Rotator Cuff Disorders: Practical Recommendations for Conservative Management Based on the Literature
Adrien J.-P. Schwitzguébel

TL;DR
This paper provides a comprehensive, evidence-based protocol for non-surgical management of rotator cuff disorders, integrating diagnosis, prognosis, and rehabilitation.
Contribution
A new global protocol for conservative management of rotator cuff disorders, stratifying patients into prognostic categories with tailored treatment strategies.
Findings
A stepwise diagnostic process combining history, examination, and imaging is recommended.
Three prognostic categories (good, borderline, poor) guide treatment adaptation and monitoring.
Rehabilitation is structured around four domains, including pain control, mobility, strengthening, and anatomy preservation.
Abstract
Conservative management of rotator cuff disorders remains challenging, with no comprehensive, evidence-based framework integrating diagnosis, prognosis, rehabilitation, and biological therapies. Existing recommendations usually address isolated components of care, leading to inconsistent treatment strategies. This article proposes a global, pragmatic protocol for the non-surgical management of rotator cuff lesions, from initial assessment to long-term follow-up. Drawing on clinical expertise supported by recent literature, we outline a stepwise approach that begins with a comprehensive diagnostic process that combines history, clinical examination, and targeted imaging. Based on lesion type, associated shoulder or neurogenic conditions, and patient profile, rotator cuff disorders are stratified into three prognostic categories under conservative care: good, borderline, and poor…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
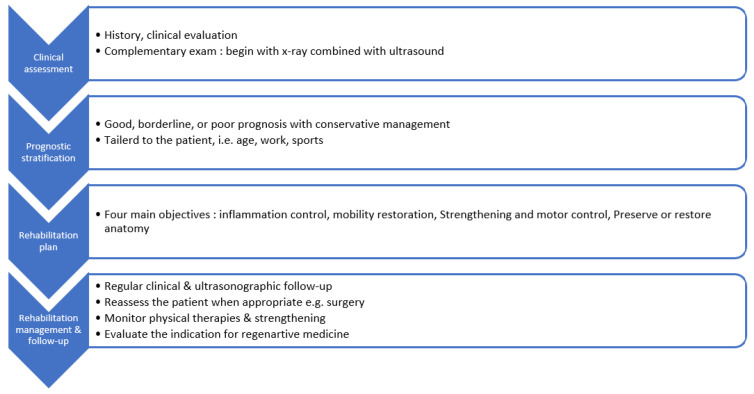 Figure 1
Figure 1| Objective | Primary Goal | Key Interventions or Strategies |
|---|---|---|
| #1—Inflammation control | To reduce pain and local inflammation in order to enable early rehabilitation |
Short course of anti-inflammatory drugs Neuromodulation or dry needling when appropriate |
| #2—Mobility restoration | To recover full, pain-free range of motion and prevent joint stiffness |
Early self-mobilization and stretching Adhesive capsulitis management if applicable Postural and scapular-control reeducation |
| #3—Strengthening and motor control | To rebuild tendon and muscle function while optimizing dynamic stability |
Progressive and tendon-sparing strengthening Scapular and kinetic-chain integration Functional or sport-specific retraining |
| #4—Preserve or restore anatomy | To support tendon healing and tissue homeostasis |
Nutritional optimization Management of calcific tendinopathy Regenerative interventions considered once impingement has been corrected |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsShoulder Injury and Treatment · Shoulder and Clavicle Injuries · Nerve Injury and Rehabilitation
1. Introduction
Rotator cuff tears represent a common cause of shoulder pain and disability in adults [1]. Despite the growing body of literature on rotator cuff related disorders, there remains substantial heterogeneity across nonoperative rehabilitation programs and clinical follow-up strategies, which may contribute to variability in day-to-day clinical decision-making [2,3,4]. Nowadays, there is a need to help harmonize and standardize non-surgical management practices in outpatient settings and training environments specializing in Sports Medicine and Physical and Rehabilitation Medicine. In particular, existing guidelines rarely provide practical recommendations on longitudinal follow-up, imaging indications, or treatment adaptation, which can lead to variability in clinical decision-making. This narrative review is based on targeted literature searches and an experience-informed synthesis of the evidence, aiming to translate current concepts into a step-by-step clinician-oriented protocol.
