Metabolic and Immune Vulnerability in Critically Ill Patients with Diabetes Mellitus
Mădălina Diana Daina (Fehér), Codrin Dan Nicolae Ilea, Cosmin Mihai Vesa, Alina Cristiana Venter, Adriana Vladu, Timea Claudia Ghitea, László Fehér, Cristian Marius Daina

TL;DR
Critically ill patients with diabetes who die in the ICU often have high blood sugar, immune issues, and organ failure, with lactate levels and need for ventilation being strong predictors of death.
Contribution
Identifies metabolic and immune factors, along with ICU interventions, as key predictors of mortality in critically ill diabetic patients.
Findings
Non-survivors had higher admission lactate, blood glucose, and creatinine, and lower lymphocyte counts.
Mechanical ventilation and hemodialysis were independently associated with increased ICU mortality.
A predictive model showed good discrimination (AUC = 0.87) for ICU mortality in diabetic patients.
Abstract
Background and Objectives: Diabetes mellitus is frequently encountered in critically ill patients and is associated with increased short-term mortality. However, the biological and clinical determinants of mortality within the diabetic intensive care unit (ICU) population remain incompletely understood. This study aimed to evaluate laboratory parameters at ICU admission and key early ICU course variables, including acute complications and organ support interventions, associated with short-term ICU mortality in critically ill patients with diabetes mellitus. Materials and Methods: We conducted a retrospective observational cohort study including adult patients with diabetes mellitus admitted to a tertiary care ICU between January and December 2024. Demographic data, laboratory parameters at ICU admission, acute complications, and ICU interventions were collected. Patients were stratified…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
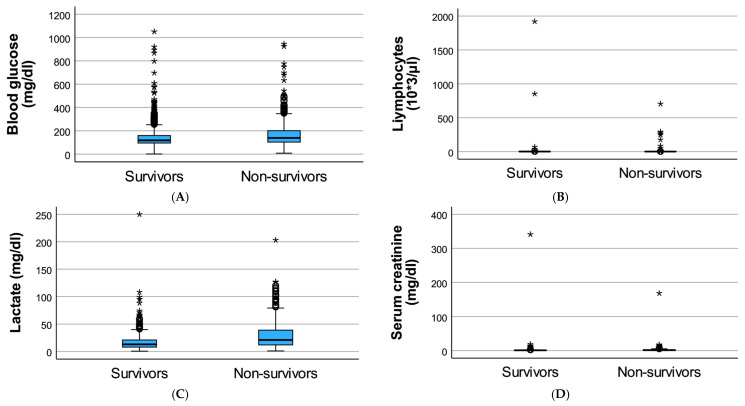 Figure 1
Figure 1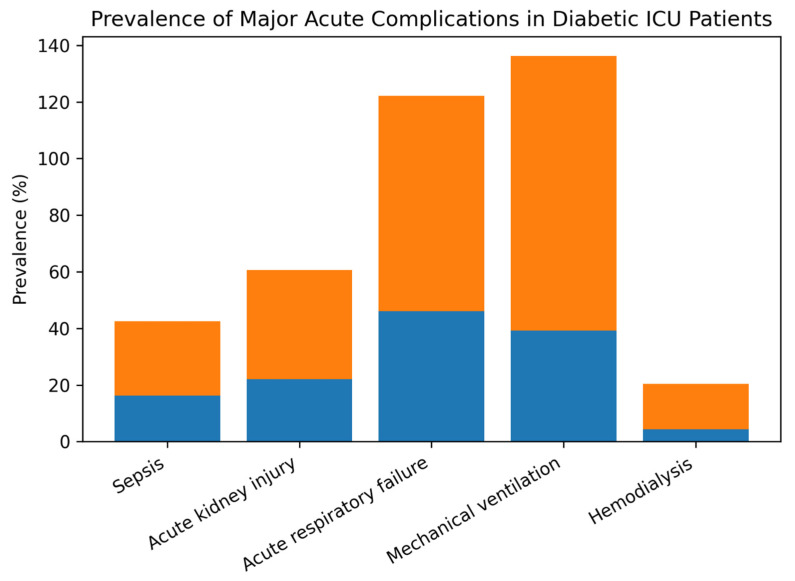 Figure 2
Figure 2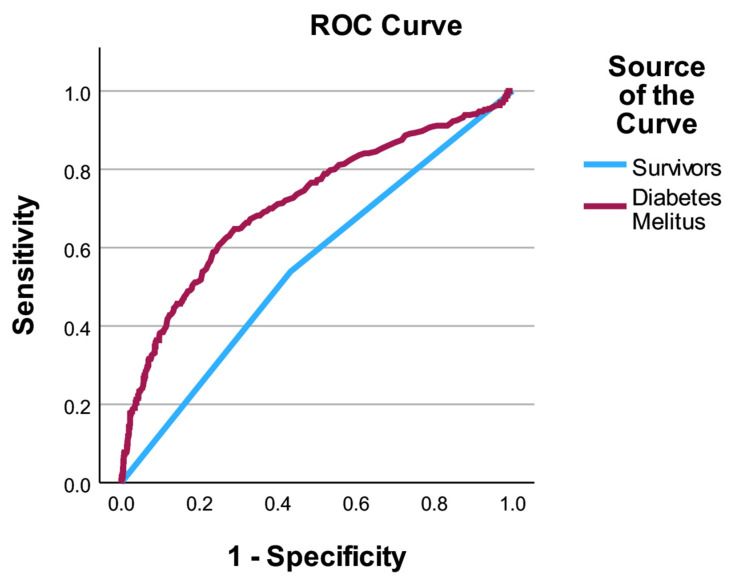 Figure 3
Figure 3- —University of Oradea
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHyperglycemia and glycemic control in critically ill and hospitalized patients · Sepsis Diagnosis and Treatment · Diabetes Treatment and Management
1. Introduction
