Spontaneous Catheter Fracture Leading to a Retained Fragment After Central Venous Access Port Removal: Should Preoperative Chest X-rays Be Obtained?
Alexis Clare, Fuad Turfah

TL;DR
This paper discusses a rare case of a broken central venous access port during removal and suggests using chest X-rays before removal to prevent complications.
Contribution
The paper introduces a recommendation for preoperative chest X-rays to detect potential catheter fractures before port removal.
Findings
Spontaneous catheter fracture during port removal is rare but can lead to retained fragments.
A preoperative chest X-ray can help identify catheter fractures before removal.
Adhesive fibrous sheaths may complicate port removal after long-term use.
Abstract
Central venous access ports are used to administer chemotherapy, antibiotics, and total parenteral nutrition, and for frequent blood draws. The device consists of a subcutaneous reservoir (port) and an intravascular piece (catheter). Access is achieved via direct venipuncture of the subclavian, internal jugular, or cephalic vein with the tip at the cavoatrial junction. Retained central venous access ports are relatively uncommon. In most cases, an indwelling time greater than two years can cause an adhesive fibrous sheath to form around the catheter, contributing to more difficult removal. Spontaneous fracture of ports is even less common. Our goal is to discuss spontaneous catheter fracture of a central venous access port leading to a retained fragment in an adult. In this paper, we suggest obtaining a preoperative chest X-ray (CXR) in certain patients prior to central venous access…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
