Traditional, Complementary, and Alternative Medicine for Self-Care in Chronic Neck and Shoulder Pain: A Scoping Review
Thi Khanh Ha Doan, Ernesta Sofija, Thu-Hang Ho-Thi, Nguyen Ngoc Phan, Hiep N. Le, Lan N. C. Nguyen, Hai Phung

TL;DR
This review explores how traditional and alternative medicine supports self-care for chronic neck and shoulder pain, highlighting gaps in psychological and social aspects.
Contribution
The study maps TCAM-based self-care strategies and identifies overlooked domains like psychological well-being and cultural context.
Findings
Most studies focused on self-care maintenance and management, such as physical activities and pain control.
Dimensions like psychological well-being and social support were frequently overlooked in TCAM research.
The review suggests a need for a more holistic approach to self-care in chronic pain management.
Abstract
Background: Traditional, complementary, and alternative medicine (TCAM) is a promising and increasingly popular approach in managing chronic neck and shoulder pain. Despite recognized benefits for pain relief and well-being, how TCAM facilitates self-care practices is poorly understood. This scoping review maps the existing evidence on TCAM-based self-care strategies for adults with chronic neck and shoulder pain to identify which domains of self-care are addressed and which are overlooked. Methods: We searched five academic databases, including PubMed, Scopus, Embase, Cinahl Complete (EBSCOhost), and Public Health Database (ProQuest). Articles published over a 20-year period that examined the use of TCAM for adults with chronic neck and shoulder pain were included. An analytical framework based on Riegel’s three core components of self-care (maintenance, monitoring, and management) was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
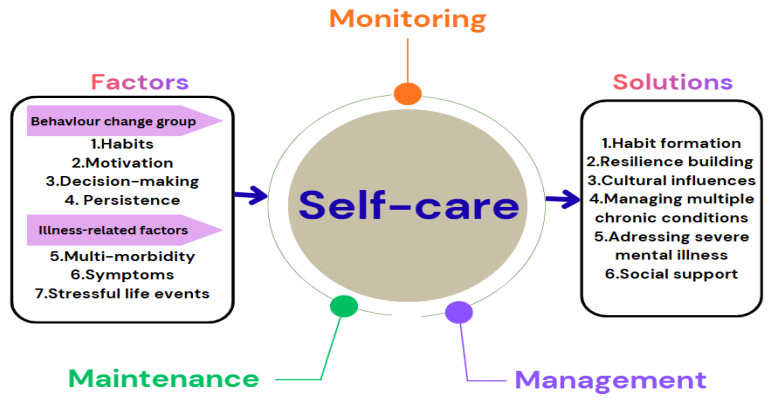 Figure 1
Figure 1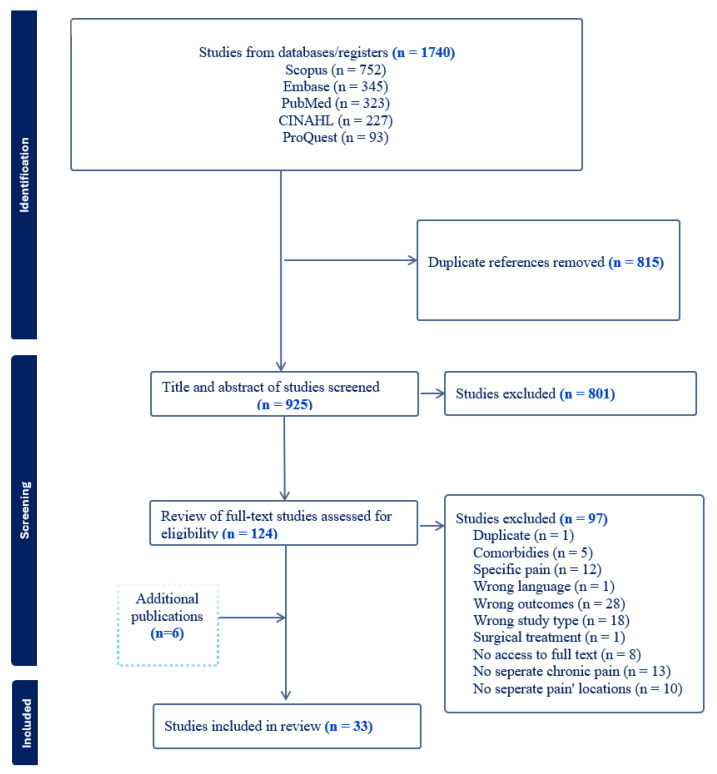 Figure 2
Figure 2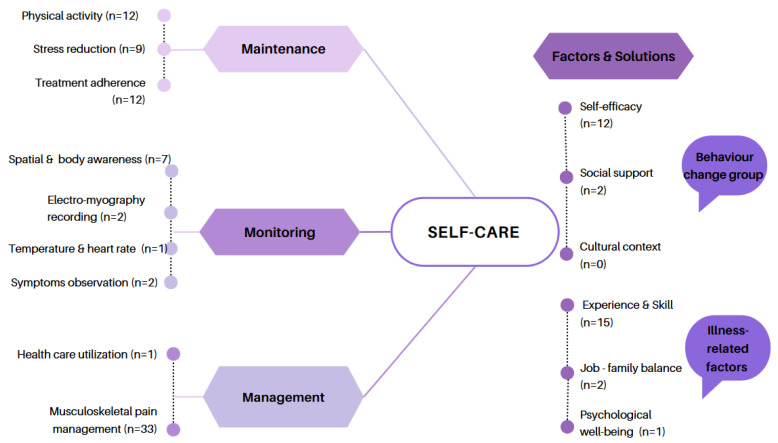 Figure 3
Figure 3| Study Reference Number | Country | Study Design | Participant Characteristics | Outcomes |
|---|---|---|---|---|
|
| ||||
| [ | Hong Kong (physiotherapy outpatient | RCT (exercise) | CNP (N = 145) | Pain, disability, |
| [ | Sweden (physiotherapy departments in primary care) | RCT (Qigong) | CNP (N = 122) | Pain, disability, grip strength, and cervical range of motion |
| [ | India (software | RCT (self-SNAGS along with conventional | CNP (N = 38) | Incidence of neck pain, range of motion, and disability |
| [ | Hong Kong (outpatient physiotherapy | RCT (active electrical | CNP (N = 49) | Pain |
| [ | US (Group Health, | Randomized, | CNP (N = 64) | Neck-related disability and symptom |