Diabetes mellitus (DM) is one of the most prevalent chronic metabolic disorders worldwide and represents a major contributor to morbidity and mortality across a wide range of clinical settings. The increasing prevalence of diabetes, driven by population aging and the growing burden of cardiometabolic disease, has led to a substantial rise in the number of patients with diabetes admitted to intensive care units (ICUs) [1,2,3].
In critically ill patients, diabetes mellitus is frequently accompanied by metabolic dysregulation, chronic low-grade inflammation, immune dysfunction, and pre-existing organ impairment. These alterations may reduce physiological reserve and limit the ability to mount an effective response to acute stress, thereby increasing vulnerability during critical illness. Consequently, patients with diabetes often experience more severe disease courses and worse short-term outcomes when admitted to the ICU [4,5,6,7].
Previous studies have shown that diabetes mellitus is associated with increased ICU and in-hospital mortality. However, most investigations have focused on comparing outcomes between patients with and without diabetes, providing limited insight into the determinants of mortality within the diabetic population itself. As a result, the biological and clinical factors that distinguish survivors from non-survivors among critically ill patients with diabetes remain incompletely characterized [7,8,9,10,11].
Early identification of high-risk diabetic patients is of particular clinical importance, as timely recognition of metabolic stress, immune impairment, and organ dysfunction may allow for optimized monitoring and targeted supportive strategies. Biological markers obtained at ICU admission, together with the development of acute complications and the need for advanced organ support, may provide valuable prognostic information in this vulnerable population [12,13].
Therefore, the present study aimed to investigate laboratory parameters at ICU admission, acute complications, and intensive care interventions associated with short-term mortality in critically ill patients with diabetes mellitus. By focusing exclusively on diabetic patients, this study seeks to elucidate key predictors of ICU mortality and to support improved risk stratification in this high-risk group.
