Tick-Borne Co-Infection in Lyme Disease: Clinical Impact, Diagnostic Challenges, and Therapeutic Perspectives
Georgi Popov, Dzhaner Bashchobanov, Radina Andonova

TL;DR
This paper reviews tick-borne co-infections with Lyme disease, focusing on their clinical impact, diagnostic challenges, and treatment options.
Contribution
The paper provides a comprehensive synthesis of current knowledge and identifies evidence gaps in managing tick-borne co-infections.
Findings
Co-infections can increase disease severity and complicate diagnosis due to overlapping symptoms.
Current diagnostic methods have limitations in detecting tick-borne co-infections.
Treatment strategies need to be pathogen-specific and sometimes combined for effective management.
Abstract
Tick-borne co-infections are an increasingly recognized and clinically important aspect of Lyme borreliosis, particularly in regions where Ixodes ticks transmit a wide range of bacterial, protozoan, and viral pathogens. In addition to Borrelia burgdorferi sensu lato, these ticks frequently harbor microorganisms such as Babesia spp., Anaplasma phagocytophilum, Ehrlichia spp., Borrelia miyamotoi, Bartonella spp., and several tick-borne viruses. Co-infections may increase disease severity, prolong symptom duration, and contribute to atypical or overlapping clinical presentations, thereby complicating diagnosis and management. Growing evidence from epidemiological studies, clinical case series, and experimental in vivo and in vitro models indicates that pathogen–pathogen and pathogen–host interactions can modulate immune responses and influence disease progression. Diagnostic challenges…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
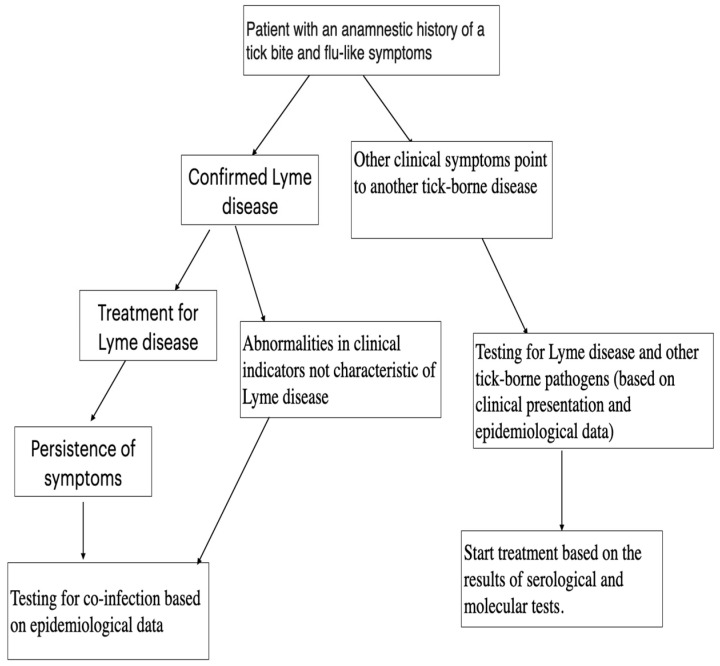 Figure 2
Figure 2|
|
|
| Tick-Borne | |||||
|---|---|---|---|---|---|---|---|---|
| doxycycline [ | atovaquone and azithromycin [ | doxycycline [ | supportive treatment [ | |||||
| ceftriaxone [ | clindamycin and quinine [ | rifampin [ | azithromycin [ | |||||
| Amoxicillin [ | fluoroquinoles [ | |||||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVector-borne infectious diseases · Bartonella species infections research · Zoonotic diseases and public health
1. Introduction
Lyme disease (LD) is a multisystemic illness and the most common tick-borne disease in the Northern Hemisphere. It is caused by spirochetes of the Borrelia burgdorferi sensu lato complex (Bbslc) and is transmitted to humans through bites from black-legged ticks of the genus Ixodes [1,2]. In Europe, the main causative agents are Bo. burgdorferi sensu stricto, Bo. garinii, Bo. afzelii, Bo. bavariensis, and the recently identified Bo. mayonii; their primary vectors are I. ricinus and I. persulcatus [1,3]. In Asia, Bo. garinii is the predominant causative agent, transmitted by I. ricinus, I. persulcatus, and I. ovatus [4]. In North America, B. burgdorferi sensu stricto and Bo. mayonii are the most common cause, with I. scapularis and I. pacificus serving as principal vectors [1,5,6].
