Cross-Induction of Anti-Complexing Antibodies in Patients Treated with Botulinum Toxin Formulations Containing Complexing Proteins
Yuttana Srinoulprasert, Surachet Sirisuthivoranunt, Chattip Sripatumtong, Tunsuda Tansit, Pornsuk Yamlexnoi, Onjira Meethong, Rungsima Wanitphakdeedecha

TL;DR
This study shows that botulinum toxin formulations containing complexing proteins can trigger cross-reactive antibodies, while a CP-free formulation causes minimal immune response.
Contribution
The study demonstrates cross-reactive antibody responses to complexing proteins in botulinum toxin formulations.
Findings
CP-containing formulations like OnaA, LetiA, and PraboA induce higher anti-CP antibody levels with cross-reactivity.
AboA mainly induces antibodies against its own CPs and those of PraboA.
IncoA, a CP-free formulation, shows minimal immunogenicity.
Abstract
Botulinum toxin type A (BoNT/A) formulations differ in their content of non-toxic accessory proteins, also known as complexing proteins (CPs), which may influence immunogenicity. Some BoNT/A products share structurally similar CPs, potentially leading to antibody cross-reactivity among formulations. This prospective study investigated whether patients treated with different BoNT/A products develop cross-reactive anti-CP antibody responses. One hundred participants were allocated into five treatment groups, each receiving a single BoNT/A formulation: incobotulinumtoxinA (IncoA), onabotulinumtoxinA (OnaA), abobotulinumtoxinA (AboA), letibotulinumtoxinA (LetiA), or prabotulinumtoxinA (PraboA). Each participant received 50 units or equivalent dosing. Serum samples were collected 180 days post-injection, and anti-CP antibodies were quantified using an absorption ELISA and compared with a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
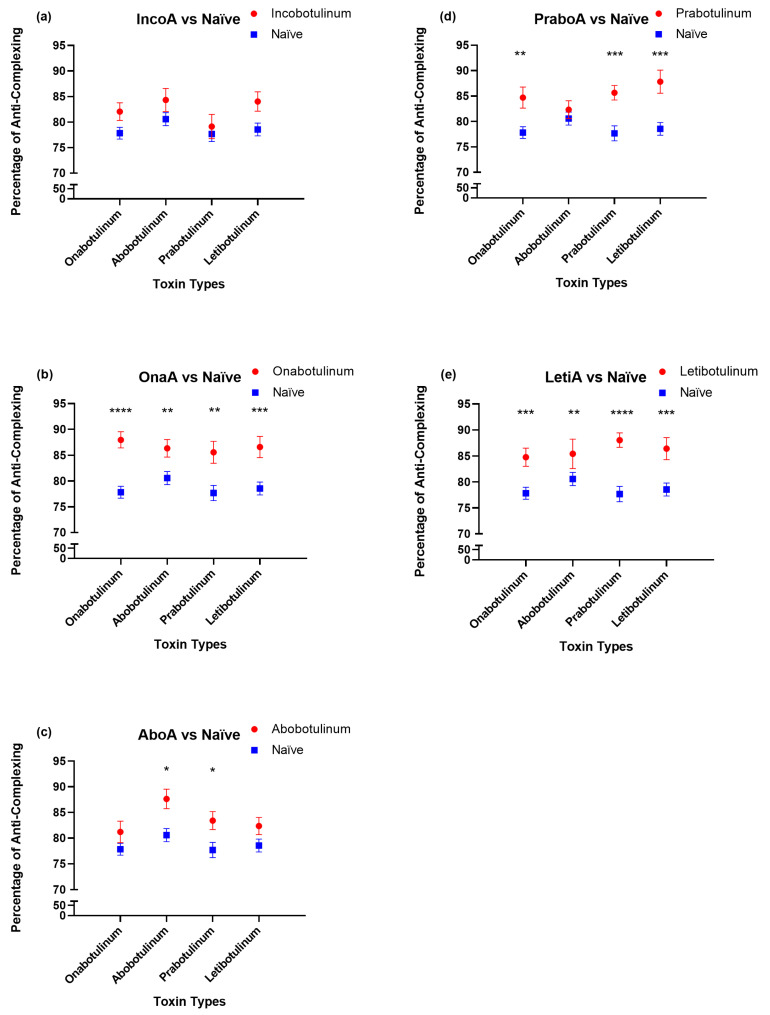 Figure 1
Figure 1- —Siriraj Foundation, Faculty of Medicine Siriraj Hospital, Mahidol University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBotulinum Toxin and Related Neurological Disorders · Facial Rejuvenation and Surgery Techniques · Diphtheria, Corynebacterium, and Tetanus
1. Introduction
Botulinum toxin type A (BoNT/A) injection has established itself as the most frequently performed minimally invasive esthetic procedure worldwide [1]. Beyond aesthetic applications, it serves as a first-line therapy for a broad spectrum of neuromuscular and autonomic disorders, including cervical dystonia, spasticity, and chronic migraine [2,3]. With the rising trend of preventative treatments in younger demographics, patients are increasingly subjected to repeated exposure over decades [4]. The toxin functions by cleaving SNAP-25 to inhibit acetylcholine release, resulting in temporary muscle paralysis [5].
