A Scoping Review of Influences on HPV Vaccine Uptake in the Rural US
Sherri Sheinfeld Gorin, Rebecca Hyman, Courtney Olson, Elizabeth Amber Fournier, Kaitlyn Yang, Diana Hanko, HPV Review Working Group

TL;DR
This study reviews factors affecting HPV vaccine uptake in rural US populations and suggests tailored interventions to improve vaccination rates.
Contribution
The paper systematically examines multilevel influences on HPV vaccine uptake in rural areas and identifies research gaps for targeted interventions.
Findings
Adolescents are the most common focus for change in HPV vaccine uptake.
Barriers include limited vaccine awareness, access to vaccination sites, and primary care recommendations.
Provider training and targeting rural healthcare workers could increase vaccine uptake.
Abstract
The human papillomavirus (HPV) is the leading cause of cervical and oropharyngeal cancers. Vaccination can prevent over 90% of HPV-attributed cancers. Rural populations are less likely to initiate and complete HPV vaccinations than urban. The primary objective of this paper is to systematically examine the multilevel (child/youth, parent/caregiver, physician/team, healthcare organization, community, and policy) influences on HPV vaccine uptake in the rural US population. As a secondary aim, we seek to identify gaps in the research that could contribute to the development of more precise intervention approaches in this population. The study adds to the limited number of recent reviews on rural HPV vaccine uptake in the US. Method: We conducted a systematic search of published empirical studies over 13 years (2010–2023), resulting in 1657 publications. The following databases were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
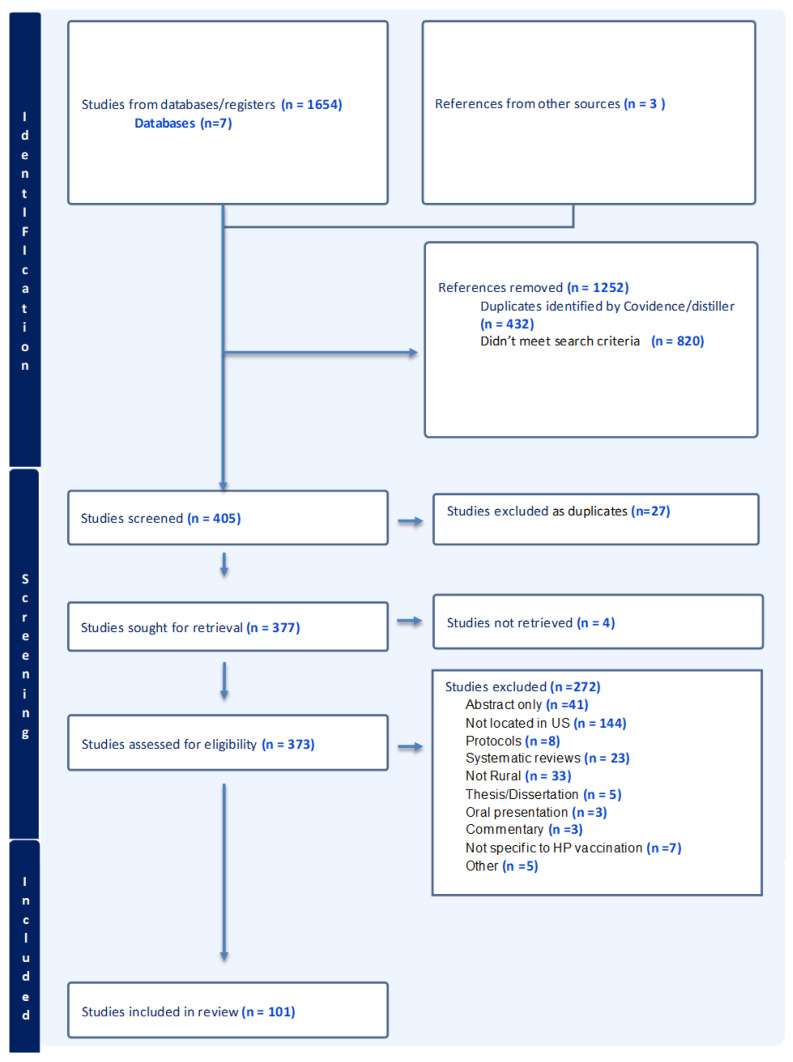 Figure 1
Figure 1- —The Undergraduate Research Program of the University of Michigan (SSG)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCervical Cancer and HPV Research · Head and Neck Cancer Studies · Vaccine Coverage and Hesitancy
1. Introduction
The human papillomavirus (HPV) is the most common sexually transmitted infection. The majority of cervical cancers are caused by persistent infections with oncogenic or high-risk types of human papillomavirus (HPV) [1]. Further, oncogenic forms of the virus cause a subset of oropharyngeal (oral cavity and pharynx) cancer, which is increasing in incidence [2]; men are more than twice as likely as women to be diagnosed [3,4,5,6,7]. The HPV vaccine is effective at preventing more than 90% of HPV infection-associated cancers. The HPV vaccine is effective at preventing more than 90% of HPV infection-associated cancers [1]. The Advisory Committee on Immunization Practices (ACIP) has recommended routine administration of the HPV vaccine for 11–12 year olds, as early as age 9, and catch-up vaccines through age 26 [8]. HPV vaccination rates remain below the Healthy People 2030 target of 80% [9]. Vaccination rates in rural communities are consistently lower than in urban communities in the rest of the country [10,11,12,13]. Among adolescents between the ages of 13 and 17 in 2024, 81.7% received more than one dose of the HPV vaccine in metropolitan areas, compared to 71.2% in mostly rural non-metropolitan areas. Additionally, 65.6% of 13–17 year olds in mostly urban areas were up-to-date with their HPV vaccine doses, compared to 54.8% in mostly rural areas. These variations in vaccination have led to higher mortality from HPV-associated cancers among rural residents [12,13].
