Contributions of Pharmacovigilance to the Understanding of Risks Associated with Ibuprofen: Descriptive and Disproportionality Analysis Using FAERS Data
Cristina Anamaria Buciuman, Carmen Maximiliana Dobrea, Anca Butuca, Adina Frum, Felicia Gabriela Gligor, Mihai Octavian Botea, Mariana Eugenia Mureșan, Octavia Gligor, Florin Maghiar, Luciana Dobjanschi, Otilia Micle, Claudiu Morgovan, Laura Grațiela Vicaș

TL;DR
This study uses FAERS data to analyze real-world risks of ibuprofen, identifying patterns and severe adverse events.
Contribution
The study applies disproportionality analysis to FAERS data to highlight new safety signals for ibuprofen.
Findings
Most reports involved female patients and adults aged 18–65 years.
Oral administration was the most common route for ibuprofen-related adverse events.
4.3% of reports resulted in death, indicating significant safety concerns.
Abstract
Background/Objectives: The objective of this study was to evaluate real-world evidence (Food & Drug Administration database, FAERS) on ibuprofen adverse events (AE) through descriptive and disproportionality analyses. Methods: Signal assessment involved analyzing the top 30 entries with the most reports. The disproportionality analysis of signals based on Evans’ criteria (number of reports > 2, chi-square > 4, and PRR > 2) was performed. A total of 70,792 reports submitted to FAERS by the end of 2024 (collected from 97 countries worldwide) indicate ibuprofen as the main suspect. Results: Of these, the highest percentage was attributed to females (n = 33,262, 47.0%) and adult patients (18–65 years) (n = 22,005, 31.1%). In the elderly group (12.4%) and in children and adolescents (11.2%), similar frequencies were reported. Oral administration was the most frequently mentioned route (n =…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
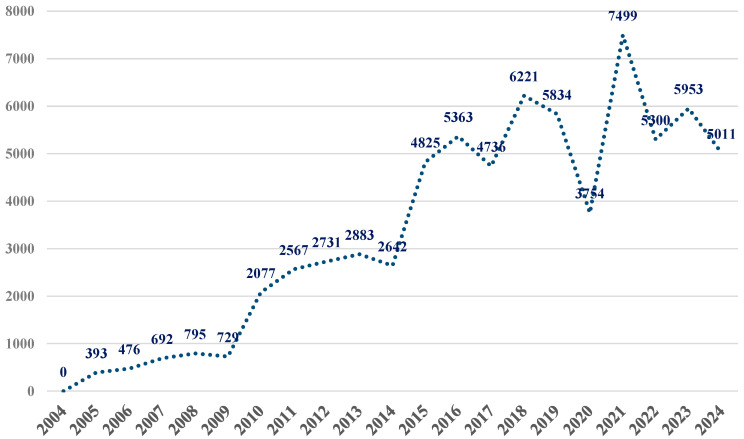 Figure 1
Figure 1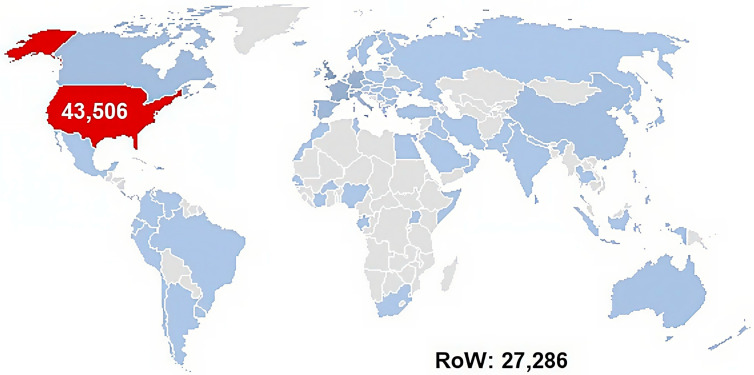 Figure 2
Figure 2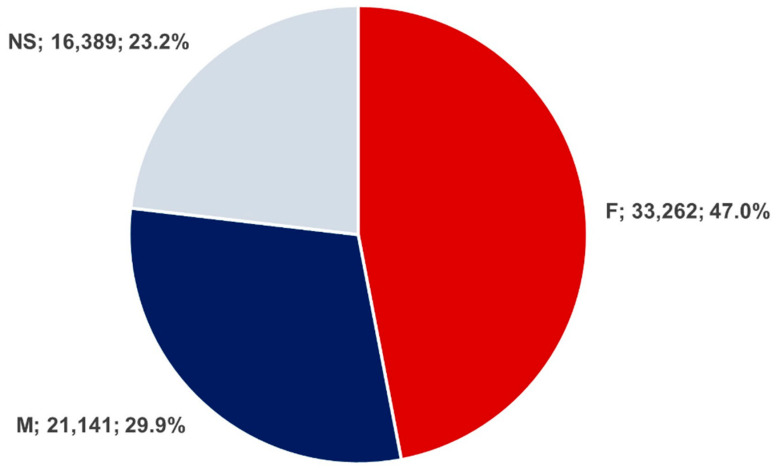 Figure 3
Figure 3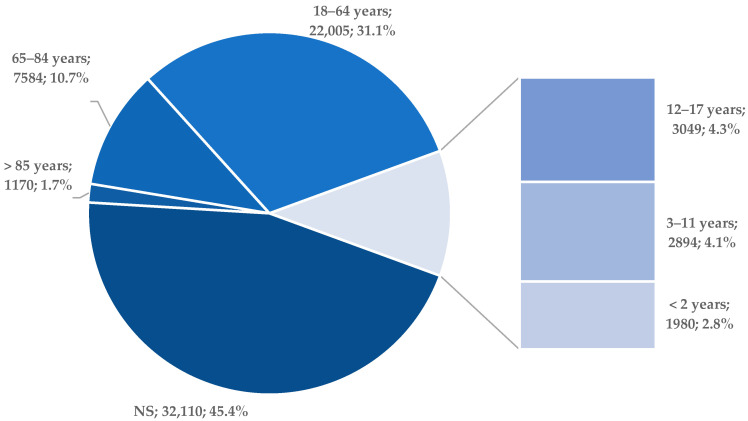 Figure 4
Figure 4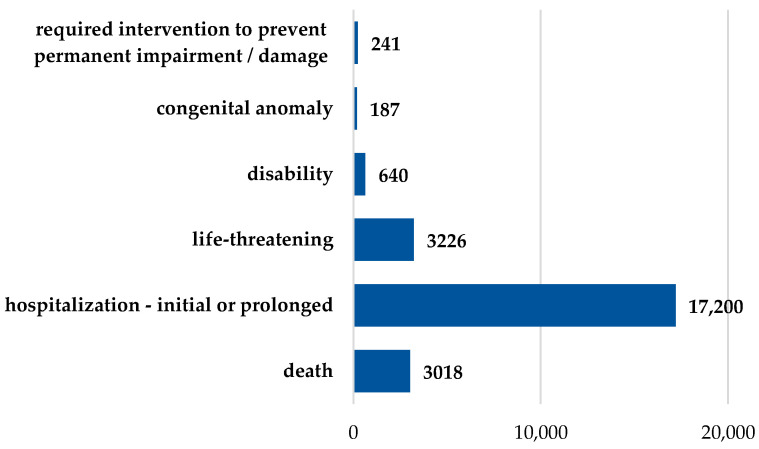 Figure 5
Figure 5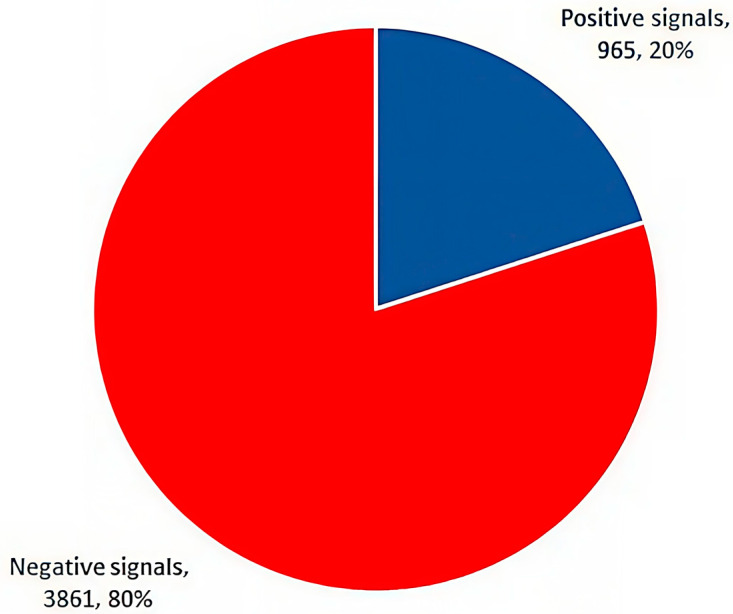 Figure 6
Figure 6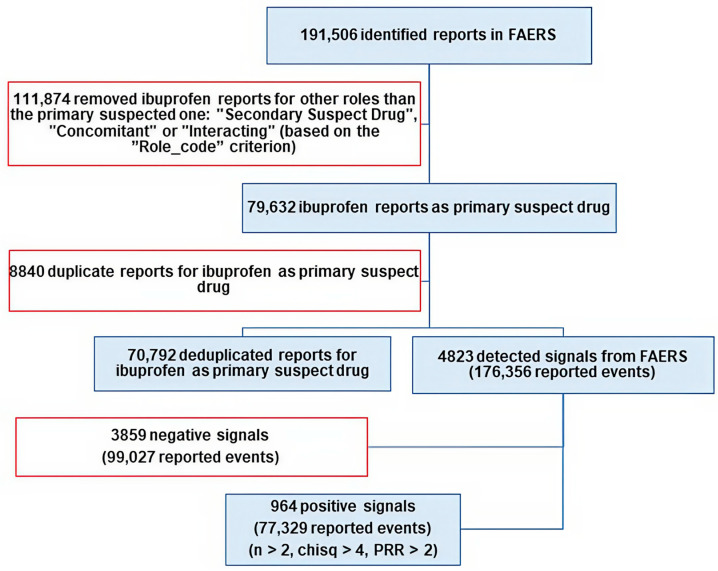 Figure 7
Figure 7- —University of Oradea
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPharmacovigilance and Adverse Drug Reactions · Inflammatory mediators and NSAID effects · Drug-Induced Adverse Reactions
1. Introduction