Commercial BoNT/A products consist of a 150 kDa core neurotoxin, with or without additional non-toxic accessory proteins referred to as complexing proteins (CPs), including hemagglutinins and non-hemagglutinating proteins [6]. These proteins naturally surround the neurotoxin in the native bacterial complex and protect it during gastrointestinal passage in natural intoxication; however, their necessity in injectable therapeutic formulations remains debated [6,7].
Immunogenicity represents a key concern in long-term or repeated BoNT/A treatment, particularly the development of antibody responses that may compromise clinical efficacy. While the core neurotoxin itself can elicit immune recognition, CPs have been implicated as potential enhancers of immunogenicity by acting as adjuvant-like proteins [8]. Specifically, hemagglutinin components have been shown to activate Toll-like receptor 2 (TLR2) on dendritic cells, triggering pro-inflammatory signaling [9]. Repeated exposure to CP-containing formulations may therefore increase the likelihood of antibody formation, potentially contributing to secondary treatment failure [6,7,8]. Recent meta-analyses estimate the prevalence of neutralizing antibodies in esthetic indications to range between ~0.2% and ~0.5%, with higher rates observed in therapeutic uses [10].
Currently available BoNT/A products differ markedly in their CP content. OnabotulinumtoxinA, abobotulinumtoxinA, letibotulinumtoxinA, and prabotulinumtoxinA contain varying amounts and compositions of CPs, whereas incobotulinumtoxinA is purified to contain only the core neurotoxin without CPs [7,8,11]. Structural similarities among CPs derived from different formulations may facilitate antibody cross-reactivity, whereby antibodies generated against one formulation recognize CPs from another. Such cross-reactivity could limit the effectiveness of switching between BoNT/A products in patients with suspected immunogenic resistance.
Although anti-CP antibodies have been detected in BoNT/A non-responders using absorption ELISA techniques [12], the extent and pattern of cross-reactivity among CPs from different commercial BoNT/A formulations have not been systematically evaluated in humans. Therefore, this study aimed to investigate whether treatment with specific BoNT/A formulations induces anti-CP antibodies that cross-react with [1] CPs from other formulations, thereby providing clinically relevant insight into formulation-specific immunogenicity.
2. Results
2.1. Patient Population and Characteristics
A total of 137 participants were enrolled, including five BoNT/A treatment groups (n = 20 per group) and a toxin-naïve control group (n = 37). All participants were Thai adults aged 18–60 years, with a predominance of female subjects (92.7%). Mean ages were comparable across groups, ranging from 33.45 ± 8.33 to 38.7 ± 8.72 years, with no statistically significant differences. None of the participants exhibited clinical BoNT/A treatment failure during follow-up. Demographic characteristics are summarized in Table 1.