Although it is widely accepted that exercise-based rehabilitation improves outcomes in rotator cuff disorders, the optimal characteristics of available rehabilitation programs remain insufficiently defined and largely clinician-dependent. While general rehabilitation principles are well described, a practical step-by-step recommendation is still lacking, supporting the need for clinician-oriented protocols. In this context, recent consensus statements, such as the Bern Consensus, which primarily targets athletes involved in shoulder demanding sports, provide useful overarching principles for rehabilitation and return to sport decision making, yet they remain relatively broad and do not translate into a rotator cuff specific, clinician oriented protocol for day-to-day management [5]. Concerning surgical decision, even if the decision-making is nowadays better documented, the decision between surgical and nonoperative management of rotator cuff tears remains complex and clinician-dependent [6], and must be balanced against the potential for tear progression over time [7], within an individualized, evidence-informed framework as outlined in current clinical practice guidelines [8].
More broadly, medical training and published recommendations often provide limited guidance on how to structure and individualize clinical follow-up over time, a competency that is frequently acquired through clinical experience rather than formal instruction. To date, step-by-step practical guidance remains scarce in the literature and is often replaced by broad conceptual principles and general decision-making recommendations.
The aim of this narrative review is to provide a clinically meaningful protocol to support clinicians in evidence-informed decision-making and up-to-date rehabilitation strategies in 2026.
2. Methods
This protocol is based on a narrative, experience-informed synthesis of the literature. The recommendations combine commonly accepted clinical practice with evidence-informed therapeutic principles. References were identified through targeted searches in PubMed using predefined keywords for each clinical situation, related to rotator cuff tears, tendinopathy, conservative treatment, rehabilitation, prognostic factors, and return-to-play. Google Scholar was used as a complementary search engine to identify additional relevant guidelines, consensus statements, and highly cited articles not retrieved through PubMed searches. Priority was given to systematic reviews, randomized controlled trials, and international recommendations, with preference for publications from the last 10 years unless older studies were considered landmark or essential for clinical context. The selection process was complemented by the author’s clinical expertise to ensure clinical applicability. This article does not follow a systematic review methodology and does not aim to provide an exhaustive analysis of all available studies.
3. Results
The stepwise clinical approach proposed in this protocol is summarized in Figure 1. The proposed approach integrates diagnostic clarification, prognostic stratification, structured rehabilitation objectives, and explicit follow-up pathways. It also describes the rational use of therapeutic options such as passive modalities, injectables, and regenerative procedures, all positioned as complementary tools that support structured active rehabilitation.
4. Discussion
Current guidelines on rotator cuff disorders primarily focus on diagnostic criteria, surgical indications, or general rehabilitation principles, but do not always provide detailed guidance on longitudinal clinical follow-up and treatment adaptation within conservative care. In contrast, the present protocol emphasizes a structured, stepwise approach integrating diagnostic clarification, prognostic stratification, rehabilitation objectives, and predefined reassessment points, allowing management to be adapted over time rather than applied as a static recommendation.
The literature on conservative management of rotator cuff disorders is abundant but remains heterogeneous. Available evidence primarily describes key rehabilitation concepts and consistently supports the effectiveness of active strengthening-based programs [2,3,4]. However, combined treatment strategies are less well described, and limited guidance exists regarding the optimal timing and integration of different interventions within a structured, longitudinal rehabilitation plan. While this flexibility allows individualization according to patient characteristics (e.g., sports participation and return-to-play demands), the step-by-step framework proposed in the present protocol may provide a clearer clinical roadmap for junior clinicians with limited experience, and may also encourage more experienced clinicians to critically integrate emerging rehabilitation techniques into their treatment planning.
