Abdominal Cocoon Syndrome With Greater Omental Hypoplasia: A Rare Anatomical Insight and Diagnostic Challenge
Sohrab Sayyadi, Keihan Shabankhani, Mohammad Mahdi Sargazi Moghaddam, Seyed Mohammad Sakhaei, Mina Alvandipour, Seyed Muhammad Mehdi Ghaffari Hamedani, Hossein Farsavian, Mohammad Javad Najafi

TL;DR
This paper describes a rare case of abdominal cocoon syndrome combined with greater omental hypoplasia, emphasizing the importance of surgical exploration for diagnosis and treatment.
Contribution
The paper reports the first documented case of abdominal cocoon syndrome co-occurring with greater omental hypoplasia.
Findings
Surgical exploration confirmed abdominal cocoon syndrome and resolved symptoms in a patient with recurrent gastrointestinal obstruction.
The co-occurrence of greater omental hypoplasia suggests potential embryologic links to the syndrome's pathophysiology.
Early surgical intervention proved both diagnostic and therapeutic in this challenging case.
Abstract
Abdominal cocoon syndrome, or idiopathic sclerosing encapsulating peritonitis (SEP), is an uncommon cause of small bowel obstruction marked by the encasement of bowel loops within a dense fibrocollagenous membrane. Due to its rarity and nonspecific presentation, diagnosis is frequently delayed, particularly in patients without prior abdominal surgery or known risk factors. We report a diagnostically challenging case of a 53‐year‐old male with an 18‐month history of recurrent gastrointestinal obstruction, including bilious vomiting, oral intolerance, and epigastric pain. Multiple prior evaluations yielded inconclusive findings. Contrast‐enhanced computed tomography raised suspicion for SEP, prompting exploratory laparotomy. Intraoperative findings confirmed SEP, along with a rare anatomical anomaly—hypoplasia of the greater omentum. Surgical excision of the encasing membrane and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
