Validation of the SCOPETAS Scale for Nursing Professionals in Pediatric Interhospital Transport
Marina Medina-Valles, Ana Elisa Laso-Alonso, Alberto Medina-Villanueva, Vicent Modesto-i-Alapont, David Zuazua Rico, Alba Maestro-Gonzalez

TL;DR
This study validates the SCOPETAS scale for nurses in pediatric interhospital transport, showing strong agreement with physicians' decisions, especially in severe cases.
Contribution
The study provides the first validation of the SCOPETAS scale specifically for nursing professionals in pediatric transport settings.
Findings
Nurses achieved 91.4% correct team composition decisions in severe cases and 73.9% in mild cases.
The SCOPETAS scale showed high concordance with physicians' decisions when used by nurses.
Having a Master’s degree was inversely associated with decision accuracy among nurses.
Abstract
Background: Pediatric Interhospital Transport demands highly specialized, coordinated care to ensure safety and continuity across settings. The SCOPETAS scale, recently adapted into Spanish from the Pediatric Transport Triage Tool, has been validated for physicians but not for nurses. Objective: To validate the SCOPETAS scale for use by nursing professionals in Pediatric Interhospital Transport. Methods: A cross-sectional inter-rater reliability study using clinical vignettes was conducted between December 2024 and February 2025 with nurses from eight hospitals within a Spanish autonomous community. Participants applied the SCOPETAS scale to two simulated pediatric transport scenarios. Agreement with physicians’ decisions (gold standard) was analyzed using weighted kappa statistics, logistic regression, and ROC curve analysis. Results: A total of 128 nurses participated (91% female;…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
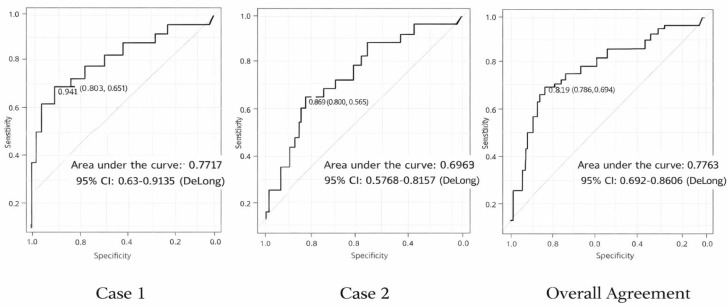 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTrauma and Emergency Care Studies · Disaster Response and Management · Travel-related health issues
1. Introduction
Interhospital transport (IHT) is a vital component of healthcare delivery, especially when patients require urgent or specialized care unavailable at the referring facility [1]. Unlike primary emergency transport, which prioritizes rapid transfer to the nearest hospital, IHT aims to ensure continuity and quality of care by relocating patients to centers equipped to provide the necessary specialized treatment. In pediatric populations, interhospital transfer of critically ill patients carries a significant risk of adverse events, especially when performed by non-specialized teams, with historical rates ranging from 5% to 20% [2,3]. Furthermore, it promotes equity in access to high-complexity services, particularly for patients from rural or peripheral areas.
Despite its importance, there is no internationally standardized model for pediatric transport teams, resulting in considerable variability in resources, competencies, and clinical practice. In Spain, the Sistema de Valoración de Pacientes para el Transporte Secundario (SVPTS) provides guidance for adjusting team composition according to patient severity in adult critical care, but its applicability is limited by regional heterogeneity and its adult-oriented design [4].
In pediatrics, validated tools are scarce. Two scales have been developed: a pediatric adaptation of SVPTS and the Pediatric Transport Triage Tool (PT3) [5], based on the Pediatric Early Warning Score (PEWS) [6]. PT3 incorporates critical transport-related factors such as sedation, vasoactive drugs, and advanced respiratory support. Recently, the PT3 tool underwent cultural adaptation into Spanish and was validated among physicians, resulting in the SCOPETAS scale [7]. A subsequent evidence-based evaluation conducted in Spain further demonstrated the utility of SCOPETAS for optimizing team composition during urgent interhospital transfers, confirming its applicability and safety in real-world clinical practice [8].
