Nasopharyngeal Swabs for Orientia tsutsugamushi Detection in Doxycycline Treatment: A Prospective Cohort Study in Hainan, China
Yuanze Chen, Siqi Chen, Jiajia An, Xiaojing Zheng, Qi Wang, Yuyan Wang, Wenjing Fu, Biao Wu, Yongguo Du, Feifei Yin, Liyuan Zhang

TL;DR
Nasopharyngeal swabs can detect scrub typhus bacteria shortly after starting doxycycline treatment, offering a noninvasive option for follow-up when blood testing becomes less reliable.
Contribution
Nasopharyngeal swabs are proposed as a supplementary noninvasive specimen for short-term follow-up of scrub typhus during doxycycline treatment.
Findings
Before treatment, 75% of blood samples and 25% of nasopharyngeal swabs tested positive for O. tsutsugamushi DNA.
At 24 hours after doxycycline, blood samples were all negative, but 15% of nasopharyngeal swabs remained positive.
Nasopharyngeal swab positives showed high genetic homology with blood samples, suggesting consistent strain detection.
Abstract
Scrub typhus, caused by Orientia tsutsugamushi, remains a neglected cause of acute febrile illness. Molecular testing of blood supports early diagnosis, yet once doxycycline is started, blood qPCR positivity can drop rapidly, complicating short-term follow-up and relapse surveillance. We compared detection across multiple clinical specimens and evaluated nasopharyngeal swabs (NPSs) as noninvasive supplementary specimens during treatment initiation. In a prospective single-center cohort from Hainan, China, we enrolled 20 patients with scrub typhus. Blood, NPS, urine, and stool were collected before doxycycline administration 24 h after the first dose and on day 5. qPCR was performed for the analysis of Orientia tsutsugamushi. qPCR-positive specimens were subjected to nested PCR targeting TSA56, and nested PCR-positive amplicons were Sanger sequenced for genotyping. Before treatment, O.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
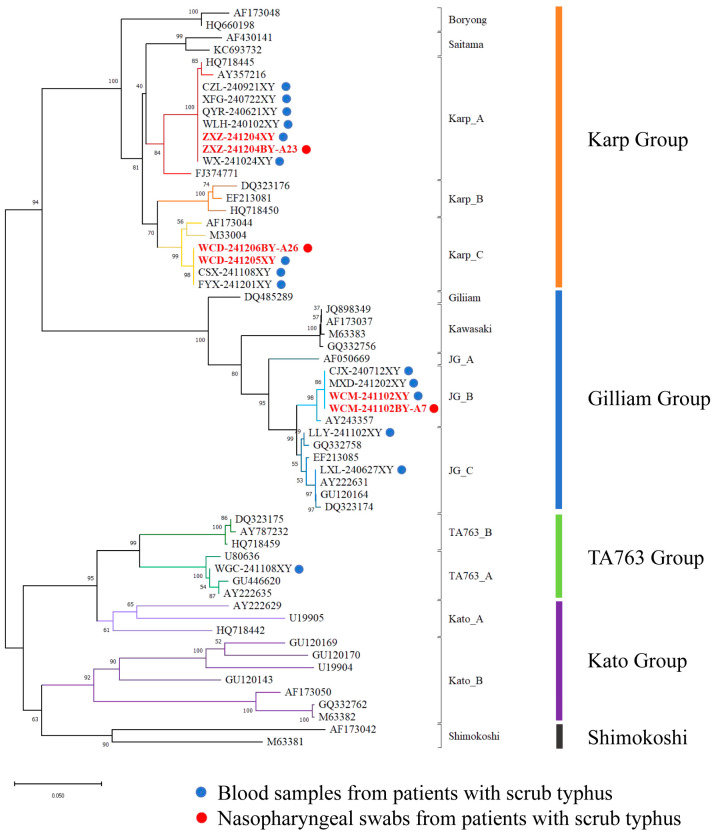 Figure 1
Figure 1- —Hainan Provincial Natural Science Foundation of China
- —Key Research and Development Plan of Hainan Province
- —Hainan Provincial International Science and Technology Cooperation Research and Development Project
- —National Natural Science Foundation of China
- —Guangzhou National Laboratory
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVector-borne infectious diseases · Complement system in diseases · Leprosy Research and Treatment
1. Introduction
Scrub typhus, also known as tsutsugamushi disease, is an acute natural focal infectious disease caused by Orientia tsutsugamushi (O. tsutsugamushi (OT)) and transmitted to humans by the bites of infected chigger mites. The annual incidence in the Asia–Pacific region is approximately 1 million cases, and the fatality rate of untreated cases can reach 30% [1,2]. Its distribution spans from Japan in the east, Pakistan in the west, Russia in the north, and Australia in the south, in a region known as the “Tsutsugamushi Triangle” [3]. However, in recent years, its geographic range has expanded, posing a growing public health concern [3,4,5,6].
