Viral Spectrum of Herpetic Keratitis: A 15-Year Retrospective Analysis from Switzerland
Muntadher Al Karam, Sadiq Said, Anahita Bajka, Irene Voellmy, Michael Huber, Sandrine A. Zweifel, Daniel Barthelmes, Frank Blaser

TL;DR
This study analyzed 15 years of data to determine which viruses cause herpetic keratitis in Switzerland, finding that HSV-1 is the most common cause.
Contribution
The study provides a detailed epidemiological profile of herpetic keratitis in a tertiary care center using triplet PCR testing.
Findings
HSV-1 was the most frequent cause of herpetic keratitis (65.4% of positive cases), followed by VZV and HSV-2.
HSV-1 keratitis occurred more frequently in men compared to women.
Co-infections with Acanthamoeba and fungi were detected in some cases.
Abstract
To evaluate the epidemiology of herpetic keratitis over a 15-year period at a tertiary care center in Switzerland, focusing on the relative incidence of herpes simplex virus (HSV)-1, HSV-2, and varicella zoster virus (VZV), gender distribution, and co-infections, we conducted a retrospective single-center analysis of polymerase chain reaction (PCR) assays from corneal and conjunctival scrapings of suspected herpetic keratitis at a tertiary referral hospital. Patient demographics, viral spectra, and microbiological co-infections were assessed. Between 2010 and 2025, we identified 9954 PCR assays from 2892 patients, with 482 samples testing positive for herpesvirus. HSV-1 was the most frequent pathogen (328 of 3358, 9.8%), followed by VZV (143 of 3112, 4.6%), HSV-2 (9 of 3290, 0.27%), and CMV (2 of 194, 1.0%). Triplet testing (simultaneous HSV-1, HSV-2, and VZV-PCR) enabled direct…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
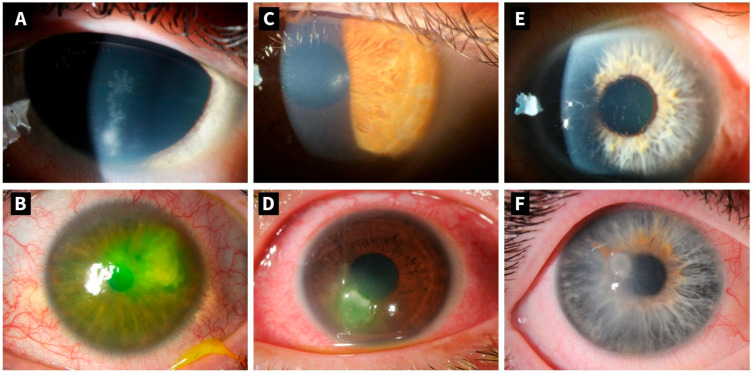 Figure 1
Figure 1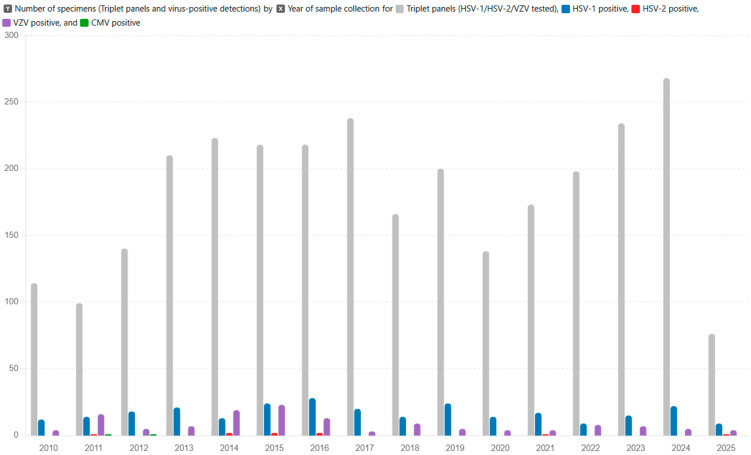 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHerpesvirus Infections and Treatments · Ocular Infections and Treatments · Ocular Diseases and Behçet’s Syndrome
1. Introduction
Herpetic corneal infections constitute a leading cause of infectious keratitis and corneal blindness worldwide [1,2]. The primary causative viruses include herpes simplex virus types 1 and 2 (HSV-1 and HSV-2), varicella zoster virus (VZV), and cytomegalovirus (CMV). Among these, HSV keratitis, predominantly due to HSV-1, is the most prevalent, and is recognized as the most common cause of infectious corneal blindness in developed countries [3]. Approximately one in five individuals with ocular HSV infection develops stromal herpes simplex keratitis, carrying a high risk of visual impairment [4]. Globally, the incidence of herpes keratitis is estimated at approximately 24 per 100,000 people per year, resulting in roughly 1.7 million new infections annually and causing substantial ocular morbidity, including vision loss due to recurrent disease and corneal scarring [5,6,7].