Ibuprofen belongs to the class of nonsteroidal anti-inflammatory drugs (NSAIDs), and it is an over-the-counter (OTC) medication or, in some cases, is dispensed based on a medical prescription. In the United States (US) of America, in 2022, ibuprofen was prescribed to more than 9 million patients, a 7% increase from 2021 [1]. The administration routes used are oral, cutaneous, rectal or intravenous [2,3,4]. Its formulation implies adapting to the specific pharmaceutical formulations via techniques that facilitate the effective delivery of the active substance [5]. In the US, over 40 products containing ibuprofen, under different pharmaceutical formulations, are included in the US Food & Drug Administration (FDA) Adverse Event Reporting System (FAERS) database [6].
Recent epidemiological data suggest that the escalating use of ibuprofen is not only driven by its analgesic efficacy but also by its expanding role in managing chronic inflammatory conditions in an aging population. This increased exposure needs a rigorous re-evaluation of its safety through large-scale real-world data, as clinical trials often lack the power to detect rare or long-term complications [7,8,9].
Ibuprofen’s main mechanism of action involves the nonselective inhibition of the group of cyclooxygenase enzymes (COX 1–3) [8]. Thus, the conversion of the arachidonic acid into prostaglandins—key mediators of pain and inflammation—is blocked [10]. Generally well tolerated, ibuprofen has been associated over the years with ADRs of gastro-intestinal [11], cardiovascular [12,13,14], cutaneous [12], renal [15], and neuropsychiatric [16,17] nature.
Furthermore, recent studies have highlighted the complexity of NSAID-induced adverse events, emphasizing that the risk profile is highly individualized. Emerging evidence points towards a significant interplay between genetic predispositions and the frequency of severe reactions, such as drug-induced liver injury or complex hypersensitivity syndromes, which remain under-reported in traditional clinical settings [18,19,20,21].
ADRs are collected and monitored by the authorities throughout databases. The monitoring system comprises reports from the pharmaceutical industry, generated by healthcare professionals, alongside patients. The terms utilized in reporting are part of the standardized Medical Dictionary for Regulatory Activities (MedDRA) [22]. Reporting is mandatory for drug manufacturers, voluntary for healthcare professionals (doctors, pharmacists, and nurses), and voluntary for patients who notice a possible ADR. This type of database can provide insight into a drug’s real-world safety profile. It can be used to continuously monitor and evaluate AEs and discover new ADRs, especially rare ones.
