Fasting and Nutrition as Promising Treatment Strategies for Women with Rheumatoid Arthritis in Transitional Hormonal Stages
Bérénice Hansen, Evdokia Alvanou, Maria Angeliki S. Pavlou, Paul Wilmes, Jochen G. Schneider

TL;DR
This paper reviews how fasting and nutrition can help manage rheumatoid arthritis in women during hormonal transitions like menopause.
Contribution
It highlights fasting and plant-based diets as promising complementary strategies for RA management during hormonal changes.
Findings
Fasting may reduce inflammation and modulate immune activity in RA patients.
Plant-based diets could improve gut health and reduce oxidative stress linked to RA.
Nutritional interventions may support better disease outcomes during hormonal transitions.
Abstract
Rheumatoid arthritis (RA) is a systemic and chronic autoimmune disease affecting about 1% of the global population, with a higher prevalence in women. Its treatment has been improved greatly over the past 30 years but there is no definitive cure available, and another unmet need exists for transitional hormonal stages such as pregnancy or menopause, which spurs the need to research new therapy options. In recent years, dietary interventions, particularly fasting and plant-based nutrition, have gained attention for their potential to alleviate RA symptoms. Fasting has been shown to reduce systemic inflammation, promote autophagy, and modulate immune cell activity, possibly leading to decreased joint pain and swelling. Nutritional strategies, such as anti-inflammatory and plant-based diets, have been shown to impact the gut microbiome and potentially support weight management, improve…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
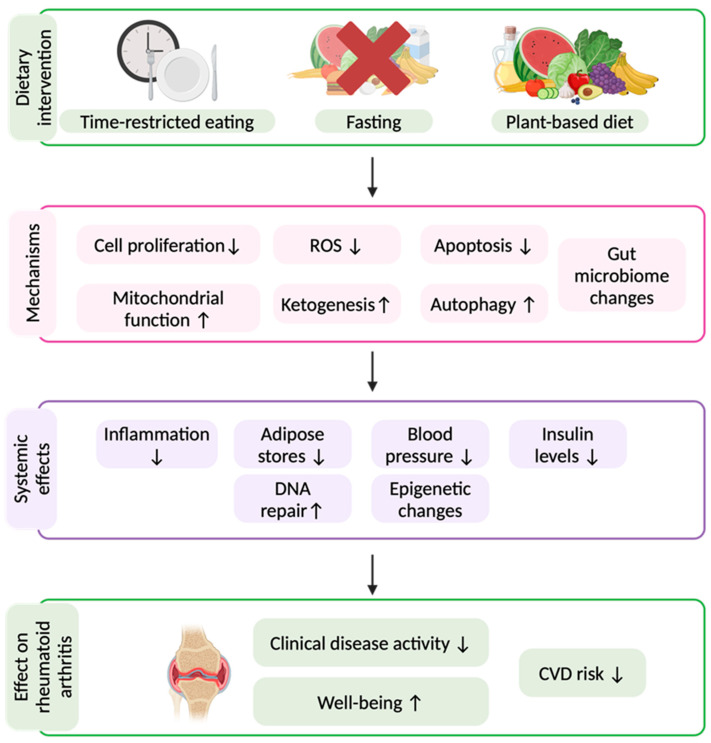 Figure 1
Figure 1- —Luxembourg National Research Fund (FNR)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDietary Effects on Health · Pregnancy and Medication Impact · Rheumatoid Arthritis Research and Therapies
1. Introduction
Modern healthcare has increasingly improved in terms of novel drugs and pharmaceutical advances, leading to significant improvements in lifespan and quality of life. However, side effects are also common, and treatment strategies are not always as efficient as desired [1,2]. Lifestyle adaptations and disease prevention rather than treatment, e.g., dietary strategies, are greatly underappreciated [3]. The typical Western diet and lifestyle have contributed to a rise in non-communicable diseases (NCDs), including autoimmune diseases (AIDs), with more patients depending on pharmacological treatments [4,5]. In AIDs, tissue damage leads to disruption of functions of the affected organs [6]. Rheumatoid arthritis (RA) is a systemic and chronic inflammatory AID [7]. The prevalence of RA is about 0.5 to 1.1% of the general population of industrialised countries, with a lower incidence in Southern Europe, and a generally higher prevalence among women, with the ratio being 2-3/1 (1a 3a) [8].