| [ | Germany (gymnasia) | RCT (Qigong or | CNP (N = 123) | Pain, disability, and quality of life |
| [ | Germany (community) | RCT (thermotherapy | CNP (N = 50) | Pain, functional |
| [ | India (Department of Musculoskeletal | RCT (self-sustained natural apophyseal glides (SNAGS), | CNP (N = 112) | Pain, disability, active cervical range of |
| [ | Germany (outpatient | RCT (a 9-week Iyengar yoga program with | CNP (N = 77) | Pain, disability, quality of life, and |
| [ | Germany (single | RCT (a 9-week yoga | CNP (N = 51) | Pain, disability, quality of life, cervical range of motion, proprioceptive acuity, and pressure pain threshold |
| [ | Spain (a university | RCT (Group 1: manual | CNP (N = 45) | Disability, fear-avoidance beliefs, neck flexor muscle endurance test, fatigue scale |
| [ | Germany (outpatient | RCT (an 8-week | CNP (N = 89) | Pain, disability, perceived stress, |
| [ | UK (primary care) | RCT (12 acupuncture | CNP (N = 517) | Pain, disability, quality of life, and adverse events |
| [ | Latvia (public health | RCT (team learning (TL) with self-management | CNSP (N = 31); bank and agricultural advisory services VDT employees; | Pain, quality of life, |
| [ | Germany (Department | RCT (Tai Chi or | CNP (N = 114) | Pain, disability, quality of life, well-being, and perceived stress, |
| [ | UK (4 outpatient | RCT (interactive behavioral modification therapy (IBMT)) | CNP (N = 57) | Disability, pain |
| [ | US (University of Idaho) | A single-group, multiple-baseline design (ten one-hour group classes in the Alexander technique) | CNP (N = 10) | Self-reports, superficial neck flexor activation and fatigue, posture |
| [ | UK (primary care) | ATLAS randomized, | CNP (N = 517) | Pain and disability, self-efficacy, self-care |
| [ | China (Department of Rehabilitation Medicine) | Press needle combined with transcutaneous electrical nerve stimulation | CNP (N = 80) | Pain and disability, range of motion, neck muscle average electromyography (EMG) |
| [ | Brazil (no mention) | A pragmatic RCT | CNP (N = 90) | Pain, disability, range of motion, fear-avoidance beliefs, and pain self-efficacy |
| [ | Spain (no mention) | RCT (a self-MRT | CNP (N = 58) | Pain and active cervical |
| [ | Brazil (the community) | RCT (guideline-based | CNP (N = 116) | Pain, disability, global perceived effect, quality of sleep, pain catastrophizing, and self-efficacy |
| [ | US (University of Idaho) | A two-group, | CNP (N = 16), | Pain/disability, pain self-efficacy, activation of the sternocleidomastoid muscles, and posture |
| [ | Iran (two rehabilitation and physiotherapy | A three-arm RCT | CNP (N = 72) | Pain/disability |