Surgical decision-making in rotator cuff disorders remains complex and controversial, and cannot be reduced to tear size or imaging findings alone [6]. In particular, the classification of partial-thickness tears exceeding 50% as a borderline category is debated, as many surgeons consider this threshold a surgical indication. However, several studies have demonstrated that conservative management can still lead to favorable clinical outcomes in selected patients, including those with larger partial tears [8,9]. Accordingly, this protocol deliberately classifies such lesions as borderline to promote individualized decision-making and to encourage reassessment based on symptom evolution and functional recovery rather than reliance on a strict morphological threshold. Tear progression is also frequently cited as a key argument to support early surgical referral [8], yet the available evidence remains difficult to interpret in routine practice due to marked heterogeneity in the definitions of progression and in reported progression rates. A recent systematic review highlighted substantial disparities across studies in how progression is defined, measured, and reported, resulting in wide variations in estimated progression rates [7]. In this context, structured conservative pathways with predefined reassessment points may facilitate timely treatment adaptation and escalation, allowing referral decisions to be guided by symptom evolution, function, and objective clinical changes rather than by imaging-based assumptions alone [8].
The proposed follow-up strategy is designed to support early active rehabilitation and, when appropriate, an early return to sport, which is often requested by athletes, while maintaining clinical safety through predefined reassessment points [10]. In selected cases, imaging can be integrated as an adjunct to clinical monitoring to document tendon status when symptoms or function evolve, or when an objective reassessment is required before progressing rehabilitation intensity [11]. Moreover, delayed follow-up imaging may help detect early worsening or progression, potentially preventing complications, and may also help to document a reduction in direct signs of tendon pathology, such as tendinosis features or Doppler hypervascularity, as well as indirect signs, such as subacromial bursitis, which may support treatment response and reinforce the decision to advance to the next rehabilitation phase. Importantly, imaging findings should not be interpreted in isolation, but rather integrated with symptom evolution, functional recovery, and load tolerance.
Another distinctive feature of this protocol is the explicit positioning of active rehabilitation as the cornerstone of conservative management, while passive modalities, injectable treatments, and regenerative approaches are framed as adjunctive options. This integration aims to promote a rational and proportionate use of available therapeutic tools while maintaining clinical coherence. Rehabilitation progression is deliberately criteria-based rather than time-based, with advancement guided by clinical and functional recovery, symptom evolution, and tolerance to load, in order to preserve clinical judgment and reflect real-world conservative practice.
A key strength of the present protocol is its longitudinal and structured follow-up strategy, which translates broad rehabilitation concepts into a practical clinical pathway. The protocol includes predefined decision nodes and reassessment points to guide treatment adaptation over time, rather than applying conservative management as a static recommendation. Rehabilitation progression is deliberately criteria-based rather than strictly time-based, allowing advancement to be driven by symptom evolution, functional recovery, and load tolerance. Finally, the protocol integrates adjunctive therapies within a rational hierarchy, emphasizing active rehabilitation as the cornerstone of care while framing passive modalities and injectable or regenerative options as supportive interventions when clinically indicated.
5. Limitations
This work has several limitations. First, it is a narrative review and does not follow a systematic review methodology, therefore reference selection may be subject to selection bias and does not aim to provide an exhaustive analysis of all available evidence. Second, the protocol was not developed through a formal Delphi process or multidisciplinary consensus panel, and it reflects a clinician-oriented synthesis rather than a consensus-based guideline. Third, the proposed pathway has not been prospectively validated, and its impact on clinical outcomes, return-to-sport trajectories, and healthcare utilization remains to be established. Future research should include implementation studies and prospective validation in other outpatient settings, ideally with multicenter designs, assessment of inter-clinician reproducibility, and cost-effectiveness analyses. Finally, the protocol may require adaptation depending on local resources and healthcare systems, including imaging availability, access to specialized rehabilitation, and the specific demands of different sports and patient populations.
6. Conclusions
This narrative review proposes a pragmatic and structured approach to conservative management of rotator cuff disorders, emphasizing individualized care, active rehabilitation, and rational use of adjunct therapies. By translating available evidence and clinical experience into a coherent and usable protocol, it aims to support consistent clinical decision-making, longitudinal follow-up, and structured progression of rehabilitation in everyday practice.
EVALUATION
1. Patient history and clinical examination
- a.History: onset and mechanism of injury (traumatic versus degenerative), and evolution or fluctuation of symptoms over time.