RA most commonly presents with articular inflammation, which can follow three distinct clinical patterns: (1) the most prevalent form is insidious onset of synovitis affecting the small joints of the extremities; (2) a subacute onset, which involves similar localisation but is accompanied by more pronounced systemic symptoms; and (3) a less frequent variation characterised by acute onset of monoarticular disease. RA mostly manifests in genetically predisposed people, such as in those with a HLA-DR4-positive genotype, who develop an immune response to post-translational modified proteins. A very common post-translational modification is citrullination of proteins in mammals, which is promoted by smoking and oral infections. The subclinical phase of the disease can last several years. It may lead to inflammation of the synovial membrane of the joints with increased production of metalloproteinases that cause cartilage degradation, bone loss, and marginal erosions of the joints. Besides the articular features, RA can have accompanying hematologic, ocular, pulmonary, cardiac, renal, and cutaneous manifestations. It is often associated with cardiovascular diseases, mood disturbances, fibromyalgia, and other comorbidities [7,9].
Various treatment strategies, such as non-steroidal anti-inflammatory agents (NSAIDs), corticosteroids, and disease-modifying anti-rheumatic drugs (DMARDs) are available. However, these drugs have significant inconveniences [9]. NSAIDs and corticosteroids are commonly used during acute outbreaks to rapidly relieve symptoms, but potentially cause gastrointestinal complications, cardiovascular risks, and immune suppression. DMARDs, used in long-term treatment strategies, vary in efficacy and often require prolonged use before therapeutic benefits are manifested [8,9].
Despite these different treatment options, responsiveness is not always obtained and only a small percentage achieve sustained remission [9,10,11]. Additionally, these medications are often unsuitable for pregnant women, especially in the third trimester, further emphasising the urgent need for alternative treatment approaches, such as nutrition and lifestyle interventions [9].
Lifestyle factors such as nutrition, exercise, sleep, and stress have been increasingly recognised as key players in health and well-being [12]. Specifically nutritional intervention strategies, like dietary composition, combined with meal timing, have been of interest in NCD prevention and treatment. Plant-based diets and fasting have been previously reported to show promising beneficial effects in RA; however, research is sparse and understanding of precise mechanisms is lacking [13]. Conversely, Western dietary patterns, characterised by high intake of red meat, refined sugars, and saturated fats, have been linked to a higher risk of RA [5]. Additionally, emerging evidence suggests that time-restricted eating (TRE), a form of intermittent fasting (IF), may influence inflammation and immune regulation in RA [14]. IF is defined as repetitive fasting periods lasting up to 48 h each, and TRE is a dietary regimen where the consumption of food is limited to a defined period of time during a 24 h window, resulting in a daily fasting window of at least 14 h [15].
2. Rheumatoid Arthritis During Critical Life Phases of Women
As previously mentioned, the RA incidence is higher in woman than in men, which is generally the case for AIDs. Several studies have tried to explore sex discrepancy, but without coming to a conclusive outcome. One hypothesis is that sex hormones might play a key role in the higher prevalence of AIDs in women [16]. Different forms of oestrogen act via their specific oestrogen receptor (ER)-alpha and ER-beta, which are also present on immune cells such as dendritic cells, B cells, and T cells [6]. Through these specific ERs, oestrogens can increase antibody production in females by promoting activation and class switch recombination of B cells [17].
Another hypothesis for the higher AID prevalence in women is linked to the X-chromosomes, as the prevalence for certain AIDs has a higher occurrence in Klinefelter (XXY) and Triple X (XXX) syndromes, while conditions like Turner syndrome (XO) show a lower risk [18]. A review published in 2023 on the higher prevalence of lupus in women explains this by three potential hypotheses: (1) non-random X-chromosome inactivation, (2) incomplete silencing of specific genes on the X-chromosome, (3) or the potential activation of the immune system by the X-Inactive-Specific Transcript ribonucleoprotein complex [18]. This higher prevalence in females introduces unique challenges in the treatment of AIDs, as women face hormonal fluctuations across their lifetime. The hormonal fluctuations across the menstrual cycle, pregnancy, and menopause are often accompanied by changes in immune function and inflammation and significantly impact the disease symptoms and the patient’s well-being [19]. While higher oestrogen levels, as seen during pregnancy, may temporarily attenuate inflammation, decreased oestrogen levels during menopause are associated with increased T cell activation, including enhanced Th17 response [20]. The menstrual cycle has a profound impact on pain perception, and especially in the case of premenstrual syndrome (PMS), many women report increased joint pain [21]. Both oestrogen decrease and ageing have been shown to independently contribute to the worsening of RA, suggesting that hormonal and age-related changes synergistically influence disease progression in women.
