Pulp–Dentin Regeneration via Cell Homing: Current Evidence and Perspectives on Cell-Free Regenerative Endodontic Therapy
Michele Beco, Francesca Di Pasquale, Chiara Valenti, Paolo Betti, Gian Luca Mascolo, Lorella Marinucci, Stefano Eramo, Stefano Pagano

TL;DR
This paper reviews recent studies on cell-free regenerative endodontic therapy, which uses the body's own stem cells to regenerate pulp and dentin, offering a potential alternative to traditional root canal treatments.
Contribution
The study provides an updated analysis of recent human studies on CF-RET, highlighting its biological potential and the need for standardized clinical protocols.
Findings
In vitro studies show growth factors and biomimetic scaffolds enhance stem cell viability and odontogenic differentiation.
In vivo studies on immature teeth show positive outcomes like root development and canal diameter reduction.
Current evidence is limited by heterogeneity and lack of standardized protocols.
Abstract
Background and Objectives: The regeneration of the pulp–dentin complex represents an alternative to conventional root canal treatment, aiming to preserve tooth biology and function. Cell-free regenerative endodontic therapy (CF-RET) exploits endogenous stem cells from the periapical region without ex vivo cell manipulation. Despite growing interest, the biological mechanisms, clinical indications, and predictability of CF-RET remain not clearly defined. This structured narrative review aimed to update a previous review by analyzing recent human studies on CF-RET. Materials and Methods: This review was conducted using the PRISMA 2020 guidelines to guide transparent reporting of the literature search and study selection process and was registered in PROSPERO (CRD420251075131). In vitro and in vivo human studies published between January 2017 and December 2024 investigating CF-RET were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
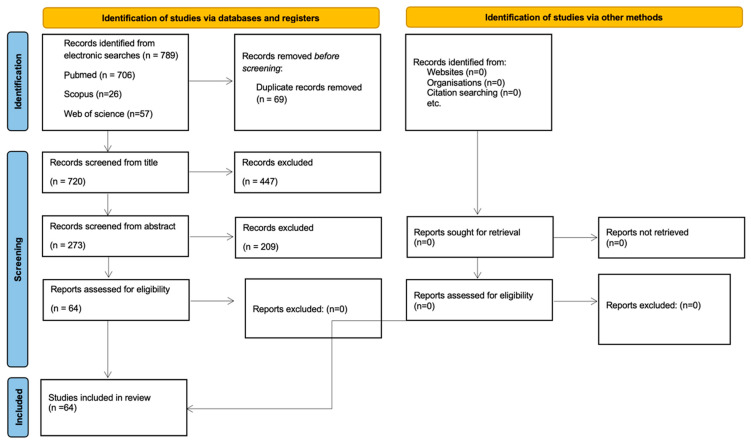 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndodontics and Root Canal Treatments · Dental Trauma and Treatments · Periodontal Regeneration and Treatments
1. Introduction
The regeneration of the pulp–dentin complex is an ambitious technique aimed at regenerating pulp tissue and has been extensively investigated to achieve predictable and clinically applicable outcomes. Chemical or mechanical agents, such as caries, exposed dentin, dental trauma, recent dental treatments, or inadequate restorations, can lead to pulpitis, an inflammation of the dental pulp. Clinically, pulpitis is distinguished as reversible or irreversible based on the reversibility of the inflammatory process.
Irreversible pulpitis necessitates treatment to remove the affected pulp and its replacement with an inert material. Root canal treatment (RCT), despite adherence to the standard procedure, is associated with a percentage of failures and adverse events, attributed to microbial factors stemming from persistent or secondary root canal infections, extra-radicular infections originating from the periapical lesion caused by pulpal pathology, or non-microbial extrinsic factors [1].
Due to the loss of nerve fibers within the pulp following RCT, the patient cannot perceive thermal, electrical, or osmotic stimuli as if the tooth were vital and thus loses the ability to sense potential active pathological conditions. The capacity for the generation of secondary or tertiary dentin is also lost, as odontoblasts are removed during RCT, and endodontically treated teeth are more vulnerable to masticatory forces [2]. Dental caries and traumatic injuries can also affect immature teeth and, similarly to teeth with complete root formation, can lead to pulpal necrosis [3]. In immature teeth, the removal of odontoblasts prevents complete root development. Teeth treated with RCT before root development is complete remain with shorter roots and larger apical foramina. Currently, pulp revascularization is employed to facilitate the complete development of the tooth roots.