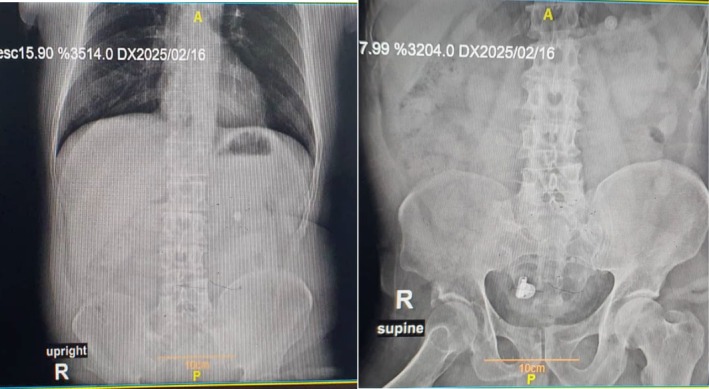 FIGURE 1
FIGURE 1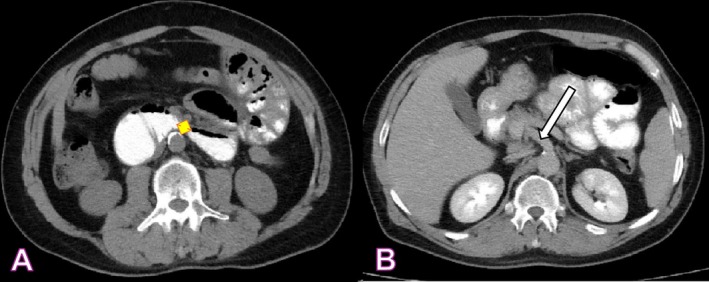 FIGURE 2
FIGURE 2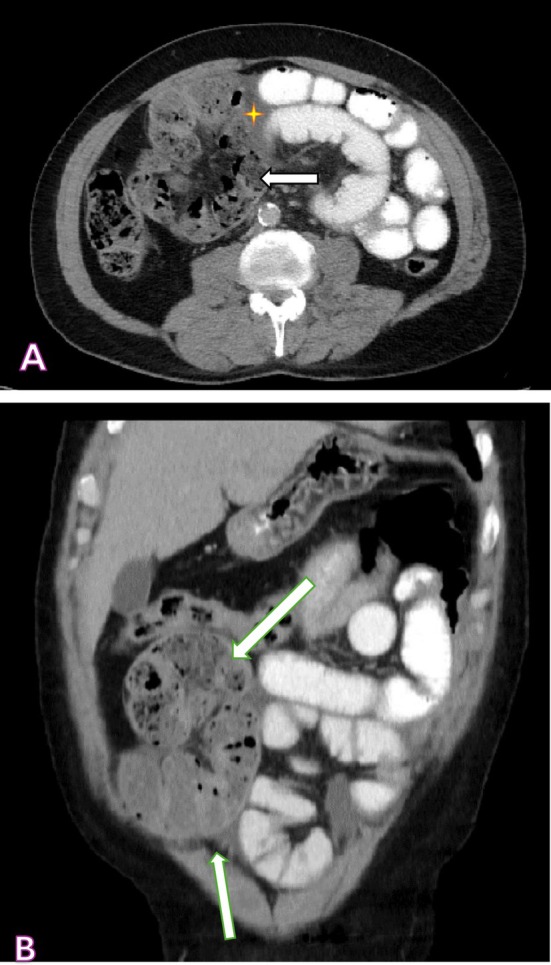 FIGURE 3
FIGURE 3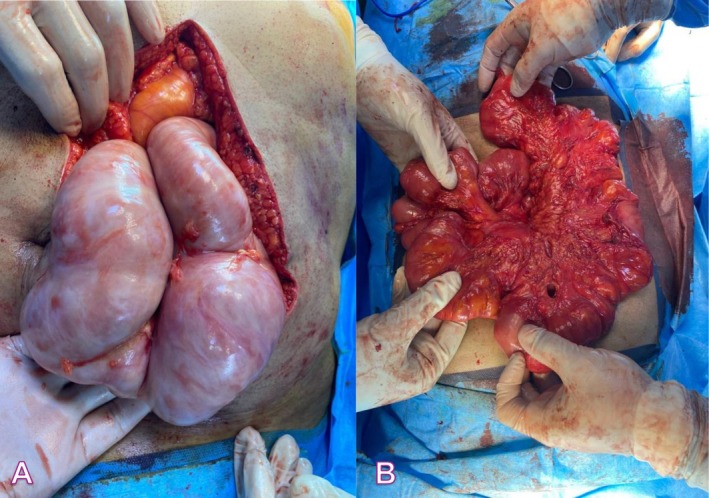 FIGURE 4
FIGURE 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOmental and Epiploic Conditions · Vascular anomalies and interventions · Spinal Dysraphism and Malformations
Introduction
1
Abdominal cocoon syndrome, or idiopathic sclerosing encapsulating peritonitis (SEP), is a rare, often under‐recognized cause of small bowel obstruction. Described in the early 1900s, it involves the small intestine encased by a dense fibrocollagenous membrane. Its exact cause is unknown, but it mainly affects young males in tropical and subtropical areas [1, 2].
Abdominal cocoon syndrome, due to its rarity and nonspecific symptoms, is often misdiagnosed or missed and is usually found only during surgery. Symptoms range from chronic abdominal pain to acute bowel obstruction [3].
Without prior abdominal surgery or risk factors, suspicion is usually low, and the condition may be mistaken for common causes like adhesive disease, internal hernia, or vascular compression [4].
Preoperative imaging frequently results in inconclusive findings when diagnosing this condition; even contrast‐enhanced computed tomography may not provide definitive results, but it remains valuable for excluding other differential diagnoses. Due to diagnostic challenges and the potential curative role of surgery, heightened clinical vigilance is essential, especially in patients with recurrent, unexplained gastrointestinal obstructions [5].