The initial validation of SCOPETAS showed excellent inter-rater reliability among physicians (κ = 1) and substantial agreement between actual clinical practice and scale recommendations (weighted κ = 0.68; p < 0.001) [7]. However, its application among nursing professionals has not been studied. Given the variability in pediatric IHT team composition and the absence of validated nursing-specific tools, assessing SCOPETAS validity in this professional group is crucial to ensure safe, efficient, and consistent care.
The primary objective of this study was to evaluate the validity of the SCOPETAS scale when applied by nursing professionals. Specifically, we aimed to determine inter-rater agreement with the physician gold standard and to analyze diagnostic performance and predictors of correct classification.
2. Materials and Methods
2.1. Design
This study used a cross-sectional validation design based on two standardized clinical vignettes previously employed in the original SCOPETAS physician validation study between December 2024 and February 2025. Nursing professionals independently applied the scale, and their decisions were compared with the established physician gold standard.
2.2. Participants
The study included nurses working in pediatric services across eight hospitals within a Spanish autonomous community: one tertiary hospital with comprehensive pediatric specialties, six hospitals with pediatric emergency and inpatient care, and one mixed adult–pediatric facility. All eligible nurses were informed about the study and invited to participate voluntarily. Those who agreed provided informed consent and accessed the online sociodemographic questionnaire. Participation was voluntary, anonymous, and non-incentivized. No exclusion criteria were applied.
2.3. Instrument
The SCOPETAS scale evaluates pediatric patient severity across three domains (neurological, cardiovascular, respiratory; 0–3 points each) and considers the presence of a significant diagnosis (Appendix A.1).
Total score (0–9) determines team composition:
- • 0–1: Emergency Medical Technician (EMT)
- • 2–4: Nurse + EMT
- • ≥5: Physician + Nurse + EMT
A score of 3 in any domain or the presence of a significant diagnosis automatically indicates a full team. The Spanish version of the scale was previously validated among physicians using simulated scenarios, yielding a weighted κ = 0.685 (95% CI: 0.582–0.789; p < 0.001) [7].
2.4. Procedure
Following the methodology of the physician validation study, participants evaluated the same two standardized clinical cases (Appendix A.2 and Appendix A.3):
- Severe case: Infant with bronchiolitis and severe respiratory distress requiring non-invasive ventilation—full team indicated (Physician + Nurse + EMT).
- Mild case: Stable patient with uncomplicated acute appendicitis—EMT only indicated.
Participants received a printed packet containing the two standardized clinical vignettes, the SCOPETAS scale, and all necessary supporting materials. They completed the assessment on paper under unsupervised conditions to minimize external influence and ensure uniform case presentation. Subsequently, they entered their sociodemographic data and transcribed their responses into a Google Forms questionnaire. No time limit was imposed to allow careful application of the scale, mirroring real-world decision-making.
2.5. Variables
Collected data included demographic (age, sex), academic (highest degree, specialized training), and professional characteristics (years of experience, pediatric experience), as well as SCOPETAS-based transport team decisions for each vignette.
2.6. Data Analysis
Analyses were performed with SPSS v.21 and R v.4.3.3. Descriptive, bivariate, andmultivariate (logistic regression) analyses were conducted. ROC curves evaluateddiscrimination. Significance was set at p < 0.05.
Bayesian posterior distributions were estimated via Markov Chain Monte Carlo (100,000 iterations) under a minimally informative Beta-Binomial prior. For the analysis, library rstan from R v.4.3.3 was used, with 4 Marcov chains, 1000 warm-up iterations per chain, and a total number of 25,000 iterations per chain in 2 cores. For the convergence diagnostics, Gelman’s Rhat and the effective sample size were used as analytical tools, and graphically, the traceplot method was used to plot the time series of the posterior draws.
2.7. Ethical Considerations
The study was approved by the Regional Research Ethics Committee (No. 2024.466). Participation was voluntary and anonymous. No real patient data were collected, and all procedures complied with the Spanish Organic Law 3/2018 on Data Protection and Digital Rights.