The FAERS database is a cornerstone of “real-world” drug safety, being frequently used in post-marketing studies. Disproportionality analysis is a validated statistical approach recommended in pharmacovigilance studies for identifying signals by comparing the observed frequency of a drug–event combination with a background frequency [23].
This methodology is particularly effective for widely used drugs like ibuprofen, where even low-frequency events can have a substantial public health impact due to the sheer volume of users [24,25].
The objective of the present study was to evaluate real-world evidence (the FAERS database) on ibuprofen safety, with the aim of examining the need for any updates to its safety profile, as known to date. By employing both descriptive and disproportionality analyses, this research seeks to bridge the gap between clinical trial data and everyday clinical practice, ensuring that the safety information remains current and evidence-based.
2. Results
2.1. Descriptive Analysis of Reported Events
In FAERS, a total of 70,792 reports were identified in association with ibuprofen as the primary suspect drug. Figure 1 shows that the number of reports increased steadily from 2004, reaching a peak in 2021 (n = 7499), followed by a slight decline in 2022–2024.
Figure 2 reveals these reports originated from 97 countries worldwide, and 1.14% of them did not have the country of provenance mentioned (n = 809). As expected, 61.5% were documented in the US, FAERS being managed by the FDA. Among the remaining reports, the largest contributions came from Western European countries: Great Britain (n = 6012, 8.5%), Germany (n = 3791, 5.4%), France (n = 3772, 5.3%), Italy (n = 2277, 3.2%), Spain (n = 2230, 3.2%), Portugal (n = 810, 1.1%), and the Netherlands (n = 500, 0.7%). Other notable contributions were from Canada (n = 1446, 2.0%), Australia (n = 563, 0.8%), and China (n = 1048, 1.5%). This geographic distribution highlights the predominance of reporting from North America and Western Europe, likely reflecting the national character of FAERS database as well as the reach of pharmacovigilance systems and reporting practices in these regions.
