Epidemiology, clinical treatment and outcomes, susceptibility patterns and genotypic analysis of 214 Nocardia strains from multiple centers in Henan Province
Xiaogai Li, Cailin Liu, Yinyin Hu, Hui Xu, Haijun Li, Jingjing Sun, Xiangyang Chen, Yujuan Meng, Nan Zhang, Gongchang Li, Xiuping Lei, Limin Guo, Juhua Chen, Wanhai Wang

TL;DR
This study analyzed 214 Nocardia strains from Henan Province to understand their spread, treatment outcomes, and resistance patterns.
Contribution
The study provides a comprehensive genotypic and phenotypic analysis of Nocardia strains from multiple hospitals in Henan Province.
Findings
N. cyriacigeorgica was the most commonly isolated species, followed by N. farcinica.
Most strains were susceptible to linezolid and trimethoprim-sulfamethoxazole.
Antibiotic resistance and virulence genes varied significantly among species.
Abstract
This study aimed to investigate the epidemiology, clinical treatment and outcomes, antimicrobial resistance profiles and genotypic analysis of 214 Nocardia strains collected from 9 hospitals in Henan Province spanning 9 years. Through retrospective analysis of hospitalized patients with nocardiosis, the epidemiological characteristics of 214 Nocardia strains were elucidated. These isolates were identified and subjected to the broth microdilution method for the antimicrobial susceptibility profiles, and the resistance and virulence genes were determined using whole-genome sequencing (WGS). Of all strains, 74.8% were collected from lower respiratory tract specimens, and N. cyriacigeorgica was the most commonly isolated species (28%), followed by N. farcinica (24.8%), N. abscessus (7.9%), N. amamiensis (7.9%), N. otitidiscaviarum (7.5%). 93.9% were obtained from in-province patients, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
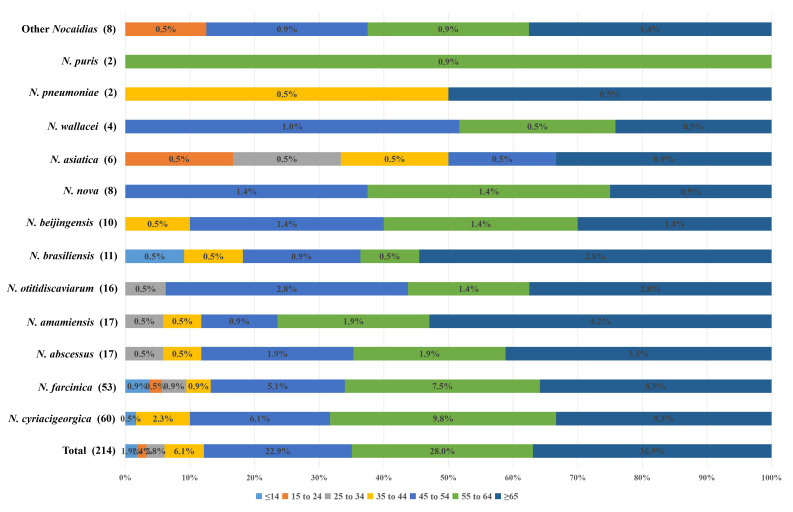 Figure 1
Figure 1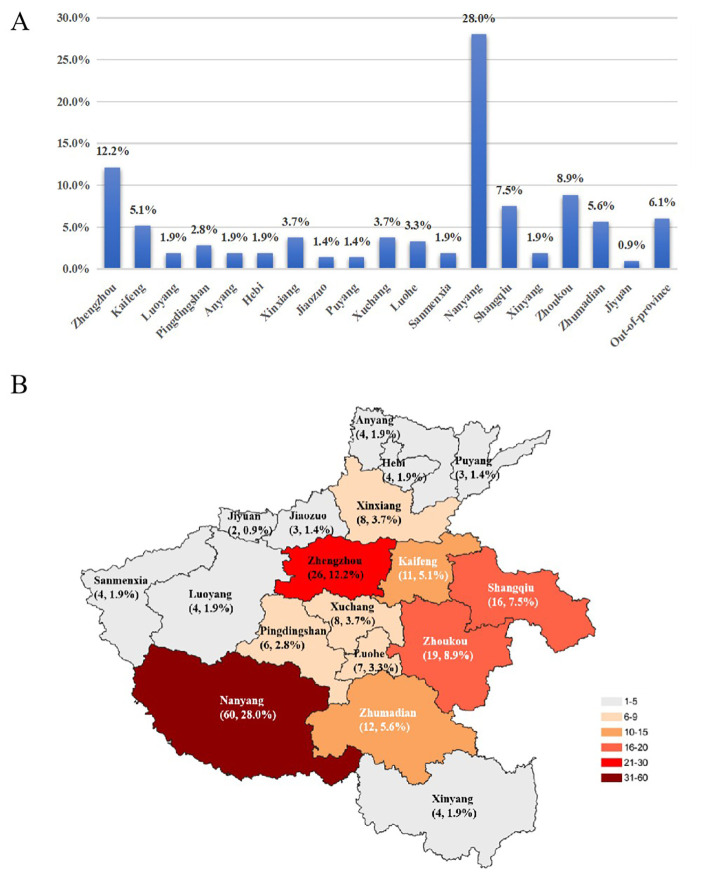 Figure 2
Figure 2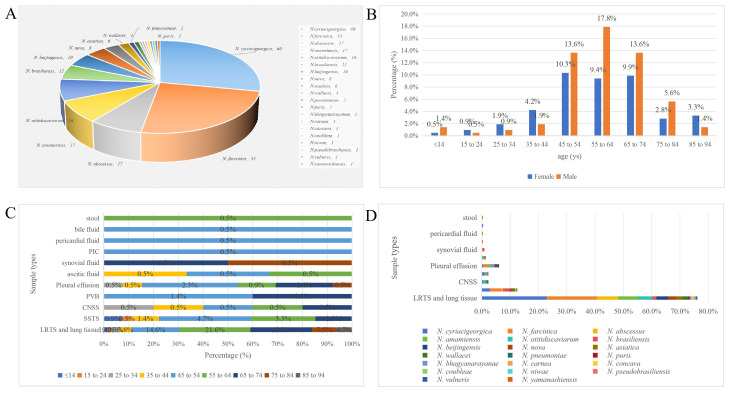 Figure 3
Figure 3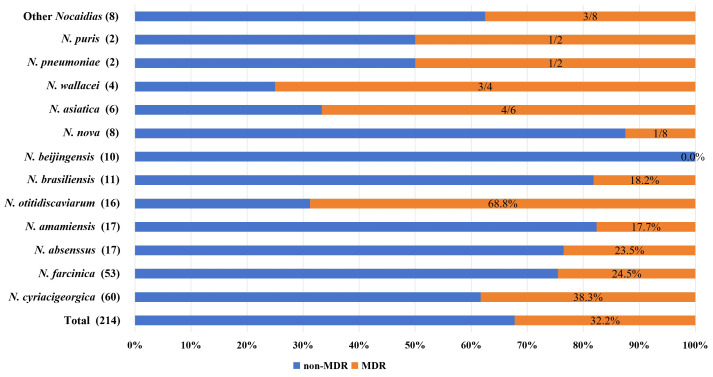 Figure 4
Figure 4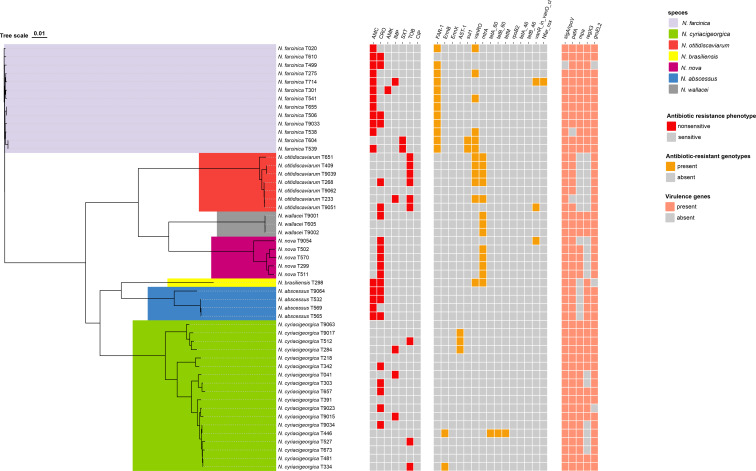 Figure 5
Figure 5| Characteristic | No. of patients (n=213) | Percentage (%) |
|---|---|---|
| Age, year [median (IQR)] | 59 (52, 69) | |
| Male, year [median (IQR)] | 60 (52, 69) | |
| Female, year [median (IQR)] | 57 (49, 70) | |
| Age range (years) | 2-93 | |
| 1 year to14 years | 4 | 1.9% |
| 15 years to 24 years | 3 | 1.4% |
| 25 years to 34 years | 6 | 2.8% |
| 35 years to 44 years | 13 | 6.1% |
| 45 years to 54 years | 51 | 23.0% |
| 55 years to 64 years | 58 | 27.2% |
| 65 years to 74 years | 50 | 23.5% |
| 75 years to 84 years | 18 | 8.5% |
| 85 years to 94 years | 10 | 4.7% |
| Gender | ||
| Male | 121 | 56.8% |
| Female | 92 | 43.2% |
| Occupational distribution | ||
| Farmer | 116 | 54.5% |
| Urban workers | 19 | 8.9% |
| Civil servants | 2 | 0.9% |
| Retirees | 23 | 10.8% |
| Students | 4 | 1.9% |
| Others | 49 | 23.0% |
| Departmental distribution of isolated strains | ||
| Department of Respiratory | 114 | 53.5% |
| ICU | 26 | 12.2% |
| Department of Rheumatology & Immunology | 11 | 5.2% |
| Department of Orthopedics | 9 | 4.2% |
| Department of Geriatrics | 8 | 3.8% |
| Department of Infectious Diseases | 6 | 2.8% |
| Department of Thoracic Surgery | 4 | 1.9% |
| Department of Neurosurgery | 4 | 1.9% |
| Department of Nephrology | 4 | 1.9% |
| Department of Gastroenterology | 3 | 1.4% |
| Department of Dermatology | 3 | 1.4% |
| Department of Cardiology | 3 | 1.4% |
| Department of Pediatrics | 2 | 0.9% |
| Department of Medical Oncology | 2 | 0.9% |
| Department of Hematology | 2 | 0.9% |
| Department of Emergency Medicine | 2 | 0.9% |
| Department of Cardiac Surgery | 2 | 0.9% |
| Others | 8 | 3.8% |
| Infection types and sample sources | ||
| Pulmonary nocardiosis | ||
| Sputum | 98 | 46.0% |
| Bronchoalveolar lavage fluid | 80 | 37.6% |
| Lung tissue | 6 | 2.8% |
| Skin and subcutaneous nocardiosis | ||
| Skin and soft tissue pus | 27 | 12.7% |
| Central nervous system nocardiosis | ||
| Cerebrospinal fluid | 1 | 0.5% |
| Brain abscess | 4 | 1.9% |
| Laboratory-confirmed bloodstream nocardiosis | ||
| Peripheral venous blood | 5 | 2.3% |
| Others | ||
| Pleural effusion | 13 | 6.1% |
| Ascitic fluid | 3 | 1.4% |
| Synovial fluid | 2 | 0.9% |
| Bile fluid | 1 | 0.5% |
| Pericardial fluid | 1 | 0.5% |
| Peripheral intravenous catheter | 1 | 0.5% |
| Stool | 1 | 0.5% |
|
| 53 | 24.9% |
|
| 33 | 15.5% |
|
| 137 | 64.3% |
|
| 98 | 46.0% |
|
| 14 | 6.6% |
|
| 39 | 18.3% |
|
| 13 | 6.1% |
|
| 81 | 38.0% |
| Underlying diseases condition | ||
| Without underlying disease | 11 | 5.2% |
| Acute or Chronic lung disease | 153 | 71.8% |
| Hypertension | 49 | 23.0% |
| Anemia | 38 | 17.8% |
| Diabetes mellitus | 38 | 17.8% |
| Acute or Coronary heart disease | 37 | 17.4% |
| Acute or Chronic liver disease | 36 | 16.9% |
| Autoimmune disease | 35 | 16.4% |
| Acute or Chronic kidney disease | 34 | 16.0% |
| Solid cancer | 24 | 11.3% |
| Skin and soft tissue infection | 24 | 11.3% |
| Acute or Chronic brain disease | 17 | 8.0% |
| Lumbar disc herniation | 6 | 2.8% |
| Hematological cancer | 5 | 2.4% |
| Empyema or Pleurisy | 5 | 2.4% |
| Fracture | 4 | 1.9% |
| Transplant recipient | 2 | 0.9% |
| Characteristic | No. of patients (n=213) | Percentage (%) |
|---|---|---|
| Chest radiograph | ||
| Unilateral lung involvement | 14 | 6.6% |
| Bilateral lung involvement | 178 | 83.6% |
| Pleural involvement | 119 | 55.9% |
| Patchy consolidation | 116 | 54.5% |
| Cloud-like or linear shadows | 108 | 50.7% |
| Nodular shadow | 104 | 48.8% |
| Cavity shadow | 45 | 21.1% |
| Air shadow | 17 | 8.0% |
| Pleural effusion | 93 | 43.7% |
| Mediastinal or Cervical or Supraclavicular lymphadenopathy | 53 | 24.9% |
| Intracranial space-occupying lesion | 3 | 1.4% |
