Redefining evidence for teprotumumab in thyroid eye disease: an updated meta-analysis of efficacy and safety
Rongjing Song, Wei Zhao, Shasha Li, Xiaofang Niu, Jing Guo, Xiuying Zhang, Xiaohong Zhang, Linong Ji

TL;DR
This study confirms that teprotumumab is effective in treating thyroid eye disease, significantly improving symptoms like eye bulging and quality of life, though it may cause side effects like high blood sugar and hearing issues.
Contribution
The paper provides an updated meta-analysis consolidating the efficacy and safety of teprotumumab in thyroid eye disease through a comprehensive synthesis of randomized trials.
Findings
Teprotumumab significantly improves proptosis, diplopia, disease activity, and quality of life in thyroid eye disease.
Common side effects include hyperglycemia, muscle spasms, dry skin, and hearing impairment.
The findings support teprotumumab as a pivotal treatment option with a balanced risk-benefit profile.
Abstract
Thyroid eye disease (TED) is a sight-threatening autoimmune disorder with limited effective therapies. Teprotumumab, an insulin-like growth factor-1 receptor inhibitor, has emerged as a promising treatment. However, a comprehensive synthesis of its efficacy and safety across randomized trials remains limited. A systematic review and meta-analysis of randomized controlled trials (RCTs) comparing teprotumumab with placebo in TED was conducted. Primary outcomes included proptosis response, overall response, change in proptosis, diplopia response, achievement of a Clinical Activity Score (CAS) ≤1, changes in Graves’ ophthalmopathy–specific quality-of-life questionnaire (GO-QOL) scores and safety outcomes. Pooled risk ratios (RRs) and mean differences (MDs) with 95% confidence intervals (CIs) were calculated using random-effects models. Seven RCTs involving 438 participants were included.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
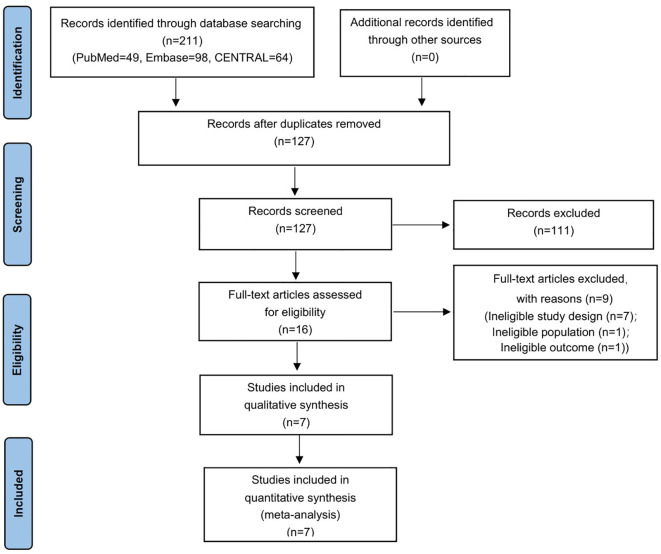 Figure 1
Figure 1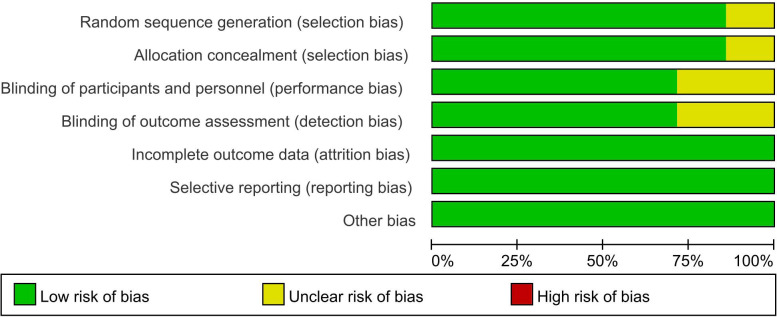 Figure 2
