New bile duct cannulation technique using a fine-needle aspiration needle to prevent post-endoscopic retrograde cholangiopancreatography pancreatitis
Ikuhiro Kobori, Ou Takagi, Haruka Kato, Masaru Kuwada, Koichi Soga, Yasumi Katayama, Masaya Tamano

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1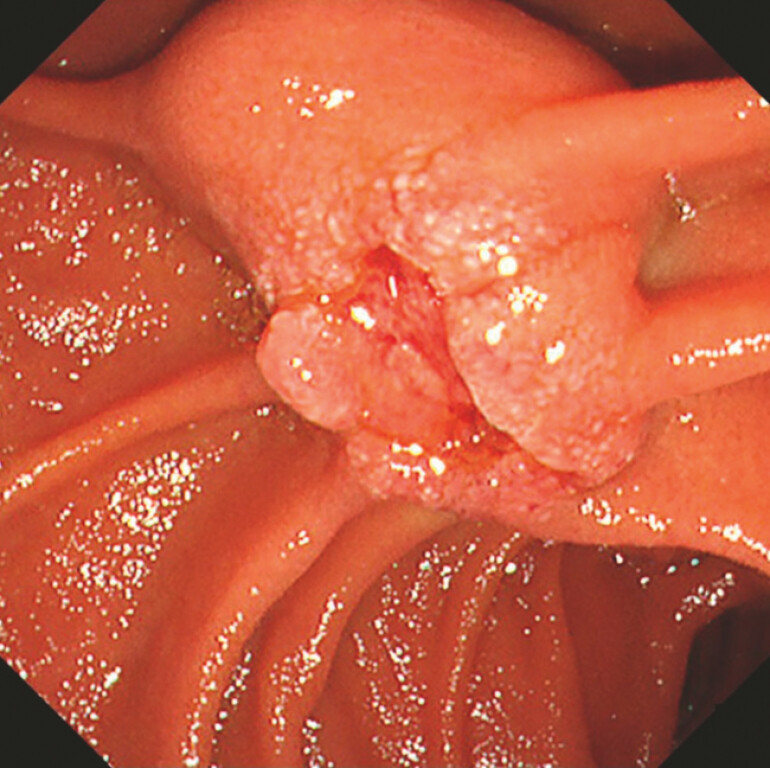 Fig. 2
Fig. 2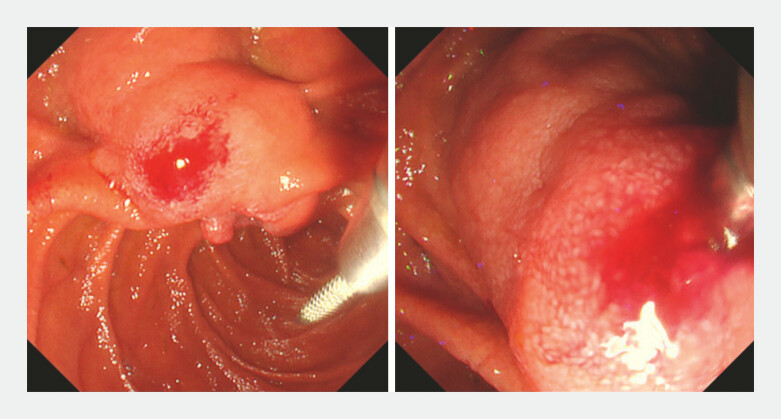 Fig. 3
Fig. 3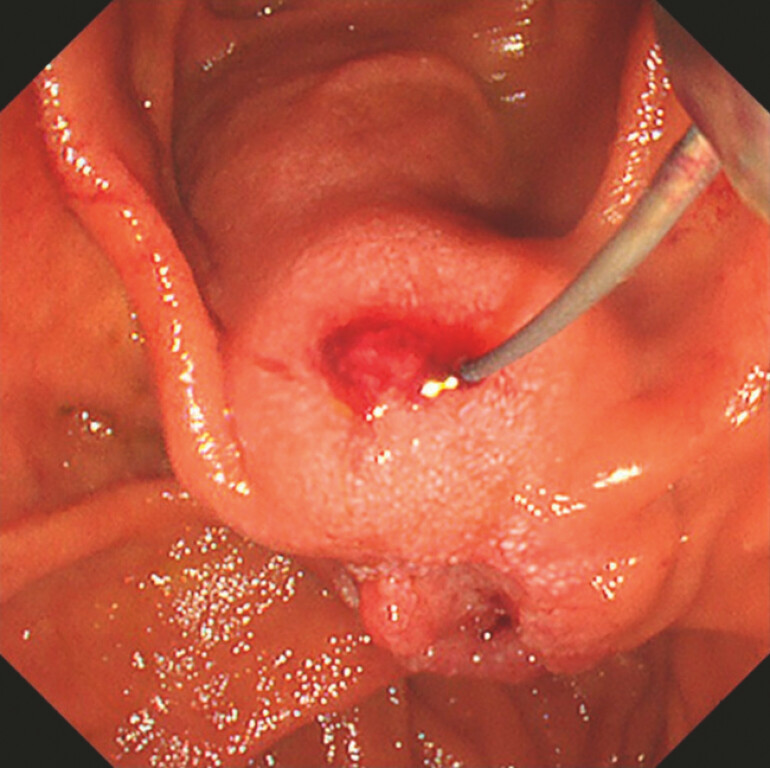 Fig. 4
Fig. 4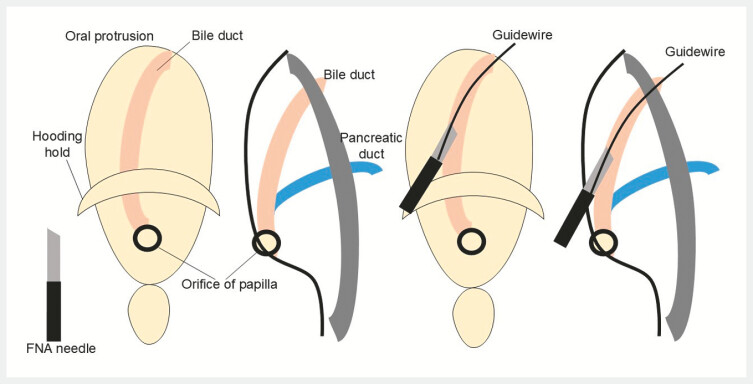 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Pancreatitis Pathology and Treatment · Pancreatic and Hepatic Oncology Research
Endoscopic retrograde cholangiopancreatography (ERCP) carries a risk of post-ERCP pancreatitis (PEP 1 ). Precut techniques and needle-knife fistulotomy carry risks such as perforation and bleeding 2 3 4 . We report a novel method for bile duct cannulation using a fine-needle aspiration (FNA) needle.