Ixodes ticks are a major public health concern because they are widespread, increasingly found near humans, and can carry multiple pathogens at once [7,8,9,10]. Besides Bbslc, they can spread bacteria like Borrelia miyamotoi (Bo. miyamotoi)-relapsing fever borreliosis [7,11] and Anaplasma phagocytophilum (An. phagocytophilum)-human granulocytic anaplasmosis [7,12], as well as Neoehrlichia mikurensis (N. mikurensis)-Neoehrlichiosis and Ehrlichia ssp.-human ehrlichiosis [7,13,14]. Transmissible viruses include tick-borne encephalitis virus (TBEV), Powassan virus (POWV), Louping Ill Virus, and Eyach virus (EYAV) [7,15,16,17,18]. Ixodes ticks also transmit parasites such as Babesia divergens (Ba. divergens), Ba. microti, Ba. duncani, and Ba. venatorum, which causes human babesiosis [7,19,20].
The potential for ticks to transmit multiple pathogens highlights the growing concern of co-infections associated with Lyme disease. Simultaneous infection with several pathogens can alter clinical presentations, complicating both the diagnosis and management of these diseases [21]. This literature review aims to explore the link between the presence of diverse tick-borne pathogens and the increased complexity in diagnosing and treating Lyme disease, with particular attention to selecting appropriate therapeutic strategies for managing co-infections.
2. Epidemiology of Vectors and Co-Occurrence Pathogens
As mentioned above, different species of Ixodes ticks are found across various continents and regions, each transmitting distinct species of Bbslc. Additionally, these ticks are associated with different co-infections.
I. ricinus, which is the main vector of Lyme disease in Europe (Bo. burgdorferi sensu stricto (Bbss), Bo. garinii, Bo. afzelii, Bo. bavariensis), can also transmit TBEV, EYAV, Anaplasma phagocytophilum, Neoehrlichia mikurensis, Ba. divergens, Ba. venatorum, and various species of Rickettsia [7]. Numerous European studies (Switzerland [22,23], Poland [24,25], Scandinavian countries [26], Bulgaria [27], etc.) demonstrate that I. ricinus can be infected with more than one pathogen, with the most common combinations being between Bbsl and An. phagocytophilum or Babesia ssp. [28], which directly increase the risk of co-infections in humans (Table 1 and Figure 1).
I. persulcatus is the main vector of LD in Northern Europe, Russia, and Asia. In addition to Bbslc, they can also transmit TBEV, Omsk hemorrhagic fever virus (OHFV), and Bo. miyamotoi, An. phagocytophilum, Neoehrlichia mikurensis, Ehrlichia muris (E.muris), Riketsia spp., and Ba. venatorum [7]. A study in Mongolia found that 49% of a total of 346 I. persulcatus ticks tested were infected with Bbslc, Ehrlichia sp.—16%, A. phagocytophilum—13.5%, Bo. mayomatoi—4.9% and TBEV—1.7%. Co-infections between Bbslc and the other pathogens studied were as follows (presented as a percentage of ticks with Bbslc and another pathogen—55 ticks)—TBEV—3.6%, Bo. mayomatoi—10.9%, A. phagocytophilum—30.9%, Ehrlichia sp.—36.4%. In 18.2% (10 ticks) of the ticks infected with Bbslc, in which more than one pathogen was detected, triple infections were found—in one of them a combination of TBEV, Bbslc, and A. phagocytophilum, and another had the following combination: TBEV, Bbslc, and Ehrlichia sp. The remaining eight were found to be simultaneously infected with Bbslc, Ehrlichia sp., and A. phagocytophilum [30]. Russia provides some of the best-documented data on co-infections in I. persulcatus, a tick species endemic to northern and eastern Eurasia. Studies from various regions—including Saint Petersburg [31], Vologda [32], Kirov [33], and Karelia [34]—show a high frequency of multiple pathogens within individual ticks. The prevalence of co-infections varies between these geographical areas. In the study by Alekseev et al. [31] from the St. Petersburg region, a total of 1282 adult ticks and 19 nymphs were collected. Among these, 120 ticks harbored two pathogens, most commonly a combination of Bo. afzelii and Bo. garinii (43%), followed by Bo. garinii and Bbss (15.5%), and Bo. afzelii and Ehrlichia muris (15.5%). Triple infections were found in 22 ticks, most frequently involving Bo. afzelii, Bo. garinii, and either E. muris (22.7%) or TBEV (22.7%). Additionally, Ba. microti and A. phagocytophilum were detected. In Eremeeva et al. [32]’s study from the Vologda region, populations of I.persulcatus. ticks were examined over two consecutive years for Bbslc, An. phagocytophilum, E. muris, and certain Rickettsia species. The most common in the presence of co-infections were Bbslc with An. phagocytophilum and Bbslc with E. muris. In the Kirov region study [33], 322 ticks were examined; 155 were infected with at least one pathogen. Out of these, a quarter contained more than one pathogen (36 with double infections and 5 with triple infections). In the Karelia region [34], ticks collected between 2007 and 2018 were studied. No An. phagocytophilum carriage was detected. Of 400 I. persulcatus ticks, 142 harbored mixed infections, most commonly Bbslc with TBEV or Bbslc with Ehrlichia spp. A study from Finland [35] examined 2014 I. ricinus and 1451 I. persulcatus ticks. Of the I. ricinus ticks, 49 (2.4%) were found to carry more than one pathogen, most commonly Bbslc and Rickettsia spp. (1.5%). Among I. persulcatus ticks, only 11 (0.8%) carried multiple pathogens, with Bbslc and Rickettsia spp. present in each case.