Figure 2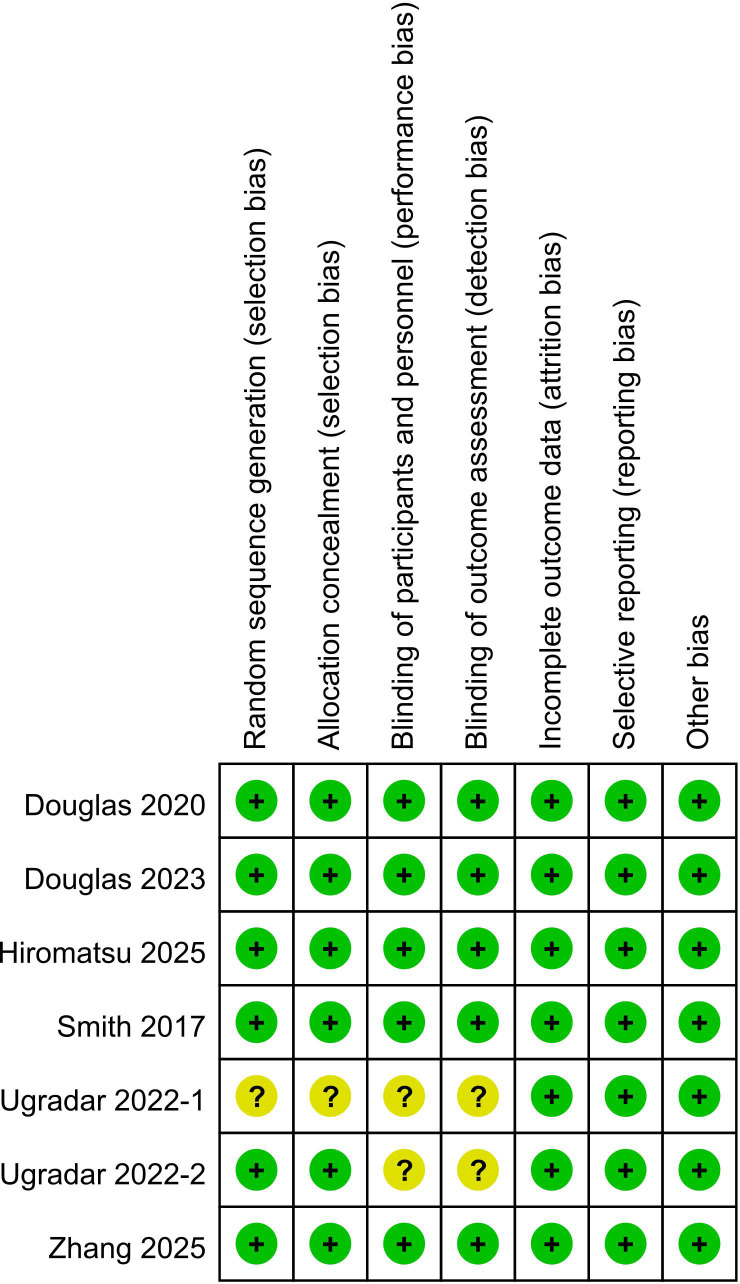 Figure 3
Figure 3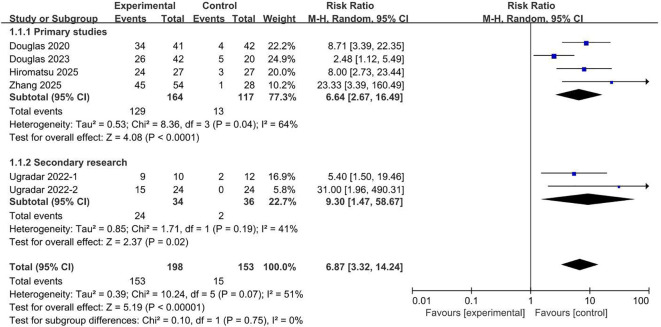 Figure 4
Figure 4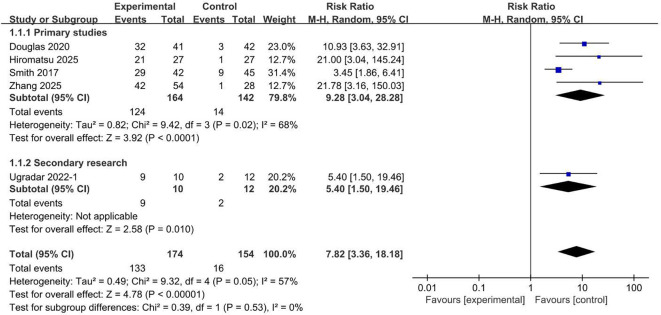 Figure 5
Figure 5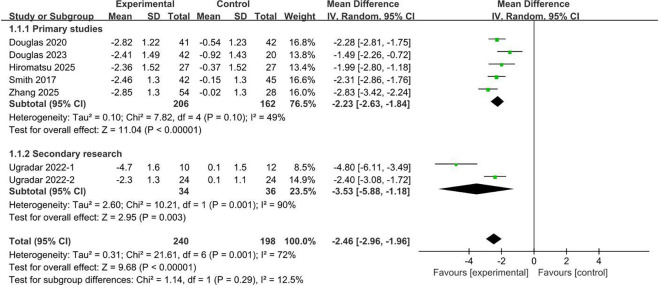 Figure 6
Figure 6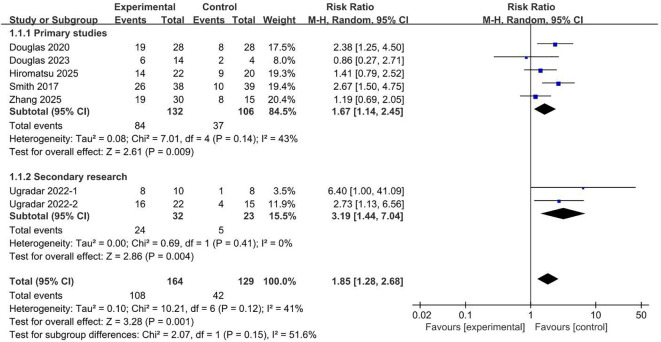 Figure 7
Figure 7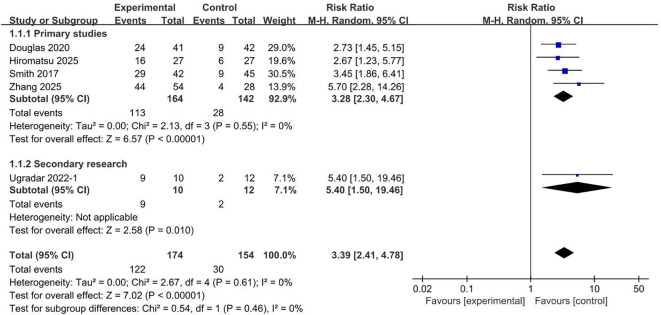 Figure 8
Figure 8 Figure 9
Figure 9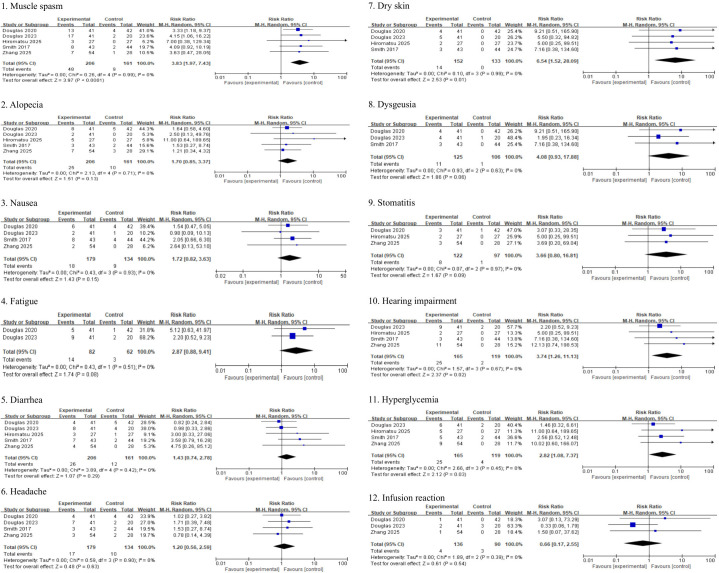 Figure 10
Figure 10| First author/publication year | Study design | Single vs multicenter | Country | Treatment groups (patients, n) | Inclusion criteria | Baseline characteristics (Teprotumumab/placebo) | Interventions | Follow-up duration (weeks) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age range (y) | CAS | Age (y) | Female (n) | Smokers (n) | Duration of GO (months) | Baseline proptosis (mm) | Diplopia at baseline (n) | |||||||
| Smith et al, 2017 ( | RCT | multicenter | Germany, Italy, United | Teprotumumab (42) | 18-75 | ≥4/7 | 52/54 | 28/36 | 11/18 | 10.7/10.8 | 23.4/23.1 | 38/31 | Eight infusions of teprotumumab* | 24 |
| Douglas et al, 2020 ( | RCT | multicenter | Germany, Italy, USA | Teprotumumab (41) | 18-80 | ≥4/7 | 52/49 | 29/31 | 9/8 | 6.2/6.4 | 22.6/23.2 | 28/28 | Eight infusions of teprotumumab* | 24 |
| Hiromatsu et al, 2025 ( | RCT | multicenter | Japan | Teprotumumab (27) | 20-80 | ≥3/7 | 47/50 | 18/20 | 4/4 | 4.2/5.2 | 21.1/20.4 | 22/20 | Eight infusions of teprotumumab* | 24 |
| Douglas et al, 2023 ( | RCT | multicenter | USA | Teprotumumab (42) | ≥18 | ≤1/7 | 49/49 | 32/18 | 6/2 | 64.8/61.2 | 24.6/24.0 | 14/4 | Eight infusions of teprotumumab* | 24 |
| Ugradar et al, 2022–1 ( | RCT | multicenter | Germany, Italy, United | Teprotumumab (10) | 18-80 | >3/7 | 50/59 | 6/10 | 2/4 | 5.8/6.0 | 24.2/22.8 | 10/8 | Eight infusions of teprotumumab* | 24 |
| Ugradar et al, 2022–2 ( | RCT | multicenter | Germany, Italy, United | Teprotumumab (24) | 18-80 | ≥4/7 | 49/50 | 14/14 | 6/4 | 6.1/6.4 | 22.2/22.7 | 22/15 | Eight infusions of teprotumumab* | 24 |