The pulp revascularization technique is based on, once the root canal has been disinfected with a combination of antibiotics or calcium hydroxide, inducing bleeding from the apical papilla with a file to allow the formation of a blood clot within the root canal. This process facilitates the migration of stem cells that can differentiate and produce dentin and ultimately leading to the completion of root development. Stem cells, present in large numbers in the periapical tissue, can differentiate into various cell types: osteo/odontogenic, neurogenic, and other lineages, such as chondrocytes and even adipocytes [4]. It has been hypothesized that the blood clot acts as a scaffold that facilitates the migration and engraftment of stem cells [5]. The blood clot is sealed within the root canal using mineral trioxide aggregate (MTA) or other bioactive endodontic cements [6]. However, the formation of this blood clot does not equate to the regeneration of an organized pulp tissue within which blood vessels and nerves. A histological examination with hematoxylin and eosin staining reveals the presence of connective tissue, fibroblasts, and blood vessels with few lymphocytes and an absence of odontoblasts [7]. Dentin development is arrested, and the thickness of the walls increases due to the formation of an ectopic, irregular cementum-like tissue on the surface of the root canal walls. In some specimens, a soft tissue, such as the periodontal ligament, where Sharpey’s fibers can also be identified, forms along this ectopic cementum. A regular layer of odontoblasts rarely forms, while bone bridges may develop within the canal [8]. A histological analysis conducted in one study revealed that only 53% of the roots in the four experimental groups (with previously infected canals) exhibited new hard tissue deposition on the internal root canal walls. Therefore, revascularization does not equate to regeneration but, rather, to tissue repair [9].
Currently, the regenerative approaches targeting the pulp–dentin complex can be broadly distinguished according to the origin of the cells involved. A recent classification [10] differentiates these strategies into cell-based regenerative endodontic therapy (CB-RET) and cell-free regenerative endodontic therapy (CF-RET). In CB-RET, stem cells derived from the host (autologous) or donors (allogeneic) are transplanted into the root canal following ex vivo expansion, with the aim of directly repopulating the pulp space and achieving true tissue regeneration. Despite its theoretical advantages, this approach presents significant limitations, including unpredictable cell availability, a risk of contamination, immune rejection, high costs, and regulatory barriers associated with ex vivo cell manipulation [11].
In contrast, CF-RET relies on the recruitment of endogenous stem and progenitor cells, primarily from periapical tissues, through cell-homing mechanisms. This strategy employs intracanal scaffolds, bioactive molecules, and/or endogenous growth factor release to stimulate cell migration, proliferation, and differentiation within the disinfected root canal, without the need for cell transplantation. CF-RET is, therefore, conceptually distinct from CB-RET and is considered more clinically feasible [10].
Conventional revascularization procedures, although often grouped under the umbrella of regenerative endodontics, differ fundamentally in their intended biological mechanism and outcome. These techniques primarily aim to induce bleeding into the root canal to promote tissue ingrowth and resolution of infection, frequently resulting in reparative tissues such as connective tissue, cementum-like tissue, or bone, rather than the consistent regeneration of a functional pulp–dentin complex.
Despite the clinical appeal of CF-RET, important uncertainties remain regarding the specific cell populations involved in tissue formation and whether stem cell recruitment originates exclusively from the apical region [12]. Moreover, current evidence does not demonstrate significant differences between CF-RET and CB-RET in terms of apical bone healing and findings related to tooth maturation remain conflicting. While CB-RET has been associated with more complete pulp-like tissue formation, CF-RET outcomes have occasionally shown altered or non-native tissue organization. However, the literature currently provides limited material on the evaluation of these aspects, which necessitate a histological approach [13]. Notably, none of the previously published works specifically focus on CF-RET by collecting both in vivo and in vitro studies but, rather, exclusively concentrate on individual aspects mentioned above, offering a simple comparison between the two studied regeneration methods [11].