Diagnostic methods for herpes keratitis include clinical examination using slit-lamp biomicroscopy, polymerase chain reaction (PCR) assays, viral culture, immunofluorescence staining, and confocal microscopy [8]. PCR testing is the gold standard of invasive procedures due to its high sensitivity and specificity, enabling rapid and precise identification of the causative virus [9]. Moreover, it is critical to distinguish herpes keratitis from other infectious causes, such as bacteria, fungi, or parasites, especially acanthamoeba. Herpes keratitis may be grouped clinically into epithelial, stromal, endothelial, or neurotrophic keratitis. The epithelial affection typically manifests with dendritic lesions visible through slit-lamp biomicroscopy. In contrast, stromal keratitis is characterized by corneal stromal inflammation, stromal opacities, edema or ulceration, and potential subsequent stromal scarring [9,10]. Figure 1 shows clinical manifestations of herpetic keratitis caused by HSV-1, HSV-2, and VZV. Endothelial herpetic keratitis presents with disciform stromal edema, keratic precipitates (usually localized in the area of the edema), anterior chamber reaction, and usually absent epithelial defect (in contrast to epithelial keratitis). As a varicella-zoster of all herpetic corneal infections, neurotrophic keratitis may occur, resulting in impaired corneal sensation and persistent epithelial defects [11,12].
The overlapping clinical features of herpes virus keratitis make it challenging to distinguish among the different entities solely on clinical examination. HSV epithelial keratitis typically presents true dendrites demonstrating central fluorescein uptake, whereas VZV pseudo-dendrites lack central ulceration and therefore do not stain centrally [13]. CMV keratitis is most often seen in immunocompromised patients or following organ transplantation [14]. Definitive diagnosis, however, relies on pathogen detection through corneal scrapings or anterior chamber paracentesis [14].
Despite advances in diagnostics and therapy, herpes keratitis remains a significant challenge owing to its recurrent nature, diverse clinical manifestations, and risk of severe visual morbidity. Our tertiary care center in Switzerland functions as a national referral center for atypical or severe keratitis, including herpes-related cases. This retrospective study assesses the incidence and patient characteristics of PCR-confirmed herpes keratitis at our institution and reviews the current literature.
2. Materials and Methods
This is an investigator-initiated, retrospective, single-center study conducted at the University Hospital Zurich in Switzerland. We identified patients diagnosed with PCR-positive herpes keratitis between January 2010 and March 2025. The leading ethics committee in Zurich waived our study protocol as it does not fall within the scope of the Human Research Act (BASEC number 2023-01146). Nevertheless, we handled all data according to Good Clinical Practice guidelines.
2.1. Data Collection
We reviewed our laboratory information system of patients regarding PCR-positive corneal or conjunctival scraping results for HSV-1, HSV-2, VZV, and CMV. We extracted the patients’ birth dates, gender, and date of positive results, inferring the patients’ age at the time of test positivity. To explore co-testing patterns and interrelationships, we identified all “triplet” tests in which a single specimen was assayed simultaneously for HSV-1, HSV-2 and VZV. Within this triplet cohort, we compared detection rates across the three viruses. Further, we investigated for Acanthamoeba and fungal co-infections, considering PCR and culture results. Bacterial co-infections were not assessed in this study, as they are presumably common, culture positivity in corneal scrapings is often due to probe contamination, and all infectious keratitis patients at our clinic receive empirical topical antibiotics before a definitive diagnosis. However, we routinely include bacterial investigations in all corneal scrapings in unclear, presumed-infectious keratitis.