| Zhang et al, 2025 ( | RCT | multicenter | China | Teprotumumab (54) | 18-80 | ≥3/7 | 40/39 | 36/20 | 11/5 | 3.9/3.4 | 20.5/20.4 | 30/15 | Eight infusions of teprotumumab* | 24 |
| Outcomes | No. of studies | No. of patients in teprotumumab group | No. of patients in control group | Mean difference (95% Cl) | Relative risk (95% Cl) | P value | I2 value |
|---|---|---|---|---|---|---|---|
| Proptosis Response | 5 | 156 | 133 | – | 8.91 [5.00, 15.86] | <0.00001 | 0% |
| Diplopia Response | 6 | 150 | 125 | – | 1.97 [1.36, 2.86] | 0.0004 | 41% |
| Change in proptosis from baseline | 6 | 198 | 178 | -2.60 [-3.10, -2.10] | – | <0.00001 | 68% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOphthalmology and Eye Disorders · Ocular Surface and Contact Lens · Ophthalmology and Visual Impairment Studies
Introduction
Thyroid eye disease (TED), also known as Graves’ orbitopathy, is an autoimmune inflammatory disorder of the orbit that is both disfiguring and potentially sight-threatening. It represents the most common orbital disease in adults, with an estimated annual incidence of 16 per 100,000 women and 3 per 100,000 men (1). The disease involves overexpression of insulin-like growth factor 1 receptor (IGF-IR) on orbital fibroblasts and immune cells, with synergistic signaling between IGF-IR and the thyrotropin receptor driving orbital inflammation, fibroblast proliferation, and tissue remodeling (2, 3). These processes lead to proptosis, eyelid retraction, diplopia, and, in severe cases, optic neuropathy and corneal damage, profoundly affecting patients’ quality of life and psychosocial well-being (4). Current first-line therapy for active, moderate-to-severe TED is intravenous methylprednisolone, administered either as monotherapy or, in selected cases, in combination with other immunosuppressive agents. However, their efficacy–particularly for proptosis and diplopia–remains limited, and treatment is frequently complicated by adverse effects and high relapse rates (5, 6). These challenges highlight an unmet need for targeted and effective therapies.