I. scapularis is one of the primary vectors of LD in North America. In addition to Bbslc, it can transmit other pathogens, including bacteria (An. phagocytophilum, E. muris, Bo. mayonii, etc.), viruses (POWV, South Bay virus, etc.), and eukaryotes/parasites (Ba. microti and Ba. duncani) [7]. Numerous studies [10,36,37] have investigated the range of pathogens found in these ticks. In one study conducted in Wisconsin [36], 112 ticks were examined: 42.9% carried Bbslc, 46.4% carried Rickettsia spp., 10.7% A. phagocytophilum, 3.6% Ehrlichia spp., 0.9% Bo. mayonii, 1.8% POWV, 51.8% South Bay virus, and 8.9% Ba. microti. A significant positive correlation was found between infection with South Bay virus and Bb (p-value = 1.4 × 10^−3^). In another study from Minnesota [37], 1240 nymphs of the species I. scapularis were examined, with 25.24% found to be infected with Bbss. Additionally, Bo. mayonii, Bo. miyamotoi, An. phagocytophilum, E. muris, Ba. microti, and POWV were detected. Co-infections occurred in 7.26% of the nymphs, involving combinations of two, three, or even four pathogens. The most common co-infections were between Bbss and An. phagocytophilum or Bbss and Ba. microti. The most frequent triple co-infection involved Bbss, An. phagocytophilum, and Ba. microti, though combinations with all studied pathogens were found. Notably, Bbss was always present in nymphs harboring four pathogens. A study from New Jersey [10] examined 662 adults and nymphs of the species I. scapularis collected between 2020 and 2021. One quarter of the nymphs and slightly more than half of the adults were carriers of pathogens. The most commonly detected pathogen was Bbslc. The study also reported data on specimens carrying two or three pathogens, with the most frequent co-infection combinations being Bbslc with An. phagocytophilum, and Bbslc with Ba. microti. The most common triple infection involved Bbslc, An. phagocytophilum, and POWV.
I. pacificus is another known vector of Lyme disease (LD) in North America, besides Bbslc. It can also transmit other pathogens, including Bo. miyamotoi, A. phagocytophilum, and Ba. duncani [7]. A Canadian study [38] examined 9858 I. scapularis and 691 I. pacificus ticks, finding that Bb was the most common pathogen: 18.8% in I. scapularis and 0.3% in I. pacificus. No other pathogens or co-infections with Bb were found in I. pacificus. In I. scapularis, the most frequent combination was Bb with A. phagocytophilum. A large-scale US study [39] analyzed 13,400 Ixodes ticks (I. scapularis and I. pacificus) from 17 states and the District of Columbia: 12,636 were I. scapularis and 764 were I. pacificus. All were tested for Bbss, Bo. miyamotoi, Bo. mayonii, A. phagocytophilum, and Ba. microti. Bbss was the most frequently isolated pathogen (26.7%), mainly in I. scapularis, while only 2.35% of I. pacificus carried it. This trend—lower rates of pathogen detection in I. pacificus compared to I. scapularis—was also seen for the other three microorganisms studied. The most common co-infection was observed between Bbss and A. phagocytophilum (2.2%). In I. pacificus ticks, however, none of the three pathogen combinations studied (Bbss + A. phagocytophilum, Ba. microti, or A. phagocytophilum + Ba. microti) were detected.
3. The Clinical Characteristics of Co-Infections in Lyme Disease
Ticks can carry more than two pathogens. Studies from Europe and North America have shown that more than one pathogen can be isolated from a single tick [22,23,24,25,26,27,28,30,31,32,33,34,35,36,37,38,39]. Experimental data confirm that Ixodes ticks can transmit at least two pathogens with one bite [40], most commonly Borrelia burgdorferi together with Anaplasma phagocytophilum or Babesia microti [20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36]. However, there are no well-documented human cases in the literature in which three or more pathogens have been transmitted by a single tick bite. This may be due to several biological factors, including the specific location of each pathogen within the tick, interactions between co-infecting pathogens, and their clearance by the human immune system [41]. Thus, while multi-pathogen transmission from a single bite is possible, it appears to be relatively uncommon.
3.1. Co-Infection with Borrelia burgdorferi and Babesia spp.: Clinical Presentation and Diagnosis
Babesia spp. can cause human babesiosis, which may present with a range of clinical symptoms depending on the level of parasitemia, patient age, immune status, and the presence of comorbidities. Mild disease may be asymptomatic, whereas moderate disease can present with flu-like symptoms such as fever, headache, myalgia, and arthralgia. In severe cases, babesiosis may lead to hemolytic anemia, acute respiratory distress syndrome, acute kidney injury, bilirubinuria, and even death [20,42,43].