Another level of complexity is added in the case of pregnancy, because as previously mentioned, most RA-specific treatments are counter-indicated during this time [22]. Conventional NSAIDs should not be used during the third trimester, potentially leading to an early closure of arteriovenous ductus [23]. While steroid use might be mostly safe due to a minimal crossing of the placental barrier, the use of several DMARDs, such as methotrexate and leflunomide, is contraindicated. Although various drug therapies do not seem to have a noxious effect on the foetus, knowledge is very limited and the current guideline recommends women to avoid pregnancy while under specific RA treatment [23]. Although disease severity might be alleviated or completely suppressed during pregnancy in some cases, especially during the third trimester, relapses are increased postpartum, and not all women experience similar improvements during gestation [6]. PubMed research found only three clinical trials targeting pregnant women with rheumatoid arthritis. The first article by Meade et al. from 2015 focusses on motherhood decision making, exposing the existing complications of the condition, proposing a “Motherhood decision aid” to at least inform the patients of their treatment options [24], however, without offering additional solutions. A second publication tried to mimic the increased levels of alpha-fetoprotein (AFP), correlating with a tendency of remission during the third trimester of pregnancy, by administering a non-glycosylated, recombinant version of AFP to non-pregnant patients with RA. The outcome was positive, offering potential therapeutic strategies for patients with RA in general, missing the opportunity to focus on treatments for pregnant women [25]. The third study in relation to pregnancy and RA had a similar approach. As pregnancy is known to have a protective effect on Th1-mediated AIDs in some cases, oral oestriol treatment was injected in patients suffering from multiple sclerosis leading to an immunomodulatory effect [26]. The previous studies suggest an improvement in RA symptoms during pregnancy, potentially suggesting no need for adapted treatment strategies. However, Jethwa et al. reported that 40% of patients did not experience improved disease activity, and additionally, 46.7% experienced postpartum flares [27]. This emphasises the need for alternative treatment strategies during pregnancy.
Another important hormonal transitional phase for women is perimenopause and menopause. This transition is a disruptive process which can last for over a decade and cause severe symptoms in the majority of women [28]. During this process, ovarian reproductive function gradually ceases, leading to an end of the menstrual cycle. However, during perimenopause, the ovarian function fluctuates greatly, inducing a range of symptoms [29]. Symptoms can range from vasomotor symptoms, mood disruption, temporary cognitive dysfunction, genitourinary symptoms, and others, severely reducing the quality of life of the affected women [28]. Common treatment includes hormonal replacement therapy (HRT). A study performed by the Women’s Health Initiative reported that joint pain or stiffness were common symptoms in menopausal women and a higher symptom relief could be achieved by HRT, although differences were only modest [30]. Although proven to be useful in menopause-specific symptom relief, a combination with RA treatments is complex and needs careful consideration [31].
Lifestyle factors are of great interest here. A randomised control trial investigated the outcomes of an IF regimen over 8 weeks in overweight and obese postmenopausal women with RA [32]. The study found that IF significantly improved body mass index, disease activity scores, and quality of life. Interestingly, certain inflammatory and oxidative stress markers did not reveal significant changes, suggesting that the benefits of IF in this population may be primarily linked to weight loss and physical improvements rather than direct modulation of inflammation or oxidative stress [32]. However, in the IF group, a significant decrease in the neutrophil-to-lymphocyte ratio was observed as well as in the malondialdehyde levels, a well-described marker of oxidative stress [14]. Finally, participants showed favourable changes in liver enzyme profiles, suggesting improved liver function [14].
Taking into account these multiple challenges in women’s health, dietary strategies such as the mediterranean diet (MD) and fasting offer promising, non-pharmacological options. Studies suggest these approaches not only reduce RA activity but also improve general well-being, including PMS and menopause-related symptoms [33]. IF strategies are especially promising as they minimise the risk of malnutrition. IF strategies include patterns such as TRE, where the eating window in a 24 h frame is typically reduced, followed by at least 14 h of fasting. Another strategy is a fasting-mimicking diet (FMD) [15], defined as periodic fasting periods of 3–7 days involving a reduced kcal intake of a low-protein, low-carbohydrate, and high-fat diet, designed to induce fasting-like metabolic states while reducing the risk of malnourishment [34,35].
