A Systematic Review of Bacterial Sampling Collection for Veterinary Microbiology in Companion Animals
Inês C. Rodrigues, Joana C. Prata, Ângela Pista, Paulo Martins da Costa

TL;DR
This paper reviews how samples for bacterial testing are collected in dogs and cats, finding significant variability and a need for standardized guidelines to improve diagnostic accuracy and antibiotic use.
Contribution
The study identifies gaps in standardized bacterial sampling practices in veterinary microbiology and advocates for evidence-based guidelines to improve diagnostic reliability.
Findings
Swabs are commonly used but less reliable compared to tissue and fluid samples.
Pre-laboratory factors like antibiotic use and transport conditions are often poorly documented.
Sampling methods and culture recommendations vary by anatomical site and suspected bacteria.
Abstract
Accurate diagnosis of bacterial infections in dogs and cats depends on proper collection, handling, storage, and transport of samples. This review examined current practices for taking and processing samples for bacterial testing, based on seventeen studies published over the last ten years. The results showed that sampling methods vary widely across body sites. Swabs were most commonly used, but tissue and fluid samples generally provide more reliable results. Key information, such as prior antibiotic use and storage or transport conditions, was often missing, which can affect test accuracy. The choice of culture method and storage depends on the suspected bacteria and the body site sampled. Overall, there are significant gaps in standardisation. Developing clear, evidence-based guidelines could improve test reliability, support responsible antibiotic use, and ultimately enhance the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
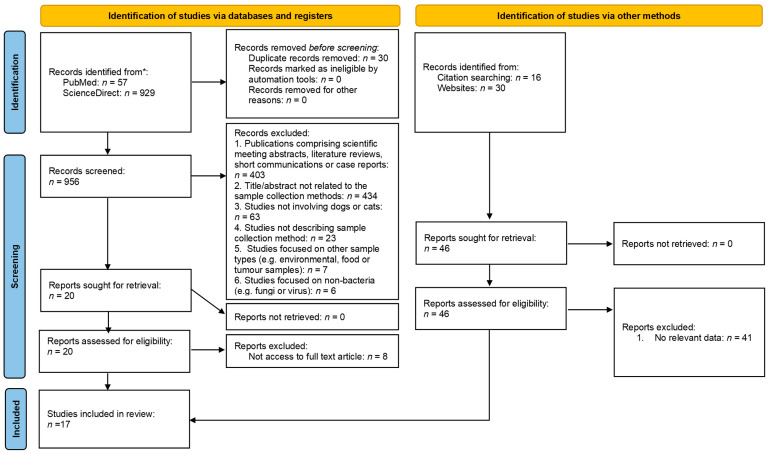 Figure 1
Figure 1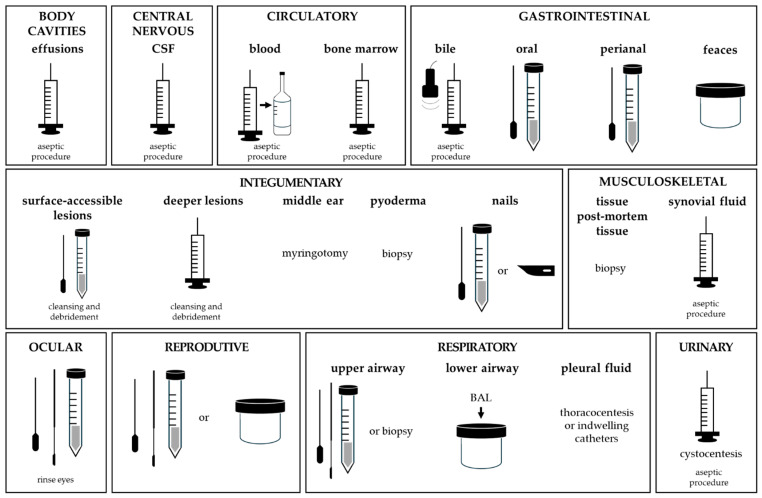 Figure 2
Figure 2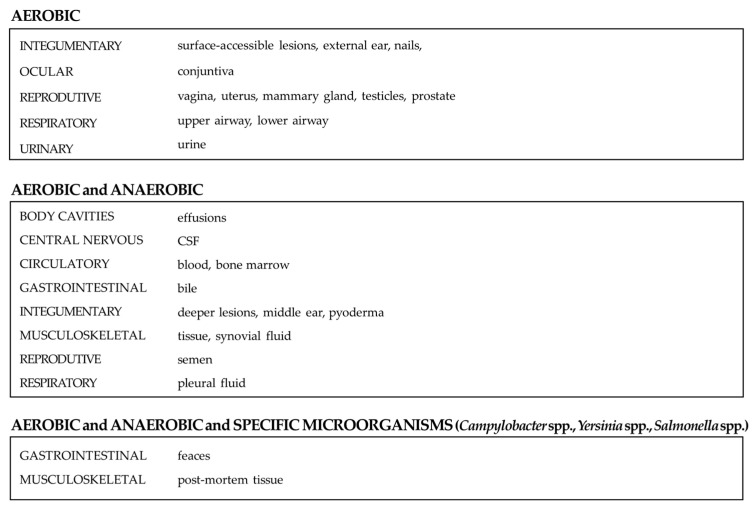 Figure 3
Figure 3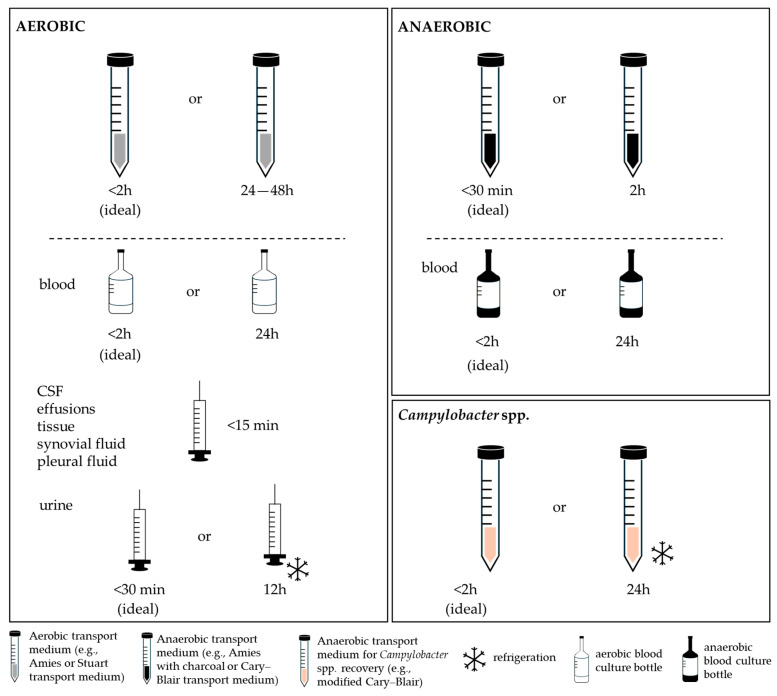 Figure 4
Figure 4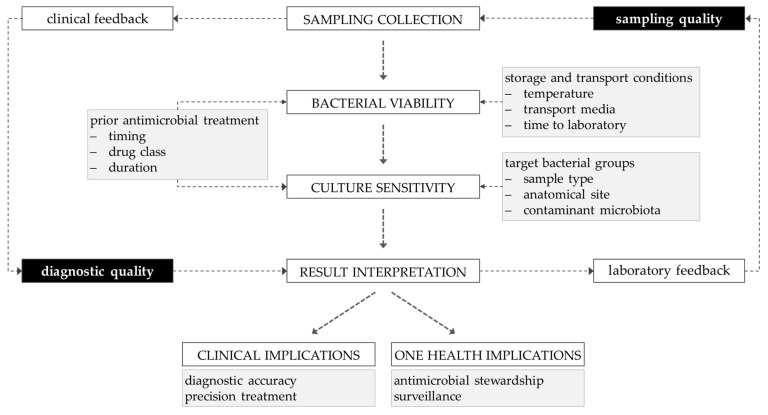 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVeterinary Medicine and Surgery · Veterinary Oncology Research · Bacterial Identification and Susceptibility Testing
1. Introduction
Microbiological diagnosis is a cornerstone of veterinary clinical practice, underpinning the identification of infectious agents and guiding antimicrobial therapy [1,2]. Bacterial infections are common in companion animals and often require prompt and accurate diagnosis to enable effective treatment [3]. However, the increasing prevalence of antimicrobial resistance (AMR) among veterinary pathogens poses a major clinical and public health challenge [3,4]. In this context, the need for accurate microbiological diagnosis becomes even more critical. Laboratory-guided antimicrobial therapy is crucial not only for improving clinical outcomes but also for promoting responsible antimicrobial use [5].