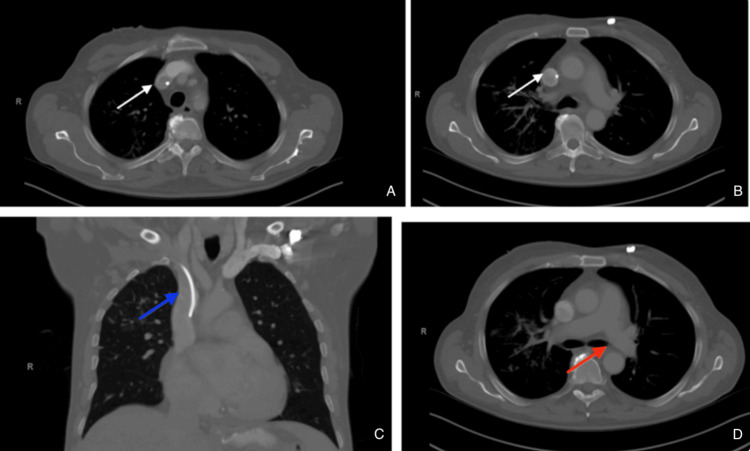 Figure 1
Figure 1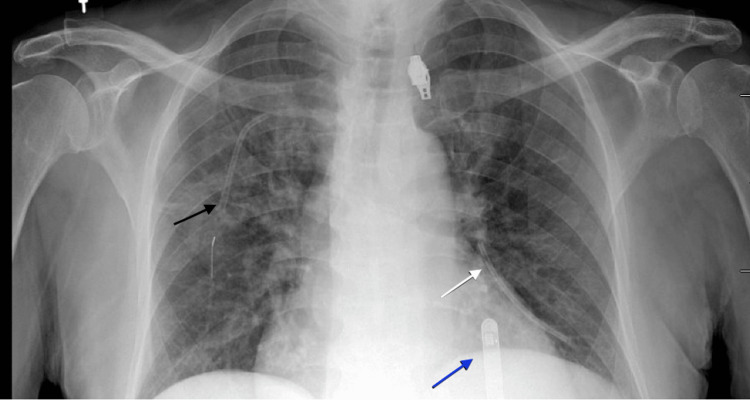 Figure 2
Figure 2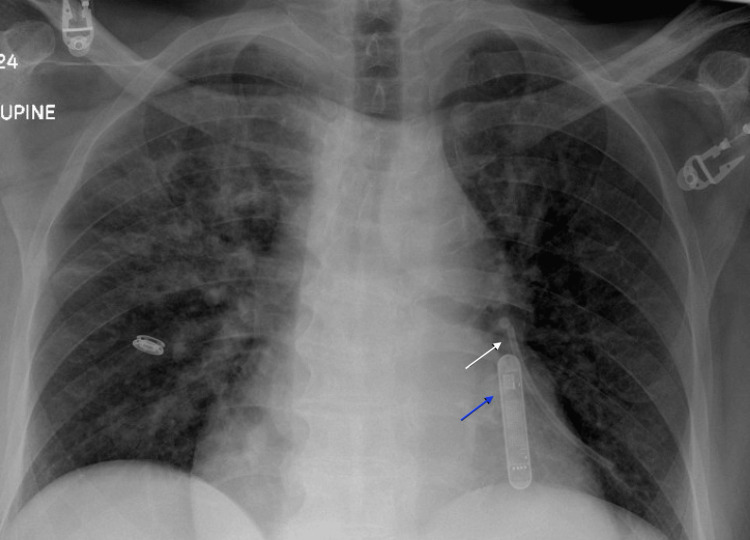 Figure 3
Figure 3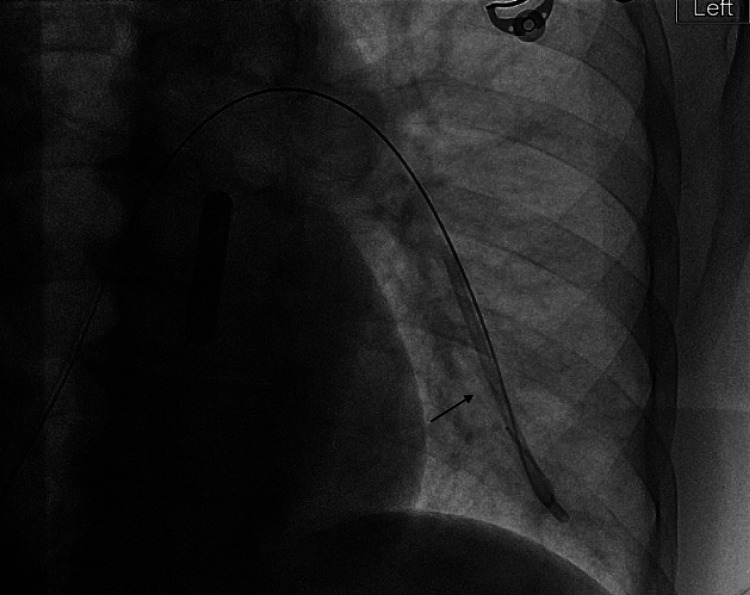 Figure 4
Figure 4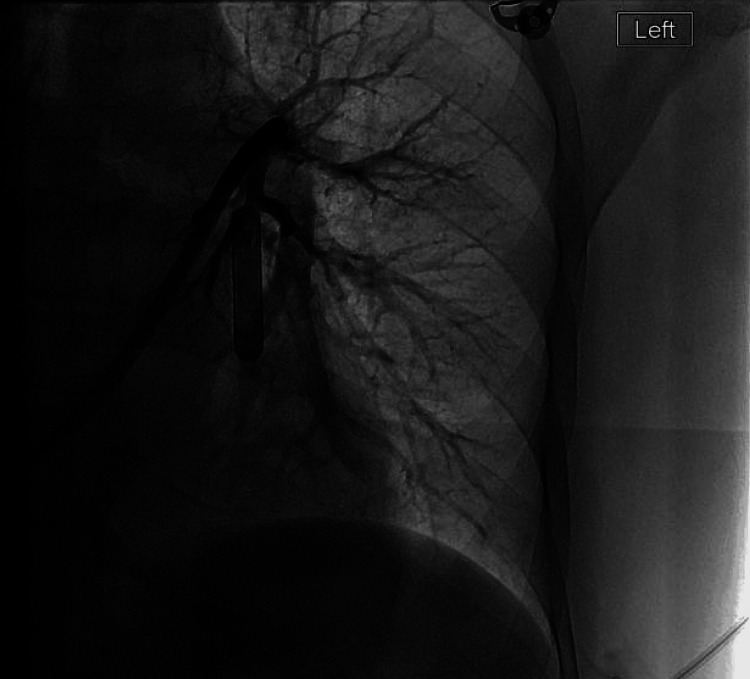 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCentral Venous Catheters and Hemodialysis · Vascular Procedures and Complications · Infection Control in Healthcare
Introduction
A portacath is a type of central venous access device that provides continuous access to a large vein in the body, usually the superior vena cava. It consists of a subcutaneous reservoir attached to a soft, flexible catheter that terminates at the junction of the superior vena cava and right atrium. The purpose of the “port” is to deliver intravenous medications and products directly into the bloodstream and to allow for frequent blood draws [1]. Central venous access ports can be removed surgically in the operating room or endovascularly in the interventional radiology suite. Port removal involves making an incision overlying the port reservoir, dissection to the reservoir and attached catheter, removal of any anchoring sutures, gentle traction to remove the catheter, and closure of the venotomy and underlying tissue [2]. Rare, but possible complications include spontaneous catheter fracture and retained catheter [3]. If one of these complications occurs, the endovascular route is typically pursued. This entails using a guidewire to endovascularly retrieve the catheter [4].