2. Materials and Methods
2.1. Study Design and Setting
We conducted a retrospective observational cohort study in the Intensive Care Unit of the Bihor County Emergency Clinical Hospital, a tertiary care center providing medical and surgical intensive care. The study included patients admitted between 1 January and 31 December 2024.
The study was designed to evaluate biological and clinical predictors of short-term mortality specifically in critically ill patients with diabetes mellitus.
2.2. Study Population
All adult patients (≥18 years) admitted to the ICU during the study period were screened for eligibility. For the present analysis, only patients with diabetes mellitus were included.
Diabetes mellitus was defined based on documented medical history, ongoing antidiabetic treatment (oral antidiabetic agents and/or insulin), or diagnostic blood glucose–based diagnostic criteria at admission. Patients with gestational diabetes or secondary forms of diabetes mellitus were excluded.
The final study cohort consisted of 443 critically ill adult patients with diabetes mellitus. Patients were stratified according to ICU outcome into survivors and non-survivors, based on mortality during ICU hospitalization.
2.3. Data Collection
Data were extracted retrospectively from electronic medical records and ICU charts. The following categories of variables were collected:
2.3.1. Demographic and Clinical Data
AgeSexType of ICU admission (medical or surgical)
2.3.2. Laboratory Parameters at ICU Admission
Only laboratory values obtained at the time of ICU admission were considered, to reflect the initial physiological status. These included:
- Blood glucose (mg/dL)
- Serum lactate (mg/dL; 1 mmol/L ≈ 9 mg/dL)
- Absolute lymphocyte count (10^3^/μL)
- Serum creatinine (mg/dL)
Lactate values were reported in mg/dL according to local laboratory standards; approximate mmol/L equivalents are provided to facilitate clinical interpretation.
2.3.3. Acute Complications During ICU Stay
The occurrence of major acute complications was recorded as binary variables (yes/no):
- Sepsis
- Acute kidney injury
- Acute respiratory failure
2.3.4. Intensive Care Interventions
The need for advanced ICU interventions during hospitalization was documented:
- Mechanical ventilation
- Hemodialysis
2.4. Outcome Definition
The primary outcome was mortality during ICU hospitalization, defined as death occurring at any time during the ICU stay.
2.5. Definitions of Acute Complications
Sepsis was defined according to Sepsis-3 criteria based on documented infection and organ dysfunction. Acute kidney injury was defined using KDIGO criteria based on serum creatinine changes during ICU stay. Acute respiratory failure was defined as the need for invasive or non-invasive ventilatory support due to hypoxemia or hypercapnia.
2.6. Statistical Analysis
Continuous variables were assessed for normality using visual inspection and were reported as mean ± standard deviation. Categorical variables were expressed as absolute numbers and percentages. Comparisons between survivors and non-survivors were performed using Student’s t-test for continuous variables and the chi-square test or Fisher’s exact test, as appropriate, for categorical variables. The proportion of missing data per variable was low (<5% for all included laboratory parameters).
To identify predictors of ICU mortality among patients with diabetes mellitus, univariate logistic regression analyses were first performed for each candidate variable. Variables showing statistical significance in univariate analysis or considered clinically relevant were subsequently included in a multivariate logistic regression model.
Missing data were handled using simple imputation, with median imputation for continuous variables and most-frequent value imputation for categorical variables, to preserve the full cohort size.
Results were reported as odds ratios (ORs) with 95% confidence intervals (CIs). Model discrimination was assessed using the area under the receiver operating characteristic curve (AUC/ROC). Model calibration was evaluated with the Hosmer–Leme show goodness-of-fit test, and overall predictive accuracy was assessed using the Brier score. To avoid overfitting, the multivariate model included clinically relevant variables and markers of disease severity.
