Metastatic Hypopharyngeal Carcinoma Involving the Stomach: A Case Report and Literature Review
Jad Kabbara, tannous Barakat, Mohamad Mouchli, Faris Shweikeh

TL;DR
A rare case of hypopharyngeal cancer spreading to the stomach is reported, highlighting the importance of considering metastasis in stomach ulcers.
Contribution
The paper presents a rare case of hypopharyngeal carcinoma metastasis to the stomach and reviews only three previously documented cases.
Findings
Metastasis of hypopharyngeal cancer to the stomach is exceedingly rare, with only three prior cases reported.
Endoscopists should consider metastatic disease when evaluating malignant stomach ulcers.
Potential therapeutic molecular biomarkers have been identified for metastatic hypopharyngeal carcinoma.
Abstract
Hypopharyngeal squamous cell carcinoma (HSCC) is a highly aggressive malignancy constituting a small proportion of all head and neck cancers. While it has significant metastatic potential, spread to the stomach is exceedingly rare. A case of HSCC with metastasis to the stomach is presented, along with a review of the relevant literature. A 71-year-old male patient with a history of HSCC was admitted to the hospital for melena and anemia. Prior to this presentation, he had documented metastases to the lungs and small bowel. Esophagogastroduodenoscopy (EGD) demonstrated a friable, non-bleeding gastric ulcer with raised margins. Biopsy findings were consistent with metastatic HSCC. He was considered for enrollment in potential oncological clinical trials. We find that while metastasis to the stomach can occur in certain cancers such as breast, lung, and renal cell carcinoma, it is not…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
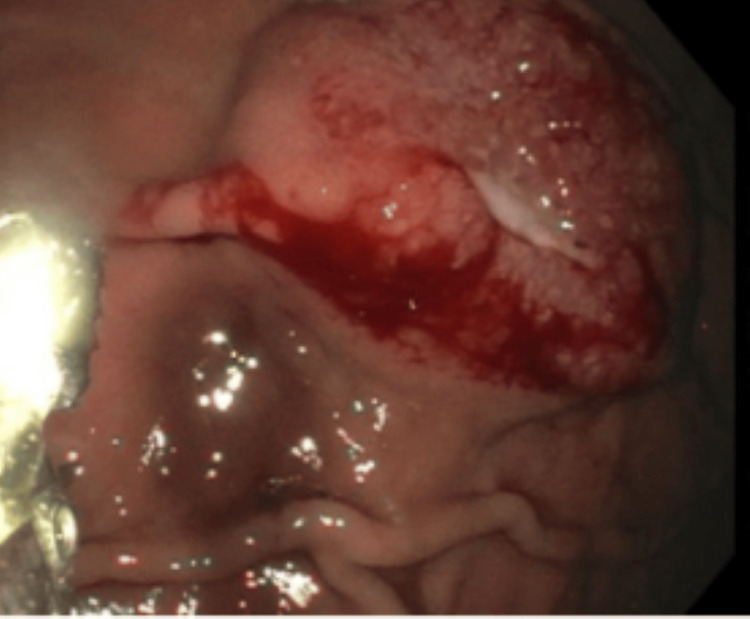 Figure 1
Figure 1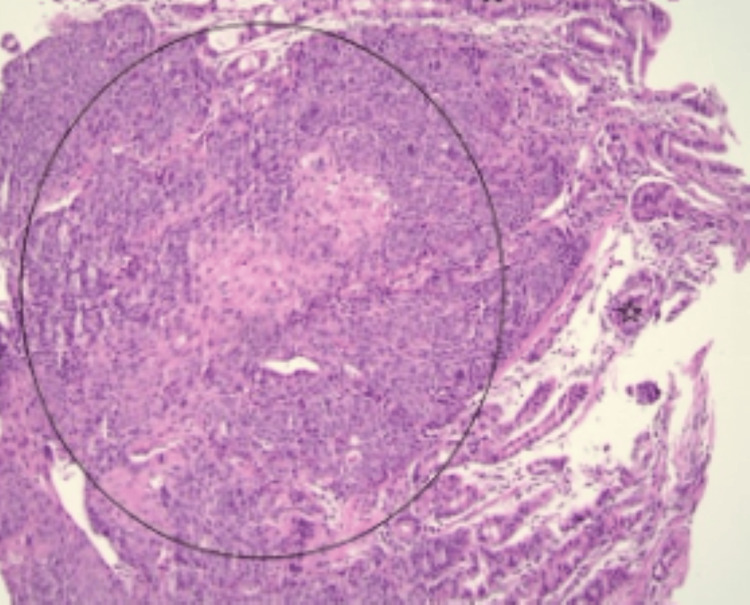 Figure 2
Figure 2| Study | Age/Sex | Primary site | Presentation | Endoscopy findings | Location (in stomach) | Treatment | Outcome | Special Aspects |
| Abdalla et al. [ | 62/M | Hypopharynx | Black-colored stool, epigastric tenderness | Large, ulcerated, non-circumferential mass | Greater curvature | Immunotherapy, palliative chemotherapy | Stabilized with oncology follow-up | NA |
| Moshref et al. [ | 65/M | Prostate | Epigastric pain, heartburn, decreased appetite, nausea, worsening anemia | Ulcerated area | Greater curvature | 20 GY radiation in 5 fractions, declined further therapy | Death at 9 months | NA |
