Predictive Value of Sustained Virologic Response at Week 4 in Patients with Hepatitis C Virus Infection Treated with Sofosbuvir/Velpatasvir
Gia Landry, Mark Sulkowski, Jordan J. Feld, Nancy Reau, Stacey Scherbakovsky, Farrah Black, Candido Hernández, Renee-Claude Mercier, Liyun Ni, Marc Bourlière, Alessandra Mangia

TL;DR
This study shows that checking for a hepatitis C cure at week 4 instead of week 12 after treatment is reliable and could help patients stay in care.
Contribution
The study demonstrates that SVR4 is a valid predictor of SVR12 in patients treated with SOF/VEL, supporting earlier cure confirmation.
Findings
In clinical trials, 99.7% of patients who achieved SVR4 also achieved SVR12.
In real-world data, 94% of patients achieved SVR4 and 95% achieved SVR12, with high concordance between the two.
Shifting cure confirmation to week 4 could reduce patient loss to follow-up.
Abstract
Direct-acting antiviral therapies can cure most people with hepatitis C virus (HCV) infection with little need for testing or monitoring. A major challenge to eliminating HCV is ensuring patients complete all steps of care, including confirmation of cure. We assessed the concordance of sustained virologic response (SVR) at 4 weeks (SVR4) and 12 weeks (SVR12) post-treatment to evaluate the viability of SVR4 as a predictor of cure in patients treated with sofosbuvir (SOF)/velpatasvir (VEL). We conducted a retrospective analysis of patients from the Phase 3 ASTRAL-1, -2, and -3 programs and a historical cohort from the Louisiana Department of Health Sexually Transmitted Infection (STI)/HIV/Hepatitis Program claims database. Concordance analyses were performed for patients with both SVR4 and SVR12 data. The concordance analysis in the ASTRAL studies included 1015 patients; 1005 and 1002…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
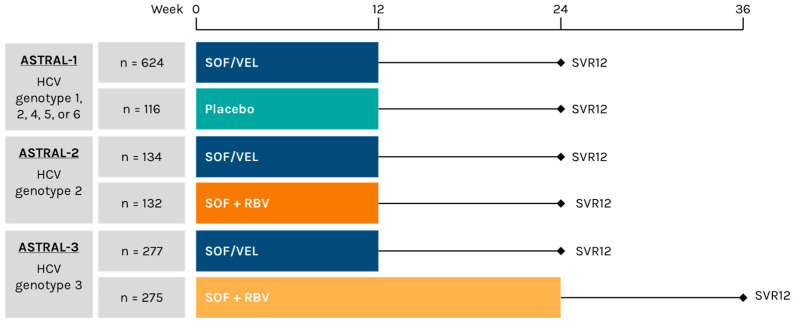 Figure 1
Figure 1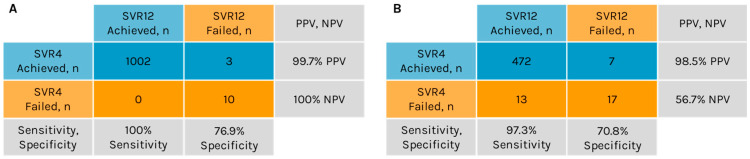 Figure 2
Figure 2- —Gilead Sciences, Inc.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatitis C virus research · HIV/AIDS drug development and treatment · HIV-related health complications and treatments
1. Introduction
Chronic hepatitis C virus (HCV) infection can lead to cirrhosis, decompensated liver disease, and hepatocellular carcinoma [1]. According to the World Health Organization (WHO), approximately 50 million people worldwide have chronic HCV infection, with an estimated 1 million individuals newly infected each year [2]. Over the past decade, direct-acting antiviral (DAA) therapies have revolutionized HCV treatment, offering a combination of high efficacy, safety, tolerability, and simplicity [1,3]. The WHO set a target to eliminate HCV as a public health threat by 2030, and the availability of DAA therapies has made this goal achievable [4].
International guidelines for HCV treatment recommend pangenotypic DAA regimens, such as glecaprevir/pibrentasvir or sofosbuvir (SOF)/velpatasvir (VEL) [5,6,7]. These regimens have enabled most patients who are diagnosed and access treatment to achieve a cure with minimal pretreatment testing and on-treatment monitoring [7,8,9]. The WHO, the American Association for the Study of Liver Diseases and the Infectious Diseases Society of America (AASLD-IDSA), and the European Association for the Study of the Liver (EASL) have endorsed the simplification of treatment as part of a global call to action for HCV elimination [5,6,7,10].