One important, though often underestimated, factor influencing diagnostic reliability is the quality of sample collection [6]. These methods, which include the technique used, the timing of collection and the conditions of transport and storage, determine the accuracy of culture and subsequent bacterial identification [6]. Equally critical is the quality and completeness of the clinical information accompanying the sample, as this contextual data is essential for the correct interpretation of microbiological findings and for distinguishing pathogens from contaminants or commensal organisms [6]. The diagnostic value of microbiological testing may be compromised by inadequate or improperly collected samples, as well as by insufficient or misleading clinical information, potentially leading to contamination, false-negative results, failure to recover the causative pathogen, or the isolation and misinterpretation of non-pathogenic or commensal microorganisms [5,7].
Despite its recognized importance, the use of these diagnostic tools, particularly culture and antimicrobial susceptibility testing, remains underused in veterinary settings. Previous studies conducted among European veterinarians have highlighted that faster results and reduced costs are key factors that could increase the use of antimicrobial susceptibility testing in this field [2,8]. Nonetheless, additional barriers, such as a lack of confidence in microbiological results, reliance on clinical assumptions and limited understanding of how to interpret susceptibility data, continue to hinder wider adoption [8]. Furthermore, antimicrobial susceptibility methods are not yet fully standardized, and for several antimicrobial agents and bacterial species, clinical breakpoints are lacking or incomplete, with epidemiological cut-off values often being the only available interpretative criteria, further complicating diagnostic reliability [9].
Sample collection practices in veterinary microbiology also remain highly variable, with limited evidence-based guidelines tailored specifically to small animal species [10]. This variability compromises diagnostic accuracy and may hinder appropriate antimicrobial selection, indirectly contributing to the AMR crisis.
While resources describing the handling of veterinary microbiological specimens upon their arrival at diagnostic laboratories are available, guidance for practitioners on best practices for sample collection remains scarce [10]. To date, no systematic review has consolidated the available evidence on microbiological sampling methods in dogs and cats. A comprehensive synthesis of current practices is therefore necessary to identify gaps, promote harmonisation, and strengthen the integration of microbiological data into both clinical decision-making and AMR surveillance.
The present systematic review aims to identify, summarise and evaluate the current sampling procedures used for microbiological diagnosis in companion animal veterinary practice, from sample collection to submission to the microbiology laboratory. Focusing on dogs and cats, the review examines collection techniques, specimen handling, and transport conditions that influence the reliability of microbiological results. The overarching goal is to support veterinary clinicians and diagnostic laboratories in improving sampling quality, thereby enhancing diagnostic accuracy, advancing antimicrobial stewardship, and ultimately safeguarding both animal and public health.
2. Materials and Methods
This systematic review was performed according to PRISMA 2020 (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines [11], with the protocol preregistered on OSF (timestamped 12 January 2026; registration number 10.17605/OSF.IO/BSVNJ).
2.1. Selection Strategy
In April 2025, an independent researcher (I.C.R.) conducted a systematic search of the PubMed and ScienceDirect databases, covering the last ten years (from 2015 onwards). This timeframe was chosen to capture the most recent and relevant evidence available in the field, in line with current recommendations for evidence-based reviews [12]. The aim was to identify peer-reviewed studies reporting sampling methods for microbiological diagnosis in dogs and cats, within a veterinary clinical context.
The following search terms were used in combination: (“microbiological diagnosis” OR “microbiological testing” OR “bacterial identification”) AND (“sampling method” OR “sample collection”) AND (“veterinary” OR “dog” OR “cat”).
Titles and abstracts were screened to assess eligibility for inclusion. Only peer-reviewed studies were considered. Studies were included if they focused on clinical samples from companion animals and provided detailed information on sampling techniques relevant to bacterial identification in dogs or cats. To complement the database search, additional studies were identified through citation searching and reference lists of relevant review articles.
The exclusion criteria were: articles not written in English; studies involving species other than dogs and cats; studies that did not describe sampling methods or that investigated non-clinical samples, such as environmental or food sources; studies focused on non-bacterial organisms (such as fungi or parasites); publications for which full-text access was not available through the university’s institutional subscriptions; and publications comprising scientific meeting abstracts, the literature reviews, short communications or case reports.
2.2. Selection Process and Data Extraction
All search results were exported to Microsoft Office™ Excel. Results from the initial search were evaluated according to the inclusion criteria. First, the results were screened by reading the article titles and excluding articles that were not relevant according to the inclusion criteria. Afterwards, the study abstracts were evaluated, and non-relevant articles were excluded. Subsequently, the selected full-text articles were retrieved and assessed according to the inclusion criteria. Any disagreements regarding study eligibility were resolved through discussion and consensus among the authors. After final selection, the following data were extracted from each selected study to elaborate a systematic database: article title, authors, article type, target animal species, origin and type of samples, method of sample collection, sample conservation method and time elapsed between collection and processing, study objectives, and information on antibiotic use prior to sample collection.
