Epstein–Barr Virus Infection Is Associated with an Elevated Tumor–Stroma Ratio and Older Age in Oral Squamous Cell Carcinoma
Eris Nurul Rahmadhini, Irna Sufiawati, Hasrayati Agustina, Okky Husain, Seto Adiantoro Sadputranto, Adi Idris

TL;DR
This study finds that Epstein-Barr virus (EBV) infection in oral cancer is linked to older age and a higher tumor-stroma ratio, suggesting a unique tumor environment.
Contribution
The study identifies a novel association between EBV positivity and elevated tumor-stroma ratio in oral squamous cell carcinoma.
Findings
EBV positivity was significantly associated with older age (p = 0.046).
All EBV-positive tumors exhibited a high tumor–stroma ratio (p = 0.031).
No significant associations were found between EBV status and tumor-infiltrating lymphocytes or clinical stage.
Abstract
Epstein–Barr virus (EBV) is an oncogenic virus implicated in several epithelial malignancies; however, its role in the tumor microenvironment of oral squamous cell carcinoma (OSCC) remains unclear. This study investigated the association between EBV infection and clinicopathological and microenvironmental features of OSCC. A cross-sectional analysis was conducted on 62 archived OSCC biopsy specimens. EBV was detected using polymerase chain reaction (PCR), and clinical data were obtained from medical records. Tumor–stroma ratio (TSR), perineural invasion (PNI), lymphovascular invasion (LVI), and histological differentiation were assessed microscopically, while tumor-infiltrating lymphocytes (TILs) were quantified using ImageJ software version 1.54j (National Institutes of Health, Bethesda, MD, USA). EBV DNA was identified in 43.5% of cases. EBV positivity was significantly associated…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