OT is an obligate intracellular pathogen. In 2002, after OT was first detected in eschar in Japan [7], PCR testing has been primarily used for blood and eschar samples and its detection results can aid in disease diagnosis. However, the detection rate in blood samples is strongly affected by antimicrobial agents. At 12–24 h after doxycycline administration, pathogen nucleic acid in blood rapidly becomes undetectable, which poses significant challenges for efficacy evaluation, relapse monitoring, and epidemiological investigations.
The study of the pathophysiology of tsutsugamushi has indicated that OT may be extensively distributed in the human body. The nasopharynx is an accessible mucosal surface involved in the early interaction of many pathogens with the host; therefore, nasopharyngeal swabs (NPSs) may provide noninvasive supplementary specimens for OT detection, particularly during treatment initiation. In this prospective cohort, 20 scrub typhus patients were enrolled at the Second Affiliated Hospital of Hainan Medical University between June 2024 and June 2025. O. tsutsugamushi detection in blood, NPS, urine, and stool was compared before doxycycline, 24 h after the first dose, and on day 5. TSA56 genotyping and phylogenetic analysis were performed on positive samples to characterize detected strains and to evaluate the feasibility of NPS for short-term follow-up after doxycycline.
2. Materials and Methods
2.1. Ethics Committee
This prospective cohort study was approved by the Ethics Committee of the Second Affiliated Hospital of Hainan Medical University. Ethical approval was granted under the reference number LW-2022-033 (approved on 31 March 2022) and remained valid through the committee’s required annual continuing review. Written informed consent to participate in this study was obtained from all the patients.
2.2. Study Population, Diagnostic Criteria, and Data Collection
Clinical samples and clinical data of patients diagnosed with scrub typhus at the Second Affiliated Hospital of Hainan Medical University between June 2024 and June 2025 were collected. The classification for suspected, clinically diagnosed, and confirmed cases was based on the Expert consensus on clinical diagnosis and treatment of scrub typhus (2024 edition) [8]. A summary of the case definitions is available in Supplementary Materials S1 Text. All patients enrolled in this study were confirmed cases.
For all enrolled patients, a comprehensive dataset was compiled, including general demographic and clinical information (sex, age, initial symptoms, prior antibiotic use, complications, comorbidities, and underlying diseases), results of routine laboratory tests (complete blood count, liver and kidney function panels, and coagulation function assays), and findings from imaging examinations (chest computed tomography (CT) and abdominal color Doppler ultrasound).
2.3. Sample Collection
For all scrub typhus patients, blood, urine, stool, and NPS specimens were obtained at three key time points: pre-doxycycline (at admission), 24 h after the first doxycycline dose, and on day 5 of doxycycline therapy. To ensure sample quality, blood, urine, stool, and NPS samples were stored at 4 °C and transported to the laboratory in a sealed refrigerated transport box (2–8 °C). Nucleic acid extraction was initiated immediately upon arrival and completed within 48 h of collection.
2.4. Sample Processing and DNA Extraction
DNA was extracted from whole blood, nasopharyngeal swabs (NPSs), urine, and stool using an automated nucleic acid extraction system with the CS-B200 extraction kit (Zybio Inc., Chongqing, China), following the manufacturer’s standardized procedures for complex clinical specimens, including respiratory matrices. Whole blood was collected into EDTA anticoagulant tubes and aliquoted prior to nucleic acid extraction.
Pre-analytical processing was performed as follows: (i) whole blood: 200 μL, was directly processed for extraction; (ii) NPS: swabs were placed in a specimen preservation medium and 1 mL of the medium was centrifuged at high speed; the supernatant was discarded, the pellet was resuspended, and 200 μL of the resuspended pellet was used for extraction; (iii) urine: specimens were centrifuged at high speed and 200 μL of the resuspended pellet was used for extraction; (iv) stool: specimens were suspended in normal saline, vigorously vortexed, and 200 μL of the homogenized suspension was used for extraction. DNA was eluted in a final volume of 60 μL.