When a study described more than one sample type, collection method, or storage condition, each instance was recorded as an independent data point. This approach ensured that all sample-specific recommendations were captured, even when derived from a single publication. Consequently, the total number of data entries exceeded the total number of studies included in the review. For instance, storage and transport condition records amounted to 54 for aerobic cultures, 24 for anaerobic cultures, and 4 for Campylobacter cultures. Relative frequencies were calculated to describe how often a given parameter or recommendation appeared across the included studies. Therefore, in Section 3.4, Section 3.5 and Section 3.6, results are presented as proportions of the total number of records.
2.3. Risk of Bias Assessment
Risk of bias (RoB) was assessed using different critical appraisal tools to ensure a comprehensive and study type-specific evaluation of the methodological quality of the included studies, considering the specific characteristics of each study type [13]. Accordingly, the Joanna Briggs Institute (JBI) Critical Appraisal Tool was used for cross-sectional, prevalence, and expert opinion studies; the QUADAS-2 tool was applied for diagnostic accuracy studies; and the AGREE II tool was employed for clinical practice guidelines. The RoB of each study was independently analysed. No software was used; the evaluation was conducted manually based on the criteria suggested by each critical appraisal tool.
For the JBI tool, the evaluation focused on the clarity of inclusion criteria, detailed descriptions of the setting and participants, validity and reliability of sampling methods, appropriateness and justification of sample size, standardisation and reliability of measurements, management of confounding factors, clear reporting of sample handling, consistency and objectivity of outcome measurement and appropriateness of statistical analysis (Table A1) [14]. The QUADAS-2 tool examined potential biases related to patient selection, index test, reference standard, and flow and timing, as well as overall applicability concerns (Table A2) [15]. The AGREE II instrument assessed guideline quality across six domains: scope and purpose, stakeholder involvement, methodological rigour, clarity of presentation, applicability, and editorial independence (Table A3) [16].
For all tools, the following scoring criteria were applied: Y = Yes, N = No, U = Uncertain and N/A = Not applicable. An overall RoB score was calculated by assigning one point to each “Yes” response and zero points to each “No” or “Uncertain” or “Not applicable”. The total score was converted to a percentage of criteria met, allowing studies to be classified as low risk (≥80% of items met), moderate risk (50–79%), or high risk (<50%) [17].
3. Results
3.1. Description of Studies
The PRISMA flow diagram provides an overview of the screening and selection process (Figure 1), while the characteristics and methodological quality of the included studies are detailed in Table 1. The initial search retrieved 986 records, of which 30 duplicates were removed, leaving 956 records for screening. Following title and abstract screening, 936 records were excluded. The full texts of the remaining 20 studies were then assessed for eligibility, resulting in the exclusion of 8 studies. In addition, five studies were identified through other methods and assessed for eligibility. In total, 17 studies met the inclusion criteria and were incorporated into this systematic review.
3.2. Quality Assessment
For cross-sectional, prevalence, and expert opinion studies (n = 10), most studies showed clear inclusion criteria, valid sampling methods, and consistent outcome measurement, while some uncertainty was noted regarding confounding factors and sample handling (Table A1). Overall, the risk of bias was rated low in four studies and moderate in six.
All diagnostic accuracy studies (n = 4) adequately addressed potential biases related to patient selection, index test, reference standard, flow and timing, and overall applicability concerns (Table A2). Consequently, all studies were rated as low risk of bias.
Among clinical practice guidelines (n = 3), scope, purpose, clarity of presentation, and applicability were generally well reported (Table A3). In contrast, stakeholder involvement, methodological rigour, and editorial independence were inconsistently described. Overall, one guideline was rated as low risk of bias, while two were rated as moderate.
Considering this overall assessment, the included studies were classified as presenting a low [20,21,24,25,26,28,29,30,32] to moderate [10,18,19,22,23,27,31,33] risk of bias and can therefore be regarded as methodologically acceptable for inclusion.
3.3. Characteristics of Studies and Outcome Measures
The characteristics of the included studies are summarised in Table 1. Of the 17 studies reviewed, 13 studies focused on sample collection in dogs and cats [18,20,21,22,24,25,26,27,28,29,31,32,33], two were limited to cats [19,30], one included dogs, cats, and exotic species [23], and one encompassed both companion and livestock animals [10].
With respect to sample types, eight studies investigated urinary tract samples [10,20,22,23,24,26,32,33], five skin samples [10,19,23,24,30], five respiratory tract samples [10,21,23,24,28], five faecal samples [10,23,24,30,31], four blood samples [10,23,24,33], four body cavity effusions [10,22,24,25], three synovial fluid samples [10,23,24], three tissue samples [10,22,23], two cerebrospinal fluids (CSF) [23,24], two ocular samples [18,23] and two reproductive tract samples [10,24]. In addition, single studies reported on other sample types, including bile [29], oral mucosa [30], bone marrow [23] and nail [23].
Regarding sampling methods for subsequent microbiological analysis, swabs were reported in nine studies [10,18,19,21,23,24,27,28,30], cystocentesis in seven [20,22,23,24,26,32,33], biopsy in five [10,22,23,24,28], aspiration in five [10,18,22,23,24], midstream urine collection in four [20,22,23,32], venipuncture in four [10,23,24,33], manual faecal collection in three [10,23,31], urinary catheterisation in three [22,23,32] and bronchoalveolar lavage (BAL) in three [10,23,24]. Less frequently reported techniques, each mentioned in a single study, included thoracocentesis [25], indwelling thoracic catheter [25], cholecystocentesis [29], spatula sampling [18], uterine lavage [24], manual milk extraction [24], semen collection [24], lumbar puncture [23] and ventricular aspiration [23], as well as tracheal washes [10] and blade collection [23].
3.4. Collection Methods and Specifications
The collection methods and specifications are summarised in Table 2.
3.4.1. Body Cavities: Reported Data
Effusion samples (n = 3) were mainly collected by aspiration, with one study reporting collection either by aspiration or swab. For aspirated samples, two studies reported placing the material in plain sterile plastic containers, while one recommended transferring the aspirated content onto a swab placed in transport medium.
3.4.2. Central Nervous System: Reported Data
Sampling was reported in two studies, both describing cerebrospinal fluid (CSF) collection. One study reported CSF collection by aspiration, while the other described either ventricular aspiration or lumbar puncture. Sterile tubes were recommended in both studies, with one study specifying the use of an aseptic subdural tap.
3.4.3. Circulatory System: Reported Data
Five studies reported sampling from blood (n = 4) and bone marrow (n = 1). For blood collection, three studies sampled from the jugular vein, and three studies used specific blood culture bottles. Volumes of blood collected varied with animal weight, ranging from 1.5 to 10 mL for microbiological analysis. Bone marrow collection was recommended by aspiration into a sterile plain container.