| Clinical manifestations and signs | ||
| Fever | 128 | 60.1% |
| Cough | 153 | 71.8% |
| Expectoration | 148 | 69.5% |
| Hemoptysis | 14 | 6.6% |
| Chest pain | 22 | 10.3% |
| Dry or wet rales | 76 | 35.7% |
| Wheezing | 14 | 6.6% |
| Altered consciousness | 10 | 4.7% |
| Meningeal irritation signs | 1 | 0.5% |
| Subcutaneous abscess | 23 | 10.8% |
| Laboratory data | ||
| WBC increased | 120 | 56.3% |
| Increased proportion of NEU (%) | 137 | 64.3% |
| C- reative protein elevation | 154 | 72.3% |
| PCT elevation | 129 | 60.6% |
| IL-6 elevation | 63 | 29.6% |
| Increased ESR | 105 | 49.3% |
| Elevated ferritin Levels | 42 | 19.7% |
| Hypoproteinemia | 117 | 54.9% |
| Co-infection | ||
| No | 77 | 36.2% |
| Respiratory viruses | 70 | 32.9% |
| HBV or HCV or HIV | 19 | 8.9% |
| MTB | 8 | 3.8% |
| NTM | 2 | 0.9% |
|
| 1 | 0.5% |
| Other bacteria | 75 | 35.2% |
| Filamentous fungi | 42 | 19.7% |
| Candida | 28 | 13.2% |
|
| 19 | 8.9% |
| Drugs | Break -point | Species, no. of strains (%) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|
|
|
|
|
|
|
|
| Other | All | |||
| 60 (28.0) | 53 (24.8) | 17 (7.9) | 17 (7.9) | 16 (7.5) | 11 (5.2) | 10 (4.7) | 8 (3.7) | 6 (2.8) | 4 (2.0) | 2 (0.9) | 2 (0.9) | 8 (3.7) | 214 (100) | |||
| TMP-SMX | S≤2/38, R≥4/76 | MIC50 | <=0.25 | 0.5 | <=0.25 | <=0.25 | 1 | <=0.25 | <=0.25 | <=0.25 | <=0.25 | <=0.25 | <=0.25 | <=0.25 | ||
| MIC90 | 0.5 | 2 | 0.5 | <=0.25 | 1 | 0.5 | <=0.25 | 0.5 | <=0.25 | <=0.25 | 0.5 | 1 | ||||
| Range | <=0.25 to 1 | <=0.25 to >8 | <=0.25 to 2 | <=0.25 to 1 | <=0.25 to 2 | <=0.25 to 0.5 | <=0.25 to <=0.25 | <=0.25 to 1 | <=0.25 to 0.5 | <=0.25 to <=0.25 | <=0.25 to 2 | <=0.25 to >8 | ||||
| S/I/R (%) | 100/0/0 | 100/0/0 | 100/0/0 | 100/0/0 | 100/0/0 | 100/0/0 | 100/0/0 | 100/0/0 | 100/0/0 | 100/0/0 | 100/0/0 | 100/0/0 | 99.1/0/0.9 | |||
| LZD | S≤8 | MIC50 | <=1.0 | 2 | <=1.0 | <=1.0 | <=1.0 | <=1.0 | <=1.0 | <=1.0 | <=1.0 | <=1.0 | <=1.0 | <=1.0 | ||
| MIC90 | 2 | 4 | <=1.0 | <=1.0 | 2 | 2 | <=1.0 | 2 | <=1.0 | <=1.0 | <=1.0 | 2 | ||||
| Range | <=1.0 to 8 | <=1.0 to 4 | <=1.0 to 2 | <=1.0 to <=1.0 | <=1.0 to 2 | <=1.0 to 2 | <=1.0 to <=1.0 | <=1.0 to 2 | <=1.0 to <=1.0 | <=1.0 to <=1.0 | <=1.0 to 2 | <=1.0 to 8 | ||||
| S/NS (%) | 100/0 | 100/0 | 100/0 | 100/0 | 100/0 | 100/0 | 100/0 | 100/0 | 100/0 | 100/0 | 100/0 | 100/0 | 100/0 | 100/0 | ||
| AMC | S≤8/4, R≥32/16 | MIC50 | 32 | 8 | 4 | 16 | >64 | 8 | >64 | >64 | >64 | 16 | 8 | 16 | ||
| MIC90 | 64 | 16 | >64 | 32 | >64 | 8 | >64 | >64 | >64 | 16 | 64 | >64 | ||||
| Range | 4 to >64 | 4 to 32 | <=2.0 to >64 | <=2.0 to 64 | 32 to >64 | 4 to 16 | <=2.0 to >64 | 8 to >64 | >64 to >64 | 8 to 16 | <=2.0 to >64 | <=2.0 to >64 | ||||
| S/I/R (%) | 10/35/55 | 41.2/41.2/17.6 | 0/0/100 | 20/10/70 | 12.5/0/87.5 | 0/0/100 | 25/75/0 | 50/0/50 | 0/50/50 | 50/12.5/37.5 | 40.2/20.6/39.2 | |||||
| CRO | S≤8, R≥64 | MIC50 | 8 | 64 | <=4.0 | <=4.0 | >64 | 8 | <=4.0 | 8 | <=4.0 | >64 | 16 | 8 | ||
| MIC90 | 16 | >64 | <=4.0 | <=4.0 | >64 | 64 | 16 | 32 | <=4.0 | >64 | 64 | >64 | ||||
| Range | <=4.0 to >64 | 8 to >64 | <=4.0 to <=4.0 | <=4.0 to 16 | 32 to >64 | <=4.0 to 64 | <=4.0 to 16 | <=4.0 to >64 | <=4.0 to <=4.0 | 16 to >64 | <=4.0 to >64 | <=4.0 to >64 | ||||
| S/I/R (%) | 71.7/23.3/5.0 | 3.8/32.1/64.1 | 100/0/0 | 94.1/5.9/0 | 0/18.8/81.2 | 54.6/9.1/36.4 | 80/20/0 | 75/12.5/12.5 | 100/0/0 | 100/0/0 | 100/0/0 | 37.5/37.5/25 | 50.9/21/28.1 | |||
| FEP | MIC50 | 8 | >32 | 8 | 8 | >32 | 32 | 8 | 8 | 4 | >32 | 32 | 32 | |||
| MIC90 | 32 | >32 | 16 | 16 | >32 | >32 | 16 | 32 | 8 | >32 | >32 | >32 | ||||
| Range | <=1.0 to >32 | 16 to >32 | <=1.0 to >32 | <=1.0 to >32 | 16 to >32 | 8 to >32 | <=1.0 to 16 | 2 to 32 | <=1.0 to 16 | 8 to >32 | <=1.0 to >32 | <=1.0 to >32 | ||||
| FOX | MIC50 | 128 | 64 | <=4.0 | 8 | >128 | 128 | 8 | 64 | 8 | >128 | 64 | 64 | |||
| MIC90 | >128 | >128 | 8 | 32 | >128 | >128 | 16 | 128 | 8 | >128 | >128 | >128 | ||||
| Range | <=4.0 to >128 | 16 to >128 | <=4.0 to 32 | <=4.0 to 64 | 64 to >128 | 128 to >128 | <=4.0 to 64 | 16 to 128 | <=4.0 to 16 | 64 to >128 | <=4.0 to >128 | <=4.0 to >128 | ||||
| IMP | S≤4, R≥16 | MIC50 | 4 | 4 | 32 | 4 | 64 | >64 | 4 | 8 | <=2.0 | 32 | 8 | 8 | ||
| MIC90 | 16 | 16 | >64 | >64 | >64 | >64 | 64 | >64 | 4 | 32 | >64 | >64 | ||||
| Range | <=2.0 to >64 | <=2.0 to 64 | <=2.0 to >64 | <=2.0 >64 | 8 to >64 | 8 to >64 | <=2.0 to >64 | <=2.0 to >64 | <=2.0 to 32 | 32 to 64 | <=2.0 to >64 | <=2.0 to >64 | ||||
| S/I/R (%) | 56.7/18.3/25 | 54.7/24.5/20.8 | 17.7/11.8/70.5 | 70.6/0/29.4 | 0/6.3/93.7 | 0/18.2/81.8 | 50/10/40 | 83.3/0/16.7 | 0/0/100 | 50/0/50 | 100/0/0 | 37.5/12.5/50 | 45.3/15/39.7 | |||
| AMK | S≤8, R≥16 | MIC50 | <=1.0 | <=1.0 | <=1.0 | <=1.0 | <=1.0 | <=1.0 | <=1.0 | <=1.0 | <=1.0 | <=1.0 | <=1.0 | <=1.0 | ||
| MIC90 | <=1.0 | <=1.0 | <=1.0 | <=1.0 | <=1.0 | <=1.0 | <=1.0 | <=1.0 | <=1.0 | 2 | <=1.0 | <=1.0 | ||||
| Range | <=1.0 to 32 | <=1.0 to 4 | <=1.0 to <=1.0 | <=1.0 to 2 | <=1.0 to <=1.0 | <=1.0 to 2 | <=1.0 to <=1.0 | <=1.0 to <=1.0 | <=1.0 to <=1.0 | <=1.0 to 8 | <=1.0 to 4 | <=1.0 to 32 | ||||
| S/I/R (%) | 100/0/0 | 100/0/0 | 100/0/0 | 100/0/0 | 100/0/0 | 100/0/0 | 100/0/0 | 100/0/0 | 100/0/0 | 100/0/0 | 100/0/0 | 100/0/0 | 99.5/0.5/0 | |||
| TOB | S≤4, R≥16 | MIC50 | <=1.0 | 16 | <=1.0 | <=1.0 | 4 | <=1.0 | <=1.0 | >16 | <=1.0 | >16 | <=1.0 | <=1.0 | ||
| MIC90 | <=1.0 | >16 | 2 | <=1.0 | 16 | <=1.0 | <=1.0 | >16 | <=1.0 | >16 | 2 | >16 | ||||
| Range | <=1.0 to >16 | 8 to >16 | <=1.0 to 8 | <=1.0 to <=1.0 | <=1.0 to >16 | <=1.0 to <=1.0 | <=1.0 to <=1.0 | <=1.0 to >16 | <=1.0 to 2 | <=1.0 to >16 | <=1.0 to 8 | <=1.0 to >16 | ||||
| S/I/R (%) | 0/15.1/84.9 | 88.2/11.8/0 | 100/0/0 | 100/0/0 | 100/0/0 | 12.5/0/87.5 | 100/0/0 | 25/0/75 | 100/0/0 | 100/0/0 | 87.5/12.5/0 | 64.5/7.0/28.5 | ||||