2.2. Detection of CMV, HSV-1, HSV-2, and VZV
Sample preparation and DNA extraction: For microbiological diagnostics, corneal scrapings were used as the primary sampling method; conjunctival swabs were obtained only in exceptional cases, such as in pediatric patients or when patient cooperation was insufficient to safely perform corneal scraping. Corneal and conjunctival swabs were placed in 2 mL viral transport medium (VTM) immediately after collection. Before sample processing, specimens were vortexed, swabs removed, and the remaining VTM centrifuged at 2000 relative centrifugal force (rcf) for 10 min. DNA was extracted using easyMAG and EMAG^®^ nucleic acid extraction systems (bioMérieux, Marcy l’Etoile, France) according to the manufacturer’s protocol from 200 microliter (μL) supernatant and concentrated in 110 elution buffer (extraction buffer 3). From 28 August 2024, nucleic acid was extracted from 600, 400, or 300 μL supernatant, depending on the number of additional analyses requested, and concentrated in 60, 40, or 30 μL elution buffer (extraction buffer 3), respectively. In addition, all specimens were spiked with a standardized amount of Phocid herpes virus type 1 (PhHV) as PCR process control before extraction (European virus archive EVAG, Marseille, France, https://www.european-virus-archive.com) [15].
DNA amplification: DNA PCR amplifications were conducted following in-house real-time PCR protocols. All primers and Taqman probes were synthesized by Microsynth (Microsynth AG, Balgach, Switzerland). The PCR tests used in this study are validated diagnostic tests with high sensitivity and specificity. The assays are specific for the individual Herpesvirus species within the Simplexvirus genus or the Orthoherpesviridae family [15,16,17,18,19]. Sequences of all primers and probes are listed in Table 1.
Until 28 August 2024, a single-plex PCR process control using GAPDH (Homo sapiens glyceraldehyde-3-phosphate dehydrogenase) was run separately for HSV-1, HSV-2, and VZV PCR tests. For CMV, the GAPDH process control was run as a duplex assay with GAPDH primers and probe incorporated in the CMV-Mastermix. Each viral target assay was performed in duplicate to increase detection sensitivity. Mastermixes for HSV-1, HSV-2, VZV, and GAPDH PCR process controls were composed of 900 nM of each respective target primer and 200 nM of each respective target probe in 25 μL of TaqMan Universal MMIX II (Applied Biosystems by Thermo Fisher Scientific, Waltham, MA, USA) and 19 μL nuclease-free water (AppliChem GmbH, Darmstadt, Germany). CMV Mastermixes contained 900 nM of CMV primers, 100 nM of GAPDH primers, and 200 nM of CMV and GAPDH probe in 25 μL of TaqMan Universal MMIX II (Applied Biosystems) and 18.8 μL nuclease-free water (AppliChem GmbH) or, from 5 May 2023, 17.9 μL nuclease-free water. All RT-PCR amplifications were conducted in a total volume of 50 μL, containing 45 μL of Mastermix and 5 μL of eluted DNA.