3.4.4. Gastrointestinal (GI) System: Reported Data
Eight studies reported sampling from the oral mucosa (n = 1), bile (n = 1), faeces (n = 5), and perianal area (n = 1). Oral mucosa sampling was performed using cotton swabs placed in transport media. Bile samples were collected through ultrasound-guided percutaneous cholecystocentesis. For faeces, four studies employed manual collection and two used swabs (with one study reporting both). Manually collected samples were placed in faeces-specific transport media (n = 2) or sterile containers (n = 2), with an approximate amount of 5 g per sample. Swabs were typically placed in Amies or Stuart transport medium. Perianal sampling was reported in a single study using a swab.
3.4.5. Integumentary System: Reported Data
Abscesses or wounds (n = 3), crusts (n = 1), epidermal collarettes (n = 1), external ear canals (n = 3), middle ear (n = 1), nails (n = 1), pustules (n = 1), pyoderma (n = 1), skin (n = 4) and surgical sites (n = 1) were described in the selected studies. Swab collection was the most common method for abscesses and wounds, with aspiration also reported in two studies. Crusts, epidermal collarettes, and surgical site samples were each collected by swab in a single study. External ear canals were sampled by swab in all three studies, while middle ear collection involved myringotomy using a stiff cat urinary catheter with a syringe. Nail samples were collected using a blade or swab; pustules by aspiration; and pyoderma by biopsy. Skin samples were consistently collected by swab (n = 4). Among swab-collected samples (n = 14), ten studies recommended placement in transport medium. Aspirated material (n = 4) was generally transferred to a swab in transport medium.
3.4.6. Musculoskeletal System: Reported Data
Sampling was reported in seven studies, including tissue (n = 3), post-mortem tissue (n = 1), and synovial fluid (n = 3). A biopsy was recommended for tissue and post-mortem samples. The samples were placed in plain sterile containers (n = 3), tubes containing transport medium (n = 1), or tubes with a clot activator (n = 1). One study suggested placing tissue in sterile tubes with a small amount of buffered solution, while another advised gently pressing the sample just below the surface of the medium, discarding the swab, and avoiding full submersion. Synovial fluid was collected by aspiration in all studies, with one also reporting swab collection. Equipment varied across studies, including sterile tubes, blood culture bottles, sterile containers, syringes, or swabs with transport medium.
3.4.7. Ocular System: Reported Data
Four studies reported ocular sampling, using swabs (n = 2), a spatula (n = 1), or aspiration (n = 1).
3.4.8. Reproductive System: Reported Data
Only one study described sampling from the vagina, uterus, mammary gland, testicles, prostate, and semen. Methods included biopsy or uterine washes, manual milk extraction, collection of the second or mid-third fraction of the ejaculate, rectal prostatic massage, cystocentesis, and swab sampling, respectively. Most samples were collected using sterile containers, except for the swab samples, which required a transport medium.
3.4.9. Respiratory System: Reported Data
Five studies described upper airway sampling and three lower airway sampling, with one study addressing pleural fluid. Upper airway samples included the nostrils, the nasal cavity, the mucosa, and the sinuses. Swabs were used in five studies and biopsies in three. Swabs were placed in Amies transport medium in four studies and moistened prior to sampling in one. Biopsies were performed blindly (n = 1) or under endoscopic guidance (n = 2). Lower airway samples were obtained exclusively by bronchoalveolar lavage (n = 3), with tracheal wash and bronchial brush reported in one study each. Pleural fluid was collected by thoracocentesis or an indwelling thoracic catheter into non-anticoagulant tubes using aseptic technique.
3.4.10. Urinary System: Reported Data
Thirteen studies reported urine sampling, most frequently by cystocentesis (n = 7), followed by catheterisation (n = 3) and midstream catch (n = 3). Of the studies using cystocentesis, two specified ultrasound-guided collection. Urine obtained by cystocentesis was collected in plain sterile containers (n = 4) or boric acid tubes (n = 2). Catheterised and midstream samples were primarily collected in plain sterile containers. The volume of urine collected varied across methods, ranging from 3 to 6 mL.
3.5. Consideration of Antibiotic Therapy Before Sampling
Among the 17 selected studies, three merely noted whether the animals had received antibiotics at the time of sampling. Two studies required a four-week antibiotic withdrawal period, and two specified a three-day withdrawal period. One study explicitly stated that ongoing antibiotic treatment should be reported on the sample submission form, and one indicated that sampling should be performed before the initiation of antibiotic therapy. The remaining eight studies provided no information regarding antibiotic administration (Table 3).
3.6. Target Bacterial Groups and Sample Storage Conditions Across Biological Systems and Sample Types
Across biological systems, most studies recommended testing for both aerobic and anaerobic bacteria, with a few notable exceptions driven by anatomical site or expected pathogens (Table 4). Body cavities effusions and CSF consistently required investigation of both groups. Similarly, blood, bone marrow and the musculoskeletal system generally followed this pattern. Notably, for post-mortem tissue, one study suggested testing for aerobes and/or anaerobes, as well as for Campylobacter jejuni, Yersinia, and Salmonella.
In contrast, skin samples frequently targeted only aerobes. This was evident in studies involving oral mucosa, external ear samples, nails, surgical sites, and several integumentary samples. Conversely, abscesses, wounds, and deeper integumentary infections typically included both aerobes and anaerobes.
Within the musculoskeletal, reproductive, and respiratory systems, recommendations varied, reflecting differences in anatomical depth and likelihood of anaerobic involvement. Upper airway samples, ocular and urine samples largely focused on aerobes, whereas lower airway and pleural samples included anaerobes more often. Semen was one of the few reproductive samples where anaerobic investigation was also suggested.
Storage conditions also varied by the bacterial group targeted. For aerobic bacteria, refrigeration was the most common recommendation, typically for up to 24–48 h, though some studies permitted longer or unspecified durations (Table A4). A minority emphasised rapid processing within 8 h. For anaerobic bacteria, recommendations tended to favour room-temperature storage, often up to 24–72 h. Reports targeting Campylobacter spp. showed no clear consensus, with both refrigeration and room temperature storage being described.
4. Discussion
The accuracy of microbiological diagnostics in veterinary practice depends primarily on the quality of the sample collected. Even when advanced laboratory techniques are available, inappropriate sampling tools, suboptimal transport conditions, or poor handling can compromise specimen integrity and reduce diagnostic accuracy [10,34]. In companion animal practice, where infections often require rapid and targeted antimicrobial therapy, the consequences of inadequate sampling include misleading culture results, delayed treatment, and a potential contribution to antimicrobial resistance [35,36]. Despite this critical role, veterinary-specific guidance on collection and storage remains limited and heterogeneous, highlighting the need for standardised, evidence-based practices.
In this systematic review, 17 articles were included to assess how sample collection methods, handling procedures, and transport conditions influence the reliability of microbiological results in dogs and cats. The findings revealed considerable variability, with potential implications for diagnostic accuracy and reproducibility.
4.1. General Patterns and Implications for Diagnostic Reliability
Across all biological systems, swab collection emerged as the most frequently reported method [37,38]. While swabs are convenient and minimally invasive, they are also more prone to contamination, yield limited sample volumes, and are less likely to capture deep or truly representative material from infected tissues [38,39].