| [ | Spain (School of | Prospective, parallel group, randomized clinical trial (an individualized | CNP (N = 53) | Disability, Fear-Avoidance Beliefs, Health-Related Quality of Life, Pain, Anxiety, and Depression |
| [ | Iran (universities, | Multicenter assessor-blinded RCT (pain | CNP (N = 80) | Pain and fear of movement |
| [ | Japan (Hamamatsu | A single-center, | CNSP (N =10) | Neck and shoulder stiffness, pain, skin temperature, heart rate variability, and baroreceptor reflex sensitivity |
| [ | Brazil (no mention) | RCT (OMT plus EG) | CNP (N = 90) | Pain, disability, range of motion, fear-avoidance beliefs, and pain self-efficacy |
| [ | Japan (no mention) | Open-label trial (2-week self-care with gentle | Chronic neck and shoulder discomfort (N = 12) | Pain sensation, discomfort, and difficulty in moving; joint range of motions |
| [ | Japan (a medical school and a medical institution) | RCT (acupuncture using press needles) | CNP (N = 50) | Pain, disability, pressure pain threshold |
|
| ||||
| [ | Germany (universities, gyms, general | Pragmatic randomized | CNP (N = 220) | Pain, pain-related stress, sick-leave days, pain medication intake, and adherence |
|
| ||||
| [ | Sweden (primary | A qualitative evaluation (Feldenkrais groups) | CNSP (N = 14) | Experiences, effects of movement exercises, self-practice |
| [ | UK (primary care) | Longitudinal sub-study within the ATLAS trial (Alexander technique lessons OR acu-puncture sessions) | CNP (N = 30) | Perspectives of |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsComplementary and Alternative Medicine Studies · Musculoskeletal pain and rehabilitation · Mindfulness and Compassion Interventions
1. Introduction
Complementary and alternative medicine (CAM) encompasses a diverse group of medical systems, practices, and products not traditionally considered part of conventional medicine and is not fully integrated into the mainstream healthcare system [1,2]. These practices, sometimes referred to simply as “traditional medicine” [3], can often be categorized into five major domains: (1) whole medical systems (e.g., naturopathy and traditional Chinese medicine); (2) mind–body medicine (e.g., yoga and meditation); (3) biologically based practices (e.g., herbal medicine and diet therapies); (4) manipulative and body-based practices (e.g., exercise and massage); and (5) energy medicine (e.g., acupuncture, reiki, Qi gong, and Tai Chi) [1]. Collectively, TCAM is associated with a range of benefits, including improvements in metabolic health, reductions in stress, anxiety, and depression, and potential healthcare cost savings [4,5,6,7].