While DAA regimens and simplified guidelines have streamlined HCV testing and treatment, ensuring effective follow-up and confirmation of cure remains crucial, particularly for individuals with high-risk behaviors or those susceptible to reinfection [5,7]. Although EASL guidelines suggest that sustained virologic response (SVR) testing can be omitted in some cases [5], it also provides an opportunity to counsel patients on the risk of reinfection and the importance of regular testing for those with ongoing risk factors [4,11]. Patient loss to follow-up (LTFU), especially during treatment, is a major barrier in the care cascade; LTFU rates among patients with HCV are commonly reported to be near 10%, although rates as high as 65% have been observed [12,13,14,15]. Risk factors for LTFU include male sex, younger age, drug or alcohol use disorder, psychiatric illness, and housing insecurity [12,16,17,18].
Simplifying HCV treatment is particularly important for marginalized populations, who often face significant barriers to accessing care [6,19]. Groups such as people who inject drugs, those experiencing homelessness, and those with a history of incarceration are disproportionately affected by HCV [20,21,22]. An estimated 52% to 67% of people who inject drugs are infected with HCV [4,20,21]. In prisons worldwide, the prevalence of HCV infection can exceed 10%, with some countries having rates as high as 32% [23,24].
HCV cure was historically defined as achieving SVR with undetectable HCV RNA at 24 weeks after treatment completion (SVR24) [25]. However, studies demonstrating a strong concordance between SVR at 12 weeks (SVR12) and SVR24, particularly with treatments such as interferon monotherapy and pegylated interferon plus ribavirin [26,27], have shown that virologic relapse beyond SVR12 is rare, leading to the adoption of SVR12 as a standard endpoint for cure [5]. EASL and AASLD-IDSA guidelines now define HCV cure based on either SVR12 or SVR24, while the Food and Drug Administration uses SVR12 [5,7,28].
Strong concordance between SVR at 4 weeks (SVR4) and SVR12 has been shown for several DAA regimens, including glecaprevir/pibrentasvir [29,30,31], ledipasvir/SOF [30,31], and SOF/VEL [30,31,32]. Australia and Saudi Arabia have introduced guidelines recommending the use of SVR4, particularly for patients at risk of LTFU [33,34]. The International Network on Health and Hepatitis in Substance Users (INHSU)—Prisons has implemented global guidelines recommending the use of SVR4 in prison settings [35]. Additionally, AASLD-IDSA guidance acknowledges SVR4 as an acceptable alternative time point to assess HCV cure for people without cirrhosis or prior DAA exposure [36,37].
A recent study of global HCV treatment patterns estimated that approximately 12.7 million people across 119 countries received DAA therapy between 2014 and 2023 [38]. Of these, roughly 11.1 million (87%) were treated with a SOF-based regimen. Given the global burden of chronic HCV, estimated at 50 million people [2], this suggests that approximately three-quarters of those affected have yet to receive DAA treatment. Furthermore, 67% of DAA treatments during this period were concentrated in just 4 regions: Egypt, Pakistan, the United States, and the European Union [38]. These findings indicate there is an ongoing need to improve DAA accessibility and simplify HCV treatment worldwide. In this study, we evaluated the concordance of SVR4 with SVR12 in patients receiving SOF/VEL in the ASTRAL-1, -2, and -3 Phase 3 randomized clinical trials (RCTs) as well as in a real-world setting by utilizing Medicaid claims from the Louisiana Department of Health Sexually Transmitted Infection (STI)/HIV/Hepatitis Program administrative claims database. Our objective was to assess the predictive value of SVR4 for HCV cure for patients treated with SOF/VEL in an RCT and a real-world setting.