- b.Differential diagnosis: Consider neurogenic, articular, and referred pain sources in the differential diagnosis.
- c.Clinical examination: Clinical examination includes assessment of range of motion, strength testing, and specific maneuvers for impingement and rotator cuff integrity.
2. Initial imaging assessment
a. Standard radiography:
- i.Should be systematically proposed, particularly to assist in differential diagnosis. To include true anteroposterior views in three rotations and a Neer view.
- ii.To add an axial view if glenohumeral osteoarthritis is suspected.
- iii.To add axial and Bernageau views if glenohumeral instability is suspected.
- iv.To add a scapular Y-view if acromioclavicular joint involvement is suspected.
b. Ultrasound:
- i.To perform systematically as a first-line imaging modality, ensuring complete and comprehensive assessment [12,13].
- ii.To include dynamic evaluation for impingement mechanisms, biceps tendon instability, and friction phenomena [14,15].
- iii.To use contralateral comparison and color or power Doppler (with the patient supine to enhance sensitivity) to assess vascularization and inflammatory activity [14].
c. MRI
- i.Indicated when surgical management is being considered; MR arthrography may be considered in selected cases.
- ii.Also indicated when diagnosis remains uncertain after radiography and ultrasound.
d. CT or MR arthrogram
- i.To determine whether a cuff lesion is full-thickness [16].
- ii.To evaluate associated intra-articular pathology, such as labral lesions, instability, or osteoarthritis.
e. CT scan or SPECT-CT
- i.To be reserved for exceptional cases (bone pathology or complex/unclear diagnosis).
- ii.To help differentiate mechanical from metabolic pain sources, particularly in cases of therapeutic failure [17].
DIAGNOSIS
1. Rotator cuff lesion (Table 1 )
a. Good prognosis with conservative management
- i.Tendinopathies without tear or with interstitial tear [18].
- ii.Small acute traumatic tears involving less than 50% of tendon thickness in any plane [19,20,21].
- iii.Calcific tendinopathies [22].
- iv.Acute isolated rupture of the long head of the biceps tendon [23].
b. Borderline prognosis with conservative management
- i.Tendon tears (bursal-, articular-, or full-thickness) occurring without tendon retraction or muscle atrophy [9].
- ii.Acute traumatic partial tears affecting ≥ 50% of tendon thickness in any plane, excluding the long head of the biceps [9].
- iii.Tendon tears showing retraction or muscle atrophy in elderly or low-demand patients [24].
- iv.Suspected instability of the long head of the biceps with pulley lesion [25].
- v.Post-fracture status of the proximal humerus with residual displacement, increasing the risk of secondary impingement.
c. Poor prognosis with conservative management
- i.Complete or high-grade partial tears associated with retraction or muscle atrophy, particularly in younger and active patients.
- ii.Instability of the long head of the biceps combined with a contiguous tear of the supraspinatus or superior subscapularis tendon [25].
- iii.Complete acute ruptures other than those involving the long head of the biceps [26].
Associated factors
a. Impingement syndromes
- i.Subacromial impingement
- ii.Posterosuperior impingement
- iii.Anterior impingement
b. Glenohumeral disorders
- i.Adhesive capsulitis
- ii.Labral lesion (SLAP)
- iii.Glenohumeral osteoarthritis
- iv.Glenohumeral instability
c. Acromioclavicular joint
- i.Arthropathy
- ii.Dislocation
d. Neurogenic conditions
- i.Cervicogenic brachialgia
- ii.Thoracic outlet syndrome
- iii.Focal neuropathies (e.g., suprascapular)
- iv.Parsonage-Turner syndrome
- v.Axillary nerve entrapment
REHABILITATION OBJECTIVES (Table 2)
1. Inflammation
a.To manage inflammatory processes, bursitis, and joint effusion effectively.b.To ensure adequate pain control and patient comfort.c.To monitor for potential nerve irritation or early signs of complex regional pain syndrome (CRPS).
2. Mobility
a.To maintain or restore full joint range of motion.b.To optimize scapular kinematics and address impingement mechanisms when present.c.To enhance proprioceptive function and promote coordinated scapulothoracic and glenohumeral motion control.