For pain management, TCAM offers several effective strategies, including acupuncture, mind–body techniques, cupping, and massage therapy [8,9,10,11]. The prevalence of this issue is significant; in the United States, more than 1 in 5 adults report experiencing pain daily or on most days and experience impacts on their daily and social activities [12]. Furthermore, chronic pain is associated with higher rates of depression and reduced physical activity, diminishing quality of life, and contributing to a significant societal burden [13,14]. The economic impact is also substantial, with chronic pain costing an estimated USD 560 billion annually from lost productivity, direct medical costs, and disability programs [15].
Despite this, in routine clinical practice, healthcare professionals often focus narrowly on the painful condition itself. As a result, patient self-management strategies are frequently ignored, overlooked during assessment, and left unincorporated into care plans. The World Health Organization (2005) emphasized the importance of self-managing chronic conditions at both the individual and population levels [16]. Therefore, developing policies and clinical practices that systematically evaluate and integrate these self-management strategies is crucial for helping patients alleviate pain during and after hospitalization.
Musculoskeletal disorders, particularly spine-related pain and disability, are recognized as a significant global threat to healthy aging [17]. Following the COVID-19 pandemic, a higher incidence of musculoskeletal pain has been reported [18,19]. Consequently, the trend in the use of TCAM among people suffering from chronic neck and shoulder pain has shown a notable rise. Therefore, cervical pain is a prevalent health issue affecting people of all ages, not just the aging population, in modern societies [20,21].
Another motivation for using TCAM during episodes of neck pain includes skepticism toward conventional medicine (28%) and the financial burden of out-of-pocket expenses (13%) [22]. Despite current policies encouraging those with chronic neck and shoulder pain to seek conventional medical care, many individuals still have confidence in TCAM. For example, adults who self-manage their spinal health through physical activity can enhance muscle strength, reduce the risk of chronic diseases, alleviate anxiety and stress, and help maintain meaningful social connections [23]. Clinical guidelines also advocate for addressing psychological factors and adopting active self-management strategies, including relaxation techniques, exercise, and mindfulness [24]. Given these trends, there is a pressing need for research that systematically maps TCAM-based self-care strategies for managing chronic neck and shoulder pain. Understanding the impact of these approaches is essential for improving outcomes not only for individuals but also for their families and communities.
Self-management for spine pain requires behavior changes and clear communication between practitioners and their patients [25]. The reason for this is that mid-life and older adults have unique motivations for maintaining musculoskeletal health, including accessing social engagement, fear of falling, and exercising for fitness and to feel young [26,27]. Additionally, safety is the most important aspect of self-management strategies. Therefore, healthcare professionals and their patients must work as a team to obtain enough knowledge and skills so that the patients can have confidence to practice by themselves [28]. Furthermore, multimodal training has demonstrated beneficial effects on both functional outcomes and symptom relief in individuals with chronic neck and shoulder pain [29]. Consequently, Riegel’s theory is applicable not only to patients or nurses but also to all healthcare professionals involved in promoting self-care for people with chronic neck and shoulder pain.
This scoping review uses Riegel’s (2012) middle-range theory of self-care of chronic illness (Figure 1), which defines self-care as maintaining health through proactive behavior and effective illness management [30]. The theory comprises three key components: (i) self-care maintenance—daily health-promoting practices like sleep, exercise, nutrition, and treatment adherence; (ii) self-care monitoring—tracking health indicators including physical symptoms (pain, stress, or temperature), sensations, daily routines, or cognitive processes; and (iii) self-care management—responding to symptoms through medication, activity adjustments, or seeking support. In 2018, this theory was refined to clarify the link between symptoms and self-care [31], yet the complexity of self-care behaviors remains poorly understood. Riegel (2021) expanded on barriers to self-care and highlighted key knowledge gaps, identifying seven influencing factors grouped into two categories: behavioral (habits, motivation, decision-making, and persistence) and illness-related (multimorbidity, symptoms, and stressful life events) [32]. Six proposed solutions include habit formation, resilience-building, cultural influences, managing multiple chronic conditions, addressing severe mental illness, and social support. This framework offers a comprehensive view of self-care components, highlighting both addressed areas and existing gaps.