The elucidation of the central role of IGF-IR in TED pathogenesis has paved the way for novel biologic therapies. Teprotumumab, a fully human monoclonal antibody against IGF-IR, represents a major breakthrough in TED treatment. By blocking IGF-IR signaling, it disrupts the inflammatory and pro-fibrotic cascades (3, 7). Early randomized controlled trials (RCTs) demonstrated remarkable efficacy of teprotumumab compared with placebo, showing significantly higher proptosis response rates (≥ 2 mm reduction), greater reductions in Clinical Activity Score (CAS), and substantial improvements in diplopia and Graves’ ophthalmopathy-specific quality-of-life (GO-QOL) scores (8, 9). Based on these pivotal findings, teprotumumab received approval from the U.S. Food and Drug Administration and has been incorporated into international guidelines for the treatment of active TED (10). More recently, trials conducted in Asian populations using an analogous IGF-IR inhibitor (IBI311) have confirmed comparable benefits, with rapid and clinically meaningful reductions in proptosis and disease activity (11, 12).
Despite these compelling results, the broader evidence base for teprotumumab continues to evolve, and several uncertainties remain. While overall efficacy is robust, the magnitude of improvement in diplopia has not been uniformly consistent across all patient subgroups or subsequent trials (12). Furthermore, although the safety profile appears acceptable, emerging post-marketing data have highlighted adverse events of concern, including hearing impairment, hyperglycemia, and muscle spasms (13–16). The publication of new RCTs from diverse ethnic populations and the availability of extended follow-up data provide an opportunity to re-evaluate the totality of evidence (11, 12). Accordingly, we conducted a systematic review and meta-analysis to assess the efficacy and safety of teprotumumab across all available high-quality RCTs, aiming to provide an updated, quantitative synthesis to guide clinical practice and future guideline development in the management of TED.
Materials and methods
This meta-analysis was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline. The corresponding PRISMA flow diagram is shown in Figure 1.
Study selection flowchart.
Inclusion and exclusion criteria
Studies were eligible for inclusion if they met the following criteria: 1) participants were diagnosed with TED; 2) the intervention group received eight infusions of teprotumumab (10 mg/kg for the first infusion and 20 mg/kg for each of the remaining seven infusions) administered once every three weeks; 3) primary and secondary end points reported in the trials included proptosis response rate (defined as a reduction in proptosis of ≥2 mm from baseline at week 24), overall response rate (defined as a composite of a ≥ 2 mm reduction in proptosis and ≥2-point reduction in CAS), change in proptosis from the baseline, diplopia response rate (defined as a reduction in diplopia of ≥1 grade from baseline according to the Gorman subjective diplopia score at week 24) (2) among patients with diplopia at baseline, the proportion of subjects achieving a CAS of 0/1 at week 24, change in GO-QOL score from baseline; 4) the study design was a randomized control trial; 5) the language used for the study was either English or Chinese; and 6) the full text was available online. Retrospective cohort studies, systematic reviews, case reports, studies without human data, conference abstracts and single-arm trials were excluded.
Literature search and study selection
A systematic literature search was conducted in PubMed, EMBASE, and the Cochrane Central Register of Controlled Trials (CENTRAL) from database inception to October 2025. The search strategy combined the following key terms: thyroid eye disease, thyroid-associated ophthalmopathy, Graves’ orbitopathy, teprotumumab, and randomized controlled trial. Additional relevant studies were identified through manual searches of Google Scholar and other sources. The detailed search strategy is provided in Supplementary Table S1. Study selection was performed independently by two investigators according to the predefined eligibility criteria. Discrepancies were resolved by discussion and, when necessary, adjudicated by a third reviewer.
Assessment of risk of bias and data collection
Two reviewers independently assessed the methodological quality of each included study using the risk of bias tool outlined in the Cochrane Handbook for Systematic Reviews of Interventions. The following domains were evaluated: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, completeness of outcome data, selective reporting, and other potential sources of bias. Each domain was classified as having a low, high, or unclear risk of bias, and an overall judgment was summarized across domains. Data regarding baseline characteristics and all relevant outcomes were extracted in accordance with the predefined criteria. Any discrepancies between reviewers were resolved through consensus discussion.