Disparities in HPV vaccination rates among rural residents relative to urban and suburban residents are due to a number of factors. Allocations of healthcare and other resources across rural populations are impacted by the definition of rurality that is applied, and these definitions vary considerably [14,15]. Individual studies have found that travel time and low density of healthcare resources may pose challenges for accessing primary care to administer the vaccine in rural areas [16,17]. Some rural public health programs do not have resources to promote HPV vaccination or to devote to immunization in general [18]. These resources—as well as HPV vaccination messages—may not be well coordinated [17,19]. Many children in rural areas are seen by family practice providers whose panel includes very few adolescents and, thus, may not be comfortable making strong recommendations that are key to reducing HPV vaccine hesitancy [20,21,22,23,24]. Lack of awareness, limited knowledge, fear, and community stigma may increase hesitancy among adolescents and their caregivers [25,26,27,28]. Structural barriers like limited access to care and lack of insurance coverage influence HPV vaccine uptake, particularly in rural areas [10,29,30]. These influences may vary across and within rural communities [31,32], for example, due to the diversity of residents, including migrant agricultural workers, and Native Americans [33,34,35].
Importantly, the COVID-19 pandemic dramatically changed the uptake of all vaccines, including those against HPV. Studies reported increased levels of HPV vaccination hesitancy, vaccine refusals, and overall lower uptake within certain communities in the United States, including in rural areas [36,37]. The pandemic created major disturbances for routine HPV vaccine administration that were not captured in many early studies, nor in early reviews [38].
The majority of the reviews published on HPV vaccine uptake over the past 13 years have been narrow in focus [10,29,30,39,40,41,42,43,44]. In particular, none of these reviews have described the influences on HPV vaccine uptake in rural subpopulations in the US, although they have included rural residents as study participants [30,40,41,42,43,44]. The earliest of these reviews by Peterson et al. showed that increased HPV knowledge, peer-influence factors, and receiving other vaccines have been associated with HPV vaccine initiation and completion in rural communities [10]. This scoping review limited its search criteria to barriers and facilitators of vaccination at the individual level. The scoping review provided limited data on organizational, community- level and societal factors for their effects on HPV vaccination.
Other earlier reviews of rural HPV vaccine uptake were narrow in scope, either focused on measures [29] or interventions alone [39]. A recent systematic review and meta analysis explored the contribution of healthcare worker (HCW) practices to HPV vaccine recommendations worldwide. The systematic review and meta analysis results found mixed levels of HCW HPV vaccine confidence that varied by geographic location and gender of the vaccine recipient, as well as by type of physician. Worldwide, HPV vaccine recommendations were less common in rural areas than in urban communities, and within countries without national programs, as in the US. To increase recommendations, they highlighted the need for more contextually relevant approaches to addressing HCW vaccine hesitancy, as in the multilevel model of this scoping review [40].