| CLR | S≤2, R≥8 | MIC50 | 8 | >16 | 8 | 0.12 | >16 | >16 | 1 | <=0.06 | 8 | 4 | 2 | 8 | ||
| MIC90 | >16 | >16 | >16 | 4 | >16 | >16 | 2 | 0.12 | >16 | 8 | 16 | >16 | ||||
| Range | 0.25 to >16 | 4 to >16 | <=0.06 to >16 | <=0.06 to >16 | 16 to >16 | 2 to >16 | 0.25 to 4 | <=0.06 to 0.12 | 1 to >16 | 4 to 8 | <=0.06 to >16 | <=0.06 to >16 | ||||
| S/I/R (%) | 33.4/13.3/53.3 | 0/1.9/98.1 | 29.4/5.9/64.7 | 76.5/11.8/11.7 | 0/0/100 | 18.2/0/81.8 | 90/10/0 | 100/0/0 | 33.3/0/66.7 | 0/50/50 | 100/0/0 | 0/0/100 | 50/12.5/37.5 | 30.4/7.5/62.1 | ||
| CIP | S≤1, R≥4 | MIC50 | >4 | 1 | 4 | >4 | 4 | 4 | >4 | >4 | >4 | 1 | 2 | 4 | ||
| MIC90 | >4 | 4 | >4 | >4 | >4 | >4 | >4 | >4 | >4 | 1 | 4 | >4 | ||||
| Range | 0.5 to >4 | 0.25 to 4 | <=0.12 to >4 | 4 to >4 | 2 to >4 | 2 to >4 | 0.5 to >4 | >4 to >4 | >4 to >4 | 0.5 to >4 | 0.25 to >4 | <=0.12 to >4 | ||||
| S/I/R (%) | 5/15/80 | 56.6/30.2/13.2 | 17.7/0/82.3 | 0/0/100 | 0/31.3/68.7 | 0/36.4/63.6 | 20/0/80 | 0/0/100 | 0/0/100 | 0/0/100 | 0/0/100 | 37.5/37.5/25 | 20.6/17.3/62.1 | |||
| MFX | S≤1, R≥4 | MIC50 | 2 | 0.5 | 4 | 8 | 2 | 1 | >8 | 4 | >8 | <=0.25 | 0.5 | 2 | ||
| MIC90 | 4 | 1 | 8 | >8 | 4 | 1 | >8 | 4 | >8 | <=0.25 | 1 | 8 | ||||
| Range | 1 to >8 | <=0.25 to 2 | <=0.25 to >8 | 2 to >8 | 0.5 to 4 | 0.5 to 2 | <=0.25 to >8 | 2 to 4 | >8 to >8 | <=0.25 to 8 | <=0.25 to 4 | <=0.25 to >8 | ||||
| S/I/R (%) | 23.4/38.3/38.3 | 88.7/11.3/0 | 17.7/17.6/64.7 | 0/5.9/94.1 | 25/50/25 | 100/0/0 | 20/0/80 | 0/0/100 | 0/0/100 | 75/0/25 | 0/0/100 | 0/100/0 | 87.5/0/12.5 | 42.1/21/36.9 | ||
| MNO | S≤1, R≥8 | MIC50 | 2 | 2 | <=1.0 | <=1.0 | 2 | 2 | <=1.0 | 4 | <=1.0 | <=1.0 | <=1.0 | 2 | ||
| MIC90 | 4 | 4 | <=1.0 | <=1.0 | 2 | 2 | <=1.0 | 8 | <=1.0 | <=1.0 | 4 | 4 | ||||
| Range | <=1.0 to >8 | <=1.0 to 4 | <=1.0 to 4 | <=1.0 to 2 | <=1.0 to 4 | <=1.0 to 4 | <=1.0 to <=1.0 | <=1.0 to >8 | <=1.0 to <=1.0 | <=1.0 to <=1.0 | <=1.0 to 8 | <=1.0 to >8 | ||||
| S/I/R (%) | 30/63.3/6.7 | 7.6/92.4/0 | 88.2/11.8/0 | 94.1/5.9/0 | 37.5/62.5/0 | 36.4/63.6/0 | 100/0/0 | 12.5/50/37.5 | 100/0/0 | 100/0/0 | 50/50/0 | 100/0/0 | 62.5/25/12.5 | 43/53.3/3.7 | ||
| DOX | S≤1, R≥8 | MIC50 | 2 | 4 | 0.25 | <=0.12 | 1 | 4 | <=0.12 | 8 | <=0.12 | 0.25 | 0.25 | 2 | ||
| MIC90 | 4 | 8 | 0.5 | 0.5 | 2 | 4 | 1 | 16 | 0.5 | 0.25 | 4 | 4 | ||||
| Range | 0.25 to 8 | 1 to 8 | <=0.12 to 2 | <=0.12 to 0.5 | 0.25 to 4 | 1 to 8 | <=0.12 to 1 | 8 to 16 | <=0.12 to 1 | <=0.12 to 0.25 | <=0.12 to 8 | <=0.12 to 16 | ||||
| S/I/R (%) | 31.7/66.7/1.6 | 5.7/79.3/15.0 | 94.1/5.9/0 | 100/0/0 | 50/50/0 | 27.3/63.6/9.1 | 100/0/0 | 0/0/100 | 100/0/0 | 100/0/0 | 100/0/0 | 100/0/0 | 50/37.5/12.5 | 43.9/47.2/8.9 | ||
| TGC | MIC50 | 0.25 | 1 | 0.25 | 0.12 | 0.25 | 0.25 | 0.5 | 2 | 0.25 | 0.25 | 0.5 | 0.5 | |||
| MIC90 | 1 | 2 | 0.5 | 1 | 0.5 | 0.5 | 1 | 4 | 0.5 | 0.25 | 1 | 2 | ||||
| Range | 0.06 to 1 | 0.06 to >4 | 0.06 to 1 | 0.03 to 1 | 0.12 to 0.5 | 0.06 to 0.5 | 0.06 to 1 | 0.25 to 4 | 0.12 to 0.5 | 0.12 to 0.5 | 0.12 to 2 | 0.03 to >4 | ||||
| MDR, XDR, PDR | 38.3, 0, 0 | 24.5, 0, 0 | 23.5, 0, 0 | 17.7, 0, 0 | 68.8, 0, 0 | 18.2, 0, 0 | 0, 0, 0 | 1/8, 0, 0 | 4/6, 0, 0 | 3/4, 0, 0 | 1/2, 0, 0 | 1/2, 0, 0 | 3/8, 0, 0 | 32.2, 0, 0 | ||
| Infection Types (strains) | Species (n) | Treatment | Number | Outcomes |
|---|---|---|---|---|
| Simple pulmonary infection (164) | TMP-SMX monotherapy | 9 | Recovered (8), Failure (1) | |
| TMP-SMX with β-lactam antibiotics | 7 | Recovered (6), Failure (1) | ||
| TMP-SMX with linezolid | 9 | Recovered (8), Failure (1) | ||
| TMP-SMX with Quinolone antibiotics | 1 | Recovered (1) | ||
| Triple Therapy | 6 | Recovered (5), Failure (1) | ||
| Moxifloxacin monotherapy | 5 | Recovered (4), Failure (1) | ||
| IMP/MEM monotherapy | 4 | Recovered (3), Failure (1) | ||
| Other antibiotics | 7 | Recovered (7) | ||
| TMP-SMX monotherapy | 6 | Recovered (6) | ||
| TMP-SMX with β-lactam antibiotics | 6 | Recovered (5), Failure (1) | ||
| TMP-SMX with linezolid | 1 | Recovered (1) | ||
| TMP-SMX with Quinolone antibiotics | 4 | Recovered (3), Failure (1) | ||
| Triple Therapy | 3 | Recovered (2), Failure (1) | ||
| Moxifloxacin monotherapy | 6 | Recovered (6) | ||
| β-lactam antibiotic monotherapy | 4 | Recovered (3), Failure (1) | ||
| Other antibiotics | 9 | Recovered (7), Failure (2) | ||
| TMP-SMX monotherapy | 2 | Recovered (1), Failure (1) | ||
| β-lactam antibiotic monotherapy | 2 | Recovered (2) | ||
| Quinolone antibiotic monotherapy | 1 | Recovered (1) | ||
| linezolid monotherapy | 1 | Recovered (1) | ||
| TMP-SMX with linezolid | 3 | Recovered (1), Failure (2) | ||
| TMP-SMX with β-lactam antibiotics | 3 | Recovered (3) | ||
| Triple Therapy | 2 | Failure (2) | ||
| Other antibiotics | 2 | Recovered (2) | ||
| TMP-SMX monotherapy | 4 | Recovered (4) | ||
| TMP-SMX with β-lactam antibiotics | 1 | Recovered (1) | ||
| TMP-SMX with linezolid | 1 | Failure (1) | ||
| TMP-SMX with Quinolone antibiotics | 2 | Recovered (1), Failure (1) | ||
| β-lactam antibiotic monotherapy | 3 | Recovered (3) | ||
| Other antibiotics | 3 | Recovered (3) | ||
| TMP-SMX monotherapy | 1 | Recovered (1) | ||
| β-lactam antibiotic monotherapy | 1 | Recovered (1) | ||
| Quinolone antibiotic monotherapy | 2 | Recovered (2) | ||
| linezolid monotherapy | 1 | Recovered (1) | ||
| TMP-SMX with linezolid | 1 | Recovered (1) | ||
| TMP-SMX with Quinolone antibiotics | 1 | Recovered (1) | ||
| TMP-SMX with β-lactam antibiotics | 1 | Failure (1) | ||
| Triple Therapy | 2 | Recovered (2) | ||
| Other antibiotics | 3 | Recovered (3) | ||
| TMP-SMX monotherapy | 1 | Recovered (1) | ||
| linezolid monotherapy | 2 | Recovered (2) | ||
| β-lactam antibiotic monotherapy | 2 | Recovered (1), Failure (1) | ||
| TMP-SMX with Quinolone antibiotics | 1 | Recovered (1) | ||
| TMP-SMX with β-lactam antibiotics | 3 | Recovered (2), Failure (1) | ||