Statistical analysis
Statistical analyses were performed using Review Manager (version 5.3). Data were synthesized according to outcome type. Dichotomous outcomes were reported as risk ratios (RRs) with 95% confidence intervals (CIs), and continuous outcomes were reported as mean differences (MDs) with 95% CIs. The inverse variance method was applied for continuous outcomes, and the Mantel–Haenszel method for dichotomous outcomes. Heterogeneity among studies was assessed using the I² statistic, with values > 50% indicating substantial heterogeneity. A random-effects model was used for all pooled analyses. A two-sided p-value < 0.05 was considered statistically significant.
Results
Literature search and study selection
The detailed search strategy is presented in the Supplementary Table S1, and the study selection process is summarized in Figure 1. A total of 211 studies were identified through database searches (PubMed = 49, EMBASE = 98, and CENTRAL = 64) with no additional studies retrieved from other sources. After removal of duplicates, 127 unique records were screened by title and abstract, of which 111 were excluded. Sixteen full-text articles were subsequently assessed for eligibility, and nine were excluded with documented reasons (ineligible study design, ineligible population or ineligible outcome). Ultimately, seven randomized controlled trials met the inclusion criteria and were included in the meta-analysis, comprising 438 participants in total (teprotumumab, n = 240; placebo, n = 198) (2, 6, 8, 11, 12, 17, 18).
Study characteristics and data extraction
The characteristics of the studies included in this meta-analysis are summarized in Table 1. The publications ranged from 2017 to 2025, and all were multicenter randomized controlled trials conducted across Asia, Europe, and the Americas. Sample sizes per study ranged from 10 to 54 participants per treatment arm. The enrolled populations consisted predominantly of adults, with no significant sex differences reported. Most studies included patients with a CAS greater than 3 at baseline except for the trial by Douglas et al. (6). The duration of TED ranged from 3.4 to 64.8 months, and mean baseline proptosis ranged between 20.4 mm and 24.6 mm. In most trials, the proportion of patients presenting with baseline diplopia was slightly higher in the teprotumumab group than in the placebo group. All studies administered eight intravenous infusions of teprotumumab in the intervention group and reported a follow-up period of 24 weeks. Relevant data were extracted and categorized according to the efficacy and safety profiles of teprotumumab. Efficacy outcomes comprised proptosis response rate, overall response rate, change in proptosis from baseline (mm), diplopia response rate, the proportion of patients achieving a CAS of 0 or 1, change in GO-QOL score from baseline. Safety outcomes were obtained from the included studies, defined as: ‘Muscle spasm’, ‘Alopecia’, ‘Nausea’, ‘Fatigue’, ‘Diarrhea’, ‘Headache’, ‘Dry skin’, ‘Dysgeusia’, ‘Stomatitis’ (or ‘Noninfective gingivitis’), ‘Hearing impairment’ (or ‘Hypoacusis’), ‘Hyperglycemia’ (or ‘Diabetes’, ‘Diabetes mellitus’), ‘Infusion reaction’.
Additionally, for change in proptosis from baseline (2, 6, 8, 12) and change in GO-QOL score from baseline (2, 12), the outcomes were presented as mean ± standard error (SEM), the formula Standard Deviation (SD) = SEM × √N was used to obtain the SD. In Hiromatsu et al. (11), change in proptosis from baseline and change in GO-QOL score from baseline were presented as 95% CI, and the corresponding SD was calculated using the built-in calculator in Review Manager (version 5.3) by entering the mean, sample size, and 95% CI. For dichotomous outcomes, the proportion of subjects with a CAS ≤ 1 was reported as percentages in Smith et al. (8), and we obtained the corresponding numerical data through simple multiplication. Two researchers independently perform data extraction and conversion, with any disagreements resolved through discussion or consultation with a third researcher.
Assessment of risk of bias
A methodological quality assessment was conducted for all seven included studies. Figure 2 depicts the risk of bias for each individual studies comparing teprotumumab with placebo, and Figure 3 presents a summary of these findings. Six studies explicitly reported adequate methods for random sequence generation and allocation concealment (2, 6, 8, 11, 12, 18), while one study did not provide sufficient details in these domains (17). With respect to blinding, five studies were judged to have a low risk of bias for both participants/personnel and outcome assessment (2, 6, 8, 11, 12), while two were rated as having an unclear risk (17, 18). No evidence of attrition bias or selective reporting bias was detected in any of the included studies (2, 6, 8, 11, 12, 17, 18), and no other substantial sources of bias were identified. Overall, the majority of the data synthesized in this meta-analysis originated from studies with a low risk of bias.
Risk of bias of studies comparing teprotumumab and placebo.
Risk of bias summary of studies comparing teprotumumab and placebo.
Meta-analysis for the efficacy of teprotumumab
Six studies reported data on the proptosis response rate. At the predefined 24-week endpoint, teprotumumab was associated with a significantly higher likelihood of achieving a proptosis response rate compared to placebo (Figure 4). The pooled RR for response was 6.87 (95% CI, 3.32 to 14.24; P < 0.00001). Analyses stratified by trial type produced consistent findings: the four primary trials demonstrated a RR of 6.64 (95% CI, 2.67 to 16.49; P < 0.0001) (2, 6, 11, 12), and the two secondary trials yielded a RR of 9.30 (95% CI, 1.47 to 58.67; P = 0.02) (17, 18). Collectively, these results provide robust evidence that teprotumumab is highly effective in achieving a proptosis response in patients with TED.