Following a tick bite, Babesia spp. enter the capillary circulation, invade red blood cells, then mature and multiply. Once they reach the merozoite stage, they exit and lyse the red blood cells, then invade new erythrocytes [42].
Co-infection with Borrelia burgdorferi and Babesia spp. has been documented in endemic regions where the two pathogens share the same vector. In a study conducted by Krause et al. [44], 240 patients with Lyme borreliosis were followed longitudinally. Among them, 26 patients (11%) showed evidence of co-infection with Babesia microti. These co-infected individuals experienced a more severe clinical course, characterized by prominent symptoms such as headache, fever, splenomegaly, and profuse sweating. Moreover, half of the co-infected patients had symptoms lasting 3 months or longer, compared with only 7 of 184 patients with Lyme disease alone. In another study from Spain, Folgueras et al. [45] followed 120 patients with confirmed Lyme disease, 47 of whom (39.2%) were seropositive for Ba. venatorum/divergans. They found that patients with coinfection more frequently experienced cardiorespiratory symptoms, such as dyspnea and atrioventricular (AV) block. Hoversten et al. [46] presented a clinical case of a woman who, at the end of a 21-day course of amoxicillin for Lyme disease, developed a fever of 39.4 °C and myalgia, nausea, and fatigue. Laboratory results revealed anemia and thrombocytopenia. A PCR test for Ba. microti DNA was positive, and she was treated with azithromycin and atovaquone for 10 days, which led to an improvement in her general condition, normalization of body temperature, and an increase in erythrocyte, hemoglobin, and platelet counts.
In an experimental study with mice, Djokic et al. [47] found that Ba. microti can suppress the acquired immune response, significantly reducing the number of B and T cells in the spleen of mice co-infected with Bo. burgdorferi and Ba. microti compared to naïve mice. The ELISA method was used to assess the humoral immune response to Bo. burgdorferi and showed a suppressed humoral response in co-infected mice. This leads to higher tissue colonization and more severe clinical manifestations of Lyme disease. Destruction of the marginal zone and atrophy of B cells in the spleen begin in the acute phase of parasitemia, resulting in weaker antibody production, which is necessary for clearing Bo. burgdorferi from the body. This is observed in younger mice, in which it is assumed that, during co-infection, a Th1-mediated immune response predominates, in contrast to co-infected older mice, in which a Th2-mediated response predominates [48]. It has been found that, in co-infection, inflammatory arthritis is more severe and can persist for up to 16 weeks after infection [49].
On the other hand, infection with Bo. burgdorferi activates the TLR2 signaling pathway, leading to activation of macrophages and polymorphonuclear cells. This results in a reduction in parasitemia in mice co-infected with Ba. microti and Bo. burgdorferi [50,51,52]. Other studies in humans [53] and mouse models [54] have not found a statistically significant difference in the clinical course between infection with Bo. burgdorferi alone and co-infection with Bo. burgdorferi and Babesia spp.
Diagnosis in patients co-infected with Bbslc and Babesia spp. can be challenging, as both diseases may present with a wide range of clinical signs and overlapping symptoms [55]. As mentioned above, human babesiosis may follow a mild course with flu-like symptoms such as myalgia, fever, and headache. Although rare, LD may present in a similar way, particularly when the initial erythema migrans goes unnoticed. In a study from Italy involving residents of an LD-endemic region, approximately 17% of individuals with confirmed LD reported flu-like complaints [56]. In a meta-analysis by Boyer [57], about 48.1% of patients diagnosed with LD had flu-like symptoms and positive serology or PCR results. According to the recommendations of the Infectious Diseases Society of America (IDSA) [58,59], the diagnosis of LD is based on positive two-tier serology—an initial positive ELISA followed by a positive Western blot—whereas the diagnosis of human babesiosis is based on a positive polymerase chain reaction (PCR) result or visualization of protozoa on a blood smear, which is considered the gold standard [20]. In cases of co-infection with both pathogens, immune dysregulation may occur, potentially leading to negative serological results for Bbslc infection and, consequently, delayed diagnosis and treatment [42]. Co-infection with Bbslc and Babesia spp. should be considered in patients who present with more severe and/or persistent symptoms despite adequate treatment, or with hematological abnormalities such as hemolytic anemia, thrombocytopenia, hepatomegaly, and splenomegaly. In these cases, in addition to serological testing for Bbslc infection, PCR testing for Babesia spp. and a blood smear are recommended [42].
3.2. Co-Infection with Borrelia burgdorferi and Anaplasmosis phagocytophilum: Clinical Presentation and Diagnosis
An. phagocytophilum is an obligate intracellular, Gram-negative rickettsia. Unlike other Gram-negative organisms, it lacks surface lipopolysaccharides, which, together with its ability to block lysosome fusion, protects it from neutrophil activity and allows it to survive within these cells. During infection with An. phagocytophilum, proinflammatory cytokines are produced, leading to neutrophil degranulation and tissue damage [60].