| Paricio et al. [ | 85/F | Cutaneous melanoma of right foot | Severe asthenia, anemia, weight loss | 4 gastric lesions with central ulceration and blackish area and friable consistency | Body and subcardial region | NR | NR | Positive for S100, HMB-45, Melan-A |
| McIlwaine et al. [ | 80/F | Kidney (clear cell) | Malaise, weight loss, raised inflammatory markers, acute hematemesis | Polypoidal lesion, irregular pit pattern | Greater curvature | None, patient preference | NR | Pulmonary metastases also |
| Fu et al. [ | 63/F | Lobular carcinoma of breast | Upper abdominal discomfort and fatigue | Scattered polyps and mucosal infiltration throughout the stomach | Gastric antrum, body, cardia | Endocrine therapy | Reached stable disease course | Immunohistochemistry: ER positive |
| Reise-Filteau et al. [ | 63/F | cSCC of right temple, HIV+ | Functional decline, ascites, SOB, anemia | Submucosal ulcerated lesion, raised lesion on duodenum | Gastric antrum | Palliation | Death 3 weeks after readmission | Genomic profiling: MetS had similar mutations as cSCC, |
| Fuladi et al. [ | 72/F | Thyroid (anaplastic carcinoma) | Nausea, vomiting | 7-8 large polypoidal lesions | NR | NR | Death due to hemorrhagic shock following admission | NA |
| Wu et al. [ | 68/M | Hypopharynx | Hematemesis | Polypoid mass with a ragged surface and irregular ulcerations | Greater curvature | None, patient died, refused invasive surgical treatment | Death due to aspiration pneumonia and multiorgan failure | Metastasized to duodenum as well |
| Glick et al. [ | 49/F | Hypopharynx | Continuous chest pain | Submucosal mass, lesser curvature | Gastric cardia | NR | NR | NA |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMetastasis and carcinoma case studies · Cancer Diagnosis and Treatment · Colorectal and Anal Carcinomas
Introduction
Metastatic cancer mostly occurs via spread through lymphatic drainage and blood supply. Some organs may be more common targets; however, metastases can develop at any site. Metastases to the stomach, specifically, are a fairly rare occurrence, with clinical incidence in autopsy series reporting a rate between 0.2% and 0.7% [1]. The main mechanism is not commonly understood and can be hematogenous, lymphatic, peritoneal dissemination, or direct invasion. The most common primary tumor sites of gastric metastases include breast cancer (27%), lung cancer (23%), and renal cell carcinoma (7%) [2].