From 28 August 2024, GAPDH process controls were replaced by the amplification of phocid herpes virus (PhHV) glycoprotein B in combination with spiking all clinical specimens with a standardized amount of PhHV. Each PCR assay was run in a duplex protocol, also containing primers and TaqMan probe for PhHV detection. Mastermixes from 28 August 2024 thus contained 780 nM of each respective diagnostic target primer, 50 nM of PhHV forward primer, 200 nM of PhHV reverse primer, 200 nM of respective diagnostic target probe and 100 nM of PhHV probe in 21.7 μL of TaqMan Universal MMIX (Applied Biosystems) and 17.3 μL nuclease-free water for HSV-1, HSV-2, and VZV or 16.5 μL nuclease-free water for CMV (AppliChem GmbH). All RT-PCR amplifications were conducted in a total volume of 50 μL, containing 40 μL of Mastermix and 10 μL of eluted DNA modifications of the new protocol (i.e., DNA extraction protocol leading to a 10-fold concentration of eluted DNA and doubling the volume of eluted DNA added to the PCR reaction mix) resulted in a 10-fold increase in sensitivity with potentially higher target detection rates. Thus, assay duplicates were eliminated. DNA amplifications were conducted in a QuantStudio™ 3 Real-Time PCR System (Applied Biosystems) under the following conditions: 2 min at 50 °C, 10 min at 95 °C and 50 cycles of 15 s at 95 °C, and 1 min at 60 °C. In each run, negative and positive controls were included. Elution buffer (NUCLISENS^®^ easyMAG^®^ Extraction Buffer 3, bioMérieux) was used as negative control and target-specific positive controls were all obtained from ATCC [ATCC, Manassas, VA, USA] as follows: CMV: purified viral DNA, ATCC VR-538, strain AD-169; HSV-1: purified viral DNA, ATCC VR-539, strain MacIntyre; HSV-2: purified viral DNA, ATCC VR-734, strain G; VZV: purified viral DNA, ATCC VR-586, strain Ellen. Signals reaching cycle thresholds of <38 were interpreted as positive; tests raising signals after ≥38 cycles were repeated and reported as positive if a signal was also detected in the repeated test. If assays were run in duplicates, tests were interpreted as positive, if at least one test result was positive. Signals of GAPDH or PhHV process controls were required before 33 cycles, i.e., the reaction showed no inhibition or reduction of DNA during extraction and PCR [16,17,18,19,20].
2.3. Statistical Analyses
In descriptive statistics, we present means with standard deviation and medians with interquartile ranges (IQR), or minimum to maximum values for continuous data and numbers and percentages for categorical data. To assess potential gender predominance, we tested whether the observed proportion of male positive results for each virus differed significantly from a neutral distribution of 50%. For each pathogen (HSV-1, HSV-2, VZV, and CMV), we performed a two-sided exact binomial test under the null hypothesis that the probability of a positive result being male was 0.5. To account for multiple comparisons across the four pathogens, we applied a Bonferroni correction, adjusting the significance threshold from α = 0.05 to α = 0.0125 (0.05 divided by 4). We considered a p-value statistically significant only if it was below the corrected threshold and the corresponding 95% confidence interval (CI) for the male proportion did not include 0.5. All statistical analyses were conducted using R version 4.2.1 (R Foundation for Statistical Computing, Vienna, Austria).
3. Results
From January 2010 to March 2025, we identified a total of 9954 herpesvirus PCR test results performed on corneal and conjunctival scrapings. Demographic information was available for 8693 individual test entries, corresponding to 2892 patients. Hence, all the following demographics were only conducted on the latter dataset. The median (IQR; range) patient age was 48.0 (31.7–66.3; 0–97) years, with a quasi-balanced gender distribution (49.7% female). In total, 3358 PCR tests were targeted for HSV-1, 3290 for HSV-2, 3112 for VZV, and 194 for CMV. Among these, 328 (9.8%) were positive for HSV-1, 9 (0.3%) for HSV-2, 143 (4.6%) for VZV, and 2 (1.0%) for CMV. Table 2 summarizes the patient demographics stratified by virus type.
We identified 2913 corneal-scraping specimens tested in triplets (i.e., simultaneous testing for HSV-1, HSV-2, and VZV), enabling direct comparisons of detection rates across these three viruses. Among the 419 positive results obtained within the triplet cohort, 274 (65.4%) were positive for HSV-1, 136 (32.5%) for VZV, and 9 (2.1%) for HSV-2. Table 3 displays detailed results of the triplet analyses. For each pathogen, we tested whether the proportion of male patients among positive cases differed from an equal distribution between males and females. Applying a two-sided exact binomial test, we found that 161 of 274 HSV-1 positive cases were male, corresponding to a male proportion of 58.9% (95% CI: 52.7–64.7%), with a p-value of 0.0044, indicating a statistically significantly higher incidence in men. For HSV-2, 3 of 9 positive cases were male (33.3%, 95% CI: 7.5–70.1%; p = 0.5078), for VZV, 65 of 136 were male (47.9%, 95% CI: 39.2–56.5%; p = 0.6683), and for CMV, 2 of 2 were male (100%, 95% CI: 15.8–100%; p = 0.5000), none of which differed significantly from equal distribution.