Among the deduplicated cases, 47.0% were female (n = 33,262) and 29.9% were male (n = 21,141), while in 23.1% of reports the patient’s sex was not specified or was reported as unknown (n = 16,389). As shown in Figure 3, this distribution reflects the known limitations of spontaneous reporting systems such as FAERS.
Figure 4 shows the age distribution of ibuprofen-associated adverse event reports in FAERS. Approximately 11.0% of cases involved children and adolescents, while 12.4% were reported for elderly individuals over 65 years old. As expected, the majority of reports were for adults aged 18–64 (n = 22,005, 31.1%). However, a large proportion of cases (45.4%) lacked information on patient age. Therefore, the age-stratified analysis reflects only a subset of the dataset and may not fully represent the true age distribution of ibuprofen-associated adverse events.
Table 1 displays the administration routes mentioned in the reports recorded in FAERS for ibuprofen. A large number of reports did not contain the administration route (n = 45,020, 63.6%). The oral route was the most frequently specified (n = 25,035, 35.4%). The transplacental (n = 367, 0.5%) and transmammary (n = 13, 0.02%) routes were notable, suggesting the occurrence of adverse events in newborns. Of the parenteral routes, the intravenous route (n = 153, 0.22%) was the most reported and, consequently, was the second most reported of these routes.
Adverse events of ibuprofen reported having an unfavorable outcome represented approximately 30%. Hence, at least one unfavorable outcome was reported for 21,077 cases. Death was reported for 3018 patients (4.3%). According to Figure 5, initial or prolonged hospitalization of the patient was required for 24.3% of the cases (n = 17,200). A life-threatening event was reported in 4.6% of the cases (n = 3226), and 640 cases (0.9%) led to a disability. Remarkably, a congenital anomaly was linked to ibuprofen in 187 cases (0.3%). Lastly, medical intervention in order to prevent permanent impairment or damage of the patient’s condition was necessary in 241 cases (0.3%).
2.2. FAERS Recorded Signal Assessment
A total of 176,356 adverse events were reported for the 4826 signals. Analyzing the top 30 signals with the most reports (representing a total of 56,546 events), most events were: product use in unapproved indication (n = 3569), drug hypersensitivity (n = 3407), drug effective for unapproved indication (n = 2459), and vomiting (n = 2447) (Table 2). A total of 8772 reports (5.00% of the dataset) indicated a lack of therapeutic effect (drug ineffective). These reports are presented here descriptively to provide context regarding ibuprofen use and patient-reported outcomes.
Based on the disproportionality analysis, only 17 of the first 30 signals, in terms of number of reported events, were possible ADRs for ibuprofen. These were categorized as:
- Gastrointestinal disorders: abdominal pain upper, abdominal discomfort, and gastrointestinal hemorrhage;
- Immune system disorders: drug hypersensitivity, urticaria, angioedema, and anaphylactic reaction;
- Renal disorders: acute kidney injury;
- Psychiatric disorders: somnolence and suicide attempt;
- Injuries, intoxications, and procedural complications: product use in unapproved indication, drug effective for unapproved indication, overdose and intentional overdose, and toxicity to various agents.
Among these 17, the 5 most frequent ADRs with clinical manifestations were: drug hypersensitivity (ROR: 4.85, 95% CI: 4.69–5.03; PRR: 4.67; Χ^2^: 9675.03), urticaria (ROR: 3.88, 95% CI: 3.70–4.06; PRR: 3.80; Χ^2^: 3722.68), acute kidney injury (ROR: 3.93, 95% CI: 3.75–4.12; PRR: 3.86; Χ^2^: 3713.88), abdominal pain upper (ROR: 2.82, 95% CI: 2.68–2.96; PRR: 2.78; Χ^2^: 1850.02), and angioedema (ROR: 11.54, 95% CI: 10.97–12.13; PRR: 11.29; Χ^2^: 14,491.17).
Nonetheless, for some reported events, the possibility of these being ADRs was unlikely (false signals), although they are mentioned in the Prescribing Information of ibuprofen-containing products: nausea, vomiting, dyspnea, rash, pruritus, dizziness, and headaches.
Of the total of 4826 signals recorded for ibuprofen in FAERS, 20.0% (n = 965, 77,329 reports) were positive signals, while the remaining 80.0% (n = 3861, 99,027 reports) were classified as false signals (Figure 6).