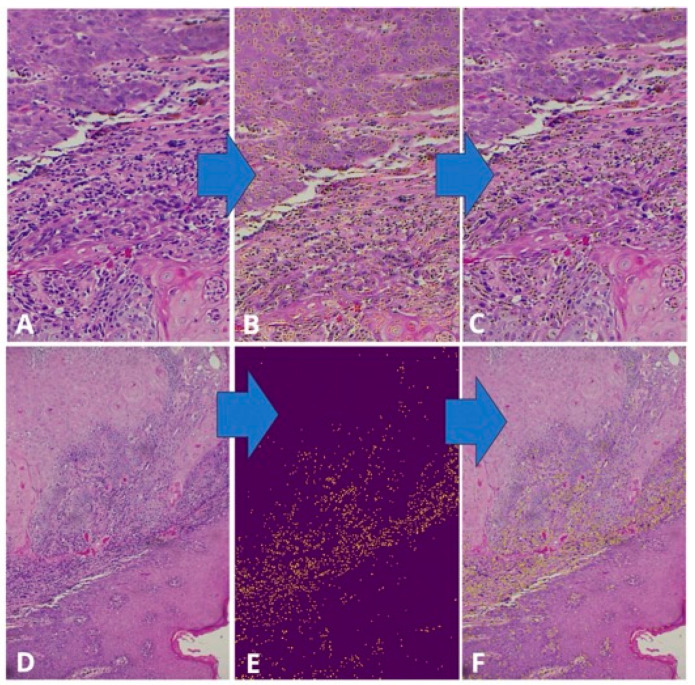 Figure 1
Figure 1 Figure 2
Figure 2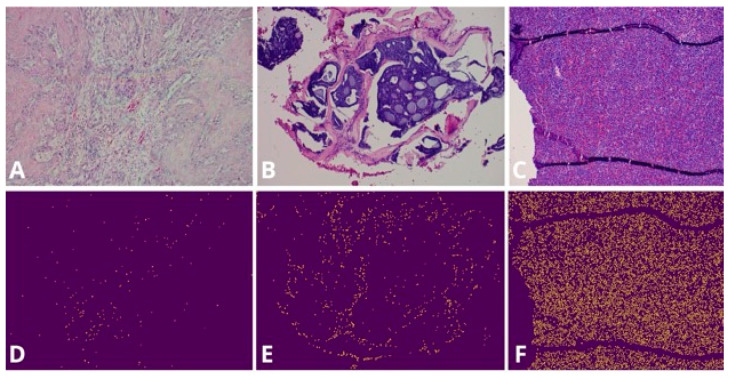 Figure 3
Figure 3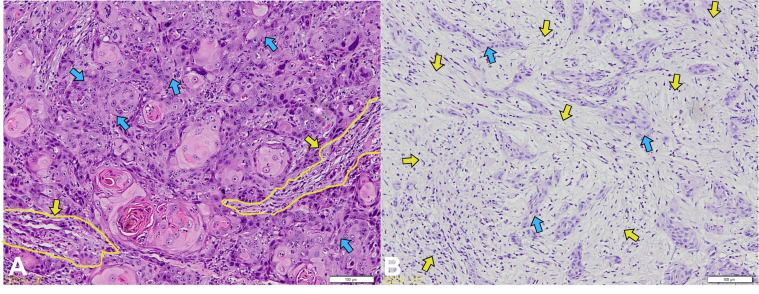 Figure 4
Figure 4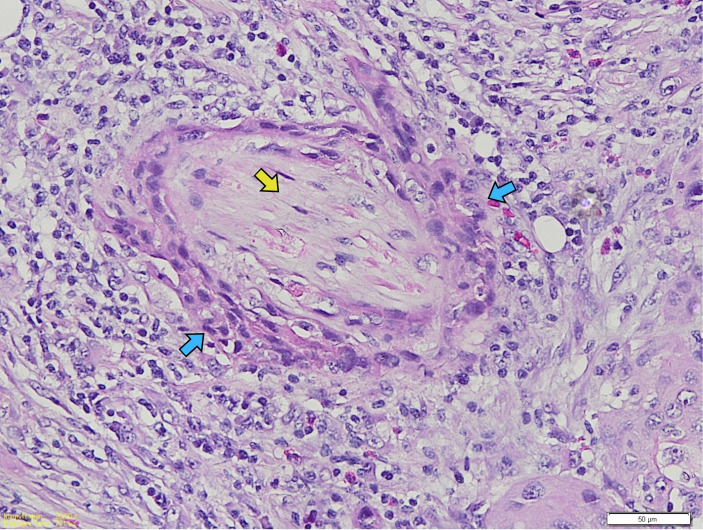 Figure 5
Figure 5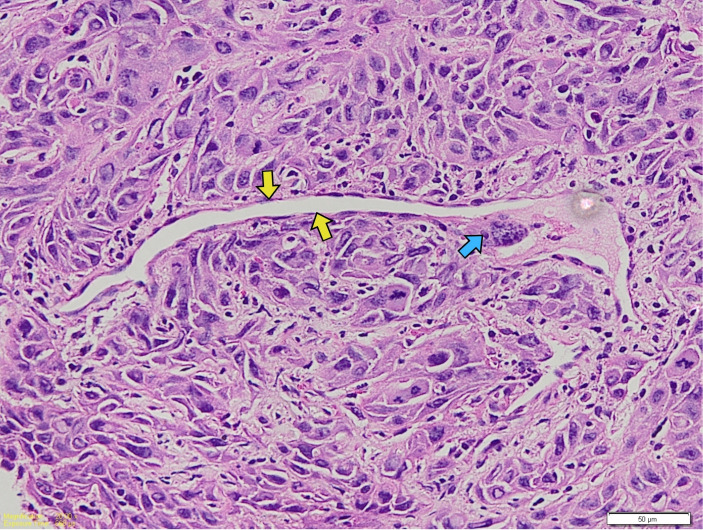 Figure 6
Figure 6 Figure 7
Figure 7- —Ministry of Higher Education, Science, and Technology of the Republic of Indonesia
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral-associated cancers and disorders · Head and Neck Cancer Studies · Cervical Cancer and HPV Research
1. Introduction
Oral squamous cell carcinoma (OSCC) accounts for approximately 90% of oral cancers and represents the most prevalent oral malignancy [1,2,3,4]. Major risk factors include tobacco use, alcohol consumption, betel nut chewing, ultraviolet radiation, genetic and nutritional factors, and viral infections [1].
Epstein–Barr virus (EBV) is a ubiquitous oncogenic herpesvirus with a well-established role in several epithelial and lymphoid malignancies. EBV infection of oral epithelial cells has been demonstrated in experimental models, suggesting that the virus is capable of infecting and persisting within oral squamous cells [5]. In addition, molecular studies have shown that EBV may influence epithelial cell behavior through delayed differentiation, epigenetic reprogramming, and metabolic alterations, including activation of the Warburg effect, which are implicated in cancer-related pathways such as cell proliferation, migration, invasion, and resistance to apoptosis [6].