2.2. Anti-Complexing Protein Antibody Responses
Anti-CP antibody levels differed markedly among BoNT/A formulations (Figure 1). Sera from participants treated with OnaA and LetiA demonstrated significantly elevated anti-CP antibody levels against all tested BoNT/A formulations compared with the toxin-naïve group (p ≤ 0.01 to p ≤ 0.0001), indicating broad cross-reactivity. PraboA treatment also induced elevated antibody responses with cross-reactivity against CPs from other formulations, particularly abobotulinumtoxinA and letibotulinumtoxinA.
In contrast, AboA treatment resulted in a more restricted antibody profile, with a modest but significant increase in antibodies primarily directed against its own CPs and those of PraboA (p < 0.05). Notably, participants treated with IncoA did not demonstrate any significant increase in anti-CP antibody levels relative to toxin-naïve controls, indicating minimal immunogenicity with respect to CPs (Figure 1).
Collectively, these findings reveal distinct formulation-specific immunogenic profiles, ranging from broad cross-reactive responses to minimal antibody induction, depending on CP composition.
3. Discussion
This prospective clinical study provides direct human evidence that BoNT/A formulations containing complexing proteins can induce cross-reactive antibody responses against CPs derived from other commercial products. In contrast, the CP-free formulation incobotulinumtoxinA demonstrated minimal immunogenicity, with antibody levels comparable to those observed in toxin-naïve individuals. These findings extend previous observations regarding CP-associated immunogenicity and provide new insight into cross-formulation immune recognition.
The broad cross-reactivity observed among OnaA, LetiA, and PraboA suggests that these formulations may share structurally similar CP components, which are recognized by the immune system across products [13,14,15]. Manufacturing processes, bacterial strains, and purification techniques are likely to influence CP composition and may account for the observed immunogenic similarities. Conversely, abobotulinumtoxinA exhibited a more limited cross-reactive profile, possibly reflecting differences in molecular weight distribution and CP structure [14]. This distinct immunological signature may have implications for product switching strategies, although further validation is required.
It is important to distinguish between antibodies directed against complexing proteins and neutralizing antibodies against the 150 kDa core neurotoxin. While anti-CP antibodies do not necessarily equate to functional neutralization of BoNT/A activity, their presence reflects increased antigenic exposure and may predispose patients to broader immune recognition with repeated treatments.
Additionally, the detection of heterogeneity levels of anti-CP antibody in individuals may be explained by molecular mimicry. It is well-established that the human immune system is frequently primed by exposure to various Clostridium species within the commensal gut microbiota or through environmental contact. Furthermore, standard immunization protocols, such as the tetanus toxoid vaccine, involve proteins that share high structural homology with botulinum neurotoxins [16]. These prior exposures can induce a population of memory B cells and circulating antibodies that recognize conserved, structurally related epitopes on the complexing proteins of BoNT/A. These pre-existing antibodies account for the heterogeneity of basal hIgG levels observed across our study cohorts. To account for this individual variability and to ensure that our data reflected the specific immunogenic impact of the BoNT/A formulations rather than baseline cross-reactivity, we therefore expressed anti-CP IgG levels as a percentage of the individual’s own basal whole-toxin IgG.
Several limitations should be acknowledged. First, this was a single-center study conducted in a homogeneous Thai population, which may limit generalizability. However, this approach minimized confounding factors related to genetic and procedural variability and provides valuable data for an underrepresented population. Second, the sample size was designed to identify immunological patterns rather than to determine the precise incidence of clinical immunoresistance. Finally, although absorption ELISA enables selective assessment of anti-CP antibodies, functional neutralization assays were not performed; therefore, direct correlations with clinical non-response cannot be conclusively established.
From a clinical perspective, understanding formulation-specific immunogenicity is crucial when selecting BoNT/A products for patients requiring repeated treatment. In cases of suspected antibody-mediated treatment failure, immunological testing may inform product choice. When antibody involvement is confirmed or suspected, CP-free formulations such as incobotulinumtoxinA may offer a rational alternative with a lower risk of further immune stimulation [12].