2.5. PCR Detection and Sequence Analysis of Orientia tsutsugamushi
A real-time fluorescent quantitative PCR (qPCR) assay and a nested PCR protocol were implemented based on the 56-kDa type-specific antigen gene (TSA56) of O. tsutsugamushi. Primer/probe design was guided by representative TSA56 sequences (GenBank accession nos. AY357216, AF050669, AY222631, AY222635, and M33004) and previous publications. A two-step molecular workflow was used for screening and genotyping.
First, DNA extracts were screened using an O. tsutsugamushi Nucleic Acid Detection Kit (Zybio Inc., Chongqing, China) targeting species-specific loci, including the 47-kDa, 56-kDa, and groEL genes; commercial quality control materials supplied for the assay were used as the negative and positive controls and testing was performed according to the manufacturer’s instructions. All samples were tested in replicate reactions. A sample was considered OT positive when all three target loci showed typical amplification curves with Ct < 40 in the replicate reactions and the internal/process control met the predefined acceptance criteria. Borderline (near-threshold) or discordant results between replicates were retested. Second, TSA56 was measured separately for quantitative detection of O. tsutsugamushi using a singleplex TaqMan qPCR assay (TaKaRa Bio Inc., Otsu, Shiga, Japan). A recombinant plasmid containing a TSA56 gene fragment served as the positive control and quantification standard. The TSA56 primers and hydrolysis probe were: forward 5′-TGATAAGGATATTAAAGGGCATA-3′, reverse 5′-ATACACCCTCAGCAGCATTAAT-3′, and probe 5′-(FAM)-ATGGTTGCATCAGGAGCACTTGG-(BHQ1)-3′.
The nested PCR targeting TSA56 was performed to generate an expected 483 bp amplicon. The first-round PCR used forward 5′-TCAAGCTTATTGCTAGTGCAATGTCTGC-3′ and reverse 5′-AGGGATCCCTGCTGCTGTGCTTGCTGCG-3′. The second-round PCR used forward 5′-GATCAAGCTTCCTCAGCCTACTATAATGCC-3′ and reverse 5′-CTAGGGATCCCGACAGATGCACTATTAGGC-3′. Nucleic acid extracted from an O. tsutsugamushi-positive clinical specimen was included as the positive control, and a no-template control was included in each run to monitor potential contamination. Amplicons were purified and subjected to bidirectional Sanger sequencing for downstream phylogenetic analyses. Nested PCR amplicons were purified and submitted to Sangon Biotech (Shanghai, China) for bidirectional Sanger sequencing on an ABI 3730xl DNA Analyzer (Applied Biosystems, Foster City, CA, USA). Forward and reverse reads from the same specimen were assembled and manually checked using SeqMan (DNASTAR Lasergene v18.1.1; Madison, WI, USA) to generate a confirmed consensus sequence for downstream analyses. The obtained sequences were deposited in GenBank (accession nos. PX714883–PX714900). Closest matches were identified by BLAST v2.17.0 (National Center for Biotechnology Information, Bethesda, MD, USA) against the NCBI database, and alignments were generated using CLUSTALX v2.1 (European Bioinformatics Institute, Hinxton, UK) with the closest related and representative global reference sequences. Phylogenetic trees were reconstructed using the neighbor-joining method with 1000 bootstrap replicates.
2.6. Data Analysis
R4.2.2 software was used for statistical analysis. Measurement data that conformed to a normal distribution were analyzed using the independent sample t test and are described as ( ± SD). The Mann–Whitney U-rank sum test was used, and the median and interquartile range [M (Q1, Q3)] were used to describe the data. Count data are expressed as the number of cases or percentage.
3. Results
3.1. General Information
The 20 patients included 12 males and 8 females, aged 58.00 ± 10.31 years. Five patients had a clear history of field activities. Among the 14 patients who sought medical care after symptom onset, visits were made to secondary medical institutions (namely, seven Class II Grade A hospitals, three community hospitals, and four local clinics), but none received a definitive diagnosis. All the patients were admitted to the hospital with fever as the first symptom. After admission, they were given doxycycline for infection control, an antipyretic, supplemental oxygen, and supportive therapy for liver and kidney protection. The general information is shown in Table 1.