Missing data were limited and primarily affected laboratory parameters at ICU admission. Simple imputation was performed prior to regression analyses to preserve cohort size, using median imputation for continuous variables and most-frequent category imputation for categorical variables. Given the retrospective design and low proportion of missingness, sensitivity analyses were not performed; however, the potential for residual bias related to missing data is acknowledged as a limitation.
Candidate variables for multivariate modeling included demographic factors, admission laboratory parameters, and clinically relevant ICU course variables. Collinearity between related variables (e.g., creatinine, AKI, hemodialysis) was assessed conceptually, and only variables providing complementary clinical information were retained. Continuous predictors were modeled linearly in the logit, acknowledging potential non-linearity as a limitation.
All statistical analyses were performed using IBM SPSS Statistics for Windows, version 30.0 (IBM Corp., Armonk, NY, USA). A two-sided p-value < 0.05 was considered statistically significant.
2.7. Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Bihor County Emergency Clinical Hospital (Approval No. 36976/23.10.2023) and the Ethics Council of the same institution (Opinion No. 36746/20.10.2023). Due to the retrospective observational design, the requirement for informed consent was waived by the institutional ethics committees. All data were anonymized prior to analysis to ensure patient confidentiality.
3. Results
3.1. Study Population and Outcome in Patients with Diabetes Mellitus
A total of 443 critically ill adult patients with diabetes mellitus admitted to the intensive care unit during the study period were included in the analysis. All patients had a confirmed diagnosis of diabetes mellitus prior to or at the time of ICU admission, as defined by medical documentation, antidiabetic treatment, or diagnostic blood glucose–based diagnostic criteria.
The study population was stratified according to ICU outcome into survivors and non-survivors. Overall, 239 patients (54.0%) died during ICU hospitalization, while 204 patients (46.0%) survived until ICU discharge, indicating a high short-term mortality rate within the diabetic subgroup.
Patients with diabetes mellitus who did not survive ICU hospitalization were generally older compared to survivors. No major differences were observed in sex distribution between the two groups. Medical admissions predominated in both survivors and non-survivors, reflecting the clinical complexity and acute illness severity typical of diabetic ICU patients.
This stratification provided the basis for subsequent analyses focusing on laboratory parameters at ICU admission, the occurrence of acute complications, and the need for intensive care interventions in relation to short-term mortality among patients with diabetes mellitus.
Baseline characteristics of diabetic ICU patients stratified by survival status are presented in Table 1. Non-survivors were significantly older than survivors and were more frequently admitted for medical conditions. Sex distribution was similar between the two groups.
3.2. Laboratory Profile at ICU Admission in Diabetic Patients
At ICU admission, diabetic patients who did not survive exhibited a significantly altered laboratory profile compared to survivors. Non-survivors presented with higher markers of metabolic stress and impaired organ function, reflecting increased physiological vulnerability at the onset of critical illness.
Admission blood glucose and lactate levels were higher in non-survivors, while lymphocyte counts and renal function, reflected by higher serum creatinine levels were significantly lower compared to survivors. These differences suggest an association between early metabolic imbalance, immune dysregulation, renal dysfunction, and short-term mortality in critically ill patients with diabetes mellitus.
The comparative laboratory profile of diabetic ICU patients according to survival status is summarized in Table 2 and Figure 1.
3.3. Acute Complications During ICU Stay in Patients with Diabetes Mellitus
The occurrence of acute complications during ICU hospitalization differed markedly between survivors and non-survivors among patients with diabetes mellitus (Table 3).
Non-survivors developed acute organ dysfunctions significantly more frequently than survivors. Acute respiratory failure was the most common complication overall and was observed in 76.2% of non-survivors compared to 46.1% of survivors. Similarly, mechanical ventilation was required in nearly all non-survivors (97.1%), while less than half of survivors required ventilatory support (39.2%).
Renal complications were also more prevalent among non-survivors. Acute kidney injury occurred in 38.5% of non-survivors compared to 22.1% of survivors, and the need for hemodialysis was almost four times higher in non-survivors (15.9% vs. 4.4%).