2. Materials and Methods
2.1. Randomized Clinical Trials
HCV RNA data from patients enrolled in ASTRAL-1 (NCT02201940), ASTRAL-2 (NCT02220998), and ASTRAL-3 (NCT02201953) were evaluated. Patients in ASTRAL-1 were enrolled at 81 sites in the United States, Canada, Europe, and Hong Kong [39]. ASTRAL-2 enrolled patients at 51 sites in the United States, and ASTRAL-3 enrolled patients at 76 sites in the United States, Canada, Europe, Australia, and New Zealand [40]. The study designs are shown in Figure 1; detailed methodologies for each study were published previously [39,40]. Participants in ASTRAL-4, which enrolled patients with decompensated cirrhosis [41], and ASTRAL-5, which enrolled patients with HCV and HIV-1 coinfection [42], were excluded. SVR was defined as an HCV RNA level below the lower limit of quantitation (15 IU/mL) 12 weeks after treatment, as measured by the COBAS AmpliPrep/COBAS TaqMan HCV Quantitative Test, version 2.0 (Roche Molecular Diagnostics, Pleasanton, CA, USA).
For the ASTRAL-1, -2, and -3 studies, eligible patients were aged 18 years or older and had chronic HCV infection with HCV genotype (GT) 1, 2, 3, 4, 5, or 6 [39,40]. Patients could be either treatment-naïve or treatment-experienced, with treatment-experienced patients defined as those who had previously failed a regimen containing interferon, with or without ribavirin, and completed treatment at least 8 weeks prior to baseline (day 1). The ASTRAL-1, -2, and -3 protocols aimed to enroll approximately 20% treatment-experienced patients and allowed for approximately 20% of participants to have compensated cirrhosis.
Exclusion criteria for the ASTRAL-1, -2, and -3 RCTs included current or historical evidence of hepatic decompensation or a diagnosis of hepatocellular carcinoma. Patients who had discontinued any prior HCV treatment due to an adverse event or who had previously been treated with any nucleotide analog HCV nonstructural protein 5B (NS5B) inhibitor or any NS5A inhibitor were not eligible for enrollment. For this analysis, all patients enrolled in ASTRAL-1, -2, or -3 were included, although concordance analyses only included those with both SVR4 and SVR12 data.
All trials were conducted in accordance with the International Conference on Harmonisation Good Clinical Practice guidelines, the Declaration of Helsinki, and local regulations. The protocols were approved by the relevant institutional review boards or independent ethics committees.
2.2. Real-World Data
A historical cohort was analyzed using comprehensive medical and pharmacy Medicaid claims from the Louisiana Department of Health STI/HIV/Hepatitis Program administrative claims database, covering the period from 15 July 2019 to 31 December 2024. This hepatitis surveillance program collects detailed information, including patient demographics (e.g., sex, gender, age, ethnicity, and race), diagnostic testing information (e.g., results of HCV antibody tests, qualitative and quantitative HCV RNA tests, and HCV GT), and clinical data (e.g., comorbid conditions, pregnancy status, medications taken, dates of use, and duration). Only treatment-naïve patients were included in the cohort.
The cohort for this analysis included adults aged 18 years or older enrolled in Medicaid who had at least 1 HCV diagnosis (chronic or acute) and who initiated SOF/VEL treatment during the study period. Patients with cirrhosis were not excluded. Measurements of SVR4 were taken between 4 and 6 weeks post-treatment, while measurements of SVR12 were taken at least 10 weeks post-treatment. For the concordance analysis, only patients with both SVR4 and SVR12 data were included.
As the data obtained from the Louisiana Department of Health are de-identified and publicly available, this analysis does not involve human subjects research and therefore did not require approval by an institutional review board.
2.3. Statistical Analysis
Concordance analyses included only patients treated with SOF/VEL who had both SVR4 and SVR12 data, with no imputation of missing data. Positive predictive value (PPV) was defined as the proportion of patients achieving SVR12 among those with SVR4. Negative predictive value (NPV) was defined as the proportion of patients not achieving SVR12 among those who did not achieve SVR4. Sensitivity was calculated as the proportion of patients achieving SVR4 among those achieving SVR12. Specificity was calculated as the proportion of patients not achieving SVR4 among those not achieving SVR12. All statistical analyses were performed using SAS software version 9.4.
3. Results
3.1. Randomized Clinical Trial Data from the ASTRAL Trials
A total of 1035 patients received SOF/VEL in the ASTRAL-1, -2, and -3 studies. The majority were male, and the mean age was 53 years; 28% were treatment-experienced, and 21% had cirrhosis (Table 1). All HCV GTs were represented, with the most common being GT1 (32%), GT2 (23%), and GT3 (27%).