| TMP-SMX monotherapy | 1 | Recovered (1) | ||
| IPM with AMK | 1 | Failure (1) | ||
| Triple Therapy | 1 | Recovered (1) | ||
| Other antibiotics | 2 | Recovered (2) | ||
| TMP-SMX with β-lactam antibiotics | 2 | Recovered (2) | ||
| TMP-SMX with linezolid | 1 | Recovered (1) | ||
| Triple Therapy | 2 | Recovered (1), Failure (1) | ||
| linezolid monotherapy | 1 | Recovered (1) | ||
| TMP-SMX with linezolid | 1 | Recovered (1) | ||
| IPM with TGC | 1 | Recovered (1) | ||
| Aminoglycoside with β-lactam antibiotics | 1 | Recovered (1) | ||
| Triple Therapy | 1 | Recovered (1) | ||
| Quinolone antibiotic monotherapy | 1 | Recovered (1) | ||
| Triple Therapy | 1 | Recovered (1) | ||
| β-lactam antibiotic monotherapy | 1 | Recovered (1) | ||
| IPM with TGC | 1 | Recovered (1) | ||
| MOX with linezolid | 1 | Recovered (1) | ||
| TMP-SMX with β-lactam antibiotics | 1 | Recovered (1) | ||
| Aminoglycoside with β-lactam antibiotics | 1 | Recovered (1) | ||
| AMK with MEM | 1 | Recovered (1) | ||
| TMP-SMX with β-lactam antibiotics | 1 | Failure (1) | ||
| β-lactam antibiotic monotherapy | 1 | Recovered (1) | ||
| Simple skin infection (20) | TMP-SMX monotherapy | 1 | Recovered (1) | |
| TMP-SMX with Quinolone antibiotics | 1 | Recovered (1) | ||
| Aminoglycoside with β-lactam antibiotics | 1 | Recovered (1) | ||
| Other antibiotics | 1 | Recovered (1) | ||
| Debridement | 1 | Recovered (1) | ||
| Quinolone antibiotic monotherapy | 1 | Recovered (1) | ||
| TMP-SMX with linezolid | 1 | Recovered (1) | ||
| Other antibiotics | 2 | Recovered (2) | ||
| Debridement | 1 | Recovered (1) | ||
| β-lactam antibiotic monotherapy | 1 | Recovered (1) | ||
| linezolid with LEV | 1 | Recovered (1) | ||
| Triple Therapy | 1 | Recovered (1) | ||
| β-lactam antibiotic monotherapy | 1 | Recovered (1) | ||
| Triple Therapy | 1 | Recovered (1) | ||
| TMP-SMX with β-lactam antibiotics | 1 | Recovered (1) | ||
| Other antibiotics | 1 | Recovered (1) | ||
| Triple Therapy | 1 | Recovered (1) | ||
| Triple Therapy | 1 | Recovered (1) | ||
| Simple intra-abdominal infection (2) | Quinolone antibiotic monotherapy | 1 | Recovered (1) | |
| β-lactam antibiotic monotherapy | 1 | Recovered (1) | ||
| Simple bloodstream infection (1) | LEV with MEM | 1 | Recovered (1) | |
| Pulmonary infection and skin infection (6) | TMP-SMX with Quinolone antibiotics | 1 | Recovered (1) | |
| β-lactam antibiotic monotherapy | 1 | Recovered (1) | ||
| Triple Therapy | 1 | Recovered (1) | ||
| β-lactam antibiotic monotherapy | 1 | Recovered (1) | ||
| TMP-SMX with β-lactam antibiotics | 1 | Recovered (1) | ||
| TMP-SMX with linezolid | 1 | Recovered (1) | ||
| Pulmonary infection and intracranial infection (5) | β-lactam antibiotic monotherapy | 1 | Failure (1) | |
| Triple Therapy | 1 | Failure (1) | ||
| β-lactam antibiotic monotherapy | 1 | Recovered (1) | ||
| MOX with MEM | 1 | Recovered (1) | ||
| Quinolone antibiotic monotherapy | 1 | Failure (1) | ||
| Pulmonary infection and cardiovascular infection (1) | β-lactam antibiotic monotherapy | 1 | Recovered (1) | |
| Pleural infection and intra-abdominal infection (1) | β-lactam antibiotic monotherapy | 1 | Failure (1) | |
| multiple-site infection (2) | TMP-SMX with linezolid | 1 | Recovered (1) | |
| TMP-SMX with linezolid | 1 | Recovered (1) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsActinomycetales infections and treatment · Infectious Disease Case Reports and Treatments · Infectious Diseases and Mycology
Introduction
The genus Nocardia includes ubiquitous environmental saprophytes and the most frequently isolated aerobic actinomycete human pathogen responsible for localized or disseminated infection (Wang et al., 2022; Wang et al., 2023). Infections caused by the Nocardia species are referred to as nocardiosis. It is a rare but life-threatening infection caused by the aerobic, gram-positive, and weakly acid-fast bacteria, moreover, is commonly seen in the lower respiratory tract, skin and soft tissues, and central nervous system (CNS) in both immunocompromised and immunocompetent individuals (Yang J. et al., 2023). The genus Nocardia usually infects hosts through inhalation of the organism and traumatic inoculation into the skin, especially in patients who have had contact with soil or plant materials. Conditions compromising chronic lung disease, including chronic bronchitis, bronchiectasis, bronchial asthma, chronic obstructive disease, pulmonary tuberculosis, etc., chronic kidney disease, and chronic liver disease increase vulnerability. While systemic immunodeficiency, such as diabetes mellitus, Human Immunodeficiency Virus (HIV), systemic corticosteroids, or chemotherapy, further increases the risk of dissemination (Rathish and Zito, 2025). Specifically, hematogenous dissemination is a vital factor that notably increases mortality rates, with amounting to 85% in immunocompromised individuals (Di et al., 2025; Yang et al., 2025).
The timely diagnosis is essential and relies on a high index of suspicion, aided by gram staining, modified acid-fast staining, prolonged culture, and molecular biological techniques such as matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS), polymerase chain reaction or gene sequencing technology. Management of initial therapy includes TMP-SMX as topical and first-line therapy, and LZD considered for use in combination therapy for moderate-to-severe or disseminated nocardiosis (Davidson et al., 2020; Wang et al., 2025). Delayed treatment of Nocardia infections may produce disseminated infections and multi-organ involvement as systemic infections, and may even cause severe complications such as brain abscesses and meningitis. The prognosis depends on the extent of involvement in the patient and the timeliness of intervention.