This study is important for four key reasons. First, it explores the self-care strategies employed by adults with chronic neck and shoulder pain within TCAM practices, offering insights into how individuals manage pain in everyday life. Second, it identifies the most frequently associated self-care components within TCAM, helping to clarify which practices are commonly integrated into pain management routines. Third, it examines the factors influencing self-care behaviors during pain episodes, including personal, cultural, and contextual elements. Finally, it highlights recommended solutions to enhance self-care during pain episodes, contributing to more effective and sustainable approaches for individuals, healthcare providers, and policymakers. To achieve these aims, this scoping review will systematically investigate the multifaceted nature of TCAM-related self-care strategies for managing chronic neck and shoulder pain, addressing gaps in the existing literature and guiding future interventions.
In this review, the following research questions are addressed:
What self-care strategies are employed by adults with chronic neck and shoulder pain within TCAM practices?
Which self-care components are most frequently associated with TCAM in pain management?
What factors are related to self-care practices during pain episodes?
What solutions are recommended to enhance self-care during pain episodes?
2. Materials and Methods
2.1. Design
This scoping review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses-Extension for Scoping Reviews (PRISMA-ScR) guidelines [33] and the Joanna Briggs Institute (JBI) Manual for Evidence Synthesis [34]. The protocol was registered on Figshare (DOI: 10.6084/m9.figshare.28955390). A completed PRISMA-ScR checklist is provided in the Supplementary Materials.
2.2. Eligibility Criteria
The inclusion criteria were guided by the PICO framework [35]:
- Population: Adults (≥18 years) with chronic neck and/or shoulder pain.
- Intervention: Any TCAM-based self-care strategy (excluding pharmacological interventions). This also includes integrative approaches combining TCAM with conventional care.
- Outcomes: Pain, disability, psychosocial variables, or other relevant outcomes.
- Study Types: Original peer-reviewed research articles published between 2004 and November 2024, with the timeframe selected due to the increased utilization of CAM since 2010 and its association with multi-level self-care approaches since 2005 [16,36].
In this review, disability was operationalized using validated self-report instruments widely used in musculoskeletal research, including the Neck Disability Index (NDI), Northwick Park Neck Pain Questionnaire (NPQ), Copenhagen Neck Functional Disability Scale, and similar tools. These measures assess functional limitations related to neck and shoulder pain rather than formal diagnostic criteria such as those defined by the Americans with Disabilities Act (ADA).
Language: Initially, only English-language studies were included. Following reviewer feedback, we have expanded eligibility to include studies published in other languages if they provide an English abstract and sufficient methodological detail for data extraction. This change did not require a full re-execution of the search; instead, previously excluded records were rescreened under the revised criterion. Ultimately, all included studies were either published in English or had comprehensive English abstracts, and no full-text non-English studies were incorporated. This limitation is noted in the Section 4.
Exclusions: Systematic reviews, conference abstracts, letters, opinions, books, and protocols were excluded. No geographic restrictions were applied.
2.3. Search Strategy and Information Sources
A comprehensive literature search was conducted in five databases: PubMed, Scopus, Embase, CINAHL Complete (EBSCOhost), and Public Health Database (ProQuest). The search strategy combined terms for neck/shoulder pain, TCAM interventions, and self-care concepts. The full search strategy for each database is provided in Appendix A. Reference lists of included studies were hand-searched for additional articles.
2.4. Study Selection
All records were imported into EndNote version 21 and screened in Covidence (https://app.covidence.org/reviews/active, accessed on 5 November 2024). Two independent reviewers (T.K.H.D. and N.N.P.) screened titles and abstracts against eligibility criteria. Full texts of potentially relevant studies were assessed independently. Discrepancies were resolved through discussion or consultation with a third reviewer.