Infectious complications followed a similar pattern, with sepsis being significantly more frequent among non-survivors (26.4%) than survivors (16.2%). Overall, the presence of acute organ failure and the need for advanced ICU interventions were strongly associated with mortality in diabetic patients (Figure 2).
3.4. Predictors of ICU Mortality in Patients with Diabetes Mellitus
To identify predictors of ICU mortality among patients with diabetes mellitus, we performed univariate and multivariate logistic regression analyses. In univariate analyses, older age, higher lactate and serum creatinine levels, the presence of sepsis, acute kidney injury, acute respiratory failure, the need for mechanical ventilation, and hemodialysis were associated with increased odds of ICU death. Lower lymphocyte counts showed a borderline association with mortality.
In the multivariate model, lactate levels at ICU admission remained independently associated with mortality (OR = 1.02 per 1 mg/dL increase, 95% CI 1.00–1.04, p = 0.014). In addition, mechanical ventilation showed the strongest association with ICU mortality; however, this finding should be interpreted as reflecting advanced respiratory failure and overall disease severity rather than a direct causal effect (OR = 47.30, 95% CI 19.13–116.98, p < 0.001), and hemodialysis was also independently associated with mortality (OR = 3.38, 95% CI 1.13–10.11, p = 0.029). Other variables, including age, sepsis, acute kidney injury, acute respiratory failure, lymphocyte count, and serum creatinine, did not retain independent significance after adjustment, likely reflecting shared variance with markers of acute organ failure severity. Diabetes type was not consistently documented and was therefore not stratified.
The results of univariate and multivariate analyses are summarized in Table 4.
The multivariate model showed good discriminatory performance, with an AUC/ROC of 0.87. Model calibration was acceptable, as indicated by the Hosmer–Lemeshow test (χ^2^ = 12.63, p = 0.125). The overall probabilistic accuracy was supported by a Brier score of 0.135, suggesting good agreement between predicted and observed outcomes.
3.5. Model Performance and Risk Stratification
The performance of the multivariate logistic regression model was assessed in terms of discrimination and calibration. The model demonstrated good discriminatory ability, with an area under the receiver operating characteristic curve (AUC/ROC) of 0.87, indicating a high capacity to distinguish between survivors and non-survivors among diabetic ICU patients.
Model calibration was evaluated using the Hosmer–Lemeshow goodness-of-fit test, which showed no evidence of poor calibration (χ^2^ = 12.63, p = 0.125). Overall predictive accuracy was further supported by a Brier score of 0.135, reflecting good agreement between predicted probabilities and observed outcomes.
Taken together, these results highlight clinically relevant associations with ICU mortality; however, the model should be considered exploratory and requires external validation before use for formal risk stratification. The combination of early biological markers, particularly lactate levels, with indicators of advanced organ support allows for meaningful prediction of short-term ICU mortality in this high-risk population.
The discriminatory performance of the multivariate model is illustrated in Figure 3.
4. Discussion
In this study focusing exclusively on critically ill patients with diabetes mellitus, we identified a distinct clinical and laboratory profile associated with short-term ICU mortality. By restricting the analysis to diabetic patients, we were able to explore determinants of mortality beyond the mere presence of diabetes, highlighting factors that reflect metabolic stress, immune dysfunction, and acute organ failure.
At ICU admission, non-survivors exhibited significantly higher lactate levels, elevated blood glucose, impaired renal function, and lower lymphocyte counts compared to survivors. These findings suggest that diabetic patients who ultimately die during ICU hospitalization present with an early state of metabolic and immune vulnerability, which may predispose them to rapid clinical deterioration. Among these parameters, lactate emerged as an independent predictor of mortality, underscoring its role as a robust marker of tissue hypoxia, altered cellular metabolism, and global disease severity in critically ill patients with diabetes [14,15,16,17,18].