Ongoing related studies are constantly updating the taxonomy of the genus Nocardia. It’s reported that over 200 Nocardia species have been documented (Di et al., 2025), and about 54 of them have been clearly associated with human infections (Hamdi et al., 2020), and this number may be updated. Clinical data show that the main species causing human Nocardia infections include the N. nova complex, N. abscessus complex, N. otitidiscaviarum, N. farcinica, N. cyriacigeorgica and N. brasiliensis. The distribution of Nocardia species varies geographically, and there are differences in drug susceptibility, carriage of resistance or virulence genes, clinical manifestations, and treatment regimens among different Nocardia species, highlighting a significant gap in both recognition and antimicrobial management of clinical nocardiosis. Fortunately, these differences are increasingly recognized and diagnosed by clinical medical personnel.
In the study, by analyzing the species distribution, the clinical characteristics, treatment and outcomes, the drug susceptibility phenotypes and genotypic characteristics, it is hoped to require a deeper understanding of the species diversity, biological properties and virulence mechanisms of Nocardia isolates in Henan Province and provide a reference for the diagnosis and treatment decision-making of Nocardia infections. What’s more, continuous AST surveillance is essential for characterizing antimicrobial resistance profiles across different regions of our country and for detecting novel resistance traits.
Materials and methods
Ethical approval and consent to participate
This study was approved by the Research and Clinical Trial Ethics Committee of the First Affiliated Hospital of Zhengzhou University (2024-KY-2063). Meanwhile, the study has been registered on National Medical Research Registration and Filing Information System (https://www.medicalresearch.org.cn/), record number:MR-41-24-055644. Our study adhered to the Declaration of Helsinki. Since the study was centered around the clinical epidemiological data, phenotype and gene analysis of Nocardia isolates, and did not involve human participants and strains were collected as part of the routine clinical management of patients. Therefore, the informed consent was not sought, and an informed consent waiver was approved by the Research and Clinical Trial Ethics Committee of the First Affiliated Hospital of Zhengzhou University.
Nocardia infection cases
The study included 213 cases of Nocardia infection that presented from August 2016 to July 2025 at 9 hospitals in Henan Province, China. Nocardia infection was defined as at least two positive sputum cultures or one positive culture from transbronchial or lung biopsy, bronchial lavage fluid, blood, other sterile body fluids, skin and soft tissue infections, or tissue specimens, along with clinical signs and/or radiological evidence of organ involvement (lung, skin and soft tissue, brain and peritoneum) (Yang J. et al., 2023).
Clinical characteristics, treatment, and outcomes
The clinical characteristics of all patients were based on their medical records. Clinical treatment was based on the antibiotic regimens used during hospitalization, and the outcomes were categorized as follows: recovered (clinical symptoms resolved but radiological changes persisted), and failure (no clinical improvement or death following treatment). Information on treatment and outcomes was derived from the medical records.
Collection and identification of strains
The nonrepetitive Nocardia strains collected from each hospital were sent for further examination to the First Affiliated Hospital of Zhengzhou University (Zhengzhou, China). Isolates of Nocardia strains were preserved in brain heart infusion broth supplemented with 25% glycerol at -80°C for subsequent studies. The isolation of bacteria and creation of bacterial culture were performed as detailed previously (Han et al., 2024). Species identification was performed mainly using formic acid extraction method of MALDI-TOF MS (VITEK^®^-MS, IVD database, version 3.0, updated November 2022), while in those strains which were failed to achieve species-level identification by MALDI-TOF MS, final identification would be used through the 16S rRNA sequencing.
DNA extraction, 16S rRNA sequencing
The genomic DNA from each unidentified Nocardia strain was extracted using a TakaRa MiniBEST Bacteria Genomic DNA Extraction kit [TaKaRa Bioengineering Company Limited, Dalian, China], following the manufacturer’s protocols. The extracted DNA samples were sent to Ruibo Xingke Sequencing Company (Beijing, China) for 16S rRNA sequencing to obtain the final identification of Nocardia species. The sequences were compared using the Basic Local Alignment Search Tool algorithm with the database in the National Center for Biotechnology Information GenBank (http://www.ncbi.nlm.nih.gov). Species identification was based on the similarity value of equal to or greater than 99.6% for 16S rRNA sequencing (Yang J. et al., 2023).
Antibiotic susceptibility testing in vitro
The commercial Sensititre RAPMYCO microdilution panels (ThermoFisher Scientific, OH, USA) were used to detect the AST of the Nocardia strains, following the manufacturer’s protocols. The minimum inhibitory concentrations (MICs) of the broth microdilution method were determined for the 15 drugs, including trimethoprim-sulfamethoxazole (TMP-SMX), linezolid (LZD), amoxicillin-clavulanate (AMC), ceftriaxone (CRO), cefepime (FEP), cefoxitin (FOX), imipenem (IPM), amikacin (AMK), tobramycin (TOB), clarithromycin (CLR), ciprofoxacin (CIP), moxifloxacin (MFX), minocycline (MNO), doxycycline (DOX) and tigecycline (TGC). The MIC values of Nocardia strains were interpreted as susceptible (S), intermediate (I), and resistant (R) according to the breakpoint criteria of the Clinical and Laboratory Standards Institute (CLSI, M24S-Ed2) for Nocardia spp (Parrish et al., 2023). Quality control for AST was ensured by employing Escherichia coli ATCC 35218, and Staphylococcus aureus ATCC 29213 as reference strains.
Detection of antibiotic resistance and virulence genes
The presence of antimicrobial resistance and virulence genes were analyzed by WGS in those Nocardia strains different from the acknowledged resistance patterns. WGS (denovo) was performed on a HiSeq sequencer (Illumina) following the manufacturer’s instructions by Hangzhou Jieyi Biotechnology Company Limited (Zhejiang, China). FASTQ files were independently assembled using a de novo SPAdes genome assembler (version 3.13.1).
Statistical analysis
The geographic distribution of Nocardia species was analyzed using Quantum GIS (version 3.40.10), and the epidemiological data and clinical information data were demonstrated using Microsoft Office Excel 2012. The MICs data for each antibiotic were recorded and analyzed using WHONET 5.6 software, and MIC_50_ and MIC_90_ were calculated, defined as the MICs of a given agent that inhibits the grown of 50% and 90% of the isolates, respectively. The data of the acquired resistance and virulence genes were used to analyze the resistance mechanisms of Nocardia through the website (https://www.chiplot.online/tvbot.html).
Results
Demographic characteristics and geographical distribution
A total of 213 cases of nocardiosis were involved. Since two different Nocardia strains were isolated from the same specimen in 1 case, there were 214 Nocardia strains collected. The basic characteristics of 213 nocardiosis cases were summarized in Table 1. The median age of all cases was 59 with ranging from 2 to 93 years old, and there were 36.7% (78 of 213) ≥65 years old and only 1.9% (4 of 213) ≤14 years old, and the majority (187, 87.8%) were older than 45 years, as shown in Table 1 and Figure 1. The gender ratio of male/female was approximately 1.3:1 (121/92). Among these cases, the majority of the patients were farmers (116, 54.5%), and the main department involved was respiratory department (114, 53.5%). Please refer to Table 1 for more details.
The age distribution (%) of 214 Nocardia strains from 2016-2025 in Henan Province.
The most common specimen sources were recovered from the lower respiratory tract with sputum 46.0%, bronchoalverolar lavage fluid (BLF) 37.6%, and lung tissue 2.8%; 12.7% (27 of 213) were recovered from skin wound, pus, abscess, and soft tissue; 6.1% (13 of 213) were recovered from pleural effusion; 2.8% (6 of 213) were recovered from peripheral venous blood, and 2.3% (5 of 213) were recovered from cerebrospinal fluid and brain abscesses. In our cases, there were two or more different specimen types positive for the same Nocardia sp., such as N. cyriacigeorgica might isolate from both BLF and sputum in one case, being analyzed as one strain. The sources of 214 Nocardia strains were summarized in Table 1.
As shown in Figure 2A, among the 214 strains, 93.9% (201 of 214) were obtained from in-province patients and 6.1% (13 of 214) from out-of-province patients. The geographical distribution of the 201 strains from within the province is shown in Figure 2B. Nanyang City (60, 28.0%) was with the highest isolation rate, followed by Zhengzhou (26, 12.2%), Zhoukou (19, 8.9%), Shangqiu (16, 7.5%), Zhumadian (12, 5.6%) with the top 5 of in-province patients. The remaining 13 (6.1%) strains were obtained from patients of Shandong Province (5, 2.3%), Shanxi Province (1, 0.5%), Anhui Province (1, 0.5%), Shanxi Province (2, 0.9%), Heilongjiang Province (1, 0.5%) and the Xinjiang Uyghur Autonomous Region (3, 1.4%), respectively.
Geographica distribution of 214 Nocardia isolates collected from August 2016 to July 2025. (A) All 214 Nocardia isolates collected in 9 laboratories in Henan Province. (B) Geographica distribution of 201 strains collected from patients within Henan Province covering all 18 cities.
Clinical characteristics
Among the nocardiosis patients, 24.9% (53 of 213) had a history of smoking, 15.5% (33 of 213) had a history of alcohol consumption, 46.0% (98 of 213) had invasive procedure, and about 62.4% (133 of 213) had history of immunosuppressant use, steroid use, and chemotherapy. Of the 213 patients, 5.2% (11 of 213) without underlying disease, 94.8% (202 of 213) had at least one underlying disease. Here, acute and chronic pulmonary diseases had the highest proportion (153, 71.8%), and hypertension (49, 23.0%), anemia (38, 17.8%), diabetes mellitus (38, 17.8%), and acute/coronary heart disease (37, 17.4%) were followed. Among these patients with pulmonary nocardiosis, the most common comorbidities included pulmonary infection (119, 55.9%), bronchiectasis (33, 15.5%), chronic obstructive pulmonary disease (COPD) (19, 8.9%), pulmonary fibrosis (12, 5.6%), and emphysema (11,5.2%). The most common clinical manifestations and signs of nocardiosis were cough (153, 71.8%) and expectoration (148, 69.5%), which were followed by fever (128, 60.1%), and further details shown in Table 2.