Tissue biopsies demonstrate the highest diagnostic yield, with superior sensitivity, specificity, and predictive values, particularly for periprosthetic joint infections and infected diabetic foot ulcers [40,41]. In situations where biopsy is not feasible, pus aspirates provide a less invasive alternative, enabling the collection of diagnostically relevant material while acknowledging their lower sensitivity compared with tissue biopsy [38]. Nevertheless, the predominance of swab use, even in body sites where aspiration or biopsy would be more appropriate, may be driven more by logistical considerations than by evidence-based criteria. A similar pattern has been reported in human medicine, where pre-analytical errors remain a major contributor to diagnostic inaccuracy, often exceeding those arising from analytical or post-analytical phases [42].
4.2. Sampling Methods by Organ System
4.2.1. Body Cavities, the Central Nervous and Circulatory Systems
For cerebrospinal fluid (CSF) and body cavity effusions, aspiration was consistently used, reflecting good procedural standardisation. CSF samples were collected using aseptic subdural tap and sterile tubes, following recommendations similar to those in human medicine [43]. When immediate culture is not possible, CSF may alternatively be submitted in blood culture vials to improve microorganism recovery during delayed processing (Figure 2) [44].
Blood sampling appeared relatively uniform, with jugular venipuncture and blood culture bottles reported as standard. Sample volumes were generally modest, typically around 2.5 mL per bottle, or adjusted according to the animal’s weight, particularly in dogs. Although these volumes are lower than those recommended in human protocols, diagnostic sensitivity may still be compromised in cases of very low bacteraemia. Similar observations have been reported in human medicine, where insufficient blood volumes can lead to false-negative results, delayed therapy, and increased morbidity [45,46,47]. The sensitivity of blood cultures is directly correlated with the volume collected, as microbial loads in bloodstream infections may be as low as 1–10 CFU/mL [46,48]. Adult human protocols recommend 40–60 mL distributed across multiple bottles to optimise pathogen recovery, but such volumes are impractical in veterinary settings due to the wide variability in body sizes and circulating blood volumes [45]. Furthermore, contamination with commensal skin microorganisms during sample collection remains a significant cause of false-positive results, leading to unnecessary antibiotic treatment and extended hospitalisation [47]. As bloodstream infection–associated pathogens may originate from the skin and bacterial loads in blood can be as low as 0.25 CFU/mL, minimising contamination collection and preserving pathogen viability during transport to the laboratory are critical for accurate diagnosis [44].
Bone marrow sampling (BMS), reported in only one study, was performed by aspiration under aseptic conditions, in accordance with currently accepted best practices [49]. BMS provides valuable diagnostic informations for haematological and infectious diseases, such as Leishmania, feline leukaemia virus (FeLV), and Histoplasmosis [50]. Despite being minimally invasive, it remains underutilised in clinical practice, often due to misconceptions regarding technical difficulty and the perceived need for specialised equipment [49].
4.2.2. Gastrointestinal System
Sampling within the gastrointestinal system ranged from the oral mucosa and bile to faeces and perianal sites. Ultrasound-guided cholecystocentesis was used for bile, reflecting high technical standard [51]. Faecal samples were typically collected manually, whereas swabs were commonly used for oral mucosa and perianal sites. Swab-based collection may limit bacterial representation due to smaller sample volumes. However, modern swab, such as flocked swabs with dedicated transport media, have substantially improved culture recovery and overall specimen quality [52].
Rectal swabs, in particular, have been highlighted as a practical alternative to bulk faecal samples. Their ease of collection and transport supports surveillance of multidrug-resistant organisms (VRE, CRE) [53]. In addition, swabs have demonstrated comparable sensitivity to faecal specimens for enteric bacterial culture, and recent PCR-based studies indicate equivalent diagnostic performance for Clostridium difficile infection, enabling faster turnaround times and improved infection control [54]. Despite their practicality, swabs still pose several limitations. In humans, inadequate contact with mucosal surfaces can result in false-negative results, particularly in self-sampling contexts. Furthermore, rectal swabs have shown lower sensitivity than stool for real-time PCR detection of Giardia duodenalis, performing optimally only at higher parasite loads [55,56]. Nevertheless, multiple studies comparing rectal swabs and faecal samples in microbiota research have demonstrated strong correlations in bacterial community composition, diversity, and inferred functional pathways, with additional metabolomic analyses confirming high concordance across most metabolites [57,58].
Overall, rectal swabs, especially when collected using flocked designs and appropriate transport systems, represent a valid and efficient alternative to faecal samples for bacterial culture, molecular diagnostics, and microbiota profiling. Their use should, however, take into account sampling adequacy, reduced volume of collected material, and potential variation in sensitivity across different target organisms.
4.2.3. Integumentary System
Samples from the integumentary system encompassed the widest diversity of specimen types in this review, including abscesses or wounds, crusts, epidermal collarettes, external and middle ear canals, nails, pustules, pyoderma, general skin lesions and surgical sites. Prior cleansing and debridement is essential to minimise contamination and recover true pathogens rather than surface colonisers [59].
For surface-accessible lesions, such as crusts, epidermal collarettes, the external ear canal, skin in general and surgical sites, swab collection remains the most recommended and practical because of its ease of use and minimal invasiveness [60]. Moreover, comparative studies in human skin-microbiome research indicate that swabs effectively capture superficial microbiota, although the yield of viable bacteria may be lower than that obtained with deeper sampling methods [61].
In contrast, for lesions extending into deeper tissue (such as abscesses, wounds with pus, or pustules), fine-needle aspiration is preferred, as it allows direct access to the focus of infection while minimising surface contamination [59]. Interestingly, our review identified several studies that recommended transferring aspirated material onto a swab before submission. However, this practice may inadvertently reintroduce surface contamination and undermine one of the principal advantages of aspiration, particularly direct sampling of the lesion core. Therefore, this approach warrants caution in the context of veterinary dermatologic microbiology protocols.
For middle ear sampling, myringotomy is the recommended procedure, as it provides access to the middle ear exudate while minimising contamination from the external ear canal. This procedure is particularly relevant in chronic or refractory cases of otitis media, in which cultures obtained directly from the middle ear cavity yield more representative microbiological data [62].
In cases of pyoderma, biopsy sampling is advised. In human medicine, studies comparing superficial swabs and deep-tissue biopsies in skin and soft tissue infections have shown that biopsies offer greater sensitivity and more accurate pathogen identification [63]. This finding supports similar recommendations for veterinary pyoderma, particularly when empirical therapy fails or when a deep-seated infection is suspected.
Finally, for nail samples, the choice between blade scraping or swabbing depends on the lesion type and the suspected pathogen. For superficial nail plate colonisation, a moistened swab may be sufficient, whereas for subungual or peri-ungual involvement, scraping with a sterile blade yields better diagnostic material [64].