Acute organ dysfunctions occurring during ICU stay were markedly more frequent among non-survivors. Acute respiratory failure, acute kidney injury, and sepsis were all significantly associated with mortality in univariate analyses. However, in the multivariate model, mechanical ventilation and hemodialysis remained independently associated with ICU mortality. Importantly, these variables represent integrative markers of severe organ dysfunction and clinical deterioration during the ICU course, rather than modifiable prognostic factors on par with admission laboratory markers. Importantly, these interventions should not be interpreted as causal determinants of death but rather as integrative markers of disease severity and advanced organ failure. Their strong association with mortality reflects the profound physiological derangement present in patients requiring intensive organ support. This finding should be interpreted cautiously, as these interventions represent markers of disease severity rather than direct causal factors. Their strong association with mortality reflects the profound physiological derangement present in patients requiring advanced organ support [19,20,21,22]. Their strong association with mortality reflects the profound physiological derangement present in patients requiring advanced organ support.
The loss of statistical significance for several biological and clinical variables in the adjusted model likely reflects collinearity and shared variance with markers of severe organ failure. For example, renal dysfunction, sepsis, and respiratory failure frequently coexist in critically ill diabetic patients, forming a cascade of interrelated pathophysiological processes. In this context, mechanical ventilation and hemodialysis may act as integrative indicators of multisystem failure, capturing the cumulative burden of acute illness more effectively than individual variables [23,24,25,26,27].
Importantly, the good discriminatory performance of the multivariate model (AUC = 0.87) suggests that a combination of early biological markers and ICU interventions can provide meaningful prognostic information in diabetic patients. This supports the concept that risk stratification within the diabetic ICU population should account not only for baseline metabolic status but also for the rapid development of organ dysfunction requiring intensive support [28,29,30,31].
From a clinical perspective, these findings emphasize the importance of early recognition of metabolic stress and immune compromise in diabetic patients admitted to the ICU. Elevated lactate levels, lymphopenia, and early renal impairment may identify patients at particularly high risk, warranting closer monitoring and aggressive supportive management. Furthermore, the high mortality associated with advanced organ support highlights the need for preventive strategies aimed at mitigating progression to respiratory and renal failure in this vulnerable population.
Limitations
Several limitations of this study should be acknowledged. First, the retrospective observational design precludes causal inference; therefore, the identified predictors should be interpreted as associations rather than direct determinants of ICU mortality. These variables may reflect the severity of critical illness rather than exert a causal effect on patient outcomes.
Second, this was a single-center study, which may limit the generalizability of the findings to other ICU settings with different patient populations, admission criteria, and clinical management protocols. Multicenter studies are warranted to validate these results across diverse healthcare systems.
Third, although key laboratory parameters at ICU admission were analyzed, data on chronic diabetes-related factors—such as HbA1c levels, duration of diabetes, and prior antidiabetic treatment—were not consistently available and could not be included. These factors may influence metabolic resilience and immune function during critical illness and should be considered in future prospective studies.
The use of single imputation rather than multiple imputation may have attenuated variance and influenced effect estimates; therefore, results should be interpreted cautiously.
Fourth, the study focused on short-term ICU mortality and did not assess post-discharge outcomes, long-term survival, or functional recovery. Consequently, the prognostic value of the identified predictors beyond the ICU stay remains uncertain.
Established ICU severity scores (e.g., SOFA, APACHE), detailed comorbidity indices, vasopressor use, and baseline renal function prior to admission were not consistently available and could not be incorporated into the multivariate model. As a result, residual confounding by illness severity cannot be excluded, particularly given the strong correlation between lactate levels, organ failure, and the need for intensive organ support.
Finally, some predictors included in the multivariate model, particularly mechanical ventilation and hemodialysis, should be interpreted as markers of advanced organ dysfunction and disease severity rather than direct causal factors. Their strong association with mortality reflects the extent of multisystem failure in critically ill patients with diabetes mellitus.