During the diagnostic process for nocardiosis, 205 patients underwent complete imaging. Through CT scans, it was found that unilateral lung involvement accounted for 6.6% (14 of 213), while bilateral lung involvement was as high as 83.6% (178 of 213), followed by pleural involvement for 55.9% (119 of 213), patchy consolidation for 54.5% (116 of 213), respectively. In the laboratory data, 56.3% (120/213) had elevated white blood cell counts, and 64.3% (137/213) had increased neutrophil proportions. Additionally, the rates of elevated inflammatory factors, including CRP (72.3%), ESR (49.3%), PCT (60.6%) and IL-6 (29.6%), also varied. Besides, 54.9% of patients had hypoproteinemia, and 19.7% involved elevated ferritin levels. Among them, 0.5% (1 of 213) were determined to be Nocardia colonization, and 63.4% cases (135 of 213) co-infected with other pathogens. These cases included 32.9% (70 of 213) of respiratory virus infection and 3.8% (8 of 213) of MTB infection, as summarized in Table 2.
Distribution of Nocardia species
Among the 214 Nocardia isolates, 20 different species were identified, including N. cyriacigeorgica (60, 28.0%), N. farcinica (53, 24.8%), N. abscessus (17, 7.9%), N. amamiensis (17, 7.9%), N. otitidiscaviarum (16, 7.5%), N. brasiliensis (11, 5.1%), N. beijingensis (10, 4.7%), N. nova (8, 3.7%), N. asiatica (6, 2.8%), and N. wallacei (4, 1.9%), respectively. These 10 Nocardia species constituted 94.4% (202 of 214) of all collected isolates. Furthermore, 12 strains for the rare Nocardia species were showed in Figure 3. Here, 3 isolates were misidentified by MALDI-TOF MS as Nocardia, but 16S rRNA sequencing showed 2 strains to be Micromonospora chokoriensis and 1 strain to be Saccharopolyspora hordei, Additionally, we also had provided a comparison analysis of MALDI-TOF MS and 16S rRNA sequencing results for these difficult-to-identify isolates in the Supplementary Material (Supplementary Table S1).
Demographic features of Nocardia isolates and nocardiosis patients. (A) Species distribution of 214 Nocardia isolates. (B) Correlation between ages and genders of the enrolled nocardiosis patients. (C) Correlation between ages and sample types of Nocardia spp. (D) Correlation between the commonly isolated Nocardia species and sample types. LRTS, Lower respiratory tract specimens: SSTS, skin and soft tissue specimens; CNSS, central nervous system specimens; PVB, peripheral venous blood; PIC, peripheral intravenous catheter.
Antibiotic susceptibility profiles
The susceptibility profil to 15 antibiotics for 214 Nocardia strains are summarized in Table 3, showing the MIC_50_, MIC_90_, the range, or S/I/R (%) for each antibiotic. All Nocardia strains were 100% susceptible to LZD, followed by AMK 99.5% (1 of 60 N*. cyriacigeorgica* was AMK-intermediate) and TMP-SMX 99.1% (2 resistant strains belonged to N. farcinica). For β-lactam antibiotics, including AMC, CRO, FEP, FOX and IPM, almost all data demonstrated a poor performance against Nocardia strains, whereas CRO demonstrated 100% susceptibility to N. abscessus, and high heterogeneity between Nocardia species, as shown in Table 3. For TOB, N. amamiensis, N. brasiliensis, and N. beijingensis were 100% sensitive, but the resistance rate for N. farcinica were 84.9%. However, for macrolides, 69.6% Nocardia strains were nonsusceptible to CLR. For quinolone antibiotics, CIP had a high resistance rate 62.2% against all Nocardia species, and the resistance rate to MFX was as high as 36.9%. For tetracyclines, DOX and MNO-resistant Nocardia accounted for 8.9% and 3.7%, respectively, but the intermediate rates were relatively high: 47.2% and 53.3%, respectively. TGC showed low MIC values against different Nocardia species, with its MIC_50_ and MIC_90_ at 0.5 and 2 mg/mL, respectively.
The antibiotic resistance profiles varied within different Nocardia species. The susceptibility rate of N. cyriacigeorgica to AMK (98.3%), TOB (95%), and CRO (71.7%) had decreased. The N. farcinica had a 0% sensitivity rate to CLR and TOB, and showed extensive resistance to β-lactam antibiotics (CRO, 3.8%), quinolones (CIP, 55.6%), and tetracyclines (MNO, 7.6%). The N. amamiensis, as an independent species in Nocardia genus, was fully resistant to quinolones and had a high resistance rate to β-lactam antibiotics. It was worth noting that the resistance phenotypes of N. abscessus and N. beijingensis were analyzed in our study separately, which were studied usually as the N. abscessus complex in other studies (Hamdi et al., 2020; Wang et al., 2022; Yang J. et al., 2023; Han et al., 2024). They are both founded 100% sensitive to TMP-SMX, LZD, and AMK, however, there were significant differences in resistance rates to other antibiotics excluding quinolones. Moreover, except for N. beijingensis, other strains always had poor activity to CLR. Additionally, 8 different rare Nocardia strains with only 1 isolate per specie were combined into the category of “Other Nocardia” to analyse their overall sensitivity rate, as shown in Table 3.
The antimicrobial susceptibility patterns in our study were compared with those provided by CLSI standard M24S-Ed2 (Parrish et al., 2023). In Table 3, a strong correlation between the drug pattern types and Nocardia species identified was illustrated. Nevertheless, some variations were highlighted in red italic bold font of Table 3. Especially the following 7 species of Nocardia: for N. cyriacigeorgica isolates, the sensitivity rate of CRO, TOB and AMK were 71.7%, 95% and 98.3%, respectively, despite the drug pattern indicating sensitivity. And the sensitivity rate of AMC and TMP-SMX in N. farcinica isolates were 77.4% and 96.2%, whose drug patterns were determined to be susceptible. The sensitivity rate of AMC in N. abscessus isolates was only 76.5%, and similarly, the sensitivity rate of AMC in N. brasiliensis was 90.9%. The N. otitidiscaviarum isolates, the sensitivity rate of TOB was 56.3%.
As described by Valdezate S (Valdezate et al., 2017) in the definition of MDR, the detection rates of MDR, XDR, and PDR for Nocardia species with assigned drug patterns varied due to the acquired resistance of the strains. To avoid statistical bias, we showed “n (MDR isolates)/n (total isolates)” as MDR ratio for Nocardia species (n < 10). Table 3 and Figure 4 showed us in descending order as follows: 68.8% for N. otitidiscaviarum, 38.3% for N. cyriacigeorgica, 24.5% for N. farcinica, 23.5% for N. abscessus, 18.2% for N. brasiliensis, 3/4 for N. wallacei and 1/8 for N. nova. For species without a corresponding susceptibility pattern, MDR values ranged from 17.7% for N. amamiensis to 4/6 for N. asiatica. No strains exhibited the extensively XDR and PDR phenotypes.
The proportion of MDR strains of 214 Nocardia isolates.
Detection of antibiotic resistance genes and virulence genes
Given the significant differences in resistance phenotypes between the 7 species of Nocardia (51 strains) mentioned above and the previously published resistance patterns in CLSI standard M24S-Ed2 (Parrish et al., 2023), WGS was used to analyze whether these 51 strains carried antibiotic resistance and virulence genes. The sequences were annotated for gene functions by aligning against the Comprehensive Antibiotic Resistance Database (CARD) antibiotic resistance gene database and the pathogen virulence factor database (VFDB) using the Diamond program (Yang et al., 2025). The gene results were typed by aligning against the PUBMLST database (https://pubmlst.org) using the MLST (version 2.19.0) program.
As shown in Figure 5, 12 antibiotic resistance genes (such as AST-1, FAR-1, sul1, mtrA) were identified. The AST-1 gene was present in N. cyriacigeorgica isolates associated with resistance to AMC, non-sensitivity to CRO, and could also explain the elevated MIC of FEP; the FAR-1 gene was 92.3% present in N. farcinica isolates, which was associated with resistance to AMC, CRO, IPM and the elevated MIC of FEP. The sul1 gene was present in N. farcinica isolates to explain the resistance to TMP-SMX. The mtrA gene was found in N. otitidiscaviarum, N. brasiliensis, N. nova and N. wallacei, and could encode a transcriptional activator of a multidrug efflux pump, and also confer resistance to a variety of antibiotics, including β-lactams, rifampicin, and macrolides. These genes encode a variety of resistance mechanisms, including efflux pumps, β-lactamases, and plasmid-mediated methyltransferases, which confer resistance through antibiotic inactivation, active efflux, and target modification (Supplementary Table S2). No potential resistance genes were detected in the N. abscessus.
Distribution of antibiotic resistance genes and virulence genes of 7 Nocardia species (51 strains). The main associations between drug-resistant phenotypes, resistance genes, and virulence genes are marked in red, orange, and pink, respectively.
A total of 11 virulence genes were detected, including sigA/rpoV, ahpC, plr/gapA, pafA, mpa, regX3, groEL2, etc. These virulence genes were involved in promoting bacterial adhesion, invasion, and survival within macrophages, or in regulating the expression of other virulence factors, or in enhancing bacterial survival and adaptation to environmental stress within host cells through protein degradation mechanisms, thereby enhancing the pathogenicity of the 7 Nocardia species. More details were provided in Supplementary Table S3.
Treatment and outcomes
In the 213 nocardiosis cases, treatment details were available for 202 cases, while 10 cases were missing of the treatment plans, and 1 case was considered to be Nocardia colonization without targeted treatment. Of 202 cases, 53.5% (108 of 202) patients received TMP-SMX monotherapy or with fluoroquinolones or β-lactam antibiotics or LZD multidrug regimen, 85.6% (173 of 202) patients had clinical improvement and 14.4% (29 of 202) failed.
Based on the data presented in Table 4, there were 164 cases with simple pulmonary infection, 14.6% (24 of 164) patients received TMP-SMX monotherapy, 15.2% (25 of 164) received TMP-SMX plus β-lactam antibiotics combination regimen, 11.0% (18 of 164) received TMP-SMX plus LZD combination regimen, 4.9% (8 of 164) received TMP-SMX plus fluoroquinolones antibiotics combination regimen, 11.0% (18 of 164) received triple therapy regimen, and 43.3% (71 of 164) received other antibiotics regimens. Furthermore, 84.8% (139 of 164) patients had clinical improvement and 15.2% (25 of 164) failed.
Of the 20 patients with simple skin and soft tissue infections, 20% (4 0f 20) patients received TMP-SMX monotherapy or with fluoroquinolones or β-lactam antibiotics or LZD combination regimen, 25% (5 of 20) patients received LZD, fluoroquinolones, and β-lactam antibiotics monotherapy or combination regimen, 20% (4 of 20) received triple therapy regimen, and 10% (2 of 20) received debridement. Furthermore, no case was failed.