2.5. Data Charting Process
Data charting followed an iterative process recommended by JBI:
- A data extraction template was developed and piloted on five studies, then refined for clarity and completeness.
- Extracted variables included author(s), year, country, study design, setting, sample characteristics, intervention details, outcomes, and key findings.
- Additional columns captured self-care components (maintenance, monitoring, and management) and behaviors based on Riegel’s middle-range theory of self-care of chronic illness.
- Two reviewers independently charted data; discrepancies were resolved through consensus.
The final charting table is presented in Appendix B and Appendix C.
2.6. Synthesis of Results
Findings were synthesized using a narrative approach and mapped to the three self-care domains (maintenance, monitoring, and management). We summarized patterns across interventions, identified gaps, and highlighted underrepresented factors (e.g., cultural context, psychological well-being). Although most of the included studies were randomized controlled trials, the decision not to weigh the strength of evidence aligns with the scoping review methodology, which prioritizes mapping the breadth of research rather than evaluating its quality.
Explicitly mentions PRISMA-ScR compliance.Adds detail on data charting (development, piloting, refinement, and dual extraction).Revises language inclusion criteria per reviewer request.Clarifies synthesis approach and rationale for no critical appraisal.
3. Results
3.1. Literature Selection
The literature search yielded 1740 records. Following the removal of duplicates and a two-stage screening process, 27 studies met the eligibility criteria. An additional six studies were identified through a hand-search of reference lists, resulting in a final sample of 33 studies for synthesis. The full study selection process is detailed in the PRISMA flowchart (Figure 2).
3.2. Characteristics of Included Studies
The details of the 33 studies included in the final analysis are presented in Table 1 and Appendix B. These studies were published between 2005 and 2024, with the majority (n = 21) published in the last 10 years. The evidence base is primarily composed of quantitative efficacy trials. The majority of studies were randomized controlled trials (n = 27) focused on chronic neck pain (n = 29), with only two studies employing qualitative methods to explore patient experiences. Other designs were used infrequently, including single-arm trials (n = 2), a two-armed pre-test/post-test design (n = 1), and a three-armed trial (n = 1). Sample size varied widely from 10 to 517, with a median of 64 participants.
This research was geographically concentrated in high-income countries (n = 25), as classified by the World Bank [37]. These countries included the United States, the United Kingdom, Germany, Sweden, Latvia, Spain, Japan, and Hong Kong. Additionally, the study featured a notable gender imbalance, with 27 studies reporting a higher prevalence in females. The typical participant was over 40 years old, reflecting a focus on mid-life to older adult populations. Interventions were most often delivered in healthcare settings (n = 17), though universities, communities, and workplaces also featured. Therapies were split between single-approach (n = 19) and multi-approach (n = 14) formats. The single-approach format involved the use of one therapeutic technique, such as exercise, qigong, massage, thermotherapy, yoga, meditation, or acupuncture. In contrast, multi-approach formats incorporated a combination of different therapeutic techniques. Examples include individualized self-management combined with physical therapy intervention, therapeutic exercises combined with pain neuroscience education, guideline-based physical therapy plus dry needling, osteopathic manipulative treatment associated with exercise, Alexander lessons plus usual care, and acupuncture plus usual care. Pain was the most frequently assessed outcome (n = 26), followed by disability (n = 23), psychological factors (n = 13), such as depression, anxiety, fatigue, or anger, and quality of life (n = 9). Disability was defined through validated self-report measures, including the Neck Disability Index (NDI), the Northwick Park Neck Pain Questionnaire (NPQ), the Copenhagen Neck Functional Disability Scale, the Neck Pain and Disability Questionnaire, or the Neck Pain and Disability Scale (NPAD). Notably, nearly all studies (n = 32) reported positive effects, suggesting a generally favorable impact of interventions across diverse designs and settings.