5. Conclusions
In this study of critically ill patients with diabetes mellitus, we identified a distinct set of biological and clinical factors associated with short-term ICU mortality. Diabetic patients who did not survive exhibited early signs of metabolic stress, immune dysregulation, and renal impairment at ICU admission, highlighting a state of increased vulnerability at the onset of critical illness.
Among the evaluated predictors, admission lactate levels and the need for advanced organ support, particularly mechanical ventilation and hemodialysis, emerged as independent determinants of ICU mortality. These findings underscore the importance of early biological assessment and close monitoring of diabetic patients at high risk of rapid clinical deterioration.
The model highlights clinically relevant markers associated with short-term ICU mortality; however, external validation and prospective evaluation are required before application for formal risk stratification. Future prospective and multicenter studies are needed to validate these findings and to explore targeted strategies aimed at mitigating metabolic and organ dysfunction in this vulnerable population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hossain M.J. Al-Mamun M. Islam M.R. Diabetes mellitus, the fastest growing global public health concern: Early detection should be focused Health Sci. Rep.20247 e 200410.1002/hsr 2.200438524769 PMC 10958528 · doi ↗ · pubmed ↗
- 2Antar S.A. Ashour N.A. Sharaky M. Khattab M. Ashour N.A. Zaid R.T. Roh E.J. Elkamhawy A. Al-Karmalawy A.A. Diabetes mellitus: Classification, mediators, and complications; A gate to identify potential targets for the development of new effective treatments Biomed. Pharmacother.202316811573410.1016/j.biopha.2023.11573437857245 · doi ↗ · pubmed ↗
- 3Hussain A. Chronic hyperglycemia and cardiovascular dysfunction: An in-depth exploration of metabolic and cellular pathways in type 2 diabetes mellitus Cardiovasc. Diabetol.–Endocrinol. Rep.2025113910.1186/s 40842-025-00247-341382274 PMC 12699840 · doi ↗ · pubmed ↗
- 4Abbas U. Kumar H. Hussain N. Ahmed I. Laghari R.N. Tanveer M. Hadif M. Fatima K. Khalid M.U. Anwar K. Immune dysregulation in type 2 diabetes mellitus: Implications for tuberculosis, COVID-19, and hiv/aids Infect. Med.2025410021110.1016/j.imj.2025.10021141216008 PMC 12596640 · doi ↗ · pubmed ↗
- 5Nishad S.S. Dongare D. Tripathi A.C.P. Tripathi T. Tripathi P. Deciphering the intricacies of immune system dysfunction and its impact on diabetes mellitus: Revisiting the communication strategies to manage diabetes mellitus Health Sci. Rev.20241310020110.1016/j.hsr.2024.100201 · doi ↗
- 6Daryabor G. Atashzar M.R. Kabelitz D. Meri S. Kalantar K. The effects of type 2 diabetes mellitus on organ metabolism and the immune system Front. Immunol.202011158210.3389/fimmu.2020.0158232793223 PMC 7387426 · doi ↗ · pubmed ↗
- 7Al-Hassani I. Khan N.A. Elmenyar E. Al-Hassani A. Rizoli S. Al-Thani H. El-Menyar A. The interaction and implication of stress-induced hyperglycemia and cytokine release following traumatic injury: A structured scoping review Diagnostics 202414264910.3390/diagnostics 1423264939682557 PMC 11640098 · doi ↗ · pubmed ↗
- 8Barmanray R. Cheuk N. Fourlanos S. Greenberg P. Colman P. Worth L. In-hospital hyperglycemia but not diabetes mellitus alone is associated with increased in-hospital mortality in community-acquired pneumonia (cap): A systematic review and meta-analysis of observational studies prior to COVID-19BMJ Open Diabetes Res. Care 202210288010.1136/bmjdrc-2022-002880 PMC 925786335790320 · doi ↗ · pubmed ↗