Discussion
This is the largest study to date in Henan Province, China, that correlates antimicrobial susceptibility with molecular identification and resistance mechanisms of Nocardia species. As expected, in our study, the most common source of positive Nocardia cultures was the lower respiratory tract (76.1% of isolates), following by the skin and soft tissue system (12.7% of isolates), which is basically consistent with the clinical distribution in other large domestic and international Nocardia-related research case series (Mootsikapun et al., 2005; Huang et al., 2019a; Huang et al., 2019b; Lebeaux et al., 2019; Tan et al., 2020; Yeoh et al., 2022; Hershko et al., 2023; Yang J. et al., 2023; Han et al., 2024; Di et al., 2025). However, there are also studies with inconsistent detection rates, such as a study from Taiwan (Lao et al., 2022), which found that cutaneous nocardiosis was the most common (50%) and pulmonary nocardiosis was the second most common clinical form (35.3%). These may be due to differences in the sources of Nocardia - positive specimens caused by geographical and climatic differences, affected population or sampling bias in the studies.
Nocardia species grow slowly and exhibit weak biochemical reactivity. In clinical microbiology laboratories, the identification of these species primarily relies on MALDI-TOF MS. However, molecular sequencing techniques, such as 16S rRNA sequencing, are still required for the identification of certain species (Rodríguez-Temporal et al., 2023; Sharma et al., 2024). In our study, 75.7% (162 of 214) Nocardia isolates were accurately identified to the species level by MALDI-TOF MS. In a study of Body BA, 76% of Nocardia strains were correctly identified to the species using the MALDI-TOF MS, which is comparable to our findings (Body et al., 2018). As shown in Supplementary Table S1, among the 55 strains verified by 16S rRNA, 94.5% (52 of 55) were identified as Nocardia by MALDI-TOF MS with not being correctly differentiated to the species level, but 5.5% (3 of 55) reported as Nocardia were ultimately identified as non-Nocardia species by 16S rRNA sequencing, which was lower than Ölmez S’ findings with the misidentification rate 36.8% (7 of 19) for MS (Ölmez et al., 2023). Exploring the reasons: the agarophilic characteristics or the growth status of some strains such as N. abscessus and N. amamiensis, might lead to agar interference during protein extraction and then result in the incorrect identification by MALDI-TOF MS; N. africana and N. nova, which belong to the Nocardia nova complex with high homology in the 16S rRNA gene sequence, cannot be effectively distinguished by MALDI-TOF MS; for some rare Nocardia species, such as N. carnea, N. yamanashiensis, N. bhagyanarayanae, N. niwae and N. coubleae, the MALDI-TOF MS identification system lacked a more comprehensive identification database, therefore the successful identification was lower.
The 214 clinical Nocardia isolates included 20 different species. In the present study, N. cyriacigeorgica, N. farcinica, N. abscessus and N. amamiensis were the most frequently isolated ranking in the top three, which is somewhat different from the conclusions reported in other related studies (Huang et al., 2019b; Hamdi et al., 2020; Yeoh et al., 2022; Wang et al., 2023; Yang J. et al., 2023; Han et al., 2024). Moreover, N. cyriacigeorgica (30.2%) ranked first in pulmonary nocardiosis, while N. farcinica (33.3%) had the highest isolation rate in cutaneous nocardiosis. Nocardia is sporadically distributed worldwide, and the predominant pathogenic strains reported vary not only among different countries and regions but also among different areas within the same country. This variation may be associated with differences in geographical distribution, population distribution, climate, hospital levels, laboratory culture methods and capabilities, and the identification techniques employed.
Our data showed that the majority of patients were older, with an average age of 59 years, and there was a slight predominance of males, which was consistent with previous literature. In terms of occupational classification, farmers made up the majority (116, 54.5%), and the isolation rate of Nocardia in the Nanyang (60, 28.0%) area was the highest by a wide margin, followed by Zhengzhou (26, 12.15%), with the reasons of these patients, who would be more exposed to contaminated soil, and were more susceptible to environmental Nocardia infections. Furthermore, Nanyang Central Hospital as one of the participating centers, its specimen submission volume was second only followed that from the First Affiliated Hospital of Zhengzhou University. Consequently, the data primarily reflected the distribution of sample sources, thus, a wider range surveillance from other regions of Henan Province would be needed to obtain the true regional distribution. We also noted a steady increase in the number of specimens over the study period, which might indicate an increasing incidence, or more likely, enhanced awareness among clinicians of the need for Nocardia culture, identification, and AST, improved recognition of its pathogenicity, and easier access to these tests.
In this study, approximately 54% of Nocardia infection patients were immunocompetent. Studies (Fujita et al., 2016; Yang J. et al., 2023; Han et al., 2024) stated that immunocompetent patients with COPD or bronchiectasis especially if they were using oral or inhaled corticosteroids, would show a markedly increased risk of developing pulmonary nocardiosis. In chronic pulmonary diseases, corticosteroid therapy is believed to cause lower respiratory tract epithelial damage, which facilitates the colonization of Nocardia (Galar et al., 2021). Diabetes, chronic kidney disease, and cirrhosis are usually considered risk factors for invasive nocardiosis (Peleg et al., 2007). Our study showed that the most common underlying diseases in patients with Nocardia infection were acute or chronic lung disease (153, 71.8%), among these patients, the most common comorbidities, in sequence were pulmonary infection (119, 55.9%), bronchiectasis (33, 15.5%), and COPD (19, 8.9%). Yungang Han (Han et al., 2024) and Jing Yang (Yang J. et al., 2023) all reported that bronchiectasis was the most common comorbidity in patients with pulmonary nocardiosis, occurring in 54.9% and 15.4%, respectively. Yang CH’ study (Yang CH. et al., 2023) indicated that the most common comorbidities were diabetes and COPD, occurring in 30% and 26.7%, respectively. Ott (Ott et al., 2019) expounded that 58.1% of the patients had underlying pulmonary diseases, with COPD being the most common. These results differed from our study.
Patients with pulmonary nocardiosis usually have non - specific clinical manifestations, and most present with symptoms of pulmonary purulent infection. In present study, patients had cough (153, 71.8%), sputum production (148, 69.5%), with nearly half of them producing yellow - purulent sputum. Fever was the next most common symptom (128, 60.1%), all with moderate to high fever, fluctuating between 38.3 - 39.7°C. Chest pain, chest tightness, hemoptysis and fatigue were also common symptoms. On physical examination, the most frequent signs were dry/wet rales (76, 35.9%) and wheezing (14, 6.6%). Moreover, lesions often involved bilateral lungs (178, 83.6%) and were prone to involve the pleura (119, 55.9%). The most common radiological changes were patchy consolidation (116, 54.5%), nodular shadows (104, 48.8%), and various forms of high - density shadows. Because of the variable radiological appearance, it was often difficult to distinguish from tuberculosis, tumors, and other fungal infections, easily prone to misdiagnosis. Approximately one-third of patients will experience dissemination to other organs, with a preference for CNS as well as skin and soft tissues (Xue et al., 2024). Patients with skin involvement usually presented with subcutaneous abscesses (23, 10.8%), and systemic symptoms may not be obvious (Yeoh et al., 2022). Patients with compromised immune function were more susceptible to disseminated infection. Those founding CNS dissemination mainly presented with headache, meningeal irritation signs, and focal neurological deficits, with typical cranial MRI showing ring-enhancement of the lesions (Schlaberg et al., 2014). Since around 40% of cases with cerebral involvement may show asymptomatic, systematic cerebral MRI is mandatory in all nocardiosis cases (Van den Bogaart and Manuel, 2022). In laboratory tests, most patients had varying degrees of increased WBC, neutrophils, and inflammatory markers. Lymphocyte subset analysis can reflect the systemic inflammatory state of the body, also indicating that compromised immune function is a risk factor for nocardiosis (Yetmar et al., 2023a).
For the long-term treatment of Nocardia infections, it is often necessary to switch between various antibiotics or even use combination therapy. TMP-SMX and β-lactam antibiotics such as CRO and IPM are commonly used drugs for nocardiosis. LZD will be required if severe infections. Our study shows that LZD is 100% sensitive to Nocardia species, with the same sensitivity in most previous studies (Valdezate et al., 2017; Hamdi et al., 2020; Toyokawa et al., 2021; Wang et al., 2022; Yang J. et al., 2023; Han et al., 2024). Except for N. farcinica (96.2% sensitive to TMP-SMX), all other Nocardia species were 100% sensitive to TMP-SMX. And the sensitivity rates of N. farcinica to CRO and IPM are 3.8% and 54.7%, respectively, those might be related to the fact that the TMP-SMX resistance gene sul1 and class A β-lactamase gene FAR-1 were only identified in N. farcinica (Valdezate et al., 2015; Che et al., 2022; Nathar et al., 2024; Di et al., 2025). It was noteworthy that different Nocardia isolates carry different resistance genes, and the types and expression levels of resistance genes carried by the same Nocardia species may also vary. This might also explain why other research findings, such as Hamdi’s study, suggested that the sensitivity rate of N. farcinica to CRO is 3% and to IPM is 83% (Hamdi et al., 2020). Church D reported IPM resistance occurred only in strains of the N. farcinica and N. nova complex, while CRO resistance occurred only in the former (Church et al., 2025). Such similar explanations also apply to N. cyriacigeorgica, the sensitivity rate of CRO and IPM was 71.7% and 56.7%, respectively, the class A β-lactamase gene AST-1 was only identified in N. cyriacigeorgica, consistent with previous study (Di et al., 2025). N. abscessus was 100% susceptible to CRO, but its sensitivity rate to IPM was only 17.7%, different from other studies (Schlaberg et al., 2014; Hamdi et al., 2020; Wang et al., 2022; Yang J. et al., 2023; Han et al., 2024), which showed a sensitivity rate of about 95% to CRO and a sensitivity rate of 31% - 64% to IPM. This might be one possible explanation that in our study, N. abscessus, N. beijingensis, and N. asiatica in N. abscessus complex were analyzed separately. Although no related resistance genes were detected in N. abscessus, all isolates carried virulent factors such as ahpC, pafA, sigA/rpoV, regX3 and groEL2 genes, related to stress survival, regulation, and adherence. In our study, N. otitidiscaviarum was 100% resistant to β-lactam antibiotics, CLR, and CIP, while Han Y reported that 100% resistant to β-lactam antibiotics and 20% susceptible to CLR and CIP (Han et al., 2024). Also in other studies, there were around 10% susceptible to β-lactam antibiotics, CLR and CIP (Schlaberg et al., 2014; Hamdi et al., 2020; Wang et al., 2022; Yang J. et al., 2023). For N. brasiliensis, we showed 54.6% the sensitivity rate to CRO, and 0% sensitive to IPM, and other studies showed relatively low sensitivity rates to CRO (among 2% - 49%) and IPM (only 0% - 8%) (Schlaberg et al., 2014; Hamdi et al., 2020; Wang et al., 2022; Yang J. et al., 2023; Han et al., 2024). These differences may be related to the presence of the mtrA gene, which encodes multi-drug resistance efflux pump transcription activator, in N. otitidiscaviarum and N. brasiliensis in our study (Valdezate et al., 2017; Lebeaux et al., 2019). Overall, N. otitidiscaviarum is intrinsically resistant to β-lactam antibiotics. Apart from N. farcinica, other species had higher sensitivity to CRO than to IPM.