Another scoping review examined digital health interventions for HPV vaccination in the US; the review focused on racial and ethnic minority groups, rather than rural populations, however [42]. With limited broadband access to about 38% of rural communities, digital interventions have limited reach in these communities [41].
Several current systematic reviews, scoping reviews, and one meta analysis have examined increasing HPV vaccination rates and promoting interventions [30] worldwide, generally including the US. One of these systematic reviews examining childhood immunizations, including HPV, highlighted middle-and lower-income economies, although uptake in rural USA settings was not specified [43]. Another systematic review of worldwide HPV vaccinations excluded males [44]. The Escoffery et al. systematic review highlighted the need to expand the implementation of HPV vaccine promotion interventions beyond education alone and at a single level of intervention [30].
Only one review has systematically examined multilevel influences on rural HPV vaccination in the US. Multilevel influences (targeting the child/youth, parent/caregiver, physician/team, healthcare organization, community, and policy) are defined as “…change in the individual patient, as well as at least two levels of contextual influence.” Multilevel factors can influence change among children and youth, parents and caregivers, healthcare providers and teams, clinics and health systems, communities, and policies. This recent systematic umbrella review (review of reviews [45]) identified modifiable individual-, provider-, and clinic-level factors associated with HPV vaccination outcomes among U.S. adolescents and developed a multilevel framework illustrating relations between factors to inform intervention development. Our review advances this comprehensive paper by adding the community and policy levels to the scoping review. Further, as an umbrella review, quality problems and biases that might exist in primary studies and in the umbrella review process itself could be compounded and difficult to clarify [46].
An updated review of the empirical literature on rural HPV vaccine uptake is warranted to better understand the influences on lower vaccination rates. To our knowledge, no review has yet focused on HPV vaccine uptake in the rural US using a multilevel perspective that includes the community and policy levels. In accord with the aim of scoping reviews in general, we aim to provide an overview or map of the available evidence, rather than synthesized findings for implementation into policy or practice [47]. The primary objective of this paper is therefore to systematically examine the multilevel influences on HPV vaccine uptake in the rural US population. As a secondary aim, we seek to identify gaps in the research that could contribute to the development of more precise intervention approaches in this population.
2. Methods
We conducted a scoping literature review of factors influencing HPV vaccine uptake in the rural US between 2010 and 2023.
2.1. Search Strategy
A skilled informaticist searched seven databases (Medline (OVID), Embase, CINAHL, PsychInfo, Cochrane, Sociological Abstracts, and Scopus) using the inclusion criteria detailed below. The primary search was conducted in Medline (OVID), and MeSH terms were combined with keywords in the title, abstract, and author-supplied keywords. The other database searches were translations of that primary search and used the database’s controlled vocabulary when available (e.g., for EMBASE, we used EMTREE). MeSH is not always available in the other databases. Several “gold standard” articles were identified in advance; the search located each of them.
Key search terms included: HPV, virus, vaccination, measures, and rural (see Appendix A for the full search strategy).
Two systematic searches were conducted by a skilled informaticist over time; the second search updated the first search. Identical search terms were used, and the same inclusion and exclusion criteria were applied to both searches. As depicted on the PRISMA table (see Figure 1), in total, 1657 articles were identified. These included the three papers that were identified from alternative sources, other than bibliographic databases and registries.
For the first search, articles were screened using the DistillerSR software version 2.35 [48] to eliminate duplicate articles and those that did not meet the specific search criteria. In the second search, the Covidence software [49] was used to deduplicate the articles, as well as to narrow the search. Both Distiller and Covidence software are similar in their key features [50]; the search findings were consistent; the choice was made by the informaticist, as the library changed its software recommendations over time [50]. After exclusions, 101 articles met the criteria to be included in this scoping review and were systematically coded (see Figure 1).
2.2. Source of Evidence Screening and Selection
We included original peer-reviewed, empirical articles that focused on HPV vaccine uptake, hesitancy behavior, attitudes/beliefs, and awareness/knowledge at multiple levels, including rural children and youth (age 9–26), families, healthcare providers, clinics, communities, or policies. HPV vaccine uptake was the primary outcome. Uptake was defined as the recommendation for or the receipt of HPV vaccination as recorded in the medical record or in a vaccine registry, reported by healthcare providers, parents, caregivers, or youth themselves. We recorded both initiation of vaccination, that is, the administration of the first HPV dose, as well as the up-to-date or completed age-dependent dosage (two- or three-doses). We defined HPV vaccine hesitancy using the World Health Organization definition of “the reluctance or refusal to vaccinate despite the availability of vaccines” [51].