3. Strengthening
a.To improve muscular strength and global functional performance.b.To implement tendon-sparing strengthening protocols, particularly for the supraspinatus.c.To control laxity and dynamic instability while minimizing the risk of recurrent microtrauma.
4. Preserve or restore anatomy
a.To promote tissue healing and biological stimulation within the repair process.b.To support neural recovery and neuromuscular reintegration when applicable.
REHABILITATION MANAGEMENT
1. Surgical decision making
a. Indications for early surgery
- i.Acute traumatic partial tears involving more than 50% of tendon thickness, or complete ruptures, particularly in young and active patients.
- ii.Any lesion classified as poor prognosis with conservative management. Notably retracted tears, early fatty atrophy, or complex biceps pulley lesions in young and active individuals [27].
b. Indications for delayed or secondary surgery
- i.Lesions with borderline prognosis under conservative management that remain symptomatic after an adequate rehabilitation program (minimum 12 weeks including progressive active strengthening) [28].
- ii.Degenerative tendon lesions in young and active patients: conservative management remains the first-line option, with surgery considered only in case of treatment failure [27,29].
- iii.Acute small (<50%) tendon ruptures: conservative and surgical approaches generally provide comparable outcomes; surgery may remain optional [30].
- iv.Full-thickness tears in middle-aged or elderly patients: favorable outcomes are often achievable through non-operative management [24].
c. Contraindications or deferral of surgery
- i.Adhesive capsulitis: prioritize restoration of range of motion before considering surgical intervention; surgery should be reconsidered only once stiffness has resolved [31,32].
- ii.Neurogenic etiologies (e.g., cervical radiculopathy, suprascapular neuropathy, Parsonage–Turner syndrome): manage the neurological condition first, then reassess the indication for surgery.
2. Conservative management: physician-guided monitoring plan (Table 3)
a. Clinical follow-up
- i.Schedule clinical reassessments every 6–12 weeks, depending on the patient’s progression and activity level.
- ii.Consider earlier follow-up (2–4 weeks) in acute cases or in high-demand athletes to optimize load management and pain control.
- iii.At each visit, monitor pain (VAS), function (SANE or Constant score), and activity tolerance [31].
b. Ultrasound monitoring
- i.Perform ultrasonographic follow-up as part of the routine clinical evaluation to monitor tendon integrity, bursal inflammation, and impingement dynamics [11,21].
- ii.Stability or gradual improvement in echotexture and vascularization, even without complete anatomic healing, generally reflects a favorable response to conservative treatment.
- iii.Progressive tear enlargement or persistent bursal hyperemia may justify reconsidering either conservative or surgical management.
c. Multidisciplinary reassessment
- i.Reassess the indication for surgery when pain, weakness, or loss of function persist despite at least 12 weeks of appropriate, structured rehabilitation (see above).
- ii.Surgical reconsideration should also be discussed if imaging reveals progressive tendon retraction, atrophy, or loss of function despite good compliance [9,24].
- iii.Consider rheumatologic evaluation when inflammatory or systemic factors are suspected, such as atypical pain distribution, morning stiffness, or persistent synovial hypervascularization on ultrasound.
d. Return-to-play decision
- i.Return to play should be gradual and supervised by a sports physician or physiotherapist experienced in shoulder rehabilitation, with progressive workload monitoring.
- ii.Presence of mild to moderate pain showing progressive improvement over time is acceptable for return-to-play progression [10,33].
- iii.Ensure absence of dynamic impingement or tear progression on follow-up ultrasound [34,35].
- iv.Confirm sufficient strength and functional performance to execute sport-specific tasks without compensatory mechanisms, for example using a limb symmetry index ≥ 90% compared with the contralateral side [10,33].
3. Objective #1: Inflammation control
a. Analgesics and NSAIDs
- i.Use analgesics and short courses of nonsteroidal anti-inflammatory drugs (NSAIDs) to manage acute pain and reduce inflammatory response.
- ii.Prolonged or repeated use should be avoided, as it provides no proven benefit for tendon healing and may exert detrimental effects on tendon biology [36,37].
b. Corticosteroid injections (with or without hyaluronic acid)
- i.Corticosteroid injections may be considered for short-term pain control when pain significantly limits rehabilitation.
