An ultra-early biliary occlusion caused by a blood clot impaction inside a multi-hole covered self-expandable metal stent
Tesshin Ban, Yoshimasa Kubota, Yota Hirayama, Kei Ando, Naoto Imura, Shun Sasoh, Takashi Joh

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
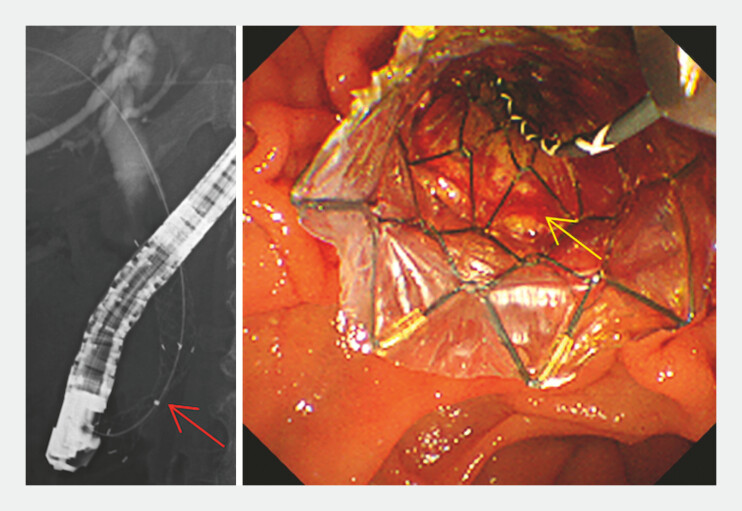 Fig. 1
Fig. 1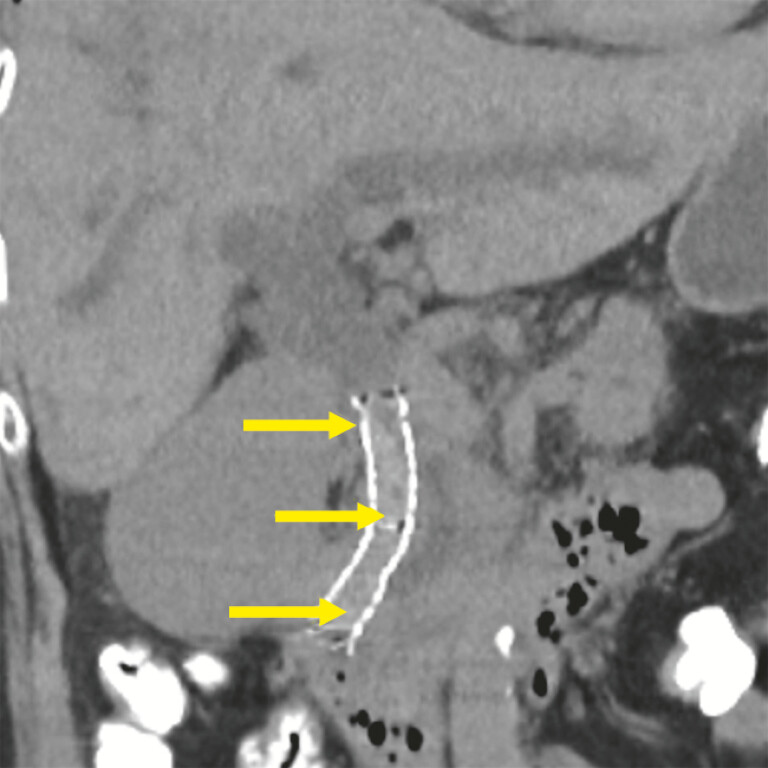 Fig. 2
Fig. 2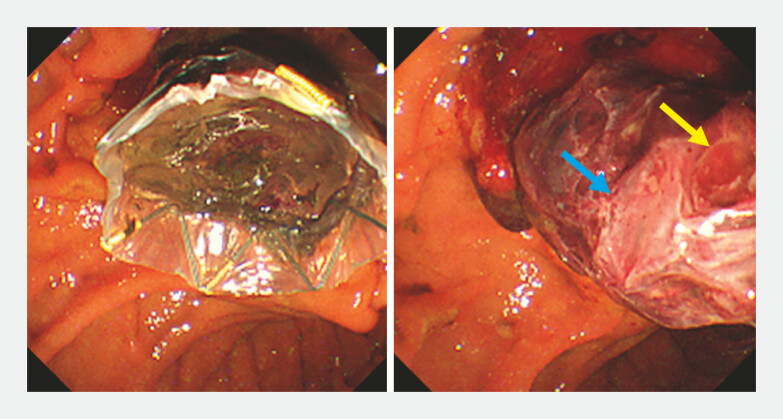 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Pediatric Hepatobiliary Diseases and Treatments · Organ Transplantation Techniques and Outcomes
There is inconclusive evidence on whether to use an uncovered self-expandable metal stent (UC-SEMS) or a covered self-expandable metal stent (C-SEMS) for patients with unresectable or borderline distal malignant biliary obstruction (D-MBO 1 2 3 ). A new multi-hole C-SEMS (MH-C-SEMS), made of nitinol mesh covered by a silicone membrane with small 1.8-mm multiple holes, has been reported to have longer patency and prevents tumor ingrowth and stent migration compared to conventionally used UC-SEMS and C-SEMS 4 .