The aim of the present structured narrative review was to update and supplement a 2017 work by Eramo et al. with the most recent in vitro and in vivo studies on CF-RET [14]. This review intends to provide an overview of the CF-RET method, stem cells, growth factors, and materials used for scaffolds in pulp–dentin regeneration, analyzing the advancements in in situ pulp revascularization, evaluating whether the fundamental principles guiding research remain the same, the mode of stem cell migration into the root canal, the conditions for migration, proliferation, and attachment, and the various growth factors that promote this process and support the potential complete regeneration of the pulp.
2. Materials and Methods
This structured narrative review was conducted using the preferred reporting items for systematic review and meta-analysis (PRISMA 2020 statement) as a reporting framework to ensure the transparency and reproducibility of the literature search and study selection process [15]. A PRISMA flow diagram (Figure 1) was used to report the study inclusion process. The review protocol was registered in the PROSPERO database (CRD420251075131) to enhance methodological transparency and avoid unnecessary duplication, despite the narrative nature of the evidence synthesis. The Population, Inclusion, Comparison, Outcome, and Study design (PICOS) format was used to structure the research question and eligibility criteria (Table 1), based on the following question: “What is the current state of knowledge regarding the effects of CF-RET or cell-homing technique on human cell populations?”, without the intent of performing quantitative synthesis. This review is an update to a previous study [14].
The search for articles was conducted in MEDLINE (via PubMed) using the following combination of terms: ((((“Regenerative Endodontics” [Mesh] OR “Pulp regeneration” [All Fields]) AND (“Cell-Free Regenerative Endodontic Therapy” [All Fields] OR “CF-RET” [All Fields]) OR “Cell homing” [All Fields] OR “cell-free” [ All Fields] OR “endogenous stem cells” [All Fields] OR “stem cell recruitment” [All Fields])) AND (“scaffold” [All Fields] OR “growth factor *” [All Fields] OR “PRF” [All Fields] OR “PRP” [All Fields] OR “CGF” [All Fields])) NOT (Systematic Review [Publication Type] OR Review [Publication Type] OR Meta-Analysis [Publication Type] OR Congress [Publication Type] OR Editorial [Publication Type] OR Case Reports [Publication Type] OR Clinical Conference [Publication Type] OR Comment [Publication Type] OR Consensus Development Conference [Publication Type])) AND ((“1 January 2017” [Date—Publication]: “31 December 2024” [Date—Publication]))). The terms were adapted for the Scopus and Web of Science databases. Only articles in English or Italian were considered.
Studies published between 2017 and 2024 on CF-RET, in vitro and in vivo, considering the use of stem cells, possibly associated with scaffolds, cytokines, or additional treatments essential for completing pulp regeneration, were included.
Exclusion criteria: Studies on non-human cell populations, case reports, review articles, editorials, opinions, surveys, guidelines, conferences, and commentary articles. Studies without original and/or actual data, studies on cell transplantation, on therapies for vital pulp, on materials with biological effects on dentine or stem cells but without reference to pulp regeneration via cell homing, or on regeneration of tissues other than pulp or dentine. Studies with no full text available.
Screening was performed in three stages, based on the title and abstract, and then by a reading of the full text of the articles that potentially met the inclusion criteria. Electronic searches were followed by a manual search of the reference lists of included articles. At each stage, two reviewers (MB and SE) independently assessed each article. The PRISMA flow diagram (Figure 1) was used to report the studies included and excluded with justification.
The titles of all articles that were initially retrieved were screened according to eligibility criteria, and duplicates were removed. Two independent reviewers assessed the titles, and those that were not relevant were excluded. Articles compatible with the inclusion criteria were selected for further review, and abstracts were analyzed. The full texts of potentially eligible studies were reviewed against the inclusion/exclusion criteria independently by the reviewers, and any disagreements were solved through discussion or consultation with the other authors (SP and CV).
Scientific and technical information was collected in two evidence tables using Microsoft Office Excel, including in vitro and in vivo studies, with information on: the author(s) and year of publication, the study population (cell lines or patients), the CF-RET intervention, biological effects, the assay used and the conditions, and the principal findings. For data analysis, a narrative approach was adopted.