The strongest positive signals were defined as those with the highest chi-square values (Table 3). Considering this criterion, the top 30 strongest positive signals included adverse drug reactions (ADRs) from the following categories:
- Gastrointestinal: seven signals (gastric hemorrhage, oral discomfort, duodenal ulcer, upper gastrointestinal hemorrhage, melaena, hematemesis, and gastric ulcer);
- Allergic: six signals (toxic epidermal necrolysis, urticaria, anaphylactic reaction, lip oedema, drug hypersensitivity, and angioedema);
- Procedural complications: five signals (product administered to patient of inappropriate age, accidental exposure to the product by child, intentional overdose, product use in an unapproved indication, and drug effective for an unapproved indication);
- Renal: four signals (minimal change glomerulonephritis, acute kidney injury, tubulointerstitial nephritis, and renal tubular acidosis);
- Respiratory: three signals (bronchopulmonary dysplasia, aspirin-exacerbated respiratory disease, and NSAID-exacerbated respiratory disease);
- Product-related issue: two signals (failure of child-resistant product closure and poor-quality drug administered);
- Metabolic: one signal (metabolic acidosis);
- Neurological: one signal (aseptic meningitis);
- Psychiatric: one signal (suicide attempt).
3. Discussion
The present study showed that, in FAERS database, a total of 70,792 reports were identified in association with ibuprofen as the primary suspect drug. The evolution of reports up to the end of 2024 shows an upward trend, with a peak in 2021 (when more than 10% of total reports from the past 20 years were recorded). Similar patterns have been reported in other pharmacovigilance studies [23]. All these suggest that temporary drops in reporting may reflect changes in prescribing or in the drug’s use. Therefore, FAERS data must be interpreted as reflecting reporting trends rather than actual incidence rates.
Ibuprofen is among the most widely used NSAID drugs. The high number of adverse events reported in FAERS could be attributed to its over-the-counter availability. Also, the widespread access to ibuprofen in diverse settings, frequently without medical supervision, can elevate the risk and reporting of adverse events. These results align with previous FAERS-based studies. Moreover, other spontaneous reporting analyses have identified significant safety signals for ibuprofen, including renal injury and gastrointestinal bleeding [26,27]. These findings underscore the need for continued caution when recommending ibuprofen for non-prescription use, especially in populations at higher risk.
This descending trend noted at the beginning of the COVID-19 pandemic could be explained as an effect of studies that initially indicated ibuprofen and the other NSAIDs increased the expression of ACE2, facilitating COVID-19 infection and affecting disease outcomes, although further research proved ibuprofen was not associated with worse clinical outcomes in patients with COVID-19 [28,29,30,31,32]. During the COVID-19 pandemic, NSAIDs have been evaluated for potential therapeutic repositioning, highlighting the importance of continuous pharmacovigilance [32,33,34]; in this context, Xianfang et al. demonstrated that computational and pharmacovigilance-driven approaches can effectively identify potential drug-repurposing candidates, further emphasizing the need for ongoing safety monitoring of widely used drugs such as NSAIDs [34]. Regarding sex distribution, the highest percentage of spontaneous reports was observed in females (47.0%), and the reported adverse event rate in males was 29.9%. Apparently, the analgesic effect was predominant in men, although no pharmacokinetic discrepancies were observed [35]. The presumed sex-related difference in nociception could be attributed to the estrogenic effects on the nervous system, resulting in an increased pain impulse transmission [36]. A higher tendency of reporting adverse events in women than in men could also be arguable.
For the age category, the highest percentage of reports was recorded for the 18–64 years age group (31.1%). The lack of documented patient age was noticed in a relatively large number of cases (45%). In the over 65 years age group, 13% of the total reported cases were recorded. It is important to carefully monitor the risk-benefit ratio in older populations, given the risk of polypathologies and potential drug interactions [37]. Moreover, a study conducted using data from the French pharmacovigilance database highlighted the fact that, of the OTC medicines, ibuprofen was the most frequently linked to severe ADRs in the pediatric population, this aspect raising serious signs of concern [38].
The current study also highlighted the discrepancy between the number of reports and the administration route. As expected, the oral route accounted for the most reported cases (35.36%). Surprisingly, in numerous cases, the administration route was omitted (63.59%). Although transplacental and transmammary routes account for a low percentage (0.52% and 0.02%, respectively), ADRs have still been reported. Thus, ADRs may occur during fetal intrauterine development or in the infant after birth. Therefore, the current work calls attention to the development of ADRs via the transmammary route, although the excreted quantity of ibuprofen in breast milk is low (less than 1 mg/day), out of a 1600 mg/day dose [39,40]. The risk of ADR development as a result of ibuprofen administration over the duration of the pregnancy arises especially from self-medication in yet to be confirmed pregnancies or inadequate treatment. Due to their mechanism of action, NSAID administration is linked with a multitude of possible ADRs in the fetus (neurological, renal, pulmonary, gastrointestinal and cardiovascular damage, i.e., after 30 weeks, oligohydramnios and premature ductus arteriosus closure) [41,42].