In clinical settings, EBV DNA has been detected in a subset of oral and oropharyngeal squamous cell carcinomas, with meta-analyses reporting a relatively high prevalence of EBV infection in these tumors compared with non-cancer controls [7]. Co-infection with EBV and HPV has been detected in 15–20% of carcinomas occurring in the oropharynx [8,9,10]. In a previous systematic review and meta-analysis, EBV and HPV co-infection was identified in a subset of oral and oropharyngeal squamous cell carcinomas, which suggests a biological interaction between oncogenic viruses in head and neck cancers [11]. Nevertheless, the clinical and histopathological relevance of EBV infection in OSCC, independent of or in conjunction with other viral infections, has not been fully elucidated.
The prognosis for oral cancer patients remains unfavorable, with the 5-year survival rate for oral cancer patients being below 50%, dropping to less than 30% in advanced stages, and not significantly improving in recent decades. Many factors, including EBV infection in oral cancer, are associated with increased tumor aggressiveness, which negatively impacts prognosis by facilitating tumor development [7,8]. Important factors related to the survival of cancer patients can include clinical, such as age, gender, cancer location, cancer stage, and histopathological parameters, including tumor-infiltrating lymphocytes (TILs), tumor–stroma ratio (TSR), perineural invasion (PNI), lymphovascular invasion (LVI), and degree of differentiation. Clinical and histopathological parameters are very useful in accurately assessing the biological aggressiveness of oral cancer and enabling the development of customized treatment plans for each specific cancer [12,13,14].
Understanding how EBV infection influences the tumor microenvironment provides valuable insights into tumor immunobiology and may uncover new therapeutic vulnerabilities. EBV-driven modulation of immune infiltration, stromal composition, and metabolic pathways could affect disease progression and treatment response. Therefore, this study aimed to analyze the association between EBV status and clinicopathological as well as microenvironmental parameters in oral squamous cell carcinoma, highlighting its potential relevance as a biomarker and therapeutic target.
2. Materials and Methods
2.1. Study Design and Sample Selection
This study utilized a comparative analytical design with a cross-sectional approach. Patients aged 18 years or older with oral cavity cancer who had not received prior chemotherapy or radiotherapy were screened for eligibility according to predefined inclusion criteria. Fresh tumor tissue specimens were initially used for EBV detection by polymerase chain reaction (PCR). The same specimens were then processed into formalin-fixed, paraffin-embedded (FFPE) blocks and subjected to hematoxylin and eosin (H&E) staining to confirm the diagnosis of OSCC and to assess histopathological parameters, including TILs, TSR, PNI, LVI, and degree of differentiation. Cases with damaged, insufficient, or unreadable tissue specimens were excluded.
Based on these criteria, a total of 62 OSCC cases met the inclusion requirements and were included in the final analysis. All samples were anonymized before analysis, and the study was conducted in accordance with institutional ethical standards.
2.2. EBV Detection
Genomic DNA was extracted from fresh tumor tissue using standard laboratory protocols. Epstein–Barr virus (EBV) DNA detection was performed with a commercial multiplex real-time PCR assay (Novaplex™ EBV assay, Seegene, Seoul, Republic of Korea) in accordance with the manufacturer’s instructions. PCR amplification and detection were carried out on a Bio-Rad Opus CFX96 real-time PCR system (Bio-Rad Laboratories, Hercules, CA, USA).
The assay utilizes proprietary primer and probe sets that target EBV-specific genomic regions and other Herpesviridae family members. Each PCR run included internal, positive, and negative controls supplied by the manufacturer. EBV positivity was determined based on amplification curves and cycle threshold (Ct) values following the predefined criteria outlined in the assay manual. Human papillomavirus (HPV) status was assessed separately using a dedicated HPV PCR assay as part of routine molecular diagnostics.
In this study, EBV positivity was defined as the presence of EBV DNA, either as a single infection or in combination with HPV. Cases exhibiting HPV infection without EBV were excluded from the analysis, while the presence of other non-HPV viruses detected by the multiplex assay was not included in the analytical model. To ensure transparency, the distribution of EBV-only cases and EBV–HPV co-infected cases is reported separately in the Section 3.