Proptosis response rate comparing teprotumumab and placebo.
The overall response was evaluated in five included studies. Pooled analysis demonstrated that teprotumumab was associated with a significantly higher overall response compared to placebo (Figure 5), with a RR of 7.82 (95% CI, 3.36 to 18.18; P < 0.00001). This treatment effect was consistent across predefined trial types, including both the primary studies (RR, 9.28; 95% CI, 3.04 to 28.28; P < 0.0001) and the secondary studies (RR, 5.40; 95% CI, 1.50 to 19.46; P = 0.01) (17). These findings reinforce the robust efficacy of teprotumumab in improving the overall therapeutic response of TED.
Overall response rate comparing teprotumumab and placebo.
All seven studies reported the mean change in proptosis from baseline. Meta-analysis confirmed that teprotumumab produced a significantly greater reduction in proptosis compared with placebo (Figure 6). Treatment with teprotumumab resulted in a pronounced decrease in proptosis, whereas a slight increase was observed in the placebo groups. The pooled MD was -2.46 mm (95% CI, -2.96 to -1.96; P < 0.00001). This therapeutic benefit was consistently observed in analyses stratified by trial type of the primary studies (MD, -2.23 mm; 95% CI, -2.63 to -1.84; P < 0.00001) and the secondary analyses (MD, -3.53 mm; 95% CI, -5.88 to -1.18; P = 0.003). Collectively, these findings confirm that teprotumumab provides a significant and clinically meaningful improvement in proptosis in TED.
Change in proptosis from the baseline comparing teprotumumab and placebo.
Data on the diplopia response rate were available from all seven studies. Six of these trials demonstrated a consistent benefit favoring teprotumumab, with only the study by Douglas et al. (6) serving as an outlier. The pooled analysis revealed a statistically significant improvement in diplopia response with teprotumumab compared placebo (Figure 7), with a RR of 1.85 (95% CI, 1.28 to 2.68; p = 0.001). This primary finding was further supported by analyses stratified by trial type, which yielded concordant and statistically significant results (RR, 1.67; 95% CI, 1.14 to 2.45; P = 0.009; and RR, 3.19; 95% CI, 1.44 to 7.04; P = 0.004). Together, these results provide robust evidence that teprotumumab effectively improves diplopia in patients with TED.
Diplopia response rate comparing teprotumumab and placebo.
Teprotumumab was associated with a significantly higher likelihood of achieving a CAS of ≤1 compared with placebo based on a meta-analysis of five studies (2, 8, 11, 12, 17) (Figure 8), reaching a pooled RR of 3.39 (95% CI, 2.41 to 4.78; P < 0.00001). This treatment effect was consistently observed across predefined trial types, including primary studies (RR, 3.28; 95% CI, 2.30 to 4.67; P < 0.00001) and secondary studies (RR, 5.40; 95% CI, 1.50 to 19.46; P = 0.01). Collectively, these findings confirm that teprotumumab significantly reduces inflammatory disease activity in TED.
Proportion of subjects with a clinical activity score ≤1 comparing teprotumumab and placebo.
Four studies reported the mean change in GO-QOL overall score from baseline. Meta-analysis confirmed that the changes in GO-QOL scores from the baseline to week 24 were greater in the teprotumumab group compared to the placebo group (Figure 9). The pooled MD was 10.87 points (95% CI, 9.91 to 11.83; P < 0.00001). These findings confirm that teprotumumab provides a significant meaningful improvement in GO-QOL in TED.
Change in GO-QOL score from baseline comparing teprotumumab and placebo.
Furthermore, trial-level analyses stratified by study region (Europe/America vs. Asia) were performed, with results presented in the Supplementary Figures S1–S6. Across regions, teprotumumab consistently demonstrated strong efficacy in achieving a proptosis response, improving the overall therapeutic response, and providing a statistically and clinically meaningful reduction in proptosis. Improvements in diplopia were observed across regions; however, in the Asian subgroup, the improvement in diplopia did not reach statistical significance. Teprotumumab was also associated with a significantly higher likelihood of achieving a CAS of ≤1 compared with placebo, as well as a statistically and clinically meaningful improvement in the GO−QOL scores.