Surgical intervention, especially laparotomy, remains the cornerstone and most effective treatment modality for SEP [6].
Nevertheless, its utilization is a subject of ongoing discourse concerning suitable indications, optimal timing, and procedural techniques. These ambiguities arise from less‐than‐ideal surgical outcomes observed in certain instances, where patients may experience postoperative complications such as recurrent small bowel obstruction or the development of new adhesions [6].
We present a middle‐aged male with a prolonged history of nonspecific gastrointestinal symptoms, diagnosed with SEP only after exploratory laparotomy. This report highlights a challenging case where surgery was crucial for diagnosis.
Case History/Examination
2
A 53‐year‐old man was referred with recurrent episodes over 18 months, involving oral intolerance, nausea, bilious vomiting, and intestinal obstruction. Each episode included severe epigastric pain worsened by eating and up to eight episodes of bilious emesis. He reported complete oral intake intolerance during these times.
He denied fever, chills, or rigors. The episodes followed a consistent pattern, prompting multiple consultations that provided temporary relief without diagnosis. Prior records showed normal labs, no air‐fluid levels, and unremarkable endoscopies.
His medical history was otherwise unremarkable, with no chronic illnesses, prior surgeries, significant family history, or alcohol use, and no unintentional significant weight loss over the last 18 months. The patient reported initiating opium use in response to recurrent episodes of abdominal pain, which subsequently progressed to opioid dependence. At the time of referral, he was enrolled in a methadone maintenance program and was not taking any other regular medications.
During a prior episode, the medical team suspected superior mesenteric artery (SMA) syndrome and referred the patient to our facility for continued evaluation and management.
On presentation, he appeared ill but was alert and cooperative. Vital signs were stable: temperature 37°C, blood pressure 125/75 mmHg, heart rate 95 bpm, oxygen saturation 99%. Ocular exam showed no pallor or scleral icterus. Cardio‐pulmonary eval was normal, with regular heart sounds and clear lungs. Abdominal exam revealed mild generalized distension. The soft abdomen was diffusely tender, especially in the epigastric area, without rebound, guarding, or organomegaly. Bowel sounds were hypoactive. Laboratory results showed normal electrolytes and blood glucose. Renal markers were elevated (BUN: 65 mg/dL, creatinine: 1.7 mg/dL), indicating dehydration‐related pre‐renal azotemia. Mild leukocytosis (WBC: 10.9 × 10^3^/μL) and thrombocytosis (436 × 10^3^/μL) were observed, with normal hemoglobin and coagulation.
Abdominal radiography revealed no diagnostic abnormalities (Figure 1). Consequently, a contrast‐enhanced computed tomography (CT) scan was performed. CT findings excluded SMA syndrome (Figure 2) and raised suspicion for SEP based on the presence of peritoneal fibrosis and mild ascites (Figure 3).
Abdominal X‐ray.
Contrast‐enhanced computed tomography (axial plane). (A) Aortomesenteric distance exceeding 12 mm; (B) Superior Mesenteric Artery indicated by a white arrow.
Encapsulating peritoneal sclerosis (EPS), characterized by fibrosis of the peritoneum (white arrow) and the encasement of the small intestine, with minimal ascites (yellow star). (A) Axial plane; (B) Coronal plane.
Differential Diagnosis, Investigations, and Treatment
3
Despite support, the patient showed symptoms of proximal intestinal obstruction, such as increasing abdominal distension and oral intolerance. Due to suspicion of abdominal cocoon syndrome and radiologic findings, the surgical team chose to perform an exploratory laparotomy. Diagnostic laparoscopy was unsafe because of severe distension.
Intraoperatively, hypoplasia of the greater omentum was observed, with the entire small intestine encased in a thick fibrous membrane and dense adhesions limiting bowel mobility, consistent with abdominal cocoon syndrome. The membrane was carefully dissected and removed, and adhesiolysis was performed to free the bowel. No resection, ischemia, or perforation was present (Figure 4).