Two independent reviewers (MB and FDP) carried out the quality assessment of the included studies using a Quality Assessment Tool with diverse studies (QuADS) [16]. The QuADS tool was used to describe the methodological quality and reporting completeness of the included studies across different designs. Quality scores were not used to weight, exclude, or stratify studies, in line with the narrative nature of the evidence synthesis. This evaluation tool examines the methodological quality of the included studies and the extent to which a study addressed the possibility of bias in its design. The QuADS tool considered details on the rationale and aim, subjects and setting, study design, sampling and recruitment, data collection, exposure measurements, analysis methods selected, stake-holder involvements and limitations. These 13 evaluation criteria were rated on a scale from 0 to 3 (0: absence of the element; 1: very limited presence of the element; 2: moderate presence of the element; and 3: complete and adequate presence of the element).
3. Results
The flow diagram of screened studies (Figure 1) shows a total of 789 potentially eligible studies following the electronic search. Reviewer agreement and duplicate removal led to the elimination of 69 articles; title screening was completed on 720 studies, resulting in 447 non-eligible studies being excluded at this stage. Abstract screening was completed using 273 studies, with 64 progressing to full-text review. Finally, 64 studies were included in the full data analysis, and 0 studies were excluded after full-text reading [17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78]. One study was included in both the in vitro studies section and the in vivo studies section [9].
3.1. In Vitro Studies
Sixty papers were included in this narrative review, primarily investigating the behavior of dental stem cells SCAPs or DPSCs by supplementing the culture with specific molecules acting as growth factors to identify readily available and clinically applicable molecules that can enhance cellular viability. The most consistently evaluated outcomes included cell viability, migration, mineralization, and osteogenic/osteoblastic differentiation, all of which are considered fundamental parameters for successful pulp regeneration. In addition to determining the optimal concentration to elicit the desired effects, the studies investigating the role of growth factors have also aimed to find a simple and safe method for their activation, as well as a secure and clinically reliable delivery system [31,57,66]. At the concentrations used, all studies demonstrate the cellular differentiation of the stem cells, which is essential for the regeneration process [17,33,36,42,72], and the induction of new angiogenesis, which could facilitate the vascularization of the pulpal tissue [50,51,52,63,67,70,73].
Neurogenic differentiation, which is critical for establishing new innervation in the neo-formed pulpal tissue, was less frequently addressed and was reported in only three studies employing specific scaffold formulations [61,70,73]. Nevertheless, all scaffold-based approaches demonstrated satisfactory biocompatibility. Conversely, several studies have investigated the molecular mechanism of action through gene regulation to either activate or suppress specific genes responsible for cellular differentiation with the aim of elucidating how growth factors influence the regenerative process [26,34,41,46,60,63]. In addition, increasing attention has been directed toward stem cell–derived exosomes, which consistently enhanced cell viability, proliferation, migration, angiogenesis, and odontogenic differentiation [21,27,61,64,67,74,79,80,81]. Cell migration rate emerged as a recurring functional parameter that is fundamental because it plays a homeostatic role in tissue maintenance and is crucial for the regeneration of damaged organs and tissues. All studies included have reported favorable results in enhancing the migration of stem cells [27,29,48].
Finally, extensive research focused on the structural and biological optimization of scaffolds, evaluating cytotoxicity, proliferation, migration, odontogenic, and neurogenic differentiation to better replicate the dental pulpal microenvironment [32,39,40,44,45,49,59,62,65,68,70,73]. Furthermore, several studies demonstrated that biologically incorporating substances like growth factor into scaffold matrices significantly increased their regenerative performance [22,23,24,35,39,40,50,53,55,56,69,71]. Platelet-based scaffolds, obtained through autologous blood centrifugation, were also widely investigated to establish the ideal formulation for CF-RET success [19,38,47,52].
The data extraction of the included in vitro studies is reported in Table 2.
3.2. In Vivo Studies
Five papers were included in this narrative review, all investigating clinically applicable scaffold strategies for pulp regenerative procedures in traumatized necrotic immature teeth. Most studies focused on platelet-based scaffolds like i-PRF (injectable platelet-rich fibrin) and PRP (platelet-rich plasma) obtained through various centrifugation protocols, with the aim of identifying a material suitable for root canal application [75].