Rurality has been defined differently by the primary studies included in this review. Rurality is defined by the US Census as a population, housing, or territory not in an urban area, with <2500 residents [13], and by the OMB by Rural–Urban Commuting Area Codes (RUCAs), with the most rural rated at 8–10 [14].
The inclusion criteria included articles published between 2010 and 2023, in the English language, and empirical research. We excluded studies that were not empirical, as well as reviews, commentaries, abstracts, and theses. Unlike systematic reviews, as yet, there are no generally accepted critical methodologic quality appraisal or risk of bias tools for scoping reviews. Our research teams rigorously followed a research protocol, with multiple internal reviews to maintain consistency, however, as inconsistency is a major concern for scoping reviews [47].
We used either the Distillr or Covidence software for the screening process, allowing for blinding. A team of 12 well-trained and closely supervised undergraduate and graduate students who were selected for a mentored research experience, led by SSG, conducted a review of abstracts. A full text review was conducted by another team of well-trained and closely supervised student researchers, again led by SSG. Any discrepancies in screening among the team members were discussed together for final inclusion.
2.3. Data Extraction
We extracted data using a standardized coding form adapted from Peterson et al. (2020) [10]. We collected descriptive data on each study, including publication year, study design, sample size, and participant type (e.g., children, youth, and parents). We collected the rates of HPV vaccine recommendation or uptake, and the findings on the associations among knowledge, attitudes/beliefs, and HPV vaccination. We also collected meta data about the multilevel focus of the study, that is, whether the study focused on individual children/youth, parents, healthcare providers/teams, clinics, communities, or policies. Each study was systematically coded by two independent members of the research team. Discrepancies in data extraction were resolved in discussion by a third reviewer.
2.4. Data Analysis
We summarized the key study characteristics using descriptive statistics (percentage, median, and mode). We conducted a narrative synthesis of the principal findings regarding knowledge, attitudes/beliefs, and HPV vaccination behaviors. The outcomes were initiation and completion of the HPV vaccination.
3. Results
3.1. Study Descriptions
We systematically reviewed 101 studies [26,27,36,37,38,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147,148] (see Appendix B). Following the PRISMA guidelines, from 1657 abstracts retrieved, after thorough systematic evaluation by two coders using a standardized coding form, we reviewed and coded 101 papers (see Figure 1). The median year of publication was 2021; the most studies were published in 2022, about 16 years after the introduction of the HPV vaccine to the US (see Table 1). Nearly half of all studies included cross-sectional studies, with surveys in the main. Secondary analyses were the second-most common design, including data from the National Immunization Survey-Teens (NIS-T) and the 2012 Youth Risk Behavior Surveillance System (YRBSS) surveys, at 11% of all studies. Cohort studies, randomized controlled trials, and quasi-experiments were next in frequency (6.9%, each). Qualitative studies were few in number (at 6%, or six studies), as were observational (4%), pilot/feasibility studies (3%), retrospective chart reviews, and other designs (e.g., mixed methods) at 2% each.
As would be expected, children and youth, aged 17 and under, were the most common study participants (30%), followed by those aged 18–26 (26%). Parents (18.8%) and healthcare providers (14.9%) were less frequent study participants. Clinics were infrequent study participants (5%). Other participants, including community stakeholders, were more frequent participants than clinics, but were least frequent overall (11.9%). The median sample size was 101–500, although studies ranged from <50 to >10,000 for studies relying on entire populations and registry data.
Nineteen percent of the US is classified as rural, according to the US Census. Nationally, 50% of rural residents live in the southern US [149]; the South was the most frequent geographic site for study participants as well (41.6% of all studies), followed by the Midwest (20.8% of all studies). National studies were 18% of the total, followed by the West (16.8%); least frequent were studies of more than one region of the country (2%). Interestingly, while the US Census notes that 61.6% of the rural US population lives in two Northeastern states (Maine and Vermont), only one study was recruited from the Northeast (the state of New Hampshire).