3. Alternative Treatment Strategies for Rheumatoid Arthritis
3.1. The Role of the Gut Microbiome in Rheumatoid Arthritis
Dietary interventions are gaining interest due to their potential impact on the GMB, a crucial player in immune regulation and systemic inflammation. Dysbiosis, an imbalance in GMB composition, has been identified as a key factor in RA pathogenesis [36]. Several significant differences in patients with RA compared to healthy controls have been previously reported, such as decreases in Bacteroidota and increases in Firmicutes and Pseudomonadota, including, amongst others, Porphyromonas gingivalis and Aggregatibacter actinomycetemcomitans [37,38]. Microbial enzymes have also been reported to enhance or reduce drug efficacy, while drugs, in turn, can alter microbial composition, influencing host responses. However, the impact of GMB–drug interactions on treatment efficacy remains unclear [39]. Notably, ex vivo studies showed that residual methotrexate (MTX) levels in distal gut samples from RA patients correlated with future treatment response, suggesting a direct role of the microbiome in MTX metabolism [40]. This is of particular interest considering that some studies suggest GMB fluctuates across the menstrual cycle, as well as that there is an impact of oral contraceptives on the GMB [41]. However, the results are conflicting. An in vitro model by Leao et al. shows a significant influence of sex hormones on microbiome structure and diversity, including specific shifts induced by hormonal fluctuations across the menstrual cycle, including increases at the phylum level in Bacteroidota and decreases in Bacillota and Pseudomonadota [42]. Some studies looked at the effect of oral contraceptives on the GMB. Terrazas et al. report an impact of oral contraceptives on the a-diversity, while Brit et al. report no difference in GMB composition, but find that the ß-diversity differs between the control group and the oral contraception group [41,43]. Krog et al. find no change in the GMB whatsoever, neither in the oral contraceptive nor the control group, and only report changes in vaginal and oral microbiome composition [44]. When it comes to pregnancy, the literature is even more limited. Only two clinical trials on GMB changes have been identified, both in relation to dietary patterns. These studies report changes over the course of the pregnancy in the GMB composition, however, only in association with different dietary interventions, such as a mediterranean diet (MD) and a vegetarian diet [45,46]. Natural GMB fluctuations without dietary intervention have not been reported yet. Similarly for menopause, while twenty-one clinical trials analysing different interventions, including probiotics, prune, and blackcurrant supplementation, have been published, no studies on long-term GMB changes during menopause were identified [47,48].
Besides a potential hormonal influence, factors like stress, sleep, physical activity, and nutrition are influential modulators of GMB composition [49]. Western diets, characterised by high sugar, high fat, and processed food intake, are associated with increased gut permeability, reduced microbial diversity, and higher systemic inflammation [50]. Conversely, diets such as the MD, rich in plant-based foods and fibre, promote beneficial microbial shifts and anti-inflammatory effects [3,5]. The TASTY trial f.ex. focuses on a traditional MD enriched with fermented foods, implemented for 12 weeks. The study is aiming to evaluate the effects of this dietary intervention on gut microbiota composition, intestinal barrier integrity, and clinical outcomes associated with RA [51].
3.2. Fasting Interventions and Their Benefits in Rheumatoid Arthritis
While traditional dietary patterns emphasise food composition, meal timing is also emerging as a critical factor in metabolic and immune regulation [52]. IF, including TRE as well as FMDs, has gained immense popularity, as it is more easily accessible than fasting protocols such as prolonged fasting (PF), a continuous fasting period of more than 4 days with a kcal intake of max. 350 kcal/day, which requires medical supervision [15]. Fasting modulates metabolism by reducing insulin levels, increasing ketogenesis, altering bile acid secretion, and suppressing pro-inflammatory pathways [53]. Key mechanisms include enhanced autophagy and mitochondrial function and reduced oxidative stress (Figure 1) [53].
In a recent study, RA patients underwent bowel cleansing and then followed a 7-day period of fasting. This protocol led to significant immunological and clinical improvements. Notably, there was a marked reduction in monocyte turnover and a decline in pro-inflammatory cytokines. These changes were accompanied by a significant reduction in disease activity scores, with patients showing clinical improvement and some achieving full remission. Additionally, serum levels of IL-6 and zonulin, a marker of gut permeability, were significantly decreased [54].