Overall, the available clinical evidence has consistently demonstrated a positive effect of platelet concentrates on regenerative outcomes.
Root development (assessed by measuring root length and canal diameter) [76,77,78], along with clinical presentation [77,78], showed significant results. No significant difference was found between groups except for the apical canal diameter (i-PRF showed significantly greater decrease in apical canal diameter than PRP) [75].
Beyond scaffold form, adjunctive biological factors were explored in a limited number of studies. Only one in vivo investigation quantified endogenous TGF-β, an essential growth factor released from the teeth following different irrigation protocols [9], highlighting its potential clinical relevance due to ease of application compared to other factors. Additionally, concentrated growth factor (CGF) supplementation was shown to provide clinically meaningful improvements when compared with non-supplemented scaffolds [78].
The data extraction of the included in vivo studies is reported in Table 3.
3.3. Quality Assessment Score
All the 64 articles included met the criteria of the quality assessment, resulting in reliability with a low risk of bias (Supplementary Table S1). The highest score was 36/36 [9,75], and the lowest was 18/36 [35]. The variability in methodological quality observed among the included studies, as highlighted by the QuADS assessment, underscores the need for a cautious interpretation of the findings, particularly given the heterogeneity of experimental models, interventions, and outcome measures. Consequently, the methodological appraisal should be considered supportive and interpretative, rather than definitive.
4. Discussion
The previous review by Eramo et al. [14] established that several cytokines, alone or in combination, have the potential to induce key biological effects (migration, proliferation, and differentiation) in dental stem cells and that various cell-homing molecules had successfully promoted pulp-like connective tissue formation in in vivo experiments [79,80]. However, it also concluded that dental pulp regeneration via cell homing still requires further investigation.
In line with topics addressed in previous studies, stem cell factors (SCFs) continue to be a major focus of investigation. They are considered potent chemokines involved in progenitor cell recruitment, as they have been observed in abundance at repair sites and are widely used in tissue engineering applications [54]. Consequently, most of the studies included aimed to identify molecules capable of mimicking the action of growth factors in order to enhance the ability of stem cells to reconstitute pulp tissue during CF-RET. Concentrated growth factor (CGF), the most recent generation of platelet concentrate products, is the most extensively investigated among the studies included in this structured narrative review. CGF contains key growth factors, including PDGF-BB, IGF-1, TGF-β1, bFGF and VEGF, which are released from platelets or autologous leukocytes, and is characterized by a fibrin network similar to that found in native tissues. These properties confer significant clinical potential [30], including the ability to promote pulp revascularization and increase root wall thickness [81,82].
The use of endogenous growth factors has also been shown to simplify clinical application, as they can be released from dental and periodontal tissues. In this context, dentin-derived matrix proteins have been reported to induce cell migration, regulate cell growth, and promote the differentiation of dental pulp cells [83]. However, the use of exogenous growth factors to stimulate healing remains associated with several technical and regulatory limitations, including high costs and potential safety concerns.
Among dentin-derived growth factors, TGF-β has been widely investigated due to its ability to modulate cell proliferation, differentiation, adhesion and migration. It can be applied at specific concentrations, which have yet to be fully defined, both exogenously and endogenously, and may be released from dentine walls by commonly used root canal irrigants, such as EDTA [9].
Although approaches involving platelet-derived concentrates, including CGF, are frequently investigated, the number of available studies does not necessarily correspond to the strength of evidence or clinical superiority. Most supporting data derive from in vitro experiments or small clinical series, which limits the robustness and generalizability of the reported findings.
To appropriately interpret these outcomes, it is essential to distinguish between true pulp–dentin regeneration and reparative or revascularization processes. A critical distinction in regenerative endodontics is that between true pulp–dentin complex regeneration and tissue repair or revascularization. True regeneration implies the re-establishment of an organized pulp tissue containing functional vasculature, neural elements, and a polarized odontoblast layer capable of physiological dentin deposition. In contrast, revascularization and repair typically result in the ingrowth of connective tissue, cementum-like or bone-like structures and limited or absent odontoblastic organization. When the in vivo human studies included in the present review are evaluated against this histological benchmark, it becomes evident that most outcomes are inferred from clinical and radiographic parameters, such as root lengthening, canal wall thickening, and periapical healing, rather than from direct histological evidence. While these findings indicate biological activity and functional improvement, they do not conclusively demonstrate the regeneration of a native pulp–dentin complex.