Among the 1035 patients who received SOF/VEL, 20 did not achieve SVR12. Of these, 12 patients experienced virologic relapse, 1 was reinfected, 4 were LTFU, 1 discontinued SOF/VEL treatment, 1 withdrew consent, and 1 died, with the death considered unrelated to treatment. Among the 13 patients who relapsed or were reinfected, 10 experienced these events by post-treatment week 4, and 3 by week 12 (Table 2). Of the 10 patients who relapsed or were reinfected before post-treatment week 4, 8 had HCV GT3 and 1 each had HCV GT1a and GT1b. All patients who relapsed or were reinfected between post-treatment weeks 4 and 12 had HCV GT3a. Additionally, 8 of these 13 patients had compensated cirrhosis, and 8 had prior treatment with pegylated interferon plus ribavirin.
A concordance analysis for SVR4 and SVR12 was conducted for 1015 patients with available data. Of the 1005 patients who achieved SVR4, 1002 also achieved SVR12, yielding a PPV of 99.7% for SVR4 in predicting SVR12 (Figure 2A). Among the 10 patients who did not achieve SVR4, none attained SVR12, resulting in an NPV of 100% for SVR4 in predicting SVR12. Sensitivity, defined as the proportion of true positive outcomes, was 100% (1002/1002), while specificity, defined as the proportion of true negative outcomes, was 76.9% (10/13).
3.2. Real-World Data from the Louisiana Department of Health STI/HIV/Hepatitis Program
3.2.1. Patient Demographics
A real-world analysis of 11,299 patients with HCV who were treated with SOF/VEL was conducted using data collected by the Louisiana Department of Health STI/HIV/Hepatitis Program. The majority of patients were male (60%), and the mean age was 47 years (Table 1). All patients were treatment-naïve. GT data were available for 10,704 (95%) patients; all HCV GTs were represented except GT5, with GT1 being the most prevalent (78%). Of the 11,299 patients, 702 (6%) and 8005 (71%) had SVR4 and SVR12 data available, respectively, while 509 (5%) had both (Table 3). Among the 702 patients with SVR4 data, 659 (94%) achieved SVR4, while 43 (6%) had virologic relapse or reinfection at week 4. For the 8005 patients with SVR12 data, 7405 (93%) achieved SVR12, and 600 (7%) had virologic relapse or reinfection at week 12.
3.2.2. Concordance of SVR4 and SVR12
Data for both SVR4 and SVR12 were available for 509 patients, who were included in the concordance evaluation. The median (range) timing of SVR4 and SVR12 measurements for these patients was 5 (4–6) and 22 (10–256) weeks post-treatment, respectively. The majority were male, and the mean age was 47 years (Table 1). As in the overall cohort, all HCV GTs except for GT5 were represented in the concordance analysis population, with GT1 being the most common (59%). Overall, patient demographics and disease characteristics among the 509 patients with both SVR4 and SVR12 data available were similar to those of the overall population of patients with HCV.
Among the 509 patients, 479 (94%) achieved SVR4 (Table 3). Of those who achieved SVR4, 472 also achieved SVR12, resulting in a PPV of 98.5% for SVR4 as a predictor of SVR12 (Figure 2B). Of the 30 patients who did not achieve SVR4, 17 also did not attain SVR12, while the remaining 13 patients did achieve SVR12, resulting in an NPV of 56.7% for SVR4 as a predictor of SVR12. The sensitivity and specificity of SVR4 for predicting SVR12 were 97.3% (472/485) and 70.8% (17/24), respectively.
Of the 509 patients analyzed, 30 (6%) did not achieve SVR4, and 24 (5%) did not achieve SVR12. Thirteen patients did not achieve SVR4 but subsequently attained SVR12; of these, 12 (92%) were male, 11 (85%) were White, and 2 (15%) had cirrhosis (Table 4). Among the 24 patients who did not achieve SVR12, 7 achieved SVR4 and subsequently failed to achieve SVR12, and 17 did not achieve SVR4 or SVR12. Of these 24 patients, 19 (79%) were male, 11 (46%) were White, 9 (38%) were Black, and 5 (21%) had cirrhosis.