4. Conclusions
BoNT/A formulations containing complexing proteins induce cross-reactive antibody responses that may contribute to immunogenic resistance with repeated exposure. IncobotulinumtoxinA, which lacks complexing proteins, exhibits minimal immunogenicity and may be preferentially considered for patients requiring long-term or repeated BoNT/A treatment.
5. Materials and Methods
5.1. Study Objectives
This study aimed to investigate the presence and cross-reactivity of antibodies against CPs in sera from patients treated with different BoNT/A formulations
5.2. Experimental Design and Population
This pilot study was conducted at a single-center, prospective study with five parallel treatment groups and one naïve control group to study antibody responses in humans. One hundred thirty-seven Thai people (males and females) aged 18 to 60 years old were included in the study. They were divided into naïve group (37 people), which are the people who never received botulinum toxin injection before and treatment groups which received the botulinum toxin treatment. Participants were excluded if they had received botulinum toxin injections within 90 days before study initiation, had underlying immunological diseases, or had a documented history of treatment non-response to BoNT/A.
Serum samples used in this study were derived from participants of a previously published study entitled “A Pilot Study of Differences in Antibody Responses of Intradermal and Intramuscular Injections of Botulinum Toxin Type A.” [17]. Written informed consent for serum storage and future use in subsequent research projects was obtained from all participants.
The sample size was appropriate for the exploration objectives of this study. The primary aim was not to establish the precise incidence of immunoresistance to BoNT/A with high statistical power, but rather to identify the existence and characterize the patterns of antibody cross-reactivity across different BoNT/A formulations. This sample size provides sufficient resolution to detect strong, clinically relevant immunological signals and is consistent with sample sizes used in prior foundational studies of immunogenicity [18]. Given the logistical challenges of recruiting patients with specific BoNT/A treatment histories and suspected immunogenic resistance, this sample size represents a practical and ethically sound approach for this initial investigation.
Participants in the treatment arm were evenly assigned into five groups (n = 20 per group), with each group receiving a different commercially available BoNT/A formulation: IncoA (Xeomin, Merz Pharma, Frankfurt, Germany), OnaA (Botox, Irvine, CA, USA), AboA (Dysport, Ipsen Ltd, Paris, France), LetiA (Hugel, Hugel, Inc., Chuncheon-si, Gangwon-do, South Korea), or PraboA (Nabota, Daewoong Pharmaceutical Co., Ltd., Seoul, South Korea). All BoNT/A products were obtained from the same lot and batch to ensure consistency throughout the study. Each participant received an injection of 50 units of BoNT/A or an equivalent dose; for AboA, a dose of 125 units was administered in accordance with established conversion ratios [19]. Treatments were performed for esthetic indications, including facial lifting or facial contouring.
5.3. Subject Sample Collection and Preparation
Stored serum samples from participants enrolled in the previously published study were used for the present analysis. For the naïve group, serum samples were obtained from baseline blood collections of individuals who had never received botulinum toxin injections. For the treatment group, serum samples collected at 180 days post-BoNT/A injection were analyzed. The 180-day time point was selected because patients commonly receive repeat BoNT/A injections around this interval [20], and this time frame allows for the evaluation of antibody development and persistence.
The study aimed to detect the presence of antibodies against complexing proteins (CPs) of each BoNT/A formulation at 180 days and to assess their potential cross-reactivity with CPs from other products. Blood samples in the original study were centrifuged at 1000 rpm for 10 min at room temperature, and the serum was stored at −20 °C. Prior to analysis, serum samples were transferred to 4 °C one day before use.