Critical insight into the nature of tissues formed after CF-RET is provided by seminal animal studies employing histological evaluation. In a well-characterized canine model, Palma et al. [84] demonstrated that regenerative endodontic procedures based on cell homing predominantly resulted in the formation of highly vascularized connective tissue associated with intracanal cementum-like deposits and, in some cases, bone-like tissue within the root canal space, rather than a structured pulp–dentin complex. Only limited and localized areas showed dentin formation with odontoblast-like cells, indicating that true pulp regeneration occurred inconsistently and was not the prevailing outcome. These histological findings are particularly relevant when interpreting clinical and radiographic success parameters reported in human studies, such as root lengthening, canal wall thickening, and apical closure. While these outcomes reflect biological activity and functional improvement, animal evidence suggests that they often arise from reparative processes involving cementogenesis or osteogenesis, rather than restoration of native pulp tissue architecture. Taken together, translational evidence from animal models indicates that CF-RET currently achieves reliable resolution of infection and promotion of tissue ingrowth but does not consistently fulfill the histological criteria of true pulp–dentin complex regeneration. This distinction is essential for avoiding overinterpretation of clinical success and for guiding future research toward strategies that promote organized pulp tissue formation, including innervation and odontoblast layer re-establishment.
It is also important to consider studies that have proposed the use of suitable scaffolds designed to provide stem cells with a regenerative microenvironment capable of mimicking the complex structure of dental pulp, thereby supporting stem cell development and proliferation. The use of materials such as decellularized human pulp [70,73], or dentine [62,65] has proven to be a successful strategy. These materials retain some of the natural properties of dental tissue by releasing bioactive substances and factors that promote regeneration, contributing to the creation of biomimetic environments that exploit the molecules responsible for the tooth’s innate self-repair capabilities and biological functions, including proliferation, migration, and odontogenic and neurogenic differentiation [85].
In addition, a careful evaluation of the scaffold microstructure and rheological properties is essential, as the physical and structural characteristics, such as substrate stiffness and geometry, directly influence cell behavior and their capacity to differentiate into multiple cell lines. In this context, photolithography has been used to fabricate a micropatterned substrate that encourages cells to adopt morphologies resembling odontoblasts, as their elongated shape, the presence of cellular processes, and palisade-like alignment appear to be fundamental to tooth physiology and the mineralizing phenotype [25,28]. Notably, Bordini et al. developed a physiologically relevant model using organoids to simulate dental pulp conditions without the need for animal models [22,23].
The review by Eramo et al. reported that odontoblastic and neural tissue regeneration has been achieved in only a limited number of studies, whereas current in vitro investigations more consistently focus on mineralization and the presence of odontoblasts through established assays. However, the standardization of methodologies aimed at evaluating nerve fiber formation and neurogenic regeneration remains a significant challenge. This suggests that, despite substantial progress in characterizing the dentin-forming phenotype, the complex requirements necessary to achieve functional pulp innervation are still incompletely understood and require more consistent and standardized experimental protocols in the scientific literature.
The findings of the present review should also be interpreted in the context of the systematic review and meta-analysis by Meschi et al. [86], which evaluated the clinical effectiveness of revitalization procedures in necrotic mature and immature permanent teeth. That analysis, based on a limited number of randomized and non-randomized clinical studies, reported no statistically significant differences in survival or success between revitalization and conventional endodontic treatments and rated the certainty of evidence as low to very low. These conclusions align with our observation that, despite encouraging biological and early clinical signals, the current human evidence does not support definitive clinical recommendations for regenerative endodontic therapies beyond carefully selected cases. Importantly, while the review by Meschi et al. focused on clinical outcomes of revitalization as a treatment modality, the present review addresses a complementary aspect by synthesizing recent in vitro and in vivo human studies specifically investigating cell-free regenerative endodontic strategies. Our findings, therefore, primarily inform biological feasibility, mechanistic understanding, and translational potential, rather than clinical effectiveness, which remains insufficiently supported by robust long-term evidence.