Of the 7 patients who achieved SVR4 but not SVR12, the median (range) timing to SVR12 testing was 43 (13–101) weeks. This was an almost 2-fold increase compared with the overall cohort with both SVR4 and SVR12 testing, in which the median (range) time to SVR12 testing was 22 (10–256) weeks. There were also increased percentages of people with substance use disorder (43%) and opioid use disorder (71%) among those who achieved SVR4 but not SVR12 compared with the overall cohort with SVR4 and SVR12 testing, in which 207 (41%) and 197 (39%) patients had substance and opioid use disorders, respectively (Table 1 and Table 4).
4. Discussion
Treatment with SOF/VEL has been shown to be highly effective in both clinical trials and real-world cohorts, benefiting diverse populations and positively impacting patient-reported outcomes [39,40,43,44,45,46,47,48,49,50]. Furthermore, SOF/VEL is well tolerated, with an extensive body of evidence supporting its safety in the treatment of chronic HCV infection [43,44,45,46,49].
We observed high concordance between SVR4 and SVR12 among patients treated with SOF/VEL in the ASTRAL program. Only 3 (0.3%) of the 1005 patients achieving SVR4 subsequently failed to achieve SVR12. All 3 of these patients had HCV GT3a; 2 had previously been treated with pegylated interferon plus ribavirin, and 2 had compensated cirrhosis. At 12 weeks post-treatment, each of these patients had HCV RNA levels greater than 5.1 log_10_ IU/mL (Table 2). In total, 12 patients who received SOF/VEL in the ASTRAL RCTs experienced virologic relapse. Additionally, 1 patient with HCV GT3a had a confirmed GT1a reinfection between post-treatment weeks 4 and 12.
Similar results were observed in the real-world data, which showed high concordance (98.5% PPV) between SVR4 and SVR12 in patients treated with SOF/VEL. Of 479 patients who achieved SVR4, 7 did not achieve SVR12. Among these 7 patients, 5 (71%) had opioid use disorder, 3 (43%) had substance use disorder, and 2 (29%) were coinfected with HIV. While the rate of HCV recurrence is low in most patients who achieve SVR [51], high-risk groups, including men who have sex with men, people coinfected with HIV, and people who inject drugs, have been shown to have higher rates of recurrence, most often due to reinfection [52,53,54]. Given that most of the 7 patients who achieved SVR4 but not SVR12 engaged in high-risk behaviors, these patients may have experienced reinfection rather than relapse. This possibility is further supported by the observation that the median time to SVR12 testing in this group was almost 2-fold longer than among all patients with both SVR4 and SVR12 testing, allowing more time for reinfection to occur. In people with ongoing high-risk behaviors, it is important to test for reinfection at least annually, regardless of whether SVR4 or SVR12 is used to document cure [11].
The PPV of SVR4 for predicting SVR12 was high for both the ASTRAL Phase 3 RCTs and the real-world program. However, the NPV was substantially lower in the real-world data (56.7%) than in the RCTs (100%). Of the 30 patients in the real-world data who did not achieve SVR4, 13 went on to achieve SVR12. It has been shown that some patients who relapse after DAA therapy will subsequently spontaneously clear HCV without additional therapy [55]. In the current study, post-treatment HCV RNA levels were unavailable for the patients who achieved SVR12, but not SVR4; however, these patients may have had very low HCV RNA levels at post-treatment week 4 and experienced spontaneous clearance by week 12. This highlights the importance of confirming SVR before initiating retreatment in patients who do not achieve SVR4, as some may still clear the virus by SVR12. The specificity of SVR4 for predicting SVR12 was also lower in the real-world data (70.8%) than in the RCTs (76.9%), but the sensitivity of SVR4 for predicting SVR12 was similar in both the RCTs and real-world data.
The high concordance observed between SVR4 and SVR12, both in Phase 3 RCTs and in the real-world dataset, supports the use of SVR4 as an indicator of HCV cure in patients treated with SOF/VEL. Adoption of SVR4 as an endpoint in HCV care would be consistent with the global efforts to simplify HCV treatment endorsed by the WHO, AASLD-IDSA, and EASL [5,6,7,10]. In addition to minimizing the risk of patients being LTFU, use of SVR4 instead of SVR12 could reduce the number of follow-up appointments required for patients who received SOF/VEL treatment, potentially lowering the cost of care for patients. Importantly, such a change would necessitate that healthcare providers counsel patients on the risk of HCV reinfection and the importance of regular testing for those with ongoing risk factors at the 4-week follow-up appointment.