Similarly to infection with Babesia spp., the clinical presentation can range from asymptomatic to severe or, very rarely, fatal. The most common symptoms are nonspecific fever, headache, myalgia, and gastrointestinal manifestations, most frequently diarrhea [20,61].
In a study conducted in Romania involving 80 participants with Lyme disease and a history of tick bites, 10% were seropositive for An. phagocytophilum [62]. In another study from Poland that examined the antibody response to Bo. burgdorferi infection in 93 forest workers (a high-risk group for tick bites), 28 showed positive serological evidence of co-infection with Bo. burgdorferi and An. phagocytophilum [63]. In a large Czech study of 314 patients, approximately 8% were seropositive for co-infection with the two pathogens [64]. According to Boyer’s systematic review, the association between erythema migrans and infection with An. phagocytophilum is the second most frequently reported [57].
Available clinical studies on co-infection with Bo. burgdorferi and An. phagocytophilum show only limited and inconclusive evidence that co-infection significantly changes the clinical course of Lyme disease [65,66]. The largest prospective study in early Lyme disease (erythema migrans) found co-infection rates of 2–10%, with a statistically significant increase in symptom number only in a small subgroup of co-infected patients [67]. Overall, disease course, severity, and response to therapy are generally similar to Lyme disease alone [58]. Systematic reviews support that most patients with Bo. burgdorferi and An. phagocytophilum do not experience clearly worse symptoms, though about one-fifth show additional systemic findings such as fever and hematologic abnormalities [57].
Data from animal models indicate that co-infection with Bo. burgdorferi and An. phagocytophilum can lead to substantial changes both in pathogen distribution and in the host immune response [68]. In the C3H/HeN mouse model, Holden et al. demonstrated that co-infection with An. phagocytophilum results in a broader tissue dissemination of Bo. burgdorferi compared with monoinfection, without significantly affecting the bacterial load of Anaplasma, suggesting an asymmetric interaction between the two pathogens [69]. At the same time, co-infected animals exhibit a reduced pathogen-specific antibody response against An. phagocytophilum, as well as alterations in the cytokine profile, characterized by decreased Th1-mediated activity (IFN-γ, IL-12) and a relative increase in pro-inflammatory mediators such as IL-6. These changes may facilitate the persistence and dissemination of Bo. burgdorferi [57,69]. Overall, data from experimental models suggest that co-infection can amplify tissue involvement and the inflammatory manifestations of Lyme disease, including arthritis, through immunomodulation, providing a biologically plausible explanation for the observed clinical variability and diagnostic challenges in humans with tick-borne co-infections [57].
Similarly to human babesiosis, the clinical presentation of HGA is heterogeneous, with flu-like symptoms being the most common. This may result in delayed diagnosis and, consequently, delayed initiation of treatment. Although serological testing is most frequently used to diagnose An. phagocytophilum infection, direct visualization on a blood smear and the use of PCR-based methods are more suitable for achieving an accurate diagnosis [70].
3.3. Co-Infection with Borrelia burgdorferi and Ehrlichia spp.: Clinical Presentation and Diagnosis
Ehrlichia species cause human ehrlichiosis. Several Ehrlichia species have been identified to date: E. chaffeensis (human monocytic ehrlichiosis, HME), E. ewingii (human granulocytic ehrlichiosis, HGE), Ehrlichia muris-like agent (EMLA), and E. muris. Similarly to the tick-borne diseases discussed above, the symptoms of ehrlichiosis are nonspecific—myalgia, fever, headache, and sometimes gastrointestinal manifestations or rash [71]. The severity of the clinical presentation varies and depends on the individual’s immunological status, which is why hospitalizations among adult patients are more frequent [72].
Unlike the pathogens discussed so far, we did not find any retrospective or prospective studies comparing patients with Lyme disease alone and those co-infected with Bo. burgdorferi and Ehrlichia spp. We identified several clinical case reports describing patients who were seropositive for both pathogens, but no significant worsening of the clinical course was reported [57,73,74,75]. Although it is biologically plausible for both pathogens to be transmitted simultaneously by a single tick bite, there are no published data on the simultaneous occurrence or exacerbation of symptoms of both infections.
In experimental mouse models, it has been reported that simultaneous exposure to both pathogens results in significantly more pronounced tissue and joint inflammation, as well as more frequent cytopenic conditions, compared with monoinfected mice. These data support the possibility of an immunomodulatory effect of concurrent infection with Bo. burgdorferi and Ehrlichia spp. [76].
Serological testing and PCR-based methods are most frequently used to diagnose Ehrlichia spp. Infections [71,72].
3.4. Co-Infection with Borrelia burgdorferi and N. mikurensis: Clinical Presentation and Diagnosis
Neoehrlichiosis, whose etiological agent is N. mikurensis [77], is a relatively new infectious disease, with the first case published in 2014 [78].