With regard to in vivo studies, compared with previous research, the present review identified clinical investigations that primarily focused on immature teeth, reporting improved outcomes in the main parameters evaluated. Previously, studies have suggested that the success of pulp regeneration depends on the clinical and biological conditions of the tooth, with cell-homing strategies not being equally effective in all scenarios, such as cases of pulp necrosis. Consequently, root canal treatment remains the standard of care for mature teeth with necrotic pulp and closed apices [14]. Consistent results for these specific clinical conditions have not yet emerged from the in vivo studies analyzed in this review.
More recently, in vivo investigations have begun to focus on clinical situations in which this type of therapy is both feasible and more likely to be successful, taking into account the initial condition of the tooth. Teeth from young patients that are not yet necrotic and present a larger exposed dentin surface release greater amounts of TGF-β, which can be exploited for regenerative purposes [9] and may be suitable for CF-RET treatment. To date, in vivo human studies on CF-RET have predominantly focused on immature teeth with incomplete root development; however, this trend reflects the current direction of clinical research, rather than definitive evidence, limiting the applicability of CF-RET to this patient group.
Although the available evidence indicates promising biological potential, its translational strength remains limited and is not yet applicable to routine clinical practice. Further studies are, therefore, required to investigate CF-RET in both immature and mature teeth and to clearly distinguish biological feasibility from clinical predictability. At present, evidence in immature teeth supports biological plausibility, rather than reliable and reproducible clinical outcomes, highlighting the need for dedicated clinical studies in adult patients with fully developed roots to expand the therapeutic indications of CF-RET.
Despite the significant progress made since the publication of Eramo et al., particularly in the development of biomimetic scaffolds and in the understanding of molecular mechanisms, a critical question remains unresolved. Although the reviewed studies collectively support the biological feasibility of CF-RET, the heterogeneity of study designs and the predominance of in vitro evidence limit the strength of clinical inferences. The current findings should, therefore, be interpreted as indicative of regenerative potential, rather than as proof of predictable clinical effectiveness. While both in vitro and in vivo results are encouraging, standardized protocols for CF-RET procedures in humans are still lacking. Such protocols are essential to ensure consistent reproducibility across different clinical settings and operators, which is a prerequisite for the safe and effective application of CF-RET.
Moreover, substantial variability in experimental conditions, scaffold composition, growth factor concentrations, and outcome assessment across studies hampers direct comparison and weakens the overall consistency of the evidence. Consequently, although biological feasibility is well supported, the clinical translatability of CF-RET remains confined to selected scenarios (primarily immature teeth) and should be regarded as investigational, rather than predictive of routine clinical success.
Study Limitations
Although this review incorporated structured methodological elements such as protocol registration in PROSPERO, a predefined search strategy, and transparent reporting of study selection, it was ultimately conducted as a structured narrative review. This approach was justified by the substantial heterogeneity of the included studies, which precluded meaningful quantitative synthesis or meta-analysis. PRISMA 2020 guidelines were used to guide reporting of the search and selection processes, while PROSPERO registration was undertaken to ensure methodological transparency and avoid duplication. Consequently, the evidence was synthesized using a qualitative, narrative approach.
A major limitation of this review is the pronounced heterogeneity in methodologies and reported outcomes across the included studies. This variability limited the feasibility of statistical aggregation and meta-analyses. In addition, only a small number of in vivo human studies were available, all of which focused on immature teeth, thereby restricting the generalizability of the findings.
The methodological quality of the included studies, assessed using the QuADS tool, also showed considerable variability. Differences in study design, reporting completeness, and experimental approaches indicate that the findings should be interpreted with caution, particularly when extrapolating in vitro results to clinical contexts.
Another limitation is the absence of studies systematically investigating the combined use of multiple key components of CF-RET, such as scaffolds, growth factors, and endogenous stem cells’ recruitment, either in vitro or in vivo. Consequently, the relative contribution of each component and the potential synergistic effects of specific combinations remain poorly understood. In addition, few studies incorporated microbiological analyses to evaluate scaffold-related bacterial growth alongside stem cell proliferation [24], and only a limited number examined cell morphology, spatial organization, or the use of scaffolds derived from natural and appropriately processed human tissues.