4.2.4. Musculoskeletal System
Tissue and post-mortem tissue, as well as synovial fluid were included. Biopsy collection was the preferred method for tissue, with specimens commonly placed in plain tubes or tubes containing a clot activator [65]. In addition, partially immersion of tissue specimens in transport medium represents good practice, as it helps to prevent desiccation and preserves the viability of infectious agents during transport and storage [66].
Synovial fluid should be aspirated aseptically [67], handled under sterile conditions to minimise contamination [67]. For microbiological analysis, transfer of the sample into plain containers is recommended, as EDTA interferes with bacterial growth and may compromise culture results [68]. Alternatively, direct inoculating into blood culture bottles has been shown to enhance microbial detection and overall diagnostic yield [69]. Nevertheless, transferring aspirates onto swabs is discouraged due to contamination risks, as discussed previously.
4.2.5. Ocular System
For conjunctival sampling, several techniques have been described in the selected studies. Before sample collection, when dyes or topical anaesthetics have been applied, the ocular surface should be thoroughly rinsed with sterile saline or sterile water to ensure optimal detection of ocular pathogens [70]. In human medicine, conjunctival samples are typically obtained using a sterile ocular swab, which is finer, softer and less traumatic, particularly suitable for small animals [71,72]. These swabs are commonly pre-moistened with sterile saline and gently rolled over the lower bulbar conjunctiva or fornix and, when indicated, along the lid margin, while carefully avoiding contact with the eyelashes and cornea [70]. Notably, flocked swabs have been shown to enhance cellular and microbial recovery when compared with conventional cotton swabs [73].
Consistent with these findings, in a study investigating the ocular surface microbiome, the lower conjunctiva was swabbed three times using either a flocked or a cotton swab, with flocked swabs yielding a higher microbial recovery, supporting their preferential use for ocular surface sampling [74]. Following collection, the swab is either placed directly into an appropriate transport medium or into a sterile dry tube, showing no significant differences if processed promptly [70,75]. It has also been recommended that, even in cases of unilateral disease, samples should be collected from both eyes (infected and non-infected) to help differentiate true pathogens from commensal flora [70].
4.2.6. Reproductive System
Reproductive sampling was sparsely reported, despite its clinical relevance in breeding animals. The two studies addressing this system described a wide range of sample types, including vaginal, uterine, and mammary gland samples, as well as prostate and semen collections. Most specimens were placed in sterile containers, whereas the use of swabs was recommended only for semen sampling.
Evidence from human medicine underscores that, when tissue or fluid is collected from deeper reproductive organs, such as the uterus or endometrium, strict aseptic conditions and careful handling are essential to minimise contamination, which could otherwise compromise data interpretation [76]. Similarly to ocular sampling, flocked swabs may also be employed for reproductive tract specimens, as their design allows enhanced recovery of epithelial cells and microorganisms while minimising trauma, and their use has already been reported in studies of the female reproductive tract [77]. Semen sampling for microbiome or fertility assessment in human medicine typically involves collecting the entire ejaculate into a sterile container following a period of abstinence, ensuring appropriate genital hygiene, and maintaining controlled time and temperature conditions before processing [78].
4.2.7. Respiratory System
Upper airway samples (ranging from the nostrils to the sinuses) were most frequently obtained using swabs or biopsies performed under rhinoscopic guidance. Flocked swabs may also be suitable for sample collection, as previously described for ocular and reproductive sampling [79]. This approach is considered practical because it is minimally invasive, allows targeted sampling of relevant mucosal sites, and has demonstrated good diagnostic performance in human medicine, where upper respiratory swabs show pooled sensitivity and specificity values of approximately 91% and 98%, respectively, for pathogen detection [80].
In contrast, sampling of the lower airways typically relies on bronchoalveolar lavage (BAL), tracheal wash, or bronchial brush techniques. BAL is widely regarded as the gold standard for lower respiratory tract sampling because it minimises contamination from upper airway flora and provides a high diagnostic yield [81]. A recent review in paediatric human patients further supports the diagnostic yield and safety of BAL, highlighting potential parallels with companion animal practice [82]. The procedure involves advancing the bronchoscope into the bronchopulmonary segment of interest until wedged, followed by instillation of 100–300 mL of sterile saline, with at least 30% of the instilled volume retrieved for optimal analysis [81]. The sample should be collected in a labelled sterile container and transported promptly to the laboratory [81]. However, some comparative studies have reported that tracheal aspirates and BAL fluid may exhibit similar microbial diversity, suggesting that less invasive approaches can still yield representative results in certain clinical contexts [83].
Notably, two of the three reviewed studies recommended transferring the aspirate onto a swab after collection. However, this practice may increase the risk of contamination and compromise downstream microbiological analyses. In line with human medical protocols, lower airway aspirates should instead be placed directly into a sterile container to preserve sample integrity [84].
Additionally, pleural fluid samples were collected via thoracocentesis or through indwelling catheters under aseptic conditions, using non-anticoagulant tubes. Although these recommendations were reported in only one of the reviewed studies, this approach represents best practice [85].
4.2.8. Urinary System
The urinary system was the most frequently investigated, showing relatively good alignment with established best practices. Cystocentesis was the preferred collection method, reflecting awareness of its greater reliability in reducing contamination when compared with midstream voided samples or catheterisation [86,87]. Although two studies reported the use of preservatives such as boric acid and four referred to the use of sterile containers, plain sterile containers remain appropriate for urine collection when samples can be promptly refrigerated and analysed within the recommended time frame (Section 4.4) [88,89]. Consequently, the choice between a plain sterile container and a tube containing a preservative is primarily determined by the expected storage and transport conditions (Section 4.5).
4.3. Impact of Antimicrobial Therapy Before Sampling
Consideration of antibiotic exposure prior to sample collection was notably inconsistent across the seventeen included studies. While a few studies defined withdrawal periods (either 4 weeks or 72 h) or recorded whether animals had received antibiotics, others required formal reporting of ongoing therapy or recommended sampling before antibiotic initiation. However, nearly half of the studies did not report any information regarding prior or ongoing antibiotic use; four were cross-sectional studies, and one was a case report, in which antibiotic exposure would not have been relevant given the study design and scope. This lack of standardisation represents a significant methodological limitation, particularly considering the well-documented suppressive effect of antibiotics on bacterial recovery [90]. Even short-term systemic antimicrobial exposure can exert a post-antibiotic effect, transiently inhibiting bacterial regrowth and thereby reducing culture sensitivity [91,92]. For example, in respiratory sampling, BAL, despite being considered the gold standard, has been shown to exhibit markedly reduced sensitivity following antimicrobial treatment, especially for fastidious microorganisms. In such cases, molecular assays such as PCR have proven to be valuable complementary diagnostic tools [81]. In both clinical and research contexts, failure to account for prior antibiotic exposure may result in false-negative culture results or underestimation of antimicrobial resistance prevalence [93,94]. Beyond their immediate microbiological impact, antibiotics can induce profound and long-lasting alterations in host-associated microbiota, reducing microbial diversity and disturbing ecological balance [95]. These dysbiotic shifts can persist for months or even years, depending on the drug spectrum and duration of treatment, thereby weakening colonisation resistance and facilitating opportunistic infections, such as Clostridium difficile and Salmonella Typhimurium [96]. Collectively, these effects highlight the broader consequences of antibiotic exposure and underscore the importance of accurate antibiotic use, as well as the adoption of precision veterinary medicine approaches in which therapeutic decisions are guided by culture and susceptibility testing, thereby reinforcing antibiotic stewardship in veterinary practice [96]. Therefore, whenever clinically feasible, samples should ideally be collected before starting antibiotic therapy. When this is not possible, sampling should be delayed until at least seven days after the last antibiotic dose, particularly in cases involving chronic or deep-seated infections or when long-acting antibiotics have been administered [23,97,98]. In such situations, complementing culture with molecular methods (e.g., PCR or metagenomic sequencing), together with careful documentation of prior antibiotic exposure, becomes essential to ensure accurate interpretation of results [97].