According to the present findings, the adverse events of ibuprofen reporting an unfavorable outcome were 30%, and 4.3% of the reported cases were related to death. In a study of the FAERS database conducted by Eugene, analyzing reports from the 2014–2017 period in the adolescent age group (12–17 years), it was revealed that ibuprofen was correlated with the highest rate of unfavorable outcome—suicide [43]. In a retrospective analysis of the United States National Poison Data System, regarding the exposure to intentional overdose (suicide attempt) of acetaminophen and ibuprofen by adolescents in the US during the period 2017–2022, Weigel et al. stated that ibuprofen was connected to central nervous system depression and metabolic acidosis [44]. A congenital anomaly was encountered in 0.3% of cases; the rate was not significantly increased, though the severe implications and the availability of ibuprofen as an OTC should be taken into consideration.
Similar to other scientific evidence [45,46,47], the analyzed data from FAERS emphasized that initial or prolonged hospitalization of the patient was necessary in 24.3% of cases. This elevated percentage could impose another burden on the healthcare system.
In the present study, the top 30 signals with the most records in FAERS were product use in an unapproved indication, hypersensitivity, drug effectiveness for an unapproved indication, and vomiting. Applying the disproportionality analysis, the study pointed out that 17 of the top 30 signals were possible ADRs associated with the active substance ibuprofen. The most notable were gastrointestinal disorders (upper abdominal pain, abdominal discomfort, and gastrointestinal hemorrhage), immune system disorders (hypersensitivity, urticaria, angioedema, and anaphylactic reaction), renal disorders (acute kidney injury), and psychiatric disorders (suicide attempt and somnolence). Hypersensitivity reactions associated with NSAIDs may involve genetic predisposition and immune-mediated mechanisms [48,49]. Tang et al. provided evidence that genetic polymorphisms in immune-regulatory genes contribute to individual susceptibility to allergic and hypersensitivity reactions, supporting the immunologic mechanisms discussed for NSAID-associated adverse events [49]. Additionally, the current findings investigated the distribution of signals according to their likelihood of being connected to ADRs, noting that 20% of the total recorded signals for ibuprofen in FAERS were positive signals, while 80% were false signals.
The signals with the highest chi-square value were regarded as the strongest positive signals. Factoring this value, ADRs were identified for the top 30 strongest positive signals, belonging to the categories of gastrointestinal, allergic, renal, respiratory, metabolic (metabolic acidosis), neurological (aseptic meningitis), psychiatric (suicide attempt), as well as product-related issues (failure of child-resistant mechanism for pharmaceutical product and poor-quality drug administered) or procedural complications (product administered to patient of inappropriate age, accidental exposure to product by child, intentional overdose, product use in unapproved indication or drug effective for unapproved indication).
PGE2 increases the synthesis of mucus that protects the stomach wall against hydrochloric acid [50,51]. NSAIDs interact with phospholipids, thereby initiating biochemical changes that modify the gastrointestinal barrier. By inhibiting the PGE2 synthesis, NSAIDSs could induce mucosal damage, leading to erosions, ulcerations, hemorrhages, structural losses or even perforation [52].
In the sphere of hypersensitivity (allergic and cutaneous reactions), ibuprofen was linked to the most ADRs, including urticaria, angioedema, anaphylaxis, vasculitis, Stevens–Johnson syndrome, and photosensitivity. Reactions to a single NSAID are assumed to be mediated by specific IgE antibodies directed towards the antigenic determinants present within the medication. Patients with this type of immune response could also react to products with a similar chemical structure to that of the inducer drug. Thus, ibuprofen cross-reactions can be found for other compounds from chemically related groups such as naproxen, flurbiprofen, fenoprofen, ketoprofen, etc. Hypersensitivity reactions seem to have COX-1 inhibition as a mechanism, leading to arachidonic acid metabolism deviation towards the 5-lipooxygenase pathway and to the excessive production of cysteinyl leukotrienes, according to the theory proposed by Szczeklik [53]. Furthermore, single-dose ibuprofen-induced Stevens–Johnson syndrome has been scientifically reported, with symptoms manifesting after the administration of a higher dose—800 mg ibuprofen [54]. Moreover, ibuprofen-induced hypersensitivity syndrome could lead to an unpredictable, idiosyncratic type B reaction and could present a significant preoccupation in clinical practice, having been also mentioned in the scientific literature [55].