In this paper, we present the case of a retained central venous access catheter in an adult. Interestingly, the indwelling time was only six months. Upon further review of imaging, the catheter appeared to have spontaneously fractured prior to attempted removal in the operating room. We propose that reviewing any existing chest x-rays (CXRs) or obtaining a preoperative CXR prior to port removal become the standard of care in specific patient populations. This includes patients with long indwelling catheter time, greater than two years, and those who present with concern for port infection. Preoperative imaging may ultimately change the method of retrieval from surgical to endovascular at the index operation, potentially saving the patient and hospital from the cost of additional operating room fees, anesthesia, and increased length of hospital stay.
Case presentation
The patient is a 69-year-old male with a history of gastric adenocarcinoma status-post total gastrectomy with Hunt-Lawrence jejunal pouch who underwent placement of a right subclavian central venous access port (9.6F, Bard Medical, NJ, USA) for adjuvant chemotherapy and total parenteral nutrition due to cancer recurrence. Six months later, he presented to the emergency department with erythema, pain, and itching around the port site. Interestingly, an outpatient CT chest three days prior to presentation showed the central venous access catheter terminating within the superior vena cava without any evidence of fracture (Figure 1).
CT chest demonstrating appropriate placement of the catheterA and B: catheter within the right subclavian vein (marked by a white arrow); C: intact catheter terminating in the correct location near the cavoatrial junction (marked by a blue arrow); D: no evidence of a fractured piece of catheter within the left pulmonary artery (marked by a red arrow).
In the emergency department, a CXR was read as “unremarkable” (Figure 2). The following day, he was taken to the operating room for removal of his central venous access port due to concern for port site infection. Intraoperatively, there appeared to be no apparent complications. The mediport and catheter were removed easily without any aggressive traction. However, upon further inspection of the catheter tip, there appeared to be approximately 9 cm of catheter missing. A postoperative CXR was obtained and read as “retained piece of catheter in the left pulmonary artery” (Figure 3). The patient was taken the same day for successful percutaneous retrieval by interventional radiology via access through the right common femoral vein (Figure 4). A final pulmonary arteriogram demonstrated complete catheter fragment removal (Figure 5).
Preoperative chest X-rayDemonstrating the proximal central venous access catheter within the right subclavian vein (marked by a black arrow) and the distal fragmented catheter piece within the left pulmonary artery (marked by a white arrow). Existing loop recorder is in the appropriate position (marked by a blue arrow).
Postoperative chest X-rayShowing the interval removal of the catheter within the right subclavian vein. Presence of a retained catheter in the left pulmonary artery (marked by a white arrow). Preexisting loop recorder in the correct location (marked by a blue arrow).
Interventional radiology percutaneous retrieval of a retained catheter in the left pulmonary artery (marked by a black arrow) via right femoral vein access
Final pulmonary arteriogram showing complete catheter fragment removalNo injuries to the left pulmonary artery branches.
On retrospective review of imaging, the CXR obtained in the emergency department the day prior demonstrated that the catheter was dislodged within the pulmonary artery prior to taking the patient to the operating room. In our case, a review of preexisting imaging was not performed. Had we reviewed the preoperative CXR or obtained one prior to surgery, we would have sent the patient to interventional radiology instead of the operating room. Thus, avoiding additional use of resources, unnecessary anesthesia, and healthcare funds.
Discussion
Complications of central venous access ports include pneumothorax, spontaneous fracture, migration of the catheter, and even thrombosis of the vein [3]. Spontaneous fracture is exceedingly rare, reported at less than 2% [5,6]. Fracture may be attributed to the material of the catheter used (polyurethane having a higher risk of fracture), location, type of chemotherapy, and indwelling time [7]. The highest amount of compression and friction is at the space between the clavicle and first rib, also known as the costoclavicular space. This area is where spontaneous fractures most often occur. On CXR, a “pinch-off sign” (POS) may be seen where the catheter is indented as it passes beneath the clavicle. This was first characterized on CXR in 1984 by Aitken and Minton [8]. In a collective review of the literature, it was found that on average, POS occurs 5.3 months after insertion but ranges from immediately to 60 months after insertion. If the subclavian vein is used as the access point, it is recommended to cannulate lateral to the midclavicular line and obtain an interval CXR periodically to rule out POS. Specifically, one, three, and five months after placement [9]. In 1990, Hinke et al. expanded on this by defining "pinch-off syndrome," which is further classified into grades 0-3. Grade 0 is described as a smooth catheter course with no evidence of narrowing, grade 1 as a catheter course with any degree of bending or deviation but no luminal narrowing, grade 2 as some degree of luminal narrowing as it passes under the clavicle, defined as a "POS," and grade 3 as showing catheter transection between the clavicle and first rib with embolization [10]. On CXR, look for catheter migration, deviation, or the “POS,” which may allude to an impending fracture.