4.4. Bacterial Target
The bacterial groups investigated varied according to the sample type and its anatomical origin (Figure 3). In general, cultures targeting aerobic bacteria were recommended for specimens obtained from sites naturally exposed to atmospheric oxygen, such as oral mucosa, external and middle ear, nails, surgical sites, conjunctiva, vagina, uterus, mammary gland, testicles, prostate, upper and lower airways, and urine. This approach is consistent with standard practices in human clinical microbiology [99,100].
With regard to urine sampling, although some authors advocate investigation of anaerobic bacteria in suspected cases of emphysematous cystitis, this condition is uncommon and is usually caused by aerobic, gas-producing bacteria, including Escherichia coli (the predominant pathogen), Klebsiella spp. and Proteus spp. [101,102]. Anaerobes such as Clostridium perfringens are only rarely implicated in urinary tract infection, and it is only in these exceptional cases that routine aerobic culture may be insufficient [103].
In contrast, samples derived from body cavity effusions, bile, abscesses, wounds, crusts, epidermal collarettes, pustules, pyoderma and pleural fluid should include investigation for both aerobic and anaerobic organisms, as these sites are frequently infected by mixed bacterial populations [99,100,104]. Similarly, for cerebrospinal fluid, blood, faeces, tissue, synovial fluid, and semen, combined aerobic and anaerobic testing is advisable, given that anaerobic pathogens can occasionally cause infections at these sites [99,105,106,107]. Post-mortem tissue samples additionally require targeted investigation for Campylobacter jejuni, Yersinia spp., and Salmonella spp., as well as faecal sampling, mirroring established protocols in human medicine [108].
In summary, superficial or air-exposed samples typically warrant aerobic cultures alone, whereas samples obtained from deeper or normally sterile anatomical sites (e.g., inner ear, blood, body cavity effusions, and deep abscesses) should prompt consideration of both aerobic and anaerobic culture strategies.
4.5. Storage and Transport Conditions
Storage and transport conditions were inconsistently described across the included studies, with critical details such as temperature and duration often omitted (Figure 4). For aerobic bacteria, refrigeration at approximately 4 °C for up to 24–48 h was the most commonly recommended condition and is consistent with general microbiological standards [109]. Ideally, samples should be transported to the laboratory within two hours of collection [99]. Bayley and colleagues further emphasise that for certain samples, such as body cavity effusions, CSF, and biopsy tissues, the interval between collection and processing should not exceed 15 min if refrigeration or appropriate transport media are not available [99]. These authors also note that when immediate processing upon arrival is not possible, specimens must be stored under suitable conditions; for example, urine, faeces, sputum, swabs, and indwelling devices (e.g., catheters) should be kept at 4 °C, whereas tissues requiring long-term storage should be frozen at −70 °C [99].
Beyond these general principles, several specimen-specific considerations emerged. Human urinalysis guidelines indicate that when immediate examination (within 30 min) is not feasible, urine should be refrigerated at 4 °C and analysed within 12 h to limit bacterial proliferation [88]. If refrigeration is not feasible, containers pre-filled with preservatives such as boric acid may be used [110]. Boric acid can maintain leukocyte integrity and stabilise bacterial counts for up to 24 h at approximately 20 °C; however, its use may impair the recovery of certain bacteria, notably Pseudomonas spp. [110]. For ocular samples, particularly conjunctival swabs, standard ophthalmic microbiology protocols recommend immediate transport at room temperature. When delays are unavoidable, samples should be placed in an appropriate transport medium and/or refrigerated to prevent desiccation and preserve bacterial viability [70].
For blood samples, some studies indicate that no significant loss in yield occurs when blood cultures are stored for less than 24 h at 25 °C [111,112]. However, guidelines recommend a maximum pre-analytical interval of 2 h from collection to incubation [99,113]. Notably, each hour elapsed from blood collection to incubation has been associated with a decrease of 0.3% in the probability of a positive result, highlighting the importance of rapid processing to maintain diagnostic accuracy [113].
Temperature control is a critical determinant of sample integrity, as it minimises enzymatic activity and uncontrolled bacterial growth. This is typically achieved through short-term refrigeration (2–8 °C) or deep freezing (−80 °C) for long-term storage [114,115]. Nevertheless, several reports described storage at room temperature for up to 72 h, a practice known to reduce bacterial viability and alter microbial community structure, particularly in microbiome-targeted analyses [116,117].
With respect to anaerobic bacteria, approximately one-third of studies recommended maintaining samples at ambient temperature for 24–72 h, while others suggested refrigeration without specifying a time limit. Current guidelines, however, recommend that anaerobic specimens be transported to the laboratory as rapidly as possible (ideally within 30 min) to minimise oxygen exposure and preserve microbial viability. Specimens collected in anaerobic transport media may be safely processed within up to two hours of collection [118,119].
Campylobacter spp. were rarely discussed, despite their clinical and epidemiological relevance [120]. Refrigeration for up to 48 h was the most common recommendation. However, Campylobacter species are highly sensitive to environmental conditions, including dehydration, atmospheric oxygen, sunlight, and temperature fluctuations [120,121]. Extreme temperatures (>20 °C or <0 °C) and fluctuations should therefore be avoided, with short-term storage at 4 °C (±2 °C) recommended when immediate processing is not possible. When collected using swabs, commercially available transport tubes containing protective media, such as Amies or charcoal-based, are advised to prevent desiccation and oxygen toxicity, while faecal material should be shipped in appropriate transport media, such as Cary-Blair or modified Cary-Blair [120,121].