Meta-analysis for the safety of teprotumumab
Figure 10 presents the pooled analysis of adverse events comparing teprotumumab with placebo. Gastrointestinal events, including nausea (RR, 1.72; 95% CI, 0.82 to 3.63; P = 0.15), diarrhea (RR, 1.43; 95% CI, 0.74 to 2.78; P = 0.29), and stomatitis (RR, 3.66; 95% CI, 0.80 to 16.81; P = 0.09), were numerically more frequent in the teprotumumab group but did not reach statistically significance. Similarly, non-significant increases were observed for fatigue (RR, 2.87; 95% CI, 0.88 to 9.41; P = 0.08), alopecia (RR, 1.70; 95% CI, 0.85 to 3.37; P = 0.13), and dysgeusia (RR, 4.08; 95% CI, 0.93 to 17.88; P = 0.06). In contrast, teprotumumab treatment was associated with a statistically increased risk of hyperglycemia (RR, 2.82; 95% CI, 1.08 to 7.37; P = 0.03], muscle spasms (RR, 3.83; 95% CI, 1.97 to 7.43; P < 0.0001), dry skin (RR, 6.54; 95% CI, 1.52 to 28.09; P = 0.01), and hearing impairment (RR, 3.74; 95% CI, 1.26 to 11.13; P = 0.02) compared to placebo. No significant differences between treatment groups were observed for headache (RR, 1.20; 95% CI, 0.56 to 2.59; P = 0.63) or infusion-related reactions (RR, 0.66; 95% CI, 0.17 to 2.55; P = 0.54).
Adverse drug reaction comparing teprotumumab and placebo.
Heterogeneity and sensitivity analysis
To assess the robustness of the primary outcomes, a sensitivity analysis was performed after excluding the trial by Douglas et al. (6), which was the only study to include patients in the inactive phase of disease (CAS < 3). As summarized in Table 2, the exclusion of this study did not materially alter the results. Teprotumumab remained associated with significantly greater efficacy than placebo across all endpoints, including proptosis response, diplopia response, and the mean change in proptosis from baseline (all P < 0.00001). Moreover, this exclusion resulted in a substantial reduction in the I² statistic, indicating that the inclusion of participants with inactive disease was a principal source of heterogeneity in the overall analysis.
Discussion
This systematic review and updated meta-analysis, encompassing seven RCTs with a total of 438 patients, provides a comprehensive evaluation of the efficacy and safety of teprotumumab for TED. The pooled evidence demonstrates that teprotumumab confers significantly greater therapeutic benefit than placebo across all prespecified efficacy endpoints, including proptosis response, overall response, mean reduction in proptosis, improvement in diplopia, change in GO-QOL overall scores and achievement of a CAS of 0 or 1. Consistent results were observed in trial-level analyses stratified by study region, further supporting the robustness of these findings. In parallel, the safety analysis revealed a generally manageable adverse event profile, although the risks of hyperglycemia, muscle spasms, and hearing impairment were significantly higher in the teprotumumab group. The consistently low risk of bias across the included trials supports the robustness and reliability of these pooled estimates.
The profound efficacy of teprotumumab demonstrated in this meta-analysis reinforces the findings of the landmark trials that established its clinical role. The marked proptosis response and significant mean reduction in proptosis are consistent with the proposed mechanistic of IGF-1R inhibition, which directly mitigates orbital tissue remodeling (2, 8, 19). These results are concordant with the pivotal trials by Smith et al. and with previous meta-analyses reporting similar magnitudes of benefit (2, 8, 20, 21). Importantly, our pooled analysis clarifies previous inconsistencies regarding diplopia improvement. While the recent RESTORE-1 trial (evaluating IBI311) did not show a statistically significant effect on diplopia, this is likely attributable to a lower baseline prevalence and different severity of diplopia in its cohort, which limited statistical power (12). By integrating data across a larger aggregate sample, our analysis provides a more precise and stable estimate, confirming that teprotumumab confers a statistically and clinically meaningful improvement in this functionally critical endpoint among patients with TED.
An important insight from this meta-analysis concerns the exploration of heterogeneity. The substantial heterogeneity (I² > 50%) observed in the initial analyses for several efficacy outcomes was markedly reduced after exclusion of the trial by Douglas et al. (6) in the sensitivity analysis. This study was uniquely enrolled patients with chronic, low-activity TED (CAS ≤ 1), a population that is both phenotypically and pathophysiologically distinct from the active TED patients included in the other trials (22). The marked reduction in I² identifies disease activity status as a major source of heterogeneity. Notably, exclusion of this trial did not affect the statistical significance of any efficacy outcome, underscoring the robustness of our primary findings. These results suggest that while the magnitude of benefit may vary with disease activity, teprotumumab retains measurable efficacy not only in active TED but potentially also in patients with chronic, inactive disease–possibly through attenuation of fibrotic remodeling (6, 23). Furthermore, analyses stratified by trial type differentiating primary interventional RCTs from smaller, secondary analyses (17, 18) demonstrated concordant directionality and significance of treatment effects, reinforcing the generalizability of teprotumumab’s efficacy beyond the narrowly defined populations of the pivotal trials.
Several patient-related factors, including smoking status and age, are known to influence disease activity, severity, and therapeutic response in thyroid eye disease (24, 25). However, none of the included randomized controlled trials reported treatment effects stratified by smoking status or age, precluding patient-level subgroup analyses. Nevertheless, baseline characteristics across the included studies were broadly comparable, with similar age distributions and smoking proportions between treatment arms within individual trials, suggesting that these factors were unlikely to have substantially confounded the pooled estimates. Future studies and individual patient data meta-analyses are warranted to further clarify the influence of these factors on response to teprotumumab.