Retained catheters in the adult population are also rare, estimated at less than 1% [11]. In the majority of cases, a prolonged indwelling time is the main contributing factor. In a paper published by the American College of Surgeons, a duration greater than two years was considered to be the most critical risk factor for retained catheter [12]. Over time, the catheter may become fixated to the wall of the vein, forming a calcified fibrin sheath. On CXR, a fibrin sheath “cast” may be seen [13]. It is imperative to avoid forceful manual traction and unnecessary dissection, as this exponentially increases the risk of fracturing the catheter and dislodging the distal end.
Clinical symptoms of fracture or migration of the catheter include pain or swelling of the arm, chest discomfort, paresthesia, cardiac arrhythmias if it migrates into the atrium, and the inability to withdraw blood or flush the port easily [14]. Many times, patients are asymptomatic and will have a silent embolization that is found incidentally [15]. If the catheter fractures, it is imperative to remove it before a terrible complication, such as myocardial perforation, vein thrombosis, or pseudoaneurysm formation, occurs. In our case, the patient presented with pain and erythema around his port site. Final pathology and culture showed no growth, suggesting that his symptoms were secondary to a spontaneous fracture rather than infection. A CT chest three days prior confirmed the proper location of the catheter tip within the cavoatrial junction (Figure 1). The port appears to have spontaneously fractured sometime within those three days prior to hospital presentation, as the CXR in the emergency department showed catheter fragments within both the subclavian vein and the left pulmonary artery.
Early removal of central venous access ports is recommended. Removal is typically via surgical intervention. However, certain cases warrant percutaneous endovascular removal. Our case highlights the importance of having a high index of suspicion for spontaneous catheter rupture and for reviewing existing preoperative imaging prior to surgical intervention. If no imaging exists and suspicion remains high, we suggest obtaining a preoperative CXR to ensure the patient has the correct method of retrieval on the index operation.
Conclusions
Spontaneous central venous access catheter fracture and retained catheter remain relatively uncommon. Timely removal of central venous access ports when they are no longer in use and selecting the appropriate method of removal for ports with long indwelling times are important factors to consider. Consideration of preoperative CXR should be made in patients where a high index of suspicion for spontaneous fracture exists and for those who have an increased risk of port retention. Preoperative imaging may ultimately change the extraction technique at the index operation, saving the patient from unnecessary procedures and potentially saving the hospital unnecessary costs associated with the need for these additional procedures.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Portacaths JAMA Oncol West HJ Jin JO 152220162672075210.1001/jamaoncol.2015.3488 · doi ↗ · pubmed ↗
- 2A new technique to remove a "stuck" totally implantable venous access catheter J Pediatr Surg Huang SC Tsai MS Lai HS 146514674420091957368210.1016/j.jpedsurg.2009.03.033 · doi ↗ · pubmed ↗
- 3Complications of central venous port systems: a pictorial review Insights Imaging Machat S Eisenhuber E Pfarl G Stübler J Koelblinger C Zacherl J Schima W 861020193146364310.1186/s 13244-019-0770-2PMC 6713776 · doi ↗ · pubmed ↗
- 4A stepwise interventional strategy for the removal of adherent totally implanted central venous access port catheters Ann Vasc Surg Ding JY Li L Fu XR Xu L Ding PX Lee EW 16216710620243882147710.1016/j.avsg.2024.03.030 · doi ↗ · pubmed ↗
- 5Port catheter fracture and migration in internal jugular vein Am J Case Rep Doley RP Brar P Chaudhary S Bedi R Swami AC Wig JD 14161320122356947510.12659/AJCR.882293 PMC 3615937 · doi ↗ · pubmed ↗
- 6The mechanisms of failure of totally implantable central venous access system: analysis of 73 cases with fracture of catheter Eur J Surg Oncol Lin CH Wu HS Chan DC Hsieh CB Huang MH Yu JC 1001033620101970984710.1016/j.ejso.2009.07.011 · doi ↗ · pubmed ↗
- 7Polyurethane versus silicone port a cath: What's going on at removal?J Pediatr Surg Alzahrani K Lejeune J Lakhal W 141714195320182868988810.1016/j.jpedsurg.2017.06.025 · doi ↗ · pubmed ↗
- 8The "pinch-off sign": a warning of impending problems with permanent subclavian catheters Am J Surg Aitken D Minton J 6336361481984649685310.1016/0002-9610(84)90340-4 · doi ↗ · pubmed ↗