With regards to the neurological reactions, cases of aseptic meningitis are likewise present within the literature, for instance, Kalfoutzou et al. discussed a case of aseptic meningitis associated with ibuprofen in a 54-year old patient after the administration of a 400 mg ibuprofen dose [56]. Pereira et al. also noted a case report from the pediatric population group, a patient aged 15 [57]. Migraine was accompanied by excessive use of NSAIDs for several pain-related conditions, the prolonged administration causing a rebound effect, with the appearance of migraines [58,59]. On the other hand, regarding the suicidal behaviors correlated with ibuprofen, controversial data have been recorded throughout the scientific literature. Therefore, in some scientific cases, the potential reduction of inflammation at the central level (through the mechanism of action of NSAIDs) could lead to the conclusion that NSAIDs decrease suicidal ideation and depression [60]. Other scientific data also support this hypothesis [48], emphasizing the fact that the physio-pathological modifications (inflammation, oxidative and nitrosative stress, and mitochondrial dysfunctions) on account of major neuropsychiatric disorders (depression, schizophrenia, Alzheimer’s disease, etc.) could be countered by aid of an NSAID class representative, such as aspirin [61]. Nevertheless, an exploratory pharmacovigilance study of FAERS database entries, evaluating the 20 most common medications associated with suicidal ideation and self-harm, revealed that ibuprofen displayed a significant reporting frequency of neuropsychiatric adverse events [62].
The results of our study referring to the renal impairment produced by ibuprofen are in concordance with the literature that highlighted the role of PGs (e.g., PGE2 and PGI2) in maintaining renal blood flow. By inhibiting COX-1 and COX-2, PG biosynthesis is affected, leading to membrane damage, reduced pore size, and decreased podocyte density. As a consequence, renal impairment may occur [63].
Study strengths consisted in the large extension of the study, both in terms of time and geography, thus ensuring the diversity and large number of patients, clearly superior to those that could be achieved by means of controlled clinical trials and with a limited number of patients.
Study Limitations
The centralized post-authorization safety monitoring of medication is essential, although the current reporting systems exhibit several well-recognized limitations [64]. On one hand, there is the lack of denominator and, on the other hand, the number of submitted reports compared to the occurrence may be reduced by the underreporting phenomenon, especially for mild adverse reactions, or increased during certain time periods, as by the Weber effect and notoriety bias. The heterogeneous nature of the safety reports, in which some data fields are inconsistently completed or left missing, may distort signal detection and hinder the accurate estimation of adverse drug reaction incidence using the FAERS database. Furthermore, confounding by indication cannot be fully excluded and reported reactions may be related to the underlying disease rather than to the medication itself. A major impediment stems from the impossibility of establishing a cause–effect relationship between the exposure to a medication and the reported event [65,66]. Despite these limitations, to assess the robustness of our findings, sensitivity analyses were conducted using multiple complementary disproportionality measures, including the reporting odds ratio (ROR) and the proportional reporting ratio (PRR). The consistency of signals detected across these methods supports the robustness of the observed associations. As disproportionality analyses involve multiple testing across numerous drug–event pairs, results derived from the FAERS database should be interpreted with caution and considered targeted safety signals that merit subsequent clinical evaluation rather than confirmatory evidence of causality.
4. Materials and Methods
The Food and Drug Administration (FDA) of the United States of America (US) possesses a reporting system of potential ADRs, referred to as the FDA Adverse Events Reporting System (FAERS), that includes national and international reports for all drugs marketed in the US.
The OpenVigil 2.1 tool [67] was used to retrieve and analyze adverse event (AE) reports for ibuprofen as the active pharmaceutical ingredient from the FAERS database due to the availability of cleaned and validated data [6].
Ibuprofen was queried in OpenVigil 2.1 using the active substance name, with the drug role restricted to “primary suspect”. The analysis included all FAERS reports recorded between 2004 and 2024. Deduplication was performed by retaining only the most recent version of each case, based on both “case_ID” and “primary_id”, thereby avoiding duplicate counts of follow-up reports. Adverse events were coded according to the Medical Dictionary for Regulatory Activities (MedDRA), version 28.1, and analyses were conducted at the Preferred Term (PT) level.
Initially, a total of 79,632 reports listing ibuprofen as the primary suspect drug were identified. To address potential duplicate entries, reports were subsequently deduplicated based on the unique “case_ID” criterion, in accordance with established FAERS methodology [68]. Following the deduplication process, 70,792 unique cases remained and were included in the final analysis. All signal detection analyses, figures, and tables were generated using this final deduplicated dataset (Figure 7).
Initially, the descriptive analysis followed the chronological evolution of the submission of these individual case safety reports (ICSRs) to FAERS until 2024 and, eventually, their origin. Demographic characteristics of patients (sex and age) and ibuprofen administration route, as well as reports with unfavorable outcomes, were further analyzed. The category of reports with unfavorable outcomes included: death, initial or prolonged hospitalization of the patient, life-threatening events, disability, and congenital anomaly that required intervention to prevent permanent impairment/damage of the patient’s condition. Reports indicating “lack of efficacy” (PT: drug ineffective) were identified and analyzed separately from the other ADRs to avoid conflating safety with effectiveness. Only reports meeting the criteria for ADRs were included in the signal detection analysis.