Hypopharyngeal squamous cell carcinoma (HSCC) accounts for 6% of all head and neck cancers, with a worldwide incidence from 0.8 to 6 cases per 100,000 [3]. A highly aggressive malignancy, it is associated with increased age, male sex, tobacco abuse, alcohol use, and Caucasian race. While it has significant metastatic potential, spread to the stomach is very unusual, and here we present such a case. In keeping with our aims, we also review investigations on molecular mechanisms in HSCC metastasis and then outline recently reported cases from other primary cancers with gastric metastasis.
Case presentation
A 71-year-old male patient with a history significant for HSCC was admitted to the hospital with melena. Three years ago, he had developed a chronic cough, an uncomfortable feeling in the throat, and swelling in the neck. Imaging revealed a left hypopharyngeal mass that was biopsied and showed invasive, moderately to poorly differentiated squamous cell carcinoma (SCC) that was p16-positive. He was treated with carboplatin, docetaxel, plus pembrolizumab, then transitioned to pembrolizumab alone. In the meantime, he received radiation to a right lung lesion due to progressive metastatic disease. His treatment was complicated by small bowel obstruction requiring resection. Pathology of two resected lesions in the jejunum revealed metastatic moderately differentiated SCC consistent with hypopharyngeal origin. He presented to our hospital with melanotic stool for six days. He was found to have anemia, and hemoglobin had dropped from 9.2 one month prior to 7.4, for which he was transfused two units of packed red blood cells.
Esophagogastroduodenoscopy (EGD) showed a friable, non-bleeding ulcer with central depression on the lesser curvature of the stomach with raised margins concerning for metastatic disease (Figure 1). Biopsies indicated metastatic HSCC in the stomach (Figure 2). The patient did not require endoscopic treatment since the ulcer was not bleeding. He followed up with oncology to determine eligibility for enrollment in clinical trials.
A friable ulcerated lesion with central crater and roll margins on the lesser curvature of the stomach, the mucosal surface is irregular and partially eroded. This endoscopic presentation is consistent with metastatic disease.
H&E-stained section at 20X, with the circle focus demonstrating cohesive nests of atypical squamous epithelial cells infiltrating the lamina propria beneath intact appearing gastric mucosa (stars). Tumor cells show eosinophilic cytoplasm and intracellular bridging consistent with metastatic SCC. H&E: Hematoxylin and eosin; SCC: Squamous cell carcinoma
Discussion
The case presented is distinctive when compared to the other three reported cases of HSCC metastasizing to the stomach. In contrast to our case, these patients either presented with a polypoid mass, a submucosal mass, or disease associated with percutaneous endoscopic gastrostomy (PEG) [4-6]. The case by Abdallah et al. was similar in clinical presentation but was hemodynamically unstable, requiring four units of packed red blood cells and admission to the ICU for close hemodynamic monitoring, highlighting the clinical variability of metastatic disease [6]. On CT imaging, multiple metastatic hepatic lesions and a gastric mass in the greater curvature were observed. The patient was treated with immunotherapy (pembrolizumab) and a palliative chemotherapy regimen [6]. Though also with stage IV hypopharyngeal cancer, this patient had a tracheostomy and PEG, which has its own mechanisms and risk for metastasis [7]. In the case by Wu et al., presentation occurred two years after cancer diagnosis; the initial symptoms two years prior were dysphagia and the presence of a bulging mass on the left upper neck that showed HSCC on biopsy. The patient then presented two years later with hematemesis, for which endoscopy showed two polypoid masses in the stomach and duodenum. The best form of treatment was surgery; however, the patient refused further advanced treatments, including surgery [4]. In the first reported case, published in 1985, a female patient presented with chest pain many months after HSCC treatment [5]. The gastric lesion in this case was a large submucosal mass, confirmed as SCC.