3.2. The Characteristics of HPV Vaccine Interventions
Twenty papers studied an intervention (see Table 2). One paper tested the feasibility of an intervention [77], and one described study implementation [21]. The remaining studies tested an intervention to increase HPV vaccine uptake. The purposes of these studies varied considerably, from parental and patient education to provider education and training, to community awareness education, and general community awareness campaigns using medias and vaccine vouchers. The “other” study explored enrolling a community pharmacy in the Vaccines For Children (VFC) program. Most studies did not include a free vaccination as a part of the intervention design, although the VFC program covers most children through 18 years of age, who are as follows: Medicaid-eligible, uninsured, American Indian or Alaska Native, or underinsured [150]. Of those seven studies that provided free HPV vaccinations, two only included these if the participants were VFC-eligible. Interventions ranged from half a year to more than one year, with most being of longer duration. Within the 12 studies relying on education and training sessions that specified the length, most were one hour. Most studies that specified a session length held one session, followed in frequency by two to four sessions; five or more sessions were least frequent. The primary intervention interaction mode was in-person, followed by virtual or remote, then indirect (including social marketing campaigns). Virtual sessions (e.g., [151]) were more common than in-person during the COVID-19 pandemic, as would be expected. Two studies did not specify the number of sessions. Research teams were the primary intervention agents, followed by community medical professionals, or others (such as a radionovela). Only two studies relied on self-directed interventions.
3.3. Theoretical Models
Few studies rested on theories or models of change; most were atheoretical (see Table 3). One of the two most common models of change was the Theory of Planned Behavior [151] (TPB; undergirding six studies) with intention as a primary explanatory construct. The Health Belief Model [152] was equally frequent, underpinning eight studies, followed by the Social Ecological Model [153], undergirding three studies. The remaining models and theories each founded one study, including the Community-Based Participatory Research Model [154], the Andersen Model [155], the Shared Treatment Decision-Making Model [156], the Competing Demands Model [157], the Comprehensive Participatory Planning [158], the Consolidated Framework for Implementation Research (CFIR) [159], the Ecological Systems Theory [160], Concept Mapping [161], the Precede-Proceed Model, and the Positive Deviance Framework [162].
3.4. Multilevel Interventions and Change
Looking at the intervention studies from the perspective of multilevel change, we did not identify any studies at the policy level that met the selection criteria (see Table 4). Only three studies systematically assessed multilevel outcomes, that is, outcomes at two levels of change or more. One study showed an increase in initiation and completion [78], one showed a decrease in missed appointments [89], and one showed no change in the measured outcome—initiation [109] (see Table 4). At the community level of change, across five studies, the intervention increased HPV vaccine initiation and completion in four studies [73,80,116,117]. One feasibility study explored enrolling a community pharmacy as a VFC provider; the approach increased HPV vaccination initiation in Alabama [77]. None of the three studies at the clinic or system level reported a change in HPV uptake [59,70,85]. Across most previous studies, provider recommendation was cited as influential on HPV uptake; similarly, the two studies of this level of change reported an increase in initiation via systematic provider-based interventions [66,88]. Individual-level interventions were most frequent, relative to provider, clinic-, or community-level interventions (see Table 4). Four separate studies focused on the parent level of change reported increases in HPV vaccine uptake, as well as intention to vaccinate and awareness and knowledge [59,61,90,143]. Of the three studies focused on change at the young adult level, one intervention focused on both providers and young adults through a documentary film and provider education [88]. One intervention study focusing on young adults reported increased HPV vaccine series completion [135]. There was no difference between rural young adults and others in HPV vaccine uptake [27]. The three separate studies at the level of the child reported increased HPV vaccine uptake; two of these also focused on the community level via schools and educational programs [116,117,145].
3.5. HPV Vaccination Outcomes of Initiation, Completion, or Both
Looking at Table 5, no changes were observed in HPV vaccine initiation across studies of provider conversation training, a cancer control survivor program, a “1-2-3 Pap” informational video, or an HPV documentary movie relative to a control condition. Similarly, a web-based electronic record-linked Clinician Decision Support with or without shared decision-making tools (SDMTs) did not increase HPV vaccine initiation.
Health campaigns improved completion of the HPV vaccine in medically underserved rural colleges. In rural Iowa VFC clinics, the most frequently implemented HPV vaccine interventions engaged changing provider and patient knowledge.