3. Results
3.1. Participant Characteristics
Of the 175 nurses invited, 128 completed the assessment (response rate 73.1%). Participants were predominantly female (91%, n = 117) with a mean age of 39.5 ± 10.3 years. Most held a Bachelor’s/Diploma degree (64.1%), followed by Master’s (15.6%), Pediatric Nursing Specialist certification (19.5%), and Doctorate (0.8%). Mean professional experience was 15.8 years, including 6.2 years in pediatrics. Most participants worked in tertiary hospitals, primarily in pediatric emergency, inpatient, or intensive care units (Table 1).
3.2. Application of SCOPETAS
In Case 1, 91.4% correctly identified the full team requirement; in Case 2, 73.9% selected the EMT-only team. Full agreement across both cases occurred in 66.9% (95% CI: 58–75%). High respiratory scores predominated in Case 1, while Case 2 showed mostly zero values (Table 2).
3.3. Factors Associated with Accuracy
Longer pediatric experience slightly reduced accuracy (OR = 0.992; 95% CI: 0.984–0.999; p = 0.03). Holding a Master’s degree decreased the odds of correct classification in both cases and for Overall Agreement (OR = 0.27; 95% CI: 0.11–0.70; p = 0.006) (Table 3).
3.4. Diagnostic Performance
For Case 1, sensitivity was 64.7%, specificity 83.3%, PPV 97.4%, and NPV 19.6%.
For Case 2, sensitivity was 80.0%, specificity 48.5%, PPV 81.7%, and NPV 45.7%.
Overall full-agreement model: sensitivity was 67.1%, specificity 81.0%, PPV 87.7%, and NPV 54.8%. Detailed indices are presented in Table 4 and Figure 1.
3.5. Comparison with Medical Decisions
Compared to physicians’ decisions (gold standard), nursing decisions achieved a sensitivity of 91%, specificity 74%, LR+ 3.48, LR-0.12, and substantial evidence weight (positive 5.4 deciban; negative −9.1 deciban) (Table 5).
4. Discussion
Pediatric Interhospital Transport (IHT) triage remains insufficiently explored in nursing research despite its growing relevance in increasingly complex care environments. This study provides the first validation of the SCOPETAS scale among nursing professionals, extending its previous physician-based validation to the nursing context and addressing a key gap in pediatric transport decision-making.
In this study, the application of the SCOPETAS scale by nursing professionals demonstrated high concordance with physicians’ decisions, particularly in the severe scenario. The lower item-level agreement observed in the respiratory domain of Case 1—where 56% of participants assigned a score of 2 despite the presence of BiPAP, which corresponds to a score of 3 according to the scale—indicates a discrepancy between domain-specific scoring and the final team selection. Importantly, SCOPETAS incorporates redundant decision pathways inherited from the original PT3 instrument, whereby a full-team recommendation is triggered either by a score of 3 in any single domain or by a cumulative total score ≥3 across domains. Consequently, even when the respiratory domain was underscored, participants frequently reached a total score consistent with the correct full-team assignment. This redundancy enhances the safety and robustness of the tool, helping to preserve final decision accuracy despite isolated item-level errors, while also underscoring the need to reinforce targeted training in domain-specific scoring—particularly regarding advanced respiratory support modalities—to ensure precision at both the item and overall decision levels.
The high positive predictive value indicates that when nurses recommend a full team, the decision is almost always appropriate, reinforcing the scale’s reliability and its potential to optimize specialized resources. The inverse association between holding a Master’s degree and accuracy should be interpreted cautiously. The small size of this subgroup, limited historical involvement of nurses in transport team decisions within the Spanish healthcare system, and heterogeneity in postgraduate training pathways may all contribute to this finding. Rather than suggesting a deficit, these results underscore the opportunity to strengthen structured, competency-based training in SCOPETAS and progressively integrate nursing professionals into transport-related decision-making. Interpretation of predictive values must consider the study design; because the two vignettes represent extreme severity levels, PPV and NPV reflect the imposed case mix rather than real epidemiological prevalence. These values should therefore not be extrapolated directly to clinical settings, where the proportion of severe cases varies across hospitals and time periods. The intermediate SCOPETAS category (Nurse + EMT) could not be evaluated because the study intentionally replicated the original physician validation, which included only mild and severe cases. This approach ensured methodological comparability but limited assessment of the scale’s full operational range. Future research incorporating intermediate-severity scenarios will be essential to evaluate the discriminative capacity and practical applicability of this category in nursing practice.