3.2. Analysis of Clinical Characteristics
All patients (100%) presented with fever as the first symptom, and the median duration of fever was 7 (5, 8.50) days. The main concomitant symptoms included dizziness, headache (13 cases; 65%), and chills (11 cases; 55%). Laboratory tests revealed abnormal liver and kidney function, changes in white blood cell and platelet counts, and abnormal coagulation. Some patients presented multisystem involvement, combination with underlying diseases, and multiple pathogen infections.
During physical examination, five patients (25%) presented with characteristic eschar, and the distribution locations included the axilla (three patients), groin (one patient), and scrotum (one patient). Four patients (20%) presented with splenomegaly, and one patient presented with a systemic rash (5%). Chest CT imaging examination revealed that 12 patients (60%) presented multiple inflammatory/exudative lesions in both lungs. Among these, three patients (15%) had small amounts of pleural effusion. Additionally, lymphadenopathy, predominantly in the axillary region, was found in three patients (15%). Moreover, three cases (15%) were associated with central nervous system abnormalities (such as lacunar infarction), and two patients (10%) had cardiovascular abnormalities (all with newly developed atrial premature beats, Table 1).
3.3. Laboratory Test Results
A total of 60 blood samples, 60 NPS samples, 60 urine samples, and 20 stool samples were collected from 20 patients with scrub typhus at different time points (Table 2). Because bowel habits vary among patients and are influenced by illness and food intake, collecting stool specimens at every scheduled time point was not feasible; therefore, stool was collected only at the first bowel movement after admission for each patient. All samples were first screened by qPCR. qPCR-positive samples were then tested by nested PCR targeting the 56-kDa TSA gene, and Sanger sequencing was performed for nested PCR-positive amplicons.
Among the 20 scrub typhus patients, 15/20 (75.00%) blood specimens before doxycycline were positive by qPCR, but all negative at 24 h after treatment and 5 days. A total of 5/20 (25.00%) NPS samples before doxycycline were positive, versus 3 positive samples at 24 h after treatment (3/20, 15.00%). All qPCR-positive reactions of NPS samples showed typical amplification curves with Ct values < 40, meeting the predefined positivity criteria (Table 3). In total, 15 whole-blood specimens yielded definitive nested PCR amplicons and were successfully sequenced, generating 15 TSA56 sequences. For NPS, 8 specimens yielded definitive nested PCR and only 3 NPS specimens produced sequenceable amplicons, generating 3 TSA56 sequences. All urine (n = 60) and stool (n = 20) specimens were negative by qPCR (Table 2).
Genetic analysis based on TSA56 gene sequences obtained from the 18 nested PCR-positive specimens identified three genotypes, namely Karp, Gilliam, and TA763 (Figure 1). Among these 18 positive specimens, paired whole-blood and nasopharyngeal swab (NPS) specimens from three patients were simultaneously positive (six specimens in total) (Table 4). Phylogenetic reconstruction showed that these six sequences clustered into well-supported genotype clades defined by GenBank reference strains, specifically the Karp_A, Karp_C, and the Gilliam-related JG_B clusters; moreover, for each of these three patients, the paired blood and NPS sequences were identical at the nucleotide level (100% identity).
The tree was constructed using TSA56 sequences generated in this study together with representative reference sequences retrieved from GenBank. All reference sequences are listed in Supplementary Table S1. Branch colors indicate distinct genotypes (annotated on the right), with major lineages including Karp, Gilliam, TA763, Kato, and Shimokoshi. Blue dots denote sequences from 15 OT PCR-positive blood samples, and red dots denote sequences from 3 OT PCR-positive nasopharyngeal swabs. Sample IDs in bold red indicate dual-site positivity (OT detected in both blood and nasopharyngeal swab specimens). Numbers at nodes represent bootstrap support values, and the scale bar indicates nucleotide substitutions per site.
4. Discussion
This study is the first report on positive nasopharyngeal swabs in OT-infected patients with scrub typhus in Hainan Province. The results of this study are important with regards to the comprehensive testing of multiple samples of stool, urine, blood and nasopharyngeal swabs from clinically diagnosed patients. Using real-time PCR and nested PCR, we successfully detected the nucleic acid of OT in nasopharyngeal swab samples from some patients. Although the positive rate was low, the 100% nucleotide level between the gene sequencing results suggested that the nasopharynx might be a site of transient colonization by OT. These findings challenge the traditional view that OT is limited to the blood or eschar and provide a new perspective for understanding the distribution of OT in the host after infection. Consistent with the findings of previous studies, the Karp genotype was dominant in this region [9,10]. Its biological characteristics may affect the distribution of pathogens in different host tissues. The positive nasopharyngeal swab samples were all prior to antibiotic treatment, and the CT values of the samples after treatment significantly increased, suggesting that antibiotic treatment may reduce the sensitivity of PCR detection by reducing the OT load, which is consistent with previous studies demonstrating the established efficacy of doxycycline against scrub typhus [11,12].