Finally, ethical constraints severely limit the feasibility of histological validation of regenerated tissues in human teeth, representing a major challenge in the interpretation of clinical regenerative endodontic studies. As a result, current evidence supporting CF-RET largely reflects reparative or revascularization processes, rather than confirmed true pulp–dentin complex regeneration. This underscores the need for caution when interpreting regenerative claims.
Future translational research should aim to bridge this gap by integrating advanced imaging, molecular markers, and validated surrogate endpoints that more accurately reflect pulp tissue organization and functionality, to determine whether emerging CF-RET strategies can consistently achieve true regeneration, rather than tissue repair alone.
An additional constraint of the present structured narrative review is the inclusion of studies combining stem cells with specific molecules or microcapsules. This is relevant because, unlike CB-RET, CF-RET relies on endogenous cells migrating from periapical tissues, rather than the direct placement of cells into the root canal in combination with scaffolds and growth factors [71].
5. Conclusions
In recent years, interest in developing a valid alternative to the conventional treatment of necrotic teeth has increased substantially. In vivo studies evaluating materials previously investigated in vitro have reported encouraging clinical and radiographic outcomes, suggestive of pulp–dentin tissue formation. However, further studies are clearly required to establish standardized methodologies and clinical guidelines for regenerative endodontic therapy, as well as to assess long-term outcomes. CF-RET represents a promising regenerative strategy, particularly in immature teeth with incomplete root development. Nevertheless, its broader clinical application remains investigational and is not yet supported by robust, long-term clinical evidence.
The heterogeneity observed in reported outcomes and clinical indications is further reflected in recent multinational surveys demonstrating substantial variability in RET adoption. These findings highlight the need for standardized clinical protocols, targeted professional training, and well-designed translational and clinical studies to support the safe and predictable implementation of CF-RET in clinical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Siqueira J.F.Jr. Aetiology of root canal treatment failure: Why well-treated teeth can fail Int. Endod. J.20013411010.1046/j.1365-2591.2001.00396.x 11307374 · doi ↗ · pubmed ↗
- 2Goto Y. Ceyhan J. Chu S.J. Restorations of endodontically treated teeth: New concepts, materials, and aesthetics Pract. Proced. Aesthetic Dent.200921818919583165 · pubmed ↗
- 3Singh R.K. Shakya V.K. Khanna R. Singh B.P. Jindal G. Kirubakaran R. Sequeira-Byron P. Interventions for managing immature permanent teeth with necrotic pulps Cochrane Database Syst. Rev.20176 CD 01270910.1002/14651858.CD 012709 · doi ↗
- 4Kang J. Fan W. Deng Q. He H. Huang F. Stem Cells from the Apical Papilla: A Promising Source for Stem Cell-Based Therapy Biomed. Res. Int.20192019610473810.1155/2019/610473830834270 PMC 6374798 · doi ↗ · pubmed ↗
- 5Thibodeau B. Trope M. Pulp revascularization of a necrotic infected immature permanent tooth: Case report and review of the literature Pediatr. Dent.200729475018041512 · pubmed ↗
- 6Staffoli S. Plotino G. Nunez Torrijos B.G. Regenerative Endodontic Procedures Using Contemporary Endodontic Materials Materials 20191290810.3390/ma 1206090830893790 PMC 6471897 · doi ↗ · pubmed ↗
- 7Torabinejad M. Faras H. A clinical and histological report of a tooth with an open apex treated with regenerative endodontics using platelet-rich plasma J. Endod.20123886486810.1016/j.joen.2012.03.00622595129 · doi ↗ · pubmed ↗
- 8Wang X. Thibodeau B. Trope M. Lin L.M. Huang G.T. Histologic characterization of regenerated tissues in canal space after the revitalization/revascularization procedure of immature dog teeth with apical periodontitis J. Endod.201036566310.1016/j.joen.2009.09.03920003936 · doi ↗ · pubmed ↗