- ii.Subacromial injections are indicated for bursitis, superficial or transfixing tendinosis, or subacromial impingement.
- iii.Glenohumeral injections are indicated for articular-sided tendinosis, labral pathology, or glenohumeral osteoarthritis.
- iv.Acromioclavicular injections are indicated for acromioclavicular joint involvement.
- v.Combination with hyaluronic acid may enhance short-term pain relief and joint mobility, and may contribute to tendon preservation [38].
- vi.Injections should be limited to single administrations or short series to minimize potential catabolic effects on tendon tissue and reduce the long-term risk of surgical conversion [39,40,41].
c. Neurogenic pain management
- i.Consider targeted management of neurogenic pain when clinical features suggest a neuropathic component, either as a primary or associated condition.
- ii.Assessment may include diagnostic nerve blocks and/or electromyographic studies when appropriate and available.
d. Physical therapies in the early subacute phase
- i.Manual therapy, gentle joint mobilizations, soft-tissue techniques, and dry needling can be initiated early in the subacute phase to reduce residual muscle tension, promote pain modulation, and facilitate recovery of shoulder mobility [42].
4. Objective #2: mobility
a. General mobility principles
- i.Maintain periscapular balance and glenohumeral articular amplitudes, especially to prevent secondary impingement [43].
- ii.Minimize shear forces on the tendon whenever possible [44].
- iii.Consider supportive taping or bracing for short-term proprioceptive feedback or pain relief [45,46].
b. Limitation of range of motion and adhesive capsulitis
- i.Focus early, controlled, and progressive rehabilitation on self-mobilization exercises [47].
- ii.Consider capsular distension [48], suprascapular nerve block [49], with or without manipulation under appropriate anesthesia [50].
c. Impingements
- i.Emphasize scapular opening, postural correction, and pectoralis minor stretching [43].
- ii.Use sleeper stretch in cases of posterosuperior impingement [51].
5. Objective #3: strengthening (Table 4)
a. Early phase
- i.Initiate a self-directed exercise program aiming to maintain neuromuscular activation and preserve muscle capacity [43,52].
- ii.Implement hypertrophic strengthening protocols [53] with minimal inflammatory impact, such as blood flow restriction training [54,55] or isokinetic strengthening [56].
- iii.Reinforce periscapular and rotator cuff muscles through progressive loading, including high-load eccentric exercises [57], to enhance dynamic stability and promote tendon remodeling.
- iv.In cases of supraspinatus tear, apply relative supraspinatus-sparing strategies, focusing on external rotators, adductors, and deltoid strengthening to support shoulder abduction and humeral head centering [58].
b. Late phase
- i.Perform objective strength testing to guide load progression and confirm readiness for higher functional demands [59].
- ii.Integrate kinetic-chain coordination once local control and strength are adequately restored, ensuring efficient transfer to complex and multiplanar movements [60].
- iii.Progress toward sport-specific and functional exercises emphasizing movement efficiency, endurance, and controlled power generation [61,62].
6. Objective #4: preserve or restore anatomy
a. Trophism & nutrition
- i.Beyond mechanical stimulation, nutritional and biological strategies can further support tendon healing and tissue homeostasis.
- ii.Ensure adequate daily protein intake (1.2–1.6 g/kg body weight) to support overall tissue recovery, including muscle maintenance and connective tissue remodeling. Carbohydrate intake should also be sufficient to maintain energy availability and prevent catabolic states during rehabilitation. [63,64].
- iii.Consider nutritional supplements that may support tendon and muscle healing, particularly collagen peptides [65], vitamins C and D [66], and omega-3 fatty acids (EPA/DHA) [66,67].
- iv.Address modifiable risk factors for tendinopathies, including exposure to quinolones or corticosteroids [68], underlying rheumatologic or autoimmune diseases, and possibly menopause (considering hormone replacement therapy) [69]. Potential dental issues may also be relevant, although current evidence remains very limited [70].
b. Calcic tendinopathy
- i.Calcifications should be removed or reduced when feasible.