The use of multiplex PCR testing increased across the study period, reflecting the broader implementation of standardized triplet panels. In 2010, we performed 114 triplet assays, with the number of assays increasing yearly to a peak of 268 in 2024. Notably, there were two transient declines: from 238 assays in 2017 to 166 in 2018, and from 200 in 2019 to 138 in 2020. Despite the overall growth in testing volume, annual positivity rates remained relatively stable (HSV-1: 8–11%; VZV: 3–6%), whereas HSV-2 detections remained rare, with only nine positive triplet assays identified in six separate years (2011, 2014–2016, 2021, and 2025). Table 4 and Figure 2 provide a detailed analysis of the temporal triplet testing patterns.
Demographically, the triplet cohort closely mirrored the overall tested population, with no significant differences in age or gender proportions compared to the full assay set. HSV-2 detections remained rare, with nine unique patients tested positive for HSV-2 keratitis; one patient had two positive results within 10 days, yielding a total of 10 positive assays. The median (IQR) age of HSV-2 positive patients was 57.2 (46.7–66.4) years, and 66.7% were female. Furthermore, we identified eight cases of simultaneous HSV-1 and VZV co-infections, of whom two (25.0%) were female, ranging in age from 16 to 70 years. Clinical documentation reported six epithelial presentations and two corneal ulcers. In addition, two patients presented with simultaneous bilateral viral detections: a 29-year-old male with bilateral HSV-1 infection and a 74-year-old male with bilateral VZV infection.
Regarding other microbiological co-infections, two (0.6%) patients with HSV-1 and one (0.7%) with VZV-positivity had concurrent Acanthamoeba infection. Neither of the HSV-1-positive cases wore contact lenses, whereas the VZV-positive case wore soft daily contact lenses. Furthermore, 15 (3.2%) patients showed positive fungal detections. Of these, 11 (73.3%) were positive for HSV-1, none were positive for HSV-2, and 4 (26.7%) were positive for VZV. Regarding contact lens use, 8 of 11 (72.7%) HSV-1-positive and 3 of 4 (75.0%) VZV-positive patients used contact lenses.
4. Discussion
This retrospective study investigated PCR test results regarding possible herpetic keratitis at our tertiary care center in Switzerland. Between January 2010 and March 2025, we identified 9954 PCR tests, obtained from 2892 patients. Over the 15-year interval, the laboratory’s adoption of multiplex triplet panels (HSV-1, HSV-2, VZV) increased markedly—from 114 triplet panels in 2010 to a peak of 268 in 2024—reflecting broader clinical uptake of PCR diagnostics for suspected viral keratitis. These trends underscore the increasing reliance on comprehensive PCR diagnostics in cases of suspected viral keratitis. We found 9.8% and 4.6% positivity for HSV-1 and VZV, respectively, whereby HSV-2 and CMV occurred much less frequently. Despite this expansion in testing throughput, the annual proportion of positive triplet results for HSV-1 and VZV remained relatively constant (HSV-1 around 8–11%; VZV around 3–6%), which supports a stable clinical threshold for testing and the epidemiological dominance of these viruses in corneal disease.
