early major AL after sphincter-preserving surgery for rectal cancer. Preoperative ARM may therefore offer clinically meaningful prognostic value and, following further validation, could assist in identifying patients who are most likely to benefit from targeted protective interventions.