Our study has several limitations. First, the ASTRAL-1, -2, and -3 Phase 3 RCTs excluded patients with active drug use within the past 12 months, though those on stable opioid substitution therapy were eligible. Additionally, the distribution of HCV GTs differed between the ASTRAL studies and the real-world dataset, and sample sizes for GT4, GT5, and GT6 were small, which may limit the generalizability of our findings for these subgroups. A major limitation of the real-world dataset is that, while 71% (8005/11,299) of patients had SVR12 testing data, only 5% (509/11,299) of patients had both SVR4 and SVR12 data available. Also, because this dataset is based on Medicaid claims, it has inherent constraints, including potential underestimation of comorbidities, such as cirrhosis, and a limited ability to distinguish between active and past use or to assess disorder severity for people with a diagnosis of opioid or substance use disorder. The lack of HCV RNA sequencing data also prevents differentiation between virologic relapse and reinfection in those who did not achieve SVR, which could affect our concordance analysis. However, the number of people who achieved SVR4 but not SVR12 was very small. Additionally, the limited availability of HCV RNA data precluded assessment of whether individuals who achieved SVR12 but not SVR4 may have experienced low-level viremia. Finally, the real-world cohort was composed entirely of Medicaid beneficiaries, which may limit generalizability. Nonetheless, there is no reason to expect substantially different results among Medicare or commercially insured populations. Across both the ASTRAL-1, -2, and -3 studies and the real-world dataset, most patients were treatment-naïve and did not have cirrhosis or HIV coinfection; as such, further studies of the concordance of SVR4 and SVR12 among these populations are warranted.
This study represents the first validation of the concordance between SVR4 and SVR12 in patients receiving SOF/VEL, comparing data from RCTs with real-world data. These results confirm that SVR4 reliably predicts long-term SVR and provide support for using SVR4 as the endpoint in post-treatment monitoring. Adoption of SVR4 as the standard endpoint for patients receiving SOF/VEL can streamline follow-up care and potentially help reduce the risk of patients being LTFU, particularly among vulnerable populations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Martinello M. Solomon S.S. Terrault N.A. Dore G.J. Hepatitis C Lancet 20234021085109610.1016/S 0140-6736(23)01320-X 37741678 · doi ↗ · pubmed ↗
- 2World Health Organization Hepatitis C Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-c(accessed on 7 April 2025)
- 3Asselah T. Marcellin P. Schinazi R.F. Treatment of hepatitis C virus infection with direct-acting antiviral agents: 100% cure?Liver Int.20183871310.1111/liv.1367329427484 PMC 7713514 · doi ↗ · pubmed ↗
- 4World Health Organization Global Health Strategy on Viral Hepatitis 2016–2021 Available online: https://iris.who.int/bitstream/handle/10665/246177/WHO-HIV-2016.06-eng.pdf?sequence=1(accessed on 7 April 2025)
- 5European Association for the Study of the Liver EASL recommendations on treatment of hepatitis C: Final update of the series J. Hepatol.2020731170121810.1016/j.jhep.2020.08.01832956768 · doi ↗ · pubmed ↗
- 6World Health Organization Updated Recommendations on Treatment of Adolescents and Children with Chronic HCV Infection, and HCV Simplified Service Delivery and Diagnostics Available online: https://iris.who.int/bitstream/handle/10665/363590/9789240052734-eng.pdf?sequence=1(accessed on 8 April 2025)37410875 · pubmed ↗
- 7Ghany M.G. Morgan T.R. AASLD-IDSA Hepatitis C Guidance Panel Hepatitis C guidance 2019 update: American Association for the Study of Liver Diseases-Infectious Diseases Society of America recommendations for testing, managing, and treating hepatitis C virus infection Hepatology 20207168672110.1002/hep.3106031816111 PMC 9710295 · doi ↗ · pubmed ↗
- 8World Health Organization Guidelines for the Care and Treatment of Persons Diagnosed with Chronic Hepatitis C Virus Infection Available online: https://iris.who.int/bitstream/handle/10665/273174/9789241550345-eng.pdf?ua=1(accessed on 7 April 2025)30307724 · pubmed ↗