(A) Encapsulated small bowel; (B) Released encapsulated small bowel.
Conclusion and Results
4
Postoperatively, the patient recovered uneventfully. Oral intake resumed 24 h later, was well tolerated, and without complications. Abdominal pain resolved, and bowel function normalized. He was discharged in stable condition. At six months, he remained asymptomatic, with no GI complaints, and resumed regular diet and activity.
Discussion
5
Abdominal cocoon syndrome is a rare but important diagnosis in patients with chronic or recurrent small bowel obstruction, especially without prior abdominal surgery or underlying issues [7] Initially described in 1907 and clarified in 1978, it is characterized by a dense fibrocollagenous membrane encasing the small bowel and sometimes other organs, causing mechanical obstruction [8].
The pathogenesis of idiopathic abdominal cocoon syndrome remains poorly understood. Proposed mechanisms include retrograde peritonitis, omental hypoplasia, and mesenteric vascular anomalies [9]. Secondary forms have been linked to factors such as peritoneal dialysis, beta‐blocker therapy, tuberculosis, sarcoidosis, and systemic autoimmune diseases. The idiopathic variant is more commonly observed in tropical and subtropical regions, primarily affecting young males; however, cases have been documented across a broader demographic spectrum [10, 11].
Clinically, the syndrome manifests as recurrent or chronic abdominal pain, nausea, vomiting, and symptoms indicative of subacute intestinal obstruction. Patients often recount intermittent episodes lasting months or years, with spontaneous remission complicating timely diagnosis [12]. In the present case, our patient experienced multiple such episodes over a period of 18 months prior to undergoing definitive surgical management.
Anatomical anomalies like greater omentum hypoplasia are very rare and rarely reported with abdominal cocoon syndrome. The greater omentum, from dorsal mesogastrium, is essential for immune surveillance, angiogenesis, and peritoneal fluid dynamics [13, 14]. Hypoplasia may reflect disrupted mesodermal differentiation or defective peritoneal folding during the 4th to 8th week of gestation [15, 16]. In our case, the absence of a fully developed omental curtain could have impaired mechanical protection and localized immune regulation, potentially contributing to aberrant fibrocollagenous membrane formation. The co‐occurrence of SEP and omental hypoplasia suggests a possible shared embryopathogenic pathway, opening avenues for future exploration into peritoneal morphogenesis and intra‐abdominal immune responses. Recognition of this pairing not only expands the spectrum of SEP presentations but also enhances the surgical understanding of rare peritoneal disorders.
Radiologic diagnosis presents considerable challenges. CT imaging may demonstrate clumped bowel loops encased within a membranous capsule, occasionally referred to as the “cauliflower sign,” in conjunction with peritoneal thickening and ascites [17]. Nevertheless, the sensitivity of imaging modalities remains limited, and a definitive diagnosis is frequently established intraoperatively. In our case, despite the administration of two contrast‐enhanced CT scans, spontaneous encapsulating peritoneal sclerosis (SEP) was not conclusively identified until exploratory laparotomy.
Surgical treatment remains the main approach for symptomatic cases. Complete excision of the fibrous membrane and adhesiolysis usually resolve symptoms with low recurrence rates when extensively removed. Conservative methods may be suitable for carefully selected, minimally symptomatic cases but are often inadequate in idiopathic cases requiring surgery due to progressive obstruction intervention [18].
Conclusion
6
This case underscores the diagnostic challenges and clinical significance of abdominal cocoon syndrome in patients presenting with unexplained, recurrent gastrointestinal obstruction. Although rare, the condition should be considered in the differential diagnosis when suggestive clinical features are present and imaging remains inconclusive. Surgical exploration offers both definitive diagnosis and curative treatment, with favorable outcomes when performed in a timely manner. Heightened awareness among clinicians is vital to ensure early recognition and avoid delays in management.