Herein, we reported a case of ultra-early stent occlusion caused by blood clot impaction on MH-C-SEM.
A 67-year-old woman with an unresectable, well-differentiated pancreatic adenocarcinoma in the groove region developed severe obstructive jaundice. She was scheduled to undergo chemotherapy; therefore, we performed transpapillary MH-C-SEMS placement across the papilla after sphincterotomy ( Fig. 1 , Video 1 ). However, she developed worsening jaundice and acute cholangitis. Two days after the index procedure, computed tomography imaging showed stent occlusion caused by blood clot impaction of MH-C-SEMS ( Fig. 2 ). When the initial MH-C-SEMS was removed with a snare, a cast blood clot shaped by the MH-C-SEMS appeared in the papilla ( Fig. 3 , Video 1 ). Therefore, we removed the blood clot using a balloon catheter, followed by the placement of double-pigtailed plastic stents ( Video 1 ). Her clinical course was uneventful, and she underwent chemotherapy.
Fluoroscopic and endoscopic images of MH-C-SEMS in the distal malignant biliary obstruction. The red solid arrow indicates an incomplete expansion of MH-C-SEMS at the stricture, very close to the papilla. The yellow solid arrow indicates a slightly protruding tumor with blood staining through a hole in the stent membrane. MH-C-SEMS, multi-hole covered self-expandable metal stent.
A computed tomography image taken 2 days after the index procedure. The yellow solid arrows indicate a high-density embolus suspected to be blood clot impaction along the entire length of the fully expanded MH-C-SEMS. MH-C-SEMS, multi-hole covered self-expandable metal stent.
Endoscopic images of an impacted MH-C-SEMS and a withdrawn cast blood clot after stent removal. A round shape is carved into the cast blood clot ( yellow arrow) indicating that the tumor protrudes through a hole in the stent membrane. The stent wire stamped a rhombus shape (blue arrow) onto the blood clot. MH-C-SEMS, multi-hole covered self-expandable metal stent.
Ultra-early biliary occlusion caused by blood clot impaction inside a multi-hole covered self-expandable metal stent.Video 1
In patients with D-MBO, the MH-C-SEMS has been shown to allow significantly longer stent patency (mean: 479 d; 95% confidence interval: 372–586 d) than the C-SEMS and UC-SEMS 4 . Stent dysfunction caused by blood clots occur in 1.9% of cases 5 . Additionally, hemorrhagic tumors or tumors involved in sphincterotomy could lead to blood oozing from uncovered holes, which can deposit acute blood clots on the stent membrane, potentially causing ultra-early stent occlusion. Physicians should consider this point if jaundice or cholangitis persists.
Endoscopy_UCTN_Code_CPL_1AK_2AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1ASGE Standards of Practice Committee Machicado JD Sheth SG American Society for Gastrointestinal Endoscopy guideline on the role of endoscopy in the diagnosis and management of solid pancreatic masses: Summary and recommendations Gastrointest Endosc 202410078679639387777 10.1016/j.gie.2024.06.002 · doi ↗ · pubmed ↗
- 2Elmunzer BJ Maranki JLGómez VACG clinical guideline: Diagnosis and management of biliary strictures Am J Gastroenterol 202311840542610.14309/ajg.000000000000219036863037 · doi ↗ · pubmed ↗
- 3Dumonceau JM Tringali A Papanikolaou IS Endoscopic biliary stenting: Indications, choice of stents, and results: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline – Updated October 2017 Endoscopy 20185091093030086596 10.1055/a-0659-9864 · doi ↗ · pubmed ↗
- 4Kulpatcharapong S Piyachaturawat P Mekaroonkamol P Efficacy of multi-hole self-expandable metal stent compared to fully covered and uncovered self-expandable metal stents in patients with unresectable malignant distal biliary obstruction: A propensity analysis Surg Endosc 20243821222137964091 10.1007/s 00464-023-10541-9 · doi ↗ · pubmed ↗
- 5Takahashi S Takeda T Kobayashi M Efficacy and safety of a novel multi-hole fully covered self-expandable metallic stent for malignant distal biliary obstruction: Multicenter retrospective study Dig Endosc 20253776677410.1111/den.1500640084472 · doi ↗ · pubmed ↗