2.3. Clinical Parameters
Clinical parameters, including age, gender, tumor location, and cancer stage, were extracted from patients’ medical records and radiological evaluations employing computed tomography (CT) scans. Age was categorized into four groups for descriptive and analytical purposes: 18–30 years, 31–45 years, 46–60 years, and >60 years, based on clinical relevance.
2.4. Histopathological Assessment
Histopathological analyses were performed using stored biological material (SBM) in the form of formalin-fixed, paraffin-embedded (FFPE) tumor tissue sections. Hematoxylin and eosin (H&E)-stained slides were reviewed by an experienced anatomical pathologist who was blinded to EBV status.
Tumor–stroma ratio (TSR) was evaluated at the invasive tumor front. TSR was classified as high when tumor cells occupied more than 50% of the selected microscopic field (stroma-poor tumors) and low when stromal components occupied more than 50% of the field (stroma-rich tumors). Perineural invasion (PNI) and lymphovascular invasion (LVI) were recorded as present or absent based on established histopathological criteria. Degree of differentiation was classified as well-, moderately-, or poorly differentiated according to Broders’ criteria. Quantitative assessment of tumor-infiltrating lymphocytes (TILs) was performed on H&E-stained sections using ImageJ software (National Institutes of Health, Bethesda, MD, USA). TILs were quantified as the proportion of stromal area occupied by mononuclear inflammatory cells following standardized evaluation guidelines (Figure 1).
2.5. Statistical Analysis
Statistical analyses were conducted using SPSS Version 30.0 for Windows (IBM Corp., Armonk, NY, USA). Categorical variables, such as age, sex, tumor location, TSR, PNI, LVI, and cancer stage, were analyzed using either the Chi-square test or Fisher’s exact test, as appropriate. Results for these variables are reported as frequencies and percentages. The Shapiro–Wilk test assessed the normality of the TIL data. Because the data were not normally distributed, the Mann–Whitney U test was used for comparisons, with results reported as median (minimum–maximum) values. All statistical tests were two-tailed, and statistical significance was defined as p < 0.05.
3. Results
A total of 62 oral cancer samples were analyzed, of which 27 (43.5%) were EBV-positive, and 35 (56.5%) were EBV-negative. Among the EBV-positive cases, 17 samples (63.0%) showed EBV infection alone, while 10 samples (37.0%) demonstrated EBV co-infection with other viruses, including cytomegalovirus (CMV), human herpesvirus-7 (HHV-7), and high-risk human papillomavirus (HPV) types 16 and 33. Samples positive for HPV alone without EBV were excluded from the analysis.
3.1. Clinical Characteristics
The distribution of clinical characteristics according to EBV status is summarized in Table 1. A significant association was observed between EBV status and age (p = 0.046). EBV-positive cases were more frequently identified in patients aged over 60 years (37.0%) compared with EBV-negative cases (11.4%). No significant associations were found between EBV status and gender (p = 0.585), tumor site (p = 0.239), or cancer stage (p = 0.406). Although not statistically significant, male patients constituted a slightly higher proportion of EBV-positive cases (55.6%) compared with EBV-negative cases (48.6%). The tongue was the most common tumor site overall, accounting for 41.9% of cases, and 44.4% of EBV-positive tumors (Figure 2). Advanced disease was predominant in both groups, with stage 4a being the most frequent stage among EBV-positive cases (64.0%).
3.2. Histopathological Parameters
Histopathological findings according to EBV status are presented in Table 2. The median TIL count was slightly higher in EBV-positive cases (median 467; range 78–1221) than in EBV-negative cases (median 392; range 73–1463); however, this difference was not statistically significant (p = 0.994) (Figure 3).
In contrast, a significant association was observed between EBV status and TSR (p = 0.031). All EBV-positive tumors exhibited a high TSR (100%), whereas 82.9% of EBV-negative tumors showed a high TSR (Figure 4).
No significant associations were identified between EBV status and PNI (p = 0.308) or lymphovascular invasion (LVI) (p = 0.136). Nevertheless, the proportions of PNI (22.2% vs. 11.4%) and LVI (37.0% vs. 20.0%) were higher in EBV-positive cases compared with EBV-negative cases (Figure 5 and Figure 6).