N. mikurensis is an intracellular, Gram-negative pathogen that infects, survives, and develops in the endothelial cells of blood vessels. Typically, the infection is accompanied by high fever, chills, sweating, thromboembolic vascular events, deep vein thrombosis, and localized muscle pain in the affected blood vessels [77,79].
In a Norwegian study, 10% of samples from patients with confirmed Lyme disease were also positive for N. mikurensis [80].
We were unable to find published data on experimental animal models that examined changes in immune response and symptoms in relation to monoinfection with Bbslc or N. mikurensis.
There are numerous European studies that have reported the simultaneous presence of both pathogens (Bo. burgdorferi and N. mikurensis) in populations of Ixodes ticks [81,82]. The most likely reason for the limited data on co-infection between these pathogens is that N. mikurensis is a recently identified pathogen and that PCR-based methods are required for its diagnosis.
3.5. Co-Infection with Borrelia burgdorferi and Bartonella spp.: Clinical Presentation and Diagnosis
Bartonella spp. are Gram-negative, facultative intracellular pathogens that can cause multisystemic disease, affecting the liver, spleen, lymph nodes, and central nervous system (CNS). Bartonella spp. can cause cat scratch disease (B. henselae), trench fever (B. quintana), Carrion’s disease (B. bacilliformis), endocarditis, and aseptic meningitis. The clinical manifestations are diverse and may include fever, neurological symptoms, lymphadenopathy, and others [83,84].
There are ample data in the literature demonstrating the presence of Bartonella spp. DNA in Ixodes ticks [85,86,87], but there is still no conclusive evidence that humans can be infected via tick bite [88,89].
Cases have been reported of patients with Lyme disease in whom infection with Bartonella spp. has been demonstrated serologically or by PCR [90]. Two of these involved patients with symptoms characteristic of neuroborreliosis who were followed over time [91]. In the study by Eskow et al., four patients with headache, fever, insomnia, and depression all tested positive for B. henselae infection, but only three had Bbslc DNA detected in their cerebrospinal fluid (CSF) [91]. In another study from Poland, 2 of 17 patients with neuroborreliosis tested positive for B. henselae DNA in CSF [92]. However, there are no controlled studies in the literature comparing the course of simultaneous infection with Bbslc and Bartonella spp. with monoinfection by either pathogen.
Despite evidence of serological and ecological co-exposure between Bo. burgdorferi and Bartonella spp. [85,86,87,90,91,92], we were unable to find published data on animal models in which clinical and immunological outcomes of simultaneous infection with both pathogens were monitored.
The diagnosis of Bartonella spp. is complex and involves several methods: serological testing for IgM/IgG titers, PCR detection, culture isolation of the pathogen, and histopathology. Each of these methods has limitations, but the most conclusive are histopathology (which is also the most invasive for the patient) and culture isolation of the pathogen (which delays diagnosis due to slow bacterial growth). For the most accurate diagnosis, at least two of these methods should be used in combination [93].
3.6. Co-Infection with Borrelia burgdorferi and Rickettsia spp.: Clinical Presentation and Diagnosis
Rickettsia spp. are Gram-negative intracellular pathogens transmitted by arthropods that cause numerous diseases in humans [94].
Epidemiological studies of ticks have found simultaneous carriage of Bbslc and Rickettsia spp., including R. helvetica (which causes Aneruptive fever) and R. monacensis (which causes Mediterranean spotted fever-like disease) [95,96,97]. This suggests that simultaneous transmission of both infections to humans is possible. However, there are no large studies in the literature on the effect of these two pathogens on the clinical presentation. In a study by Tijsse-Klasen et al., out of 67 skin biopsies examined, 47 were positive for Bbslc and only one of these was also positive for R. monacensis, but the symptoms were consistent with Lyme disease, so the effect of Rickettsia spp. was not documented [97]. We were unable to find any animal model studies examining co-infection with Bbslc and Rickettsia spp.
Acute rickettsioses usually present with a characteristic clinical picture, and the differential diagnosis between LD and rickettsioses should not be difficult [98]. However, in the context of more acute symptoms, the diagnosis of LD may be overlooked. Rickettsia spp. infections are confirmed based on clinical presentation and serological and molecular techniques.
3.7. Co-Infection with Borrelia burgdorferi and Borrelia miyamotoi: Clinical Presentation and Diagnosis
The infection with Bo. miyamotoi has a biphasic course, with the first episode dominated by flu-like symptoms, fever, headache, arthralgia, and myalgia, lasting 4–5 days, followed by a relapse of symptoms approximately 9 days later [99,100]. Cases involving the central nervous system have been reported [101,102].
A Dutch study found that 7.4% of patients with confirmed Lyme neuroborreliosis were also positive for Bo. miyamotoi infection [103]. Together with the proven simultaneous presence of both pathogens in Ixodes ticks [104,105], this finding demonstrates that Bo. miyamotoi can be a co-infection in LB.