No significant associations were found with age, sex, or hospital type, suggesting broad applicability across diverse clinical settings. The high concordance with physicians (sensitivity 91%, specificity 74%) reinforces SCOPETAS as a robust tool to support nursing decision-making in pediatric IHT. Internationally, countries with advanced pediatric transport systems, such as the UK, have implemented standardized triage protocols, though these remain predominantly physician-led [9,10,11].
Validating SCOPETAS for nursing professionals represents an innovative contribution that may enhance nursing autonomy, patient safety, and equitable access to specialized pediatric care.
From an organizational perspective, integrating SCOPETAS could improve system efficiency by accurately identifying cases that do not require full teams, thereby optimizing resource allocation without compromising safety. Digital integration may further facilitate its clinical use and enable continuous quality monitoring. Nonetheless, multicenter studies with larger samples and a broader range of clinical scenarios will be necessary to rigorously assess the external validity and real-world applicability of SCOPETAS in nursing practice.
Limitations
This study used simulated scenarios within a single autonomous community, limiting external validity. The online data collection format precluded replication of real-world transfer dynamics. Moreover, the intermediate configuration (Nurse + EMT) was not assessed, warranting future research.
5. Conclusions
The findings of this study suggest that SCOPETAS may contribute to improved patient safety and more efficient resource allocation when applied by nursing professionals. Although the tool demonstrated promising validity in this simulated context, additional research—ideally incorporating real-world clinical environments, a broader range of clinical scenarios, and multicenter designs—is needed to more accurately determine its practical applicability and to guide its potential integration into routine nursing practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vadlaputi P. Jafri M. Kohler J. Newton C. Semkiw K. Marcin J.P. Impact of the “Triple-Demic” on Interfacility Transfers and Consultations: A Retrospective Study Pediatr. Emerg. Care 202541 e 94e 9910.1097/PEC.000000000000341440386945 · doi ↗ · pubmed ↗
- 2Corniero P. Girona-Alarcón M. Alejandre C. Campos R. Millán García Del Real N. Esteban E. Assessment of Patient Safety during Interfacility Transport An. Pediatría Engl. Ed.202510250388410.1016/j.anpedi.2025.50388440527689 · doi ↗ · pubmed ↗
- 3Sociedad y Fundación Española de Cuidados Intensivos Pediátricos Grupo de Estabilización y Transporte Pediátrico. Perfil Competencial Del Médico Que Realiza Transporte Pediátrico 2018 Available online: https://secip.info/images/uploads/2018/05/perfil-competencial-medico-que-r-ealiza-transporte-pediatrico 22022018.pdf(accessed on 31 August 2025)
- 4Moreno Millán E. Serrano S. Bóveda J. Sistema de Valoración de Pacientes Para El Transporte Sanitario: Resultado de Su Aplicación En Transporte Secundario Med. Intensiv 198812432438
- 5Steffen K. Noje C. Costabile P. Pediatric Transport Triage: Development and Assessment of an Objective Tool to Guide Transport Planning Pediatr. Emerg. Care 20203624024710.1097/PEC.000000000000164130461668 PMC 6526089 · doi ↗ · pubmed ↗
- 6Akre M. Finkelstein M. Erickson M. Liu M. Vanderbilt L. Billman G. Sensitivity of the Pediatric Early Warning Score to Identify Patient Deterioration Pediatrics 2010125 e 763e 76910.1542/peds.2009-033820308222 · doi ↗ · pubmed ↗
- 7Alonso A.E.L. Norniella C.M. del Villar Guerra P. Solís D.P. Valles M.M. Villanueva A.M. Score Pediátrico de Transporte En Asturias (SCOPETAS). Triaje En Transporte Pediátrico Bol. Pediatría 202565808910.63788/rysqn 451 · doi ↗
- 8Laso-Alonso A.E. Del Villar-Guerra P. Molinos-Norniella C. Modesto-Alapont V. Pérez-Solís D. Medina-Villanueva A. Enfoque basado en la evidencia para la selección del recurso humano de transporte urgente An. Pediatría 202510350399710.1016/j.anpedi.2025.50399741224546 · doi ↗ · pubmed ↗