Rural clinics with higher HPV vaccine up-to-date rates relative to other clinics implemented standardized workflows to identify patients due for the vaccine and had vaccine administration protocols. They had a vaccine champion. Providers administered immunizations regardless of visit type; they used clear and persuasive language to recommend or educate parents and youth.
HPV vaccination coverage was not statistically significantly different among cancer survivors participating in a Childhood Cancer Survivor Program relative to others.
The COVID-19 pandemic had a negative impact on HPV vaccination initiation and completion [36,37,38,89,96]. This finding is interpreted with caution, however, as the period of observation was not lengthy.
3.6. Predictors of HPV Vaccine Initiation
Reviewing Table 6, more than two-thirds of Americans had heard of HPV and the HPV vaccine, with awareness being less in rural areas than urban areas, and less among black adult women in Alabama than others. Similarly, awareness of HPV was lower among women in rural colleges than in urban ones. Males were less likely to vaccinate than women. Among rural parents, increased initiation was associated with political affiliation and not affiliating with the Baptist religion relative to Baptists. Adolescents were less likely to initiate and complete the HPV vaccine if they were not up-to-date on the hepatitis A, meningococcal, or Tdap vaccinations. Attitudes/Beliefs were the strongest predictor of mothers’ intentions to vaccinate. Social connections, including social norms and social groups, enhanced uptake; marriage diminished the intention to vaccinate.
Looking at interventions with rural residents, implementing a video community education film increased HPV knowledge gained and attitudes towards the HPV vaccine among rural adult parents, students, and providers. Providing messages through texting on cell phones promoted HPV vaccination in rural middle school students.
Among healthcare providers, rural providers were less likely to have evening/weekend hours for adolescent vaccination appointments, to have had prior experience with adolescent vaccine quality improvement projects, and to routinely recommended HPV vaccine during urgent/acute care visits than urban providers. By contrast, significantly more rural providers had standing orders to administer all recommended adolescent vaccines and reported giving HPV vaccine information to their patients/families before it was due. Collaborative communication between providers and patients was less common among rural patients than urban patients. Medical providers, rather than others in the practice, provided more favorable recommendations for the HPV vaccine.
Rural stakeholders identified education and provider influence as key to HPV vaccination; those rated as most feasible were education and coordinated/consistent messaging. Stakeholders in the Carolinas strongly supported school-based programs and approaches to strengthen confidence and demand for the HPV vaccination [79].
4. Discussion
4.1. Summary of the Results
This scoping review has systematically examined the multilevel influences on HPV vaccine uptake in rural areas across the US. The study adds to the limited number of recent reviews on rural HPV vaccine uptake in the US. Over the past 13 years, studies measured HPV vaccine initiation (at least one injection), or completion (among those who had initiated vaccination), or both. Across all types of HPV vaccine uptake, non-rural residence, female gender, and provider recommendations tended to increase vaccination, as did educational interventions, although rigorous studies of interventions were relatively few. The Vaccines For Children program increased both HPV vaccine initiation and vaccine completion, as did other forms of insurance coverage. Within each vaccination behavior, however, different factors, such as area-based poverty and sexual history, differentially influenced initiation, completion, or both.
Across the 101 studies, most increases in initiation of the HPV vaccine were among those aged 11–17. Among studies of the completion of the HPV vaccine, increased vaccination was reported among women who felt a sense of control over vaccination, and within school settings. A video educational intervention increased completion of the vaccine series. Overall, boys were less likely to be vaccinated than girls; yet, boys in high-poverty areas were more likely to complete the vaccine than comparable others.
While a multilevel framework undergirded the review, we found only 20% of intervention studies measured change at the individual, provider, clinic, or community levels of change, with the largest number of studies assessing individual-level outcomes. Even though several of the reviewed papers addressed policy-level influences, we found no policy-level interventions in rural communities.
4.2. Sociodemographic Influences
Some studies in this scoping review found initiation higher among those aged 11–17, yet some recent individual studies have reported strong acceptance of vaccines for those starting at age 9, and increased efficacy of those vaccines among younger children [137,163]. Of late, campaigns by the ACS, CDC, and local rural health departments, as well as the HPV Roundtable action guides, have focused on initiating the vaccine among younger children, starting at age 9. Adolescent visits to healthcare providers are less frequent than children’s visits, and vaccines are not generally a part of the visit as youth age [164]. To desexualize the vaccine, that is, detach it from decisions about engaging in sexual activity that often arise in adolescence, introducing the vaccine when children are aged 9 has been found through recent preliminary studies to increase uptake, and seems well accepted by parents [165,166,167].