However, we did not identify any large clinical studies in humans or experimental animal models that specifically examined co-infection with these two pathogens and how it alters the clinical presentation or immunopathology.
A Russian study comparing patients with LB and Bo. miyamotoi infection showed that patients with relapsing fever seek hospital care earlier, as the acute stage of Bo. miyamotoi infection progresses more rapidly than in LB [11].
Bo. miyamotoi infection is detected using serological and molecular methods; a blood smear can also be used [100].
3.8. Co-Infection with Borrelia burgdorferi and Tick-Borne Encephalitis Virus: Clinical Presentation and Diagnosis
The tick-borne encephalitis virus (TBEV) is a spherical, enveloped RNA virus belonging to the genus Flavivirus in the family Flaviviridae [106]. It is found mainly in Northern and Central Europe as well as in Asia [106]. TBEV has pronounced neurotropism and causes a typically biphasic illness. The first phase is characterized by flu-like symptoms, while the second phase may present with signs of meningitis and/or encephalitis—such as headache, paralysis, and confusion. However, the second phase may not develop, and in some cases the infection remains asymptomatic [21].
In a study from Latvia, 51 patients with confirmed dual infection with Borrelia burgdorferi and TBEV were followed. These patients showed a higher frequency of neurological symptoms, biphasic fever, and overlapping systemic manifestations characteristic of both diseases [107]. In a systematic review summarizing data from 655 patients, the most common serologically proven co-infection was between Bbslc and TBEV, which was also among the most frequently confirmed active co-infections [57].
In a mouse study, Porcelli et al. [108] observed that the clinical expression of co-infection depends on the timing of pathogen exposure. Mice infected first with Bo. afzelii and then with TBEV 9 days later developed more severe symptoms and had a higher viral load than those infected with TBEV 21 days after Bo. afzelii infection. Simultaneous infection led to a more moderate clinical course and no deaths. These findings highlight the complexity of the underlying immunological mechanisms and the ways in which the two pathogens influence each other.
Because the two conditions share many clinical features and have similar incubation periods, distinguishing Lyme disease from TBEV infection can be challenging. This is particularly true in cases of co-infection by both pathogens, where their symptoms overlap. A possible co-infection should be suspected when there is an epidemiological connection between the two diseases, unusually severe neurological manifestations, and a biphasic fever pattern. Confirmation of TBEV infection relies on serological testing and molecular techniques such as PCR. The same diagnostic principles apply to the other viral infections discussed (Powassan, Louping ill, and Eyach).
3.9. Co-Infection with Borrelia burgdorferi and Other Tick-Borne Viruses: Clinical Presentation and Diagnosis
As mentioned above, Ixodes ticks can also transmit Powassan, Louping ill, and Eyach viruses [15,16,17].
Powassan virus is a flavivirus, and the disease is rare, occurring in the United States and Canada. The clinical presentation ranges from asymptomatic infection to encephalitis, with symptoms such as fever, headache, vomiting, confusion, paralysis, and seizures [109].
A study from Wisconsin found that 16.4% of 55 Lyme disease–positive samples were also positive for Powassan virus [110]. However, there are insufficient controlled studies in the literature to compare differences in symptoms between mono-infection and co-infection with Powassan virus.
Louping ill virus, similar to Powassan virus and TBEV, belongs to the genus Flavivirus and can likewise cause a wide range of clinical manifestations, from asymptomatic infection to encephalitis [111]. Eyach virus belongs to the genus Coltivirus, like Colorado tick fever virus, and is transmitted by I. ricinus in Europe, with endemic areas in Germany and France [18]. The disease is rare in humans and, like the other viruses discussed, can present with diverse clinical features, ranging from asymptomatic or flu-like illness to neurological involvement such as meningitis, encephalitis, or polyneuritis [112].
We were unable to find experimental animal models that examined co-infection between the viral pathogens considered and Bbslc, which tracked changes in the clinical presentation and immunopathology during simultaneous infection with these pathogens.
4. Treatment and Prevention of Lyme Disease and Co-Infections
Accurate diagnosis is essential for appropriate treatment. The diagram below presents, see Figure 2 a diagnostic algorithm that can be used when co-infection in Lyme disease is suspected.
Standard therapy for LB includes doxycycline, ceftriaxone, or amoxicillin, which are also effective against Rickettsia spp., An. phagocytophilum, Ehrlichia spp., and N. ehrlichia [58]. However, this regimen does not cover Babesia spp. or viral infections. Management of viral infections requires supportive, pathogenetic treatment. Babesiosis necessitates the use of antiparasitic agents: in mild cases, a combination of atovaquone and azithromycin is preferred, whereas in more severe cases, a combination of clindamycin and quinine may be used [20,59]; see Table 2.
To optimize the choice of antimicrobial therapy, randomized clinical trials are needed to evaluate the effects of different antimicrobial combinations in various co-infections. In addition, both in vitro and in vivo studies are required.