5.4. ELISA for Detection of Human Anti-Complexing Protein Antibodies (Absorption ELISA)
An absorption enzyme-linked immunosorbent assay (ELISA), developed by our group, was employed to quantify human IgG (hIgG) antibodies specific to the complexing proteins of BoNT/A. Briefly, two 96-well microplates (Corning, NY, USA) were prepared and designated as absorption plates and working plates. Absorption plates were coated overnight (16–18 h) at 4 °C with IncoA (0.028 units/mL; 50 μL/well). Working plates were similarly coated with IncoA (0.028 units/mL), LetiA (0.02 units/mL), AboA (0.116 units/mL), OnaA (0.02 units/mL), or PraboA (0.134 units/mL). Following washing, absorption plates were blocked with 1% bovine serum albumin (BSA, Merck KGaA, Darmstadt, Germany) and incubated at 37 °C for 1 h. Patient sera, diluted 1:50, were added to the absorption plates and incubated at 37 °C for 1 h; this absorption step was performed twice. Absorbed sera, together with freshly diluted unabsorbed sera, were subsequently transferred to BSA-blocked working plates and incubated at 37 °C for 1 h. After washing, horseradish peroxidase–conjugated rabbit anti-human IgG (Agilent Technologies, Santa Clara, CA, USA) was added, followed by tetramethylbenzidine substrate (Dako, Glostrup, Denmark) for color development. The reaction was terminated with 1 N HCl, and absorbance was measured at 450 nm [21]. Sera contain antibodies recognizing both core botulinum toxin and complexing proteins. Absorbed sera without antibodies specific to core botulinum toxin may mostly contain antibodies specific against complexing proteins. The amount of hIgG specific to complexing proteins was calculated by subtracting the levels of hIgG from unabsorbed samples from those of absorbed samples. Due to the heterogeneity of basal levels of hIgG specific to whole BoNT/A (including core and complexing proteins) among individuals, we normalized the amount of hIgG specific to complexing proteins by their corresponding basal levels of hIgG specific to whole BoNT/A, expressing the results as a percentage of anti-complexing protein IgG. The antibodies that were used in the project is shown in Table S3.
5.5. Statistical Analysis
Statistical analyses were conducted using GraphPad Prism version 9.5.0. Descriptive statistics were applied to demographic data. Comparisons between toxin-naïve and treated groups were performed using an unpaired t-test for parametric data or the Mann–Whitney U test for non-parametric data. A p value ≤ 0.05 was considered statistically significant.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1International Society of Aesthetic Plastic Surgery ISAPS Global Survey on Aesthetic/Cosmetic Procedures Available online: https://www.isaps.org/discover/about-isaps/global-statistics/(accessed on 6 February 2026)
- 2Jankovic J. Botulinum toxin in clinical practice J. Neurol. Neurosurg. Psychiatry 20047595195710.1136/jnnp.2003.03470215201348 PMC 1739107 · doi ↗ · pubmed ↗
- 3Nigam P.K. Nigam A. Botulinum toxin Indian J. Dermatol.20105581410.4103/0019-5154.6034320418969 PMC 2856357 · doi ↗ · pubmed ↗
- 4Michon A. Botulinum toxin for cosmetic treatments in young adults: An evidence-based review and survey on current practice among aesthetic practitioners J. Cosmet. Dermatol.20232212813910.1111/jocd.1551336445847 · doi ↗ · pubmed ↗
- 5Pirazzini M. Rossetto O. Eleopra R. Montecucco C. Botulinum Neurotoxins: Biology, Pharmacology, and Toxicology Pharmacol. Rev.20176920023510.1124/pr.116.01265828356439 PMC 5394922 · doi ↗ · pubmed ↗
- 6Martin M.U. Frevert J. Tay C.M. Complexing Protein-Free Botulinum Neurotoxin A Formulations: Implications of Excipients for Immunogenicity Toxins 20241610110.3390/toxins 1602010138393178 PMC 10892905 · doi ↗ · pubmed ↗
- 7Frevert J. Dressler D. Complexing proteins in botulinum toxin type A drugs: A help or a hindrance?Biologics 2010432533210.2147/BTT.S 1490221209727 PMC 3010823 · doi ↗ · pubmed ↗
- 8Berweck S. Banach M. Gaebler-Spira D. Chambers H.G. Schroeder A.S. Geister T.L. Althaus M. Hanschmann A. Vacchelli M. Bonfert M.V. Safety Profile and Lack of Immunogenicity of Incobotulinumtoxin A in Pediatric Spasticity and Sialorrhea: A Pooled Analysis Toxins 20221458510.3390/toxins 1409058536136523 PMC 9505819 · doi ↗ · pubmed ↗