HSV-1 was the overwhelmingly predominant pathogen in our dataset, which aligns with global epidemiology. Worldwide, HSV-1 is the leading cause of herpetic keratitis, with pooled incidence estimates of 24 per 100,000 people per year, most cases affecting the corneal epithelium [3,20,21]. Its predominance is attributable to the high prevalence of latent HSV-1 infection within the trigeminal ganglion and the lifelong risk of recurrent corneal reactivation. VZV was the second-most frequent pathogen in our cohort, which is also consistent with international data: although VZV accounts for only a minority of herpetic keratitis cases (3–12%), it remains an important cause of ocular morbidity due to its association with herpes zoster ophthalmicus [14]. By contrast, HSV-2 was rarely detected (<1%), aligning with previous European and global studies [22,23,24,25]. HSV-2 keratitis most often occurs through neonatal transmission or in immunocompromised patients, and is therefore uncommon in otherwise healthy adults [20,22,25]. Although cases of CMV epitheliitis and CMV stromal keratitis have been reported, CMV endotheliitis is the most common manifestation of corneal infection [26].
In our tertiary care center, we routinely perform multiplex PCR triplet testing, as the clinical presentation of herpetic keratitis does not allow reliable differentiation of the causative virus. In addition, initial therapy differs: current consensus recommends valaciclovir 500 mg three times daily for HSV-1 stromal keratitis, whereas VZV stromal keratitis requires 1 g three times daily [11,12].
Triplet testing in our cohort enabled a direct comparison of the relative incidence rates, with HSV-1 identified in 65.4% of positive assays, VZV in 32.5%, and HSV-2 in 2.2%. Previous studies limited to corneal specimens reported substantially higher proportions of HSV-1 (89%) compared to VZV (11%) [27]. By contrast, investigations including a broader range of ocular samples—such as conjunctival swabs, corneal scrapings, aqueous humour, and vitreous samples—demonstrated a more balanced distribution, with VZV slightly exceeding HSV-1 (12.3% versus 11.7%) [22]. These differences suggest potential tissue tropism: HSV-1 appears to have a predilection for the corneal epithelium and stroma, whereas VZV may more frequently involve multiple ocular structures beyond the cornea. The distribution in our study likely reflects the inclusion of both corneal and conjunctival scrapings, which may have increased the relative detection of VZV while proportionally reducing the apparent dominance of HSV-1 compared to studies analyzing only corneal tissue.
In this study, we observed two transient reductions in triplet testing throughout the observation period. The first decline occurred between 2017 and 2018 (from 238 to 166 triplets) and the second between 2019 and 2020 (from 200 to 138 triplets). The latter coincides with the onset of the COVID-19 pandemic and is plausibly explained by reduced outpatient activity and fewer elective procedures, resulting in fewer samplings. In contrast, the 2018 decline is less clearly attributable to a single external factor and may reflect local workflow adjustments or changes in referral patterns. These year-to-year perturbations highlight the importance of interpreting temporal trends in the context of operational and public health influences, rather than attributing them solely to epidemiologic fluctuations.
Identifying co-infections in patients with herpes keratitis is of crucial clinical importance as they may influence management and final visual outcomes. In our study, we identified cases of Acanthamoeba or fungal co-infection in patients with PCR-confirmed herpes keratitis, consistent with prior reports describing the coexistence or clinicopathologic overlap among Acanthamoeba, fungal, and herpetic keratitis [28,29]. The coexistence of amoeba and herpes may be due to a chance of dual infection or to a symbiosis in which one pathogen masks the other. Overall, contact lens use and ocular trauma remain the primary risk factors for infectious keratitis, which may explain the potential for co-infections [30]. These results emphasize the importance of comprehensive microbiological evaluations in atypical keratitis cases.
We found a statistically significant higher incidence in men in HSV-1-associated keratitis, a gender-associated observation that is difficult to explain and highlights an existing research gap regarding the underlying pathophysiology. The possible reasons for sex-related differences in the incidence of herpetic keratitis are multifactorial and remain incompletely understood. While male predominance has been reported in several studies, the extent and statistical significance of this finding vary across populations and study designs [31,32]. Conversely, not all studies show this pattern, and some pediatric cohorts have even reported a predominance of female HSV-1 infections [33]. Biological factors, such as sex hormone differences and differences in immune response, may contribute. Animal models have shown that male mice can have higher mortality and more severe disease following HSV-1 ocular infection, potentially due to androgen effects and gender-specific modulation of interferon pathways [34,35]. However, such findings have not been consistently replicated in human populations. Sociodemographic and behavioral factors may also play a role. For example, differences in occupational exposure, healthcare-seeking behavior, and risk of corneal trauma could influence gender distribution in certain cohorts [36,37]. Geographic and cultural factors, as well as comorbidities such as diabetes and immunosuppression, may further modulate risk but do not reveal a clear gender predilection [33,36,38]. Taken together, these findings underscore that the true mechanisms driving gender differences in HSV-1 keratitis remain poorly defined and warrant further investigation.