The safety profile elucidated in this meta-analysis underscores the need for careful risk-benefit evaluation and proactive monitoring. Several known adverse drug reactions consistent with the pharmacologic mechanism of IGF-1R inhibition were confirmed. The significantly increased risks of muscle spasms and hyperglycemia are well-documented in prior studies (9, 13). Reported hyperglycemia events ranged from transient, asymptomatic elevations in blood glucose to new-onset insulin-requiring diabetes (2, 13, 26). Mechanistically, teprotumumab-induced IGF-1R blockade disrupts glucose homeostasis by enhancing growth hormone-mediated insulin resistance and impairing insulin signaling through internalization of IGF-1R/insulin receptor hybrid complexes. Consequently, baseline assessment of glycemic status and regular glucose monitoring throughout treatment are strongly recommended to mitigate the risk of hyperglycemia (27–30).
Of particular clinical importance is hearing impairment, which showed a 3.74-fold increased risk compared with placebo. This otologic adverse event–manifesting as tinnitus, ear fullness, or autophony–has been increasingly characterized in recent prospective investigations (14, 16). Although often reversible following dose interruption or treatment completion, these effects can be distressing and warrant pre-treatment audiometric assessment and thorough patient counseling (15). Other adverse events, such as gastrointestinal disturbances, occurred more frequently in the teprotumumab group but were typically mild to moderate in severity.
Limitations in current evidence
Despite its strengths, this study has several limitations. First, the relatively short follow-up duration (24 weeks) of the included RCTs limits the ability to draw conclusions regarding the long-term durability of response, relapse rates, and the emergence of late-onset adverse events. Second, the modest sample size for some rare adverse events may have resulted in imprecise risk estimates. Finally, the absence of individual patient data precluded a more detailed exploration of patient-specific modifiers of treatment response–such as thyroid function status, prior therapies, and disease duration–which may influence clinical outcomes.
Conclusions
This meta-analysis provides high-level evidence that teprotumumab offers substantial clinical benefits for patients with thyroid eye disease, effectively improving the disabling manifestations of proptosis and diplopia. The consistency of these findings across diverse study populations supports the robustness of the therapeutic effect. At the same time, teprotumumab is associated with a higher incidence of specific adverse events–most notably hyperglycemia, muscle spasms, and hearing impairment-which are generally manageable with appropriate monitoring. Its clinical use should therefore be accompanied by proactive risk assessment and vigilant monitoring strategies. Future research should refine patient selection, establish long-term efficacy and retreatment frameworks, and develop management protocols to optimize the therapeutic value of this targeted IGF-1R inhibitor.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Smith TJ Hegedüs L . Graves’ disease. N Engl J Med. (2016) 375:1552–65. doi: 10.1056/NEJ Mra 1510030, PMID: 27797318 · doi ↗ · pubmed ↗
- 2Douglas RS Kahaly GJ Patel A Sile S Thompson EHZ Perdok R . Teprotumumab for the treatment of active thyroid eye disease. N Engl J Med. (2020) 382:341–52. doi: 10.1056/NEJ Moa 1910434, PMID: 31971679 · doi ↗ · pubmed ↗
- 3Smith TJ Janssen JAMJL . Insulin-like growth factor-I receptor and thyroid-associated ophthalmopathy. Endocr Rev. (2019) 40:236–67. doi: 10.1210/er.2018-00066, PMID: 30215690 PMC 6338478 · doi ↗ · pubmed ↗
- 4Baralena L Piantanida E Gallo D Lai A Tanda ML . Epidemiology, natural history, risk factors, and prevention of Graves’ orbitopathy. Front Endocrinol (Lausanne). (2020) 11:615993. doi: 10.3389/fendo.2020.615993, PMID: 33329408 PMC 7734282 · doi ↗ · pubmed ↗
- 5Bartalena L Kahaly GJ Baldeschi L Dayan CM Eckstein A Marcocci C . The 2021 European Group on Graves’ orbitopathy (EUGOGO) clinical practice guidelines for the medical management of Graves’ orbitopathy. Eur J Endocrinol. (2021) 185:G 43–67. doi: 10.1530/EJE-21-0479, PMID: 34297684 · doi ↗ · pubmed ↗
- 6Douglas RS Couch S Wester ST Fowler BT Liu CY Subramanian PS . Efficacy and safety of teprotumumab in patients with thyroid eye disease of long duration and low disease activity. J Clin Endocrinol Metab. (2023) 109:25–35. doi: 10.1210/clinem/dgad 637, PMID: 37925673 PMC 10735297 · doi ↗ · pubmed ↗
- 7Tsui S Naik V Hoa N Hwang CJ Afifiyan NF Sinha Hikim A . Evidence for an association between thyroid-stimulating hormone and insulin-like growth factor 1 receptors: a tale of two antigens implicated in Graves’ disease. J Immunol. (2008) 181:4397–405. doi: 10.4049/jimmunol.181.6.4397, PMID: 18768899 PMC 2775538 · doi ↗ · pubmed ↗
- 8Smith TJ Kahaly GJ Ezra DG Fleming JC Dailey RA Tang RA . Teprotumumab for thyroid-associated ophthalmopathy. N Engl J Med. (2017) 376:1748–61. doi: 10.1056/NEJ Moa 1614949, PMID: 28467880 PMC 5718164 · doi ↗ · pubmed ↗