It is also noted that the predominance of studies from high-income countries and the overrepresentation of women may skew the evidence toward self-care strategies common in these contexts, such as structured exercise or mind–body practices, while approaches relevant to low-resource settings or male populations may remain overlooked. This highlights socioeconomic and gender-related influences on self-care, which are further discussed in Section 4.
3.3. Self-Care Concepts and Self-Care Behaviors
The interventions from the 33 included studies were analyzed using the self-care framework of maintenance, monitoring, and management [30,31,32]. As shown in Table 2, Appendix B and Appendix C, this synthesis revealed a clear pattern in how TCAM-based self-care is currently addressed in the literature.
Our analysis showed a strong emphasis on self-care management (present in all 33 studies) and self-care maintenance (n = 20), typically involving pain control and physical activity (Figure 3). In stark contrast, self-care monitoring (n = 11) was significantly underrepresented. These monitoring elements were implemented through techniques including symptom diaries, self-observation, and physiological measurements such as temperature or EMG. A holistic approach integrating all three components was rare, found in only five studies, primarily those investigating mind–body therapies like Tai Chi. Regarding the influencing factors on self-care, “Experience and Skill” (n = 15) and “Self-efficacy” (n = 12) were the most frequently examined. However, other critical factors identified by Riegel’s theory, such as social support (n = 2), job–family balance (n = 2), cultural context (n = 0), and psychological well-being (n = 1), were almost entirely overlooked.
4. Discussion
This scoping review aimed to explore how traditional, complementary, and alternative medicine (TCAM) contributes to self-care among patients with chronic neck and shoulder pain. Utilizing the middle-range theory of self-care of chronic illness as an analysis framework, we conducted a gap analysis across its three domains: self-care maintenance, monitoring, and management. Our review found that the ‘self-care monitoring’ component is largely absent, despite being a vital element in the daily self-care of chronic patients [71]. This essential domain could provide significant information for decision-making in future actions [72]. While all studies addressed self-care management, consistent with previous reviews [73], our analysis highlights the limited integration of all components. Thus, we recommend designing interventions that holistically incorporate maintenance, monitoring, and management to enhance the heterogeneity of designs and interventions.
Another finding is that not all behaviors suggested by the middle-range theory of self-care of chronic illness have been thoroughly examined. There has been a focus on certain behaviors, such as physical activity and treatment adherence, which are frequently studied, whereas other vital behaviors, such as sleep and nutrition practices, are often overlooked. These behaviors play a significant role in pain management and overall well-being. For example, an individual may use vitamins, medicinal herbs [74], or meditation [75] or seek acupuncture at traditional clinics [76]. On the other hand, risky behaviors such as substance abuse have been linked to increasing pain-related mortality [77], and factors like sleep patterns and smoking status may confound the relationship between TCAM and pain management [78,79].
Additionally, self-care factors such as self-efficacy, experience, and skill have been well-explored in efforts to enhance self-care by fostering individual habits. However, other factors such as cultural beliefs and values have been less examined, despite their influence on treatment preferences. For example, TCAM is more commonly used in Asian culture [80], and minority populations often favor non-invasive medical treatment and self-management for their pain [81]. Our findings also revealed that existing research has predominantly been conducted in high-income countries, leaving regions most affected by chronic neck and shoulder pain, such as Southeast Asia and Africa, significantly underrepresented [39,49,50,67,82]. In fact, culture-based interventions have demonstrated positive outcomes, including lower rates of rehospitalization and mortality, increased patient satisfaction, and cost savings [83]. This highlights the need for tailored interventions that align with patients’ cultural backgrounds and customs. Therefore, another key recommendation from this analysis is to expand research into culturally informed self-care strategies that reflect patients’ values and preferences.
Psychological factors are another area of concern. Despite the high prevalence of stress, anxiety, and depression among individuals with chronic pain [84], few interventions address these dimensions. Given that everyday stress can significantly increase mortality risk in chronically ill adults [85], future self-care programs must incorporate psychological support to improve holistic outcomes. Integrating TCAM-based self-care principles into conventional educational strategies enables healthcare professionals, including nurses, physiotherapists, and primary care physicians, to deliver a more comprehensive, patient-centered approach that promotes engagement, improves adherence, and enhances overall quality of life.