While the above recommendations pertain primarily to culture-based analyses, molecular and nucleic acid–based techniques introduce additional pre-analytical considerations. Approaches such as immunohistochemistry, PCR, and Next-Generation Sequencing (NGS) require careful handling to preserve nucleic acids [122]. Samples often need rapid cooling, immediate processing, or stabilisers, and transport containers must not interfere with amplification or sequencing [123]. Non-invasive specimens may be suitable for molecular assays even when unsuitable for culture [124]. Failure to adhere to these pre-analytical precautions can reduce assay sensitivity, compromise nucleic acid integrity, and distort microbial composition, particularly in low-biomass or complex samples [125].
Overall, the substantial variability observed in storage conditions and handling procedures across studies exposes a major methodological gap between ideal laboratory standards and field implementation. The development and integration of validated, evidence-based veterinary guidelines, drawing from human diagnostic microbiology and supported by experimental validation, will be essential to improving culture accuracy, maintaining sample integrity and ensuring reproducible results across clinical and research settings.
4.6. Clinical and One Health Implications
The consequences of suboptimal or inconsistent sampling extend far beyond laboratory performance. Inaccurate or unreliable culture results undermine confidence in microbiological diagnostics, increasing the likelihood that clinicians resort to empirical or broad-spectrum antibiotic therapy [126]. This practice not only compromises individual patient care but also contributes to the emergence and dissemination of antimicrobial resistance (AMR) across animal and human populations [127].
Standardised sampling practices should therefore be regarded not merely as a technical refinement, but as a cornerstone of veterinary antibiotic stewardship and One Health-oriented AMR mitigation strategies. By improving the reliability of diagnostic results, standardisation enables clinicians to prescribe antibiotics less frequently and more judiciously, with greater confidence in therapeutic decision-making [128].
Notably, stressful handling during sample collection can trigger neuroendocrine responses that modulate host immunity and directly influence bacterial growth and microbiota composition [129,130]. Consequently, inadequate stress management may compromise the timing, precision, and quantity of the collected specimen, while operator skill directly affects its representativeness and the microbial species identified [131].
In addition, environmental and operator-induced contamination further threatens sample integrity, as clinical environments and surfaces can harbour diverse bacterial species that may confound microbiological results, and guidelines for sample collection explicitly emphasise avoiding cross-contamination between animals, instruments, and surroundings to preserve sample integrity [132,133]. In low-biomass samples, contaminants introduced during sampling workflows may even outweigh the true microbial signal, underscoring the necessity of stringent contamination control measures [134].
Importantly, bacterial identification in most studies is intrinsically linked to antibiotic susceptibility testing, which directly informs antibiotic choice. However, prior antimicrobial therapy can influence both the likelihood of pathogen recovery and the resulting susceptibility profile, potentially leading to false-negative cultures or biassed antibiograms [135,136]. Failure to account for such effects may therefore compromise both diagnostic accuracy and downstream clinical decisions.
Beyond pre-analytical factors, rapid diagnostic tools can mitigate some limitations associated with suboptimal sampling [137]. Techniques such as MALDI-TOF and FTIR spectroscopy allow fast and accurate bacterial identification, often within hours, enabling clinicians to initiate targeted therapy quickly and reduce unnecessary antibiotic use, thereby limiting the development of multidrug-resistant organisms [138,139]. By complementing conventional culture and AST workflows, these technologies provide a bridge between sample quality and timely clinical decision-making, further supporting veterinary antibiotic stewardship and One Health objectives. Enhanced communication between clinicians and diagnostic laboratories is also essential. The adoption of standardised guidelines detailing appropriate sampling methods, storage, and transport conditions, together with explicit documentation of prior or ongoing antibiotic therapy, substantially enhances the interpretability and clinical relevance of culture and susceptibility results. Likewise, consistent laboratory feedback regarding specimen quality can foster continuous improvement in sampling practices and strengthen collaboration between clinical and laboratory teams (Figure 5).
5. Conclusions
This systematic review underscores the variability and existing gaps in microbiological sampling practices for companion animals. Inconsistent reporting of sample collection, handling, storage, and transport, along with limited documentation of critical factors such as prior antibiotic exposure, compromises the reliability of culture, diagnostic accuracy, and result interpretation. Although veterinary practice faces unique logistical and biological challenges, adopting and appropriately adapting evidence-based approaches from human diagnostic microbiology offers a promising path to improve outcomes. Overall, these findings highlight the urgent need for harmonised, species-specific, and evidence-based protocols that balance clinical feasibility with microbiological integrity. Strengthened collaboration between veterinary practitioners and diagnostic laboratories will be essential to translate these recommendations into routine practices, thereby supporting antibiotic stewardship and One Health objectives.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Morency-Potvin P. Schwartz D.N. Weinstein R.A. Antimicrobial Stewardship: How the Microbiology Laboratory Can Right the Ship Clin. Microbiol. Rev.20173038140710.1128/CMR.00066-1627974411 PMC 5217798 · doi ↗ · pubmed ↗
- 2Guardabassi L. Apley M. Olsen J.E. Toutain P.-L. Weese S. Optimization of Antimicrobial Treatment to Minimize Resistance Selection Microbiol. Spectr.2018663767310.1128/microbiolspec.ARBA-0018-2017 PMC 1163357529932044 · doi ↗ · pubmed ↗
- 3Monteiro H.I.G. Silva V. de Sousa T. Calouro R. Saraiva S. Igrejas G. Poeta P. Antimicrobial Resistance in European Companion Animals Practice: A One Health Approach Animals 202515170810.3390/ani 1512170840564260 PMC 12189186 · doi ↗ · pubmed ↗
- 4Scott Weese J. Antimicrobial Resistance in Companion Animals Anim. Health Res. Rev.2008916917610.1017/S 146625230800148518983722 · doi ↗ · pubmed ↗
- 5Miller J.M. Binnicker M.J. Campbell S. Carroll K.C. Chapin K.C. Gilligan P.H. Gonzalez M.D. Jerris R.C. Kehl S.C. Patel R. A Guide to Utilization of the Microbiology Laboratory for Diagnosis of Infectious Diseases: 2018 Update by the Infectious Diseases Society of America and the American Society for Microbiologya Clin. Infect. Dis.201867 e 1e 9410.1093/cid/ciy 38129955859 PMC 7108105 · doi ↗ · pubmed ↗
- 6Meinkoth J.H. Allison R.W. Sample Collection and Handling: Getting Accurate Results Vet. Clin. N. Am. Small Anim. Pract.20073720321910.1016/j.cvsm.2006.11.00817336671 · doi ↗ · pubmed ↗
- 7Miller J.M. Poorly Collected Specimens May Have a Negative Impact on Your Antibiotic Stewardship Program Clin. Microbiol. Newsl.201638434810.1016/j.clinmicnews.2016.03.001 · doi ↗
- 8De Briyne N. Atkinson J. PokludováL. Borriello S.P. Price S. Factors Influencing Antibiotic Prescribing Habits and Use of Sensitivity Testing amongst Veterinarians in Europe Vet. Rec.201317347510.1136/vr.10145424068699 PMC 3841786 · doi ↗ · pubmed ↗