A 78-year-old woman underwent ERCP for obstructive jaundice due to duodenal papillary carcinoma ( Fig. 1 ). Endoscopic examination revealed a depressed lesion at the duodenal papilla, with indistinct bile duct openings ( Fig. 2 ). To reduce the risk of PEP and bleeding, we decided to perform biliary drainage using a new method that avoids touching the papillary orifice ( Video 1 ). First, we punctured the large oral protrusion near the papillary orifice, where the bile duct was presumed to be located, using a 22-gauge FNA needle (EZ Shot 3 Plus; Olympus Medical Systems, Tokyo, Japan; Fig. 3 ). A 0.018-inch guidewire (Fielder 18; Olympus Medical Systems, Tokyo, Japan) was placed in the bile duct ( Fig. 4 ). The FNA needle was then removed, and a 3-Fr microcatheter (Daimon ERCP catheter; Hanaco Medical, Saitama, Japan 5 ) was advanced over the guidewire and left in the bile duct. After cholangiography, the guidewire was replaced with a 0.025-inch guidewire. A tapered-tip ERCP catheter was advanced into the bile duct to dilate the puncture site and aspirate bile. Finally, a 7-Fr plastic stent was placed. No complications were observed, and jaundice resolution was favorable.
Contrast-enhanced computed tomography shows duodenal papillary carcinoma and dilation of the common bile duct.
An endoscopic view showing a large oral protrusion and a depressed lesion at the duodenal papilla, with indistinct bile duct openings.
An Endoscopic view showing the puncture of the oral protrusion (left) and insertion of a guidewire into the bile duct through a 22-gauge fine-needle aspiration needle (right).
An endoscopic view showing the insertion of a 0.018-inch guidewire into the bile duct through the puncture site.
A novel biliary cannulation technique to reduce the risk of post-endoscopic retrograde cholangiopancreatography pancreatitis, bleeding, and perforation by avoiding contact with the papillary orifice.Video 1
This method carries an extremely low risk of PEP because it avoids touching the papillary orifice ( Fig. 5 ). It also minimizes the risk of bleeding or perforation by enabling access to the bile duct without applying an electrical current. Even if the bile duct cannot be punctured initially, the small size of the puncture site permits multiple attempts through the adjustment of the puncture location, contributing to the utility of the method.
Schema of the puncture of the oral protrusion and insertion of a guidewire into the bile duct through the fine-needle aspiration (FNA) needle.
Endoscopy_UCTN_Code_TTT_1AR_2AC
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dumonceau JM Andriulli A Elmunzer BJ Prophylaxis of post-ERCP pancreatitis: European Society of Gastrointestinal Endoscopy (ESGE) guideline – updated June 2014 Endoscopy 20144679981510.1055/s-0034-137787525148137 · doi ↗ · pubmed ↗
- 2Freeman ML Guda NMERCP cannulation: a review of reported techniques Gastrointest Endosc 20056111212510.1016/s 0016-5107(04)02463-015672074 · doi ↗ · pubmed ↗
- 3Kuraishi Y Hara K Haba S Safety and feasibility of opening window fistulotomy as a new precutting technique for primary biliary access in endoscopic retrograde cholangiopancreatography Clin Endosc 20235649049810.5946/ce.2022.13037157966 PMC 10393574 · doi ↗ · pubmed ↗
- 4Sadek A Hara K Okuno N Needle puncture fistulotomy: a new technique for needle-knife fistulotomy as a primary biliary access method for biliary cannulation Endoscopy 202456 E 146E 14710.1055/a-2248-013738359884 PMC 10869223 · doi ↗ · pubmed ↗
- 5Kato A Yoshida M Kachi KA 3-Fr microcatheter is suitable for a 0.018-inch guidewire during endoscopic ultrasound-guided biliary drainage Endoscopy 202254 E 882E 88335750078 10.1055/a-1860-1981 PMC 9735334 · doi ↗ · pubmed ↗