The recommendations for males have traditionally lagged behind the female vaccine recommendations, resulting in lower adolescent and young adult male initiation rates [74,168,169,170,171]. Of late, however, coverage has increased dramatically among males and is now relatively comparable to that of females overall. Among rural males, however, overall, the vaccination rates still lag behind those for females. As a result, males may need different strategies for engagement than females.
The studies reviewed herein showed varied influences of areas of rural poverty. Area-based poverty was not linked with initiation, but was linked to HPV vaccine completion. A more recent individual study found a consistent influence of rural social deprivation on HPV vaccine uptake [172]. Interestingly, boys in high-poverty areas were more likely to complete the vaccine than comparable others, perhaps due to the wide reach of the VFC program.
4.3. Healthcare Provider Influences
One influential study in this review, followed by two more recent papers, has found that physicians who offer a presumptive announcement, stating that the vaccination would be given at that visit, increase vaccine uptake [173,174]. Strong evidence from a randomized clinical trial on presumptive announcement vs. conversational approaches in this scoping review supports the influence of the former on increased HPV vaccine uptake across rural and urban settings [175]. A recent pragmatic trial found that the approach could be effectively implemented in ongoing practice using quality improvement in diverse health department areas [173]. Recent qualitative studies of this approach in rural settings only suggest that physicians modify this approach for their rural patients, who, valuing self-sufficiency, respond less favorably to proscriptions [174]. Prescriptions could erode trust in the relationship with the physician over time [174].
4.4. Multilevel Observations and Interventions
However, none of the studies reviewed assessed care from all potential intervention levels—policy/community, organization/health system, provider/provider teams, to the family, and individual patients; most of the reviewed studies used individual-level interventions and outcomes only. The few system-level interventions that were studied need to be replicated to determine whether they are feasible and scalable, while yielding similar outcomes. There is promise for multilevel interventions, however, as found in a comprehensive umbrella review that included studies of both rural and urban participants [45].
Overall, the results from many large randomized clinical trials, community-based intervention trials, case–control studies, and observational studies suggest that clinically meaningful changes in cancer risk factors, cancer-related morbidity, and mortality are possible over time [176,177]. However, these approaches are often stronger in design than in implementation or evaluation [138], and more rigorous research focused on marginalized populations, including rural residents, is necessary [178].
4.5. Theory as a Guide
Few studies rested on theories or models of change; most were atheoretical. Yet, behavioral medicine offers a rich set of theoretical models and frameworks with which to understand multilevel influences on HPV vaccine uptake that could enrich understandings of current effective interventions and maximize their usefulness in practice. Individual, cognitive-based models such as the Theory of Planned Behavior [151], Health Belief Model [30,152] and the Theory of Reasoned Action emphasizes the importance of beliefs and values of outcomes as key variables that predict whether individuals engage in desired cancer prevention and control behaviors. The Social Ecological Model [153] emphasizes the role of the multilevel environment on HPV vaccine behavior change. Implementation Science theories and models, such as CFIR, could describe for whom theoretical models work, when they work, and when they do not (NIH, personal communication, 9/8/25). Implementation science approaches could better specify how regional cultural, economic, and healthcare system differences might influence intervention effectiveness. Implementation science approaches could subsequently inform future public health interventions, particularly to expand intervention reach.
Interventions that emphasized cancer prevention, rather than STI prevention, have been found to be more effective in promoting HPV vaccination [179,180]. In particular, within the Health Belief Model, when text messages framed the daughter’s susceptibility to HPV as a risk factor and emphasized the caregiver’s role as a protector, motivation for vaccination increased [181].
4.6. Limitations
As with all reviews, the quality of the scoping review is dependent upon the quality of the individual studies [46,182]. Limitations in sample sizes, geographic scope, variations in outcome measures, and the heterogeneity of the original studies on which the scoping review relies influence the rigor of the scoping review. There were variations in definitions of rurality. The scoping review does not include information for interventions or epidemiological associations that have not been examined in the included studies. In particular, we only evaluated a small number of studies of multilevel influences, as few of these studies have been conducted, so the findings may be limited.
While the protocol was not prospectively registered, it detailed the review’s inclusion and exclusion criteria and identified which and how data would be (and were) extracted and presented. This is a recommendation of JBI, a group that publishes influential guides for evidence synthesis [47].