Additionally, AMK and TOB separately showed 98.3% and 95% drug susceptibility to N. cyriacigeorgica, but TOB showed the lower sensitivity rates (56.3%) to N. otitidiscaviarum, which also differed from the previously published resistance patterns in the CLSI standard M24S-Ed2. However, we had not found the resistance genes related to aminoglycoside antibiotics, it may be related to virulent factors such as sigA/rpoV, pafA and groEL2 genes, ubiquitously present in these strains. In addition, our study found that 32.2% of Nocardia isolates were resistant to three or more commonly used antibiotics, indicating the widespread presence of MDR. Valdezate S reported the MDR varied from 1% in N. cyriacigeorgica and N. abscessus to 10% in N. brasiliensis, 20% in N. transvalensis, 35% N. farcinica and N. otitidiscaviarum (Valdezate et al., 2017). But Song Z reported 38.5% of Nocardia isolates were resistant to two or more commonly used antibiotics (AMK, CRO, IPM and TMP-SMX) as MDR, with 29.6% for N. farcinica, 45% for N. cyriacigeorgica, and 100% for N. otitidiscaviarum (Song et al., 2025).
Through analysis of resistance genes and virulence genes, we observed a strong correlation between genotype and phenotype. It is reasonable to assume that the differences in the resistance phenotypes of Nocardia among different countries or regions are not only related to the isolated areas and the strains number included in the study, also suggest that the differences in resistance and virulence of Nocardia isolates between studies, which in turn may account for the different outcomes (Yetmar et al., 2023b), and meaning that the resistance transmission mechanisms of Nocardia are worthy of further attention. These findings provide key insights into the different resistance patterns and genotypes of Nocardia strains, thereby emphasizing the importance of continuous genomic surveillance and personalized treatment for different nocardiosis. Nevertheless, the resistance observed in some strains lacking known resistance determinants indicates the presence of uncharacterized mechanisms that require further investigation.
Nocardiosis usually requires long - term treatment, which is often associated with significant toxicity and drug - drug interactions. Moreover, most medical institutions have difficulties in obtaining AST results, which means that the antibiotic management of nocardiosis requires clinicians to choose empirical treatment based on the severity of the infection and local epidemiology (Besteiro et al., 2023). In cases of non - severe pulmonary disease or primary cutaneous nocardiosis, TMP-SMX monotherapy is recommended by many authors (Restrepo and Clark, 2019; Margalit et al., 2021). In severe disease or CNS infection, combination therapy with at least two drugs is recommended to ensure that at least one drug is effective, or LZD monotherapy is also a good choice, and the initial multi-drug regimen usually includes IPM, AMK and TMP-SMX (Restrepo and Clark, 2019). In our study, for simple pulmonary nocardiosis, about 96% (24 of 25) received TMP-SMX monotherapy with a success rate of 91.7% (22 of 24). About 92.1% (81 of 88) received combination therapy based on TMP-SMX with a success rate of 80.3% (65 of 81). For simple cutaneous and soft - tissue nocardiosis, the success rate was 100%, regardless of TMP-SMX monotherapy, combination therapy based on TMP-SMX or debridement used. In cases of pulmonary nocardiosis combined with two or multiple-site infections, even after aggressive clinical treatment, 26.7% failure of patients still experienced, which might be due to the severity and complexity of the patients’ underlying diseases.
But intolerance to TMP-SMX will pose a big challenge to treatment. A case of N. farcinica causing brain abscess had shown that alternative regimen -IPM, AMK, AMC and MNO - combination could achieve sustained remission. Individualized treatment based on AST and patient factors is crucial (Hong et al., 2025). Saksena R reported two cases of fatal pulmonary infections caused by N. otitidiscaviarum in elderly patients, both of whom were empirically treated with TMP-SMX but died on the 2th and 5th days after admission, respectively. However, their AST showed resistance to TMP-SMX, AMC, and IPM (Saksena et al., 2020). We support this conclusion that pulmonary nocardiosis, cutaneous and soft-tissue infections, and treatment with TMP-SMX are independently associated with 90-day all-cause mortality (Peleg et al., 2007).
Our study is limited by several factors. First, the lack of representation of all species within the Nocardia genus, and the number of some Nocardia species were insufficient, thus their results were not representative. Second, the majority of the isolates were concentrated in several cities in Henan Province, therefore, the observed disparity in strains distribution were more likely attributable to submission bias, so it could not reflect the true regional epidemiological characteristics. Correspondingly, a wider-range surveillance program should be further developed. Third, the clinical outcome analysis was purely descriptive, accordingly, no causal conclusions regarding treatment efficacy could be drawn. Finally, WGS had been performed only on some strains whose resistance patterns were inconsistent with known resistance profiles. It is necessary to expand the number of strains to detect the prevalence of the resistance determinants of Nocardia as a whole or individual species and analysis their correlation with resistance phenotypes, meanwhile, the bioinformatic analysis will be needed to extensively illustrate phylogeny and determination of antimicrobial resistance genes and mutations.
In conclusion, the present study is multicenter retrospective study with 214 Nocardia strains covering 9 years and 9 different public hospitals in Henan Province. We reported not only the clinical features and epidemiological characteristics of nocardiosis but also the most frequent and susceptibility patterns of Nocardia species. We also elaborated the susceptibility patterns of clinical therapeutic drugs used for this infection. These findings suggest the need to understand the Nocardia microbiology better so that clinical treatment methods can be optimized to prevent unfavorable outcomes. Moreover, the looming threat posed by MDR Nocardia isolates and resistance mechanism, as well as the potential for resistance transmission should be noted, which will help to identify the key drug targets for combating MDR Nocardia in the future. Nevertheless, the AST methods must be standardized. Methodological challenges (e.g., preparation and treatment of bacterial suspensions, inoculum consistency, and interpretation of cutoffs) and growth characteristics of Nocardia appear to be responsible for limited reproducibility of broth microdilution, especially for some drugorganism combinations (Schlaberg et al., 2014). Likewise, AST in vitro should provide to clinical patients as much as possible, contributing an effective basis for the clinical management of nocardiosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Besteiro B. Coutinho D. Fragoso J. Figueiredo C. Nunes S. Azevedo C. . (2023). Nocardiosis: a single-center experience and literature review. Braz. J. Infect. Dis. 27, 102806. doi: 10.1016/j.bjid.2023.102806, PMID: 37802128 PMC 10582834 · doi ↗ · pubmed ↗
- 2Body B. A. Beard M. A. Slechta E. S. Hanson K. E. Barker A. P. Babady N. E. . (2018). Evaluation of the vitek MS v 3.0 matrix-assisted laser desorption ionization-time of flight mass spectrometry system for identification of Mycobacterium and Nocardia species. J. Clin. Microbiol. 56, e 00237–e 00218. doi: 10.1128/JCM.00237-18, PMID: 29643203 PMC 5971548 · doi ↗ · pubmed ↗
- 3Che Y. Xu S. Kang Y. Liu X. Yue Y. Han L. . (2022). Complete genome sequencing of transposon-mediated sulfamethoxazole resistance encoded by the Sul 1 gene in multidrug-resistant Nocardia farcinica SZ 1509. J. Glob. Antimicrob. Resist. 30, 60–65. doi: 10.1016/j.jgar.2022.03.004, PMID: 35283335 · doi ↗ · pubmed ↗
- 4Church D. Peirano G. Ugarte-Torres A. Naugler C. (2025). Population-based microbiological characterization of Nocardia strains causing invasive infections during a multiyear period in a large Canadian healthcare region. Microbiol. Spectr. 13, e 0091425. doi: 10.1128/spectrum.00914-25, PMID: 40621909 PMC 12323336 · doi ↗ · pubmed ↗
- 5Davidson N. Grigg M. J. Mcguinness S. L. Baird R. J. Anstey N. M. (2020). Safety and outcomes of linezolid use for Nocardiosis. Open Forum Infect. Dis. 7, ofaa 090. doi: 10.1093/ofid/ofaa 090, PMID: 32258209 PMC 7112726 · doi ↗ · pubmed ↗
- 6Di L. Xu A. Li Y. Gu C. Xu H. Xia X. (2025). Genomic diversity of Nocardia cyriacigeorgica and Nocardia farcinica infections. Microb. Pathog. 205, 107602. doi: 10.1016/j.micpath.2025.107602, PMID: 40280503 · doi ↗ · pubmed ↗
- 7Fujita T. Ikari J. Watanabe A. Tatsumi K. (2016). Clinical characteristics of pulmonary nocardiosis in immunocompetent patients. J. Infect. Chemother. 22, 738–743. doi: 10.1016/j.jiac.2016.08.004, PMID: 27615155 · doi ↗ · pubmed ↗
- 8Galar A. Martín-Rabadán P. Marín M. Cercenado E. Sánchez-Carrillo C. Valerio M. . (2021). Revisiting nocardiosis at a tertiary care institution: any change in recent years? Int. J. Infect. Dis. 102, 446–454. doi: 10.1016/j.ijid.2020.10.087, PMID: 33157288 · doi ↗ · pubmed ↗