Tumor differentiation grade did not differ significantly according to EBV status (p = 0.584). Moderately differentiated tumors were more common among EBV-positive cases (40.0%) compared with EBV-negative cases (25.0%), whereas well-differentiated tumors predominated in the EBV-negative group (60.0%) (Figure 7).
4. Discussion
This study showed that EBV DNA was found in 43.5% of oral squamous cell carcinoma (OSCC) cases, which means that EBV infection is relatively common in this group. This prevalence aligns with previous meta-analyses indicating EBV detection rates of roughly 40–50% in oral and oropharyngeal squamous cell carcinomas [7]. However, the present findings should be interpreted as an association rather than evidence of a causal role of EBV in oral carcinogenesis.
Among the clinical parameters evaluated, age was the only factor significantly associated with EBV status. EBV-positive tumors were more frequently observed in patients older than 60 years. This finding may be attributable to age-related immunosenescence, chronic inflammation, and cumulative genomic alterations, all of which can facilitate viral persistence or reactivation [15,16,17,18]. Previous studies have demonstrated that aging is accompanied by impaired immune surveillance and epigenetic changes, such as DNA hypermethylation, which may influence host–virus interactions [18,19]. However, the cross-sectional design of this study limits the ability to conclude temporal or causal relationships.
No significant associations were identified between EBV status and gender, tumor location, or cancer stage. Although a slightly higher proportion of males was observed among the EBV-positive cases, this difference did not reach statistical significance and may have been influenced by behavioral or environmental factors rather than virus-specific effects [20,21]. The tongue was the most frequent tumor site in both the EBV-positive and EBV-negative groups, consistent with prior reports. Keratinized squamous epithelium on the tongue, especially the lateral edges and base, has numerous CD21 receptors and lymphoid tissue, facilitating EBV entry [22]. Advanced-stage disease predominated in this cohort, which may reflect delayed diagnosis and healthcare access rather than differences related to viral status [23].
Regarding histopathological parameters, median TIL levels were numerically higher in the EBV-positive tumors, although this difference did not reach statistical significance. Increased lymphocytic infiltration may reflect host immune recognition of viral antigens; however, effective antitumor immunity may be compromised by EBV-associated immune evasion mechanisms, including the modulation of immune checkpoint pathways, such as the PD-1/PD-L1 pathway, as reported in previous studies [19]. These findings underscore the complex interplay between viral infection and immune response within the tumor microenvironment.
A main finding of this study is the strong association between EBV status and TSR, as all EBV-positive tumors exhibited a high TSR. The TSR quantifies the proportion of tumor cells relative to stromal components within the tumor microenvironment and is recognized as a reliable histopathological marker associated with tumor behavior in head and neck squamous cell carcinoma, as supported by recent systematic reviews and meta-analyses [24]. Although evidence regarding the relationship between EBV infection and TSR in OSCC remains limited, prior studies suggest that EBV may modulate tumor metabolism and the composition of the microenvironment, including increased glycolytic activity consistent with the Warburg effect and altered tumor–stroma interactions [6,25]. The Warburg effect has been associated with tumor–microenvironment interactions in experimental cancer models [6]. These mechanisms may contribute to a stroma-poor tumor phenotype and affect tumor growth dynamics as well as the distribution of immune cells within the tumor microenvironment [6,25]. However, these biological processes were not directly assessed in the present study and should be interpreted with caution. Collectively, the results indicate that the observed association between EBV status and a high TSR is biologically plausible based on existing experimental evidence, although interpretative limitations of this study remain.
No statistically significant associations were observed between EBV status and perineural invasion (PNI) or lymphovascular invasion (LVI). Although higher proportions of PNI and LVI were observed in EBV-positive tumors, these differences did not reach statistical significance and may be influenced by sample size limitations. Previous studies have reported that EBV-related signaling pathways, including NF-κB and JAK/STAT activation, may promote invasive tumor behavior [6,18,26]. However, the present findings do not support a definitive association between EBV status and these invasive features in OSCC.
Regarding tumor differentiation, no significant relationship was observed between EBV status and degree of differentiation. While a higher proportion of EBV-positive tumors exhibited well or moderately differentiated morphology, this observation did not reach statistical significance and is consistent with prior reports indicating variable associations between EBV infection and tumor differentiation in OSCC [7,27]. Immunological and microenvironmental factors may contribute to these patterns, although further investigation is required [28].