Due to the aggressiveness of HSCC and the higher propensity for late-stage disease at diagnosis, researchers have tried to elucidate molecular markers that are involved in metastasis of this malignancy. The basis for this is that malignant changes involve concordant, detectable changes at the level of gene expression. Moreover, scientific investigations in this realm can help elucidate clinical biomarkers that may aid in earlier identification and possible successful treatment of this often-deadly cancer. Recently, Zhou et al. revealed that the pyruvate kinase M2 (PKM2) gene was more highly expressed in those with lymph node metastasis than those without [8]. Further, patients with high PKM2 expression had a lower five-year survival on Kaplan-Meier analysis. Another study found that high expression of Stathmin1 (STMN1) in HSCC was directly associated with lymphatic vessel invasion [9]. Other investigators evaluated long noncoding RNAs (lncRNAs), such as lymphoid enhancer-binding factor 1 antisense RNA 1 (LEF1-AS1), and found that it supported metastatic spread of HSCC via a microRNA intermediate (miR-221-5p) [10]. Actin-binding proteins (ABPs) are theorized to regulate the actin cytoskeleton of cells, which in turn propels the process of metastasis, as investigated by Kakurina et al. [11]. Specifically, ABPs (e.g., RND3, CAP1, PFN1, etc.) can be involved in initiating metastatic processes such as epithelial-mesenchymal transition (EMT). Matrin3 (circMATR3), a type of circular RNA (circRNA), has also shown promise as a prognostic and therapeutic biomarker in HSCC due to its involvement in cellular proliferation, regulation of apoptosis, and invasion via multiple signaling cascades [12]. Finally, using reverse transcription-quantitative polymerase chain reaction (RT-qPCR) analysis and western blot, a study reported that HCLS1-associated protein X-1 (HAX-1) was overexpressed in HSCC, playing a significant role in metastasis [13]. All of these studies provide potential diagnostic and prognostic biomarkers for metastatic HSCC, with the central aim of improving overall survival.
On the other hand, a review of recent reports of metastatic disease to the stomach highlights the variability of this phenomenon. Breast cancers have previously been shown to exhibit gastric metastases. In a recent report, a patient presented 10 years after her initial cancer diagnosis with symptoms of upper abdominal discomfort and fatigue [14]. An EGD showed scattered polyps and mucosal infiltration involving the antrum, body, and cardia. Through immunohistochemical staining, it was determined that these lesions were intensely estrogen receptor (ER)-positive. The patient was started on endocrine therapy with palbociclib and tamoxifen, and she reached a stable disease course after one year. Others have also reported this tendency for multifocal spread of malignant breast cancer within the stomach [15,16]. Melanoma is notorious for metastasizing anywhere at any time, and this was highlighted in a recent case of an 85-year-old with a history of cutaneous melanoma of the right foot presenting with severe asthenia, severe anemia, and weight loss [17]. Endoscopy found four gastric lesions with central ulceration and blackish areas with a friable consistency, and immunohistochemistry confirmed primary cutaneous melanoma. Another report from a different cutaneous origin by Reise-Filteau et al. presented a 63-year-old female patient with a history of HIV and cutaneous SCC (cSCC) of the left temple [18]. The patient presented with functional decline, ascites, shortness of breath (SOB), and anemia. During the workup for her symptoms, CT scans of the chest showed multiple soft tissue lesions with a polypoid mass arising from the gastric antrum. EGD found a 2 × 2 cm submucosal ulcerated lesion in the gastric antrum and a 5 mm raised lesion in the duodenum, with genomic profiling linking these lesions to the primary cSCC. Palliative care was initiated for this patient due to the extent of her disease and poor prognosis, with her death occurring three weeks after admission.
Renal metastasis to the stomach was recently published by McIllwaine et al. in an 80-year-old female patient who previously underwent nephrectomy and presented with general malaise, weight loss, and acute hematemesis [19]. A 3 cm polypoid lesion on the greater curvature of the stomach was confirmed to be of renal origin. In a 2023 paper, there was a case of prostate cancer that began in a 65-year-old male patient with a prominent family history of cancer [20]. The patient presented nine years after his initial diagnosis of prostate cancer with epigastric discomfort, heartburn, decreased appetite, nausea, and anemia. An endoscopy was performed and found an ulcerated area on the greater curvature of the stomach. Through immunohistochemical staining, it was discovered that the tumor showed high prostate-specific antigen (PSA), indicating prostate metastasis. Radiation therapy was performed with 20 Gy in five fractions, but the patient ultimately declined further treatment and died after nine months of follow-up. Another uncommonly reported primary site is the thyroid, as published by Fuladi et al. [21]. A 72-year-old female patient with a primary diagnosis of anaplastic carcinoma of the left hemithyroid presented with persistent nausea and vomiting during adjuvant radiation therapy that was resistant to treatment with proton pump inhibitors (PPIs). Upper gastrointestinal endoscopy was performed and found seven-eight large polypoid lesions in the stomach (exact location not specified), with biopsy confirming origin from the primary anaplastic thyroid carcinoma. The patient died 2.5 months after presentation due to hemorrhagic shock.