5. Conclusions
This scoping review has systematically examined the multilevel influences on HPV vaccine uptake in rural areas across the US. It expands and updates the contribution of the one previous systematic review of this topic. Across all types of HPV vaccine uptake, non-rural residence, female gender, and provider recommendations tended to increase vaccination, as did educational interventions, although rigorous studies of interventions were relatively few. The Vaccines For Children program increased both HPV vaccine initiation and vaccine completion, as did other forms of insurance coverage. Adolescents themselves were the most common foci of change.
6. Next Steps
The findings suggest several strategies to increase rural HPV vaccine uptake [176]. Within clinics, integrating HPV vaccine surveillance data with the electronic health record could facilitate more rapid retrieval of vaccination status. The State of Michigan, for example, maintains a robust system of monitoring HPV vaccinations, but the data are not necessarily within clinical electronic health records or on dashboards, so they must be retrieved by request. Once available, routine audit and feedback of these data could increase their use by clinical teams. Further, additional workflow mapping for the HPV vaccine could facilitate routine vaccination, as noted in a previous review [40].
Among primary care physicians, training in announcing the HPV vaccine, thus integrating it with the other adolescent vaccines, could decrease hesitancy [66,183]. Practice facilitation and academic detailing with clinicians, front office staff, and others could facilitate redesign for HPV vaccination [184,185,186,187,188,189,190,191]. This redesign could include identifying community-based resources like community pharmacies that are enrolled in the Vaccines for Children program [77,192,193,194] that could increase access in rural areas. This is a critical policy-level intervention.
Importantly, tailored interventions to rural parents/caregivers could increase awareness and knowledge about the vaccine. Developing local champions among both primary care providers and rural youth for the HPV vaccine could enhance decision-making skills, disseminate accurate and unbiased information, and increase trust in the vaccine [191].
These findings will lead to approaches for vaccines to reach those who are most vulnerable to the diseases that they prevent.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1HPV Vaccine Safety and Effectiveness Available online: https://www.cdc.gov/vaccines/vpd/hpv/hcp/safety-effectiveness.html#hpvvxeff(accessed on 15 November 2025)
- 2Muñoz N. Bosch F.X. de SanjoséS. Herrero R. CastellsaguéX. Shah K.V. Snijders P.J.F. Meijer C.J.L.M. Epidemiologic Classification of Human Papillomavirus Types Associated with Cervical Cancer N. Engl. J. Med.200334851852710.1056/NEJ Moa 02164112571259 · doi ↗ · pubmed ↗
- 3American Cancer Society Cancer Facts & Figures 2020 Available online: https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2020.html(accessed on 11 November 2025)
- 4Parkin D.M. Bray F. Ferlay J. Pisani P. Estimating the world cancer burden: Globocan 2000 Int. J. Cancer 20019415315610.1002/ijc.144011668491 · doi ↗ · pubmed ↗
- 5De Vita V.T.Jr. Lawrence T.S. Rosenberg S.A. De Vita, Hellman, and Rosenberg’s Cancer: Principles & Practice of Oncology Lippincott Williams & Wilkins London, UK 2015 Available online: https://oncology.lwwhealthlibrary.com/book.aspx?bookid=1172§ionid=0(accessed on 19 January 2026)
- 6Howlader N. Noone A.M. Krapcho M. Miller D. Brest A. Yu M. Ruhl J. Tatalovich Z. Mariotto A. Lewis D.R. SEER Cancer Statistics Review, 1975–2017 National Cancer Institute Bethesda, MD, USA 2020 Available online: https://seer.cancer.gov/csr/1975_2017(accessed on 3 April 2025)
- 7U.S. Department of Health and Human Services Centers for Disease Control Prevention and National Cancer Institute. U.S Available online: https://gis.cdc.gov/cancer/USCS/#/At A Glance/value,1,2,1,1,1,1(accessed on 3 December 2025)
- 8Meites E. Szilagyi P.G. Chesson H.W. Unger E.R. Romero J.R. Markowitz L.E. Human Papillomavirus Vaccination for Adults: Updated Recommendations of the Advisory Committee on Immunization Practices MMWR Morb. Mortal. Wkly. Rep.20196869870210.15585/mmwr.mm 6832 a 331415491 PMC 6818701 · doi ↗ · pubmed ↗