This study has several limitations. EBV detection relies on PCR analysis of tumor tissue, which does not allow for the localization of EBV infection within specific cell populations. As a result, it is unclear whether EBV DNA originated from malignant epithelial cells, infiltrating EBV-infected lymphocytes, or viral particles. The lack of EBER in situ hybridization is a significant limitation. Additionally, although HPV status was assessed, the small sample size prevented stratified analyses to fully evaluate the independent or combined effects of viral co-infection on TSR.
Despite these limitations, this study highlights an association between EBV infection and specific clinicopathological features, particularly older age and a high tumor-stroma ratio, in OSCC. These results deepen the understanding of potential virus-associated tumor microenvironmental characteristics and support the need for future studies incorporating cell-specific viral localization, molecular profiling, and larger patient cohorts to further clarify the role of EBV in oral squamous cell carcinoma.
5. Conclusions
This study indicates that EBV DNA was detected in a substantial proportion of OSCC cases. EBV positivity was significantly associated with older patient age and a high tumor–stroma ratio, suggesting that EBV infection may be linked to distinct clinicopathological and tumor microenvironment characteristics in OSCC. Other clinical and histopathological parameters, including tumor-infiltrating lymphocytes, perineural invasion, lymphovascular invasion, degree of differentiation, and cancer stage, were not significantly associated with EBV status.
Although these findings do not establish a causal role for EBV in oral carcinogenesis, they highlight a potential association between EBV presence and specific microenvironmental features. Given the limitations of PCR-based EBV detection and the absence of cell-specific viral localization, further studies incorporating EBER in situ hybridization, molecular profiling, and larger cohorts are warranted. Improved understanding of the relationship between EBV infection and the tumor microenvironment may help refine future risk stratification and the biological characterization of OSCC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ahuja S. Khan A.A. Zaheer S. Ranga S. Tumor-Infiltrating Lymphocytes in Oral Cavity Squamous Cell Carcinoma and Its Association with Clinicopathological Parameters Pathol. Res. Pract.202325115488210.1016/j.prp.2023.15488237898039 · doi ↗ · pubmed ↗
- 2Bray F. Laversanne M. Sung H. Ferlay J. Siegel R.L. Soerjomataram I. Jemal A. Global Cancer Statistics 2022: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries CA Cancer J. Clin.20247422926310.3322/caac.2183438572751 · doi ↗ · pubmed ↗
- 3Swidergall M. Leibund Gut-Landmann S. Immunosurveillance of Candida Albicans Commensalism by the Adaptive Immune System Mucosal Immunol.20221582983610.1038/s 41385-022-00536-535778599 PMC 9385492 · doi ↗ · pubmed ↗
- 4Sung H. Ferlay J. Siegel R.L. Laversanne M. Soerjomataram I. Jemal A. Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries CA Cancer J. Clin.20217120924910.3322/caac.2166033538338 · doi ↗ · pubmed ↗
- 5Heawchaiyaphum C. Iizasa H. Ekalaksananan T. Burassakarn A. Kiyono T. Kanehiro Y. Yoshiyama H. Pientong C. Epstein–Barr Virus Infection of Oral Squamous Cells Microorganisms 2020841910.3390/microorganisms 803041932188127 PMC 7144007 · doi ↗ · pubmed ↗
- 6Heawchaiyaphum C. Yoshiyama H. Iizasa H. Burassakarn A. Tumurgan Z. Ekalaksananan T. Pientong C. Epstein–Barr Virus Promotes Oral Squamous Cell Carcinoma Stemness through the Warburg Effect Int. J. Mol. Sci.2023241407210.3390/ijms 24181407237762374 PMC 10531857 · doi ↗ · pubmed ↗
- 7Rodriguez-Archilla A. LopatkováK. Alberto Rodriguez-Archilla C. Relevance of Epstein-Barr Virus Infection in the Oral Squamous Cell Carcinoma: A Meta-Analysis J. Contemp. Dent. Med. Rev.20202020030720 Available online: http://www.ugr.es/~alberodr/curriculum/articulos/102.pdf(accessed on 20 May 2025)
- 8She Y. Nong X. Zhang M. Wang M. Epstein-Barr Virus Infection and Oral Squamous Cell Carcinoma Risk: A Meta-Analysis P Lo S ONE 201712 e 018686010.1371/journal.pone.018686029065191 PMC 5655447 · doi ↗ · pubmed ↗