Limitations
While this review employed a rigorous methodology, certain limitations should be acknowledged. Initially, the inclusion criteria restricted studies to those published in English, which may have led to the omission of relevant evidence from non-English sources. Following reviewer feedback, we have expanded eligibility to include studies published in other languages if they provide an English abstract and sufficient methodological detail for data extraction. Nevertheless, this approach may still underrepresent culturally diverse perspectives and interventions related to cultural groups and contextual backgrounds, particularly from regions where TCAM practices are prevalent, such as Southeast Asia and Africa. Future reviews should incorporate multilingual searches and translation strategies to ensure a more comprehensive synthesis of global evidence.
It should be noted that the included studies did not adopt a globally standardized definition of disability. Instead, most relied on self-report scales validated for musculoskeletal conditions. While these tools are widely accepted in clinical research, variability across countries may introduce conceptual differences. This heterogeneity represents a limitation and underscores the need for future research to consider harmonized definitions of disability to improve comparability.
5. Conclusions
This scoping review systematically mapped the evidence on TCAM-based self-care strategies for adults with chronic neck and shoulder pain. Current research predominantly focuses on self-care maintenance (e.g., physical activity and treatment adherence) and management (e.g., pain relief), while self-care monitoring and broader psychosocial and cultural dimensions remain underexplored. These gaps highlight the need for future research to prioritize the design of TCAM self-care interventions that explicitly integrate monitoring and psychosocial support.
Given the exploratory nature of scoping reviews, our findings should not be interpreted as prescriptive recommendations for clinical practice or policy. Instead, they provide a foundation for identifying research priorities, such as the following:
- Developing interventions that incorporate all three self-care components.
- Examining cultural influences and psychological well-being in TCAM-based self-care.
- Expanding research beyond high-income countries to ensure global relevance.
By addressing these gaps, future studies can contribute to more comprehensive and patient-centered strategies for managing chronic neck and shoulder pain.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tabish S.A. Complementary and alternative healthcare: Is it evidence-based?Int. J. Health Sci.200825 PMC 306872021475465 · pubmed ↗
- 2World Health Organization WHO Traditional Medicine Strategy: 2014–2023 World Health Organization Geneva, Switzerland 2013 Volume 188
- 3Wisneski L. The Scientific Basis of Integrative Health Taylor & Francis Group Oxford, UK 2017
- 4Anderson J.G. Flatt J.D. Jabson J. Wharton W. Use of complementary therapies by sexual minority older adults: Findings from the national health interview survey Innov. Aging 2019314910.1093/geroni/igz 038.536 · doi ↗
- 5Innes K.E. Bourguignon C. Taylor A.G. Risk indices associated with the insulin resistance syndrome, cardiovascular disease, and possible protection with yoga: A systematic review J. Am. Board Fam. Pract.20051849151910.3122/jabfm.18.6.49116322413 · doi ↗ · pubmed ↗
- 6Kessler R.C. Davis R.B. Foster D.F. Van Rompay M.I. Walters E.E. Wilkey S.A. Kaptchuk T.J. Eisenberg D.M. Long-term trends in the use of complementary and alternative medical therapies in the United States Ann. Intern. Med.200113526226810.7326/0003-4819-135-4-200108210-0001111511141 · doi ↗ · pubmed ↗
- 7Lee M.S. Pittler M.H. Guo R. Ernst E. Qigong for hypertension: A systematic review of randomized clinical trials J. Hypertens.2007251525153210.1097/HJH.0b 013e 328092 ee 1817620944 · doi ↗ · pubmed ↗
- 8Holmberg C. Farahani Z. Witt C.M. How Do Patients with Chronic Neck Pain Experience the Effects of Qigong and Exercise Therapy? A Qualitative Interview Study Evid.-Based Complement. Altern. Med.2016201610.1155/2016/8010891 PMC 493215327418938 · doi ↗ · pubmed ↗