The nasopharynx is the primary interface between the respiratory tract and the outside world. The submucosa, which is rich in macrophages and lymphoid tissues, may theoretically become the site for early adhesion, invasion, and even replication of OT. As early as 2003, using Hitachi 12A and Hitachi H-7000 transmission electron microscopes (Tokyo, Japan), Kadosaka et al. [13] reported the accumulation of a large amount of OT in the cytoplasm of the salivary glands of uneaten larvae. In 2014, they were the first to use PCR technology in an animal model and reported OT accumulation in the lungs, spleen, liver, and other organs of the animals. The detection of OT DNA suggested that the lungs could be used as a potential target organ of natural hosts [14]. The mouse model of severe scrub typhus established by Trent B et al. [15] suggested a severe inflammatory response in the lungs; the OT load in the lungs peaked on the tenth day and was significantly higher than that in any other organ (heart, liver, or brain) on the fourteenth day [14] Pathogens can be detected in bronchoalveolar lavage fluid (BALF) [16]. These experiments indirectly indicated that the respiratory tract is no longer a simple “passage channel” but instead an active place for the distribution and replication of pathogens. In this study, we detected OT nucleic acid in nasopharyngeal swab samples before doxycycline administration in some patients. Our results were consistent with those of the abovementioned animal and basic experiments. These findings suggest that OT DNA can be detectable in the nasopharynx during early human infection, though the clinical significance of this detection requires further investigation.
However, we did not detect OT in any of the urine or stool samples, which may be related to its own characteristics. OT is an obligate intracellular parasitic pathogen. Recently, many studies have shown that OT can be detected in endothelial cells, as well as spleen and lung tissues [14,17]. However, no relevant reports of active secretion or shedding into the intestinal cavity or urinary tract have been published. This may explain why the OT load is extremely low in the urine and stool of patients and is difficult to detect by high-sensitivity PCR. Our experimental results are consistent with this conclusion. Through systematic detection of clinical samples using high-sensitivity PCR, we similarly failed to detect OT nucleic acid in patient urine and stool samples. This verifies the theoretical speculation that, due to its obligate intracellular parasitic nature, OT is unlikely to be released from primary infection sites into excretions.
In the OT phylogenetic tree of the TSA56 gene sequence, approximately 66.66% of the OT strains were highly homologous with the Karp genotype, which is consistent with the dominant role of this genotype in the global epidemic of scrub typhus [18]. Notably, although this genotype has been reported many times in previous studies, it was detected in nasopharyngeal swab samples for the first time, and its nucleotide level in blood samples from patients was 100%. These findings suggested the genetic stability of this genotype in different host tissues.
As early as 2009, Kelly et al. [18] divided OT into nine major genotypes through the TSA56 gene. Among them, the Karp type is the most common, particularly in the Asia–Pacific region, accounting for approximately 40% of all genotypes. The Karp type has been detected in numerous locations, such as China (e.g., Hainan, Guangdong, Fujian, Shandong, and the Penghu Islands), the Republic of Korea, Japan, and Southeast Asia (e.g., Vietnam and Cambodia) [18,19] and gradually increased from south to north in India [20]. Kato-type strains, accounting for approximately 10% [18], were the dominant strains in India and were also sporadically found in Vietnam, Cambodia, and Japan. TA763, which was first found in Thailand, also accounted for approximately 10% [18]. Subsequently, TA763 was reported in China, Vietnam, Cambodia, and other places. The Gilliam type is the least dominant, accounting for only 5%, and is distributed mainly in Myanmar and northern India [18]. In addition, the Kawasaki, Kuroki, and JG genotypes are prevalent in Japan, whereas the Boryong genotype is predominant in the Republic of Korea [18]. Therefore, the Asia–Pacific region showed a distribution pattern dominated by the Karp genotype, with the coexistence of multiple genotypes. However, reports on genotypes and their distribution characteristics other than those of the Asia–Pacific region are rare. Therefore, future efforts should focus on expanding the scope of surveillance to address this long-standing knowledge gap.