Signal assessment focused on the top 30 entries with the highest number of reports. Disproportionality screening was performed using Evans’ criteria, including a minimum number of reports (n ≥ 2), a chi-square value greater than 4 (χ^2^ ≥ 4), and a proportional reporting ratio (PRR) greater than 2 (PRR > 2) [69]. The reporting odds ratio (ROR) was subsequently used to quantify signal strength and assess the magnitude of disproportionality. For all ROR estimates, 95% confidence intervals (95% CI) were calculated, and signal robustness was evaluated using the lower bound of the confidence interval.
The top 30 positive signals with the highest chi-square values were considered the strongest. Adverse events were classified as “Potential ADRs” if they met all Evans’ criteria and were consistent with the known pharmacology of ibuprofen and clinical guidelines. Events not meeting all criteria were categorized as “No” for potential ADR, even if some are recognized ibuprofen-associated ADRs, to ensure transparency and reproducibility of the classification. The disproportionality analysis approach is consistent with recent FAERS-based studies. Liu et al. (2025) demonstrated the applicability and robustness of disproportionality analysis for detecting safety signals from FAERS database associated with immunomodulatory therapies, supporting the methodological approach used in the present study [70].
Data uploaded until 31 December 2024 were extracted and processed using the Microsoft Excel for Microsoft 365 MSO (Version 2503). Ethical approval was not required for this study because all analyses were conducted using the publicly available FAERS database, which contains fully anonymized and de-identified adverse event reports. Similar other pharmacovigilance studies using FAERS or EudraVigilance data reports were performed [71,72].
5. Conclusions
Ibuprofen continues to be one of the popularly used NSAIDs, confirmed by the large number of reports recorded in FAERS, across all age groups. Reported adverse events fall into the characteristic classes for ibuprofen, positive signals having been highlighted for events pertaining to the gastrointestinal sphere, allergic reactions, procedural complications, and renal disorders. The disproportionality analysis led to the identification of possible ADRs, such as drug hypersensitivity, acute kidney injury, urticaria, upper abdominal pain, and angioedema. The results of the study should be interpreted while accommodating the inherent limitations of the collected data as a consequence of spontaneous reporting. The results of the present study underline the possible risks related to ibuprofen use and underscore the importance of a responsible and clinically well-founded administration.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The Top 300 of 2022 Available online: https://clincalc.com/Drug Stats/Top 300Drugs.aspx(accessed on 6 February 2026)
- 2Bookstaver B. Miller A.D. Norris L.B. Rudisill C.N. Intravenous Ibuprofen: The First Injectable Product for the Treatment of Pain and Fever J. Pain Res.201036710.2147/JPR.S 699321197311 PMC 3004645 · doi ↗ · pubmed ↗
- 3Prasaja B. Harahap Y. Sandra M. Iskandar I. Lusthom W. Cahyaningsih P. Rectal Administration of Ibuprofen: Comparison of Enema and Suppository Form Drug Res.202272182210.1055/a-1577-295534416778 · doi ↗ · pubmed ↗
- 4Moore N. Ibuprofen: A Journey from Prescription to over-the-Counter Use J. R. Soc. Med.20071002610.1177/014107680710004801 s 0118335846 · doi ↗ · pubmed ↗
- 5Irvine J. Afrose A. Islam N. Formulation and Delivery Strategies of Ibuprofen: Challenges and Opportunities Drug Dev. Ind. Pharm.20184417318310.1080/03639045.2017.139183829022772 · doi ↗ · pubmed ↗
- 6FDA Adverse Event Reporting System (FAERS) Public Dashboard for Drugs and Biologics—FDA Adverse Event Reporting System (FAERS) Public Dashboard for Drugs and Biologics | Sheet—Qlik Sense Available online: https://fis.fda.gov/sense/app/95239 e 26-e 0be-42d 9-a 960-9a 5f 7f 1c 25ee/sheet/33a 0f 68e-845c-48e 2-bc 81-8141 c 6aaf 772/state/analysis(accessed on 6 February 2026)
- 7Gómez-Acebo I. Dierssen-Sotos T. De Pedro M. Pérez-Gómez B. Castaño-Vinyals G. Fernández-Villa T. Palazuelos-Calderón C. Amiano P. Etxeberria J. Benavente Y. Epidemiology of Non-Steroidal Anti-Inflammatory Drugs Consumption in Spain. The MCC-Spain Study BMC Public Heal.2018181113410.1186/s 12889-018-6019-z PMC 615096730241493 · doi ↗ · pubmed ↗
- 8Young C. Eggleston W. Ibuprofen Encycl. Toxicol. Fourth Ed.2024544344710.1016/B 978-0-12-824315-2.00727-2 · doi ↗