Treatment options for metastatic HSCC are driven by systemic immunotherapy, with the current first line being either pembrolizumab therapy alone or combined with platinum-based chemotherapy, which has demonstrated overall survival benefits compared with the previous chemotherapeutic regimen [22]. Conventional second-line options include taxane-based regimens or cetuximab-containing combinations in patients who have progressed after exposure to platinum-based chemotherapy [23]. Control of tumor-related bleeding can be achieved through endoscopic hemostasis, and short-course radiotherapy is an effective option for local control when bleeding or pain persists [24]. Table 1 summarizes these cases, along with others.
Conclusions
Though metastasis to the stomach can happen in certain cancers, hypopharyngeal cancer does not commonly do so. Review of the literature reveals very few such cases. The case compares and contrasts in various ways with those previously reported, adding significant findings to our current knowledge. Multiple molecular biomarkers have been reported in the pathogenesis of metastatic HSCC, including novel RNAs such as lncRNAs, circRNA, and miRNA. These can serve as future oncological targets with the hope of improving patient outcomes. Current management should focus on treating the underlying disease, which generally entails systemic chemotherapy. Finally, the endoscopist should consider metastatic disease when evaluating malignant stomach ulcers.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Needle tract seeding following endoscopic ultrasound-guided fine-needle aspiration for pancreatic cancer: a report of two cases World J Surg Oncol Matsui T Nishikawa K Yukimoto H 1341720193138296410.1186/s 12957-019-1681-x PMC 6683495 · doi ↗ · pubmed ↗
- 2Metastatic disease in the stomach Gastrointest Tumors Weigt J Malfertheiner P 6164220152667400310.1159/000431304 PMC 4668793 · doi ↗ · pubmed ↗
- 3Hypopharyngeal Cancer Stat Pearls [Internet Escalante D Hohman MH Sanders O Pathak S Treasure Island, USA Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 567720/33620797 · pubmed ↗
- 4Upper gastrointestinal bleeding due to metastatic gastric and duodenal squamous-cell carcinoma from the hypopharynx Endoscopy Wu CS Chen CM Tung SY Chang KY Chen TC 262281996873974710.1055/s-2007-1005442 · doi ↗ · pubmed ↗
- 5Squamous cell metastases to the gastric cardia Gastrointest Radiol Glick SN Teplick SK Levine MS 339344101985405449910.1007/BF 01893126 · doi ↗ · pubmed ↗
- 6Metastatic squamous cell carcinoma from primary hypopharynx source to gastric mucosa presenting as massive gastrointestinal bleeding J Med Cases Abdalla M Saad E Abdalla MS 1001041420233703274010.14740/jmc 4059 PMC 10079363 · doi ↗ · pubmed ↗
- 7Percutaneous endoscopic gastrostomy site metastasis from head and neck squamous cell carcinoma: case series and literature review J Otolaryngol Head Neck Surg Huang AT Georgolios A Espino S Kaplan B Neifeld J Reiter ER 204220132367276110.1186/1916-0216-42-20PMC 3651229 · doi ↗ · pubmed ↗
- 8PKM 2 promotes lymphatic metastasis of hypopharyngeal carcinoma via regulating epithelial-mesenchymal transition: an experimental research Diagn Pathol Zhou X Li Y Pan M 48192024 https://pubmed.ncbi.nlm.nih.gov/38431604/3843160410.1186/s 13000-024-01474-5PMC 10907999 · doi ↗ · pubmed ↗