This study’s key strengths include a 15-year observation period and a large data sample of nearly 10,000 PCR assays. Furthermore, the standardized triplet testing of HSV-1, HSV-2, and VZV on the same specimen, along with transparent laboratory methods and internal controls, enables robust within-sample comparisons and temporal descriptions. However, this study has several limitations. First, the retrospective design is inherently prone to selection bias and missing data. The single-center design may introduce referral and sampling biases, potentially leading our study cohort to not accurately reflect other populations and testing practices. Further, incomplete demographic data may affect the accuracy of incidence estimates. Moreover, the mid-study laboratory changes complicate longitudinal comparisons of positivity rates. Last, the rarity of HSV-2 and CMV limits the precision of incidence for those subgroups.
5. Conclusions
To conclude, over a 15-year period at our Swiss tertiary care center, HSV-1 emerged as the most common cause of PCR-confirmed herpetic keratitis. This was followed by VZV, whereas HSV-2 and CMV were rarely detected. We advocate for triplet testing panels not only for a more complete and efficient laboratory assessment, but also for epidemiologic monitoring reasons that allow for investigating relative prevalence data. The statistically significant higher incidence of HSV-1 in men underscores a research gap in understanding the sex-specific pathophysiology of herpetic keratitis, emphasizing the need for future biological and sociodemographic studies to investigate the underlying mechanisms.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Watson S. Cabrera-Aguas M. Khoo P. Common Eye Infections Aust. Prescr.201841677210.18773/austprescr.2018.01629922000 PMC 6003010 · doi ↗ · pubmed ↗
- 2Guess S. Stone D.U. Chodosh J. Evidence-Based Treatment of Herpes Simplex Virus Keratitis: A Systematic Review Ocul. Surf.2007524025010.1016/S 1542-0124(12)70614-617660897 · doi ↗ · pubmed ↗
- 3Farooq A.V. Shukla D. Herpes Simplex Epithelial and Stromal Keratitis: An Epidemiologic Update Surv. Ophthalmol.20125744846210.1016/j.survophthal.2012.01.00522542912 PMC 3652623 · doi ↗ · pubmed ↗
- 4Cabrera-Aguas M. Robaei D. Mc Cluskey P. Watson S. Clinical Translation of Recommendations from Randomized Trials for Management of Herpes Simplex Virus Keratitis Clin. Exp. Ophthalmol.2018461008101610.1111/ceo.1331929749113 · doi ↗ · pubmed ↗
- 5Farooq A.V. Shah A. Shukla D. The Role of Herpesviruses in Ocular Infections Virus Adapt. Treat.2010211512310.2147/vaat.s 9500 · doi ↗
- 6Ung L. Rajaiya J. Chodosh J. Viral Conjunctivitis Infections of the Cornea and Conjunctiva Springer Singapore 2021175010.1007/978-981-15-8811-2_2 · doi ↗
- 7Young R.C. Hodge D.O. Liesegang T.J. Baratz K.H. Incidence, Recurrence, and Outcomes of Herpes Simplex Virus Eye Disease in Olmsted County, Minnesota, 1976–2007: The Effect of Oral Antiviral Prophylaxis Arch. Ophthalmol.20101281178118310.1001/archophthalmol.2010.18720837803 PMC 3103769 · doi ↗ · pubmed ↗
- 8Cabrera-Aguas M. Watson S.L. Updates in Diagnostic Imaging for Infectious Keratitis: A Review Diagnostics 202313335810.3390/diagnostics 1321335837958254 PMC 10647798 · doi ↗ · pubmed ↗