- ii.Consider ultrasound-guided needle aspiration when a single, swollen calcification is present [22].
- iii.Focused shockwave therapy is indicated when calcifications are small, multiple, or not amenable to needle aspiration [71,72].
c. Regenerative medicine (Table 5)
- i.Regenerative medicine should be considered with caution and only after effective management of pre-existing impingements and optimization of mechanical load and rehabilitation.
- ii.Realistic clinical indications include chronic tendinopathy or small to moderate, non-retracted partial tears.
- iii.Platelet-rich plasma (PRP) ± tendon needling, despite conflicting evidence, may promote tendon healing in selected cases [73,74,75].
- iv.Focused shockwave therapy can provide additional biological stimulation, although clinical responses are generally moderate [71,76,77].
- v.Emerging adjuncts, sometimes combined with PRP, include matrix components such as injectable collagen or viscosupplementation [38,78].
- vi.Potentially more potent but technically demanding approaches involve stromal vascular fraction or nanofat injections; these remain strictly experimental [79].
- vii.A variety of other passive or device-based regenerative modalities, including hyperbaric oxygen, electrolysis, low-level laser therapy, and TECAR, have also been proposed. Their clinical relevance remains uncertain, and structured active rehabilitation should remain the foundation of treatment before considering such complementary options [80].
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hinsley H. Ganderton C. Arden N.K. Carr A.J. Prevalence of rotator cuff tendon tears and symptoms in a Chingford general population cohort, and the resultant impact on UK health services: A cross-sectional observational study BMJ Open 202212 e 05917510.1136/bmjopen-2021-059175 PMC 947211236100305 · doi ↗ · pubmed ↗
- 2Steuri R. Sattelmayer M. Elsig S. Kolly C. Tal A. Taeymans J. Hilfiker R. Effectiveness of conservative interventions including exercise, manual therapy and medical management in adults with shoulder impingement: A systematic review and meta-analysis of RC Ts Br. J. Sports Med.2017511340134710.1136/bjsports-2016-09651528630217 PMC 5574390 · doi ↗ · pubmed ↗
- 3Lowry V. Lavigne P. Zidarov D. Matifat E. Cormier A.A. Desmeules F. A Systematic Review of Clinical Practice Guidelines on the Diagnosis and Management of Various Shoulder Disorders Arch. Phys. Med. Rehabil.202410541142610.1016/j.apmr.2023.09.02237832814 · doi ↗ · pubmed ↗
- 4Boland K. Smith C. Bond H. Briggs S. Walton J. Current concepts in the rehabilitation of rotator cuff related disorders J. Clin. Orthop. Trauma.202118131910.1016/j.jcot.2021.04.00733987078 PMC 8082254 · doi ↗ · pubmed ↗
- 5Schwank A. Blazey P. Asker M. Moller M. Hagglund M. Gard S. Skazalski C. Haugsbo Andersson S. Horsley I. Whiteley R. 2022 Bern Consensus Statement on Shoulder Injury Prevention, Rehabilitation, and Return to Sport for Athletes at All Participation Levels J. Orthop. Sports Phys. Ther.202252112810.2519/jospt.2022.1095234972489 · doi ↗ · pubmed ↗
- 6Pitt L. Mazuquin B. Littlewood C. What influences the decision to undergo rotator cuff repair surgery: A survey of clinician's perspectives Shoulder Elb.20251734134710.1177/1758573224128174339545003 PMC 11559883 · doi ↗ · pubmed ↗
- 7Garcia M.J. Caro D. Hammerle M.V. Villarreal J.B. De Angelis J.P. Ramappa A.J. Nazarian A. Disparities in Rotator Cuff Tear Progression Definitions and Rates: A Systematic Review JB JS Open Access 20249 e 24.0009710.2106/JBJS.OA.24.0009739440278 PMC 11495754 · doi ↗ · pubmed ↗
- 8American Academy of Orthopaedic Surgeons Management of Rotator Cuff Injuries: Clinical Practice Guideline American Academy of Orthopaedic Surgeons Rosemont, IL, USA 202510.5435/JAAOS-D-20-0045033156216 · doi ↗ · pubmed ↗