Diagnostic approach in patients with a history of tick bites.
Prevention of tick-borne diseases remains one of the most important measures for addressing this public health problem. There are various approaches to tackling it, including controlling tick populations through ecological, biological, and chemical methods [7]. The literature also describes the development of anti-tick vaccines that can prevent pathogen transmission [7,113],. Another strategy is the use of human monoclonal antibodies, which in experimental mouse models have shown both protective and therapeutic effects against TBEV [114] and Powassan virus [115]. Similar results have been obtained by Schaible et al. [116], who demonstrated that passive immunization of mouse models with human monoclonal antibodies against OspA protects against Bb infection.
TBEV is one of the few tick-borne pathogens for which there are licensed vaccines with proven efficacy. There are still no approved vaccines against Lyme disease, but several candidates are currently in clinical trials [7].
5. Conclusions
Ixodes ticks are the primary vectors of Lyme disease, but they can carry multiple pathogens, meaning that their bites carry the risk of transmitting more than one pathogen. These pathogens have overlapping clinical presentations, add new symptoms, or prolong the course of Lyme disease. For some of the pathogens we present (Rickettsia spp. and Bo. miyamotoi), the acute phase is more severe, which can delay the diagnosis of Lyme disease. Viral infections affecting the CNS are associated with more frequent and more severe neurological complications, while other co-pathogens (Babesia spp.) may prolong and exacerbate the symptoms of Lyme disease (LD). Despite the data presented in the literature, there are still no unified protocols for the diagnosis and treatment of co-infections in Lyme disease, and large clinical and experimental studies are needed to assess the burden of these diseases, as well as the implementation of new methods or combinations of diagnostic approaches for their detection. Patients with Lyme disease should be asked in detail about where and when they may have encountered an Ixodes tick, and clinicians should be familiar with the geographical distribution of Ixodes-borne diseases. Newer molecular methods for pathogen detection should be implemented in clinical practice, and clinicians should be aware of the characteristic clinical and laboratory abnormalities that may indicate co-exposure to more than one pathogen
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lane R.S. Piesman J. Burgdorfer W. Lyme borreliosis: Relation of its causative agent to its vectors and hosts in North America and Europe Annu. Rev. Entomol.19913658760910.1146/annurev.en.36.010191.0031032006870 · doi ↗ · pubmed ↗
- 2Hartemink N. Takken W. Trends in tick population dynamics and pathogen transmission in emerging tick-borne pathogens in Europe: An introduction Exp. Appl. Acarol.20166826927810.1007/s 10493-015-0003-426782278 · doi ↗ · pubmed ↗
- 3Goodman J.L. Dennis D.T. Sonenshine D.E. Tick-Borne Diseases of Humans ASM Press Washington, DC, USA 2005401 p
- 4Ji Z. Jian M. Yue P. Cao W. Xu X. Zhang Y. Pan Y. Yang J. Chen J. Liu M. Prevalence of Borrelia burgdorferi in Ixodidae Tick around Asia: A Systematic Review and Meta-Analysis Pathogens 20221114310.3390/pathogens 1102014335215089 PMC 8879681 · doi ↗ · pubmed ↗
- 5Pritt B.S. Mead P.S. Johnson D.K.H. Neitzel D.F. Respicio-Kingry L.B. Davis J.P. Schiffman E. Sloan L.M. Schriefer M.E. Replogle A.J. Identification of a novel pathogenic Borrelia species causing Lyme borreliosis with unusually high spirochaetaemia: A descriptive study Lancet Infect. Dis.201616556564 Erratum in Lancet Infect Dis. 2016, 16, 63610.1016/S 1473-3099(15)00464-826856777 PMC 4975683 · doi ↗ · pubmed ↗
- 6Johnson T.L. Graham C.B. Hojgaard A. Breuner N.E. Maes S.E. Boegler K.A. Replogle A.J. Kingry L.C. Petersen J.M. Eisen L. Isolation of the Lyme Disease Spirochete Borrelia mayonii from Naturally Infected Rodents in Minnesota J. Med. Entomol.2017541088109210.1093/jme/tjx 06228444198 PMC 5664935 · doi ↗ · pubmed ↗
- 7Nepveu-Traversy M.-E. Fausther-Bovendo H. Babuadze G. Human Tick-Borne Diseases and Advances in Anti-Tick Vaccine Approaches: A Comprehensive Review Vaccines 20241214110.3390/vaccines 1202014138400125 PMC 10891567 · doi ↗ · pubmed ↗
- 8Koczwarska J. Polaczyk J. Wieczorek W. Zdzienicka O. Żórańska J. Pawełczyk A. Welc-Falęciak R. Coexistence of Borrelia spp. with different tick-borne pathogens in Ixodes ricinus ticks removed from humans in Poland Sci. Rep.2025152168410.1038/s 41598-025-05885-240596119 PMC 12216539 · doi ↗ · pubmed ↗