Author Contributions
Sohrab Sayyadi: data curation, investigation, methodology, writing – original draft. Keihan Shabankhani: data curation, investigation, writing – original draft. Mohammad Mahdi Sargazi Moghaddam: data curation, investigation, writing – review and editing. Seyed Mohammad Sakhaei: conceptualization, data curation, investigation, writing – review and editing. Mina Alvandipour: investigation, writing – review and editing. Seyed Muhammad Mehdi Ghaffari Hamedani: investigation, writing – review and editing. Hossein Farsavian: investigation, writing – review and editing. Mohammad Javad Najafi: conceptualization, data curation, investigation, project administration, supervision, validation, visualization, writing – original draft, writing – review and editing.
Funding
The authors have nothing to report.
Ethics Statement
All procedures conducted were compliant with the ethical standards established by the responsible committee on human experimentation, both institutional and national, and adhered to the Helsinki Declaration of 1975, as amended in 2008. The research protocol received approval from the Research Ethics Committees (Approval Code: IR.MAZUMS.REC.1404.136).
Consent
Written informed consent was obtained from the patient to document this case report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1J. N. Tannoury and B. N. Abboud , “Idiopathic Sclerosing Encapsulating Peritonitis: Abdominal Cocoon,” World Journal of Gastroenterology: WJG 18, no. 17 (2015): 1999.10.3748/wjg.v 18.i 17.1999 PMC 334259622563185 · doi ↗ · pubmed ↗
- 2S. Akbulut , “Accurate Definition and Management of Idiopathic Sclerosing Encapsulating Peritonitis,” World Journal of Gastroenterology: WJG 21, no. 2 (2015): 675.25593498 10.3748/wjg.v 21.i 2.675PMC 4292304 · doi ↗ · pubmed ↗
- 3P. Ashok Kumar , S. Sambandam , G. Singh , et al., “Idiopathic Sclerosing Encapsulating Peritonitis: A Rare Cause of Intestinal Obstruction,” ANZ Journal of Surgery 88, no. 10 (2018): 730–731.10.1111/ans.1368527452684 · doi ↗ · pubmed ↗
- 4A. Sghair , M. Debaibi , M. Kchaou , S. Talbi , A. Sridi , and A. Chouchen , “Idiopathic Sclerosing Encapsulating Peritonitis: An Uncommon Cause of Intestinal Obstruction in a Virgin Abdomen,” Clinical Case Reports 10, no. 3 (2022): e 05603.35317068 10.1002/ccr 3.5603 PMC 8922953 · doi ↗ · pubmed ↗
- 5N. Bouardi , M. Y. A. Lamrani , M. Haloua , B. Alami , M. Boubou , and M. Maaroufi , “Idiopathic Sclerosing Encapsulating Peritonitis: A Case Report,” Pan African Medical Journal 38 (2021): 136.33912306 10.11604/pamj.2021.38.136.28043 PMC 8052624 · doi ↗ · pubmed ↗
- 6N. Li , W. Zhu , Y. Li , et al., “Surgical Treatment and Perioperative Management of Idiopathic Abdominal Cocoon: Single‐Center Review of 65 Cases,” World Journal of Surgery 38, no. 7 (2014): 1860.24519587 10.1007/s 00268-014-2458-6 · doi ↗ · pubmed ↗
- 7A. P. Karl , H. Leebmann , and N. Zorger , “Abdominal Cocoon Syndrome,” Deutsches Ärzteblatt International 116, no. 27–28 (2019): 486.10.3238/arztebl.2019.0486 b PMC 671889031431239 · doi ↗ · pubmed ↗
- 8A. Chorti , S. Panidis , D. Konstantinidis , et al., “Abdominal Cocoon Syndrome: Rare Cause of Intestinal Obstruction—Case Report and Systematic Review of Literature,” Medicine 101, no. 27 (2022): e 29837.35801789 10.1097/MD.0000000000029837 PMC 9259168 · doi ↗ · pubmed ↗