In China, genotypes significantly differ between the north and south. In southern China, in regions such as Hainan [10], Guangdong [21], and Yunnan [22], the predominant genotypes are Karp, Gilliam, and TA763. In contrast, in northern areas such as Shandong [23] and Inner Mongolia [1], the Kawasaki type is dominant. Kim et al. [24] reported that different genotypes may affect the clinical outcomes of patients. In Karp-type strains, a relatively high viral load is associated with a high likelihood of organ failure and an increased likelihood of admission to the intensive care unit (ICU). The mechanism may be related to the immune response of the body to pathogens. During OT infection, the body secretes many proinflammatory cytokines, such as IFN-γ, TNF-α, and IL-6, resulting in a “cytokine storm”, causing damage to vascular endothelial cells and multiple organ failure [25]. Similar findings were reported by Jiali Long et al. [21], in which patients infected with Karp-type strains showed more frequent multi-organ involvement and worse prognostic indicators. However, whether genotype information can inform risk stratification or genotype-guided management requires validation in larger, prospective studies integrating genotypes with bacterial load, severity, and treatment response
This study has several limitations, such as its small sample size and single-center nature. Nevertheless, studies simultaneously assessing OT in NPS, urine, and feces remain scarce, and the present study may help clinicians better understand its distribution across these specimens. This study provides a new perspective and basis for disease prevention and control. In the future, we should increase the sample size and use multicenter studies to confirm the feasibility and scope of the application of the nasopharyngeal swab test.
5. Conclusions
In summary, this study suggested that NPS is not sensitive enough to replace blood (or eschar) for initial diagnosis, but it can serve as a noninvasive, supplementary specimen during the short window after antibiotics are started—useful for follow-up in outpatient or community settings. These pilot data from a single center provide a practical option for clinicians and there is a need for larger studies to define accuracy and timing more precisely.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Taylor A.J. Paris D.H. Newton P.N. A systematic review of mortality from untreated scrub typhus (Orientia tsutsugamushi)P Lo S Negl. Trop. Dis.20159 e 000397110.1371/journal.pntd.000397126274584 PMC 4537241 · doi ↗ · pubmed ↗
- 2Hazra S. Dutta A.P. Moitra S. Das S. Mallick S.K. Sarkar A. Binita P. Ayan C. Debapriya B. Arnab S. Seroprevalence of scrub typhus among patients with acute febrile illness J. Fam. Med. Prim. Care 2025141423142910.4103/jfmpc.jfmpc_1761_2440814548 PMC 12349805 · doi ↗ · pubmed ↗
- 3Luce-Fedrow A. Lehman M.L. Kelly D.J. Mullins K. Maina A.N. Stewart R.L. Ge H. John H.S. Jiang J. Richards A.L. A Review of Scrub Typhus (Orientia tsutsugamushi and Related Organisms): Then, Now, and Tomorrow Trop. Med. Infect. Dis.20183810.3390/tropicalmed 301000830274407 PMC 6136631 · doi ↗ · pubmed ↗
- 4Yue Y. Ren D. Liu X. Wang Y. Liu Q. Li G. Spatiotemporal patterns of scrub typhus in mainland China, 2006–2017 P Lo S Negl. Trop. Dis.201913 e 000791610.1371/journal.pntd.000791631790406 PMC 6917297 · doi ↗ · pubmed ↗
- 5Jiang J. Richards A.L. Scrub Typhus: No Longer Restricted to the Tsutsugamushi Triangle Trop. Med. Infect. Dis.201831110.3390/tropicalmed 301001130274409 PMC 6136623 · doi ↗ · pubmed ↗
- 6Liu Q. Ji H. Shang M. Notified Vector-Borne Diseases—China, 2005–2024 China CDC Wkly.2025796196610.46234/ccdcw 2025.16240832060 PMC 12360307 · doi ↗ · pubmed ↗
- 7Ono A. Nakamura K. Higuchi S. Miwa Y. Nakamura K. Tsunoda T. Kuwabara H. Furuya Y. Dobashi K. Mori M. Successful diagnosis using scab for PCR specimen in Tsutsugamushi disease Intern. Med.2002540841110.2169/internalmedicine.41.40812058894 · doi ↗ · pubmed ↗
- 8Jiang T. Jiang F. Qi W. Gu L. Wang L. Sun L. Expert consensus on the clinical diagnosis and treatment of scrub typhus Chin. J. Zoonoses 2024401610.3969/j.issn.1002-2694.2024.00.01 · doi ↗