The NutriFast trial, conducted at the Charité in Germany, showed that both 1 week of PF followed by 11 weeks of a plant-based diet (PBD) as well as 12 weeks of AD without prior fasting lead to significant improvements in patients with RA [55,56]. Decreased clinical disease activity and improved well-being in RA were accompanied by improvements in cardiovascular risk factors [57]. The results are promising but only observed over the course of 12 weeks. The ExpoBiome study, however, follows patients undergoing one week of PF continued by a maintenance diet of TRE, a form of IF, for 12 months. The results of this study show, amongst others, that PF followed by TRE leads to a sustained decrease in activity, lower BMI, and overall increased well-being for at least 12 months [58,59]. Additionally, the above-mentioned studies portray feasibility and high adherence of the patients with RA to the different fasting regimens. In-depth analyses will focus on the gut microbiome composition and changes as well as on alternations in metabolite production and circulation, such as bile acid and lithocholic acid. The latter has been shown to activate, amongst others, AMPK, a potential key player in fasting-mediated health benefits [60,61]. It needs to be noted that the ExpoBiome trial has one arm of patients with RA, and a similar set-up with a higher patient number and an additional control group would be essential for a follow-up study.
While research is still ongoing, emerging evidence suggests that IF may offer beneficial effects for autoimmune and inflammatory conditions like RA, primarily by reducing inflammation and modulating immune responses [62].
3.3. Other Dietary Intervention Studies
Recent and ongoing studies focus on the impact of dietary interventions such as a PBD or an AD and their effect on RA. A systematic review of PBD on patients with RA suggests that the observed beneficial effects may stem from the diet’s anti-inflammatory properties and antioxidant content, which together could enhance GMB, reduce immune reactivity to food allergens, and lower intestinal inflammation often associated with meat consumption [63].
In the MADEIRA randomised control trial, women with RA underwent a three-month intervention that combined a personalised isocaloric MD plan with the encouragement of physical activity, all assisted by a clinical decision support system platform. The intervention group demonstrated significantly higher adherence to the MD compared to the control group. These women also showed notable reductions in disease activity scores, along with improvements in dietary intake, physical activity levels, body weight, blood glucose levels, and serum 1,25-dihydroxyvitamin D concentrations. These results suggest that this combined protocol may lead to meaningful improvements in disease activity and cardiometabolic health in women with RA [64].
Another approach concerns the Autoimmune Protocol (AIP) diet that has been implemented in several studies in patients with autoimmune diseases. The AIP diet is a patient-specific tailored elimination diet designed to identify and remove foods that may provoke immune reactions due to a dysfunction in the gut barrier, contributing to inflammation and symptoms linked to autoimmune conditions. It involves three key stages: elimination of all potential foods that trigger an immune reaction, reintroduction of the reaction-free foods, and long-term maintenance of the individual-appropriate diet [65]. The initial finding suggest that the AIP may serve as a promising complementary approach in the management of RA, requiring further clinical investigation to confirm its efficacy [66].
3.4. Fasting and Dietary Intervention Studies in Transitional Hormonal Stages
Research into female-specific conditions such as menstruation, including PMS and PCOS, as well as pregnancy and menopause, has only gained attention relatively recently. As a result, the scientific landscape in these areas remains comparatively sparse. While no clinical trials on fasting and PMS symptoms are found, several publications suggest improved symptom outcomes for fasting interventions, mostly TRE, in PCOS and postmenopause, including weight reduction and improvements in hyperandrogenaemia, body composition, and several metabolic parameters in obese women [67,68,69]. Similar improvements have been reported for dietary interventions such as a MD combined with other lifestyle changes, including increased physical activity [70,71].
4. Discussion
RA disproportionately affects women, particularly during critical hormonal transitions such as pregnancy, postpartum, and menopause. These phases are often accompanied by shifts in immune function and inflammatory responses, underlining the need for prevention and treatment strategies that are specifically tailored to women’s health. For instance, the interplay between oestrogen levels and immune modulation has been shown to influence RA onset and activity, with symptoms often improving during pregnancy and flaring postpartum. The symptom alleviation could potentially be increased by applying diverse lifestyle changes, such as TRE and adapted dietary intake. To avoid any kind of nutrient deficiencies during pregnancy, the focus should ideally be on IF or short-term fasting protocols, such as brief fasting periods of 2–4 days, which may exert metabolic and immunomodulatory effects without sustained caloric deprivation. Any consideration of such strategies during pregnancy would require strict clinical oversight and individualised assessment to ensure maternal and foetal nutritional adequacy. Unfortunately, nutrition is still underappreciated. A strong emphasis on pharmacological knowledge in medical education, while essential, sometimes overshadows the role of nutrition in clinical practice. Combined with society’s tendency toward a preference for quick solutions, this can limit the active application of diverse dietary and lifestyle strategies for symptom alleviation.
A combined approach that integrates pharmacological treatments with lifestyle interventions could significantly enhance the management of RA and other NCDs. While medications such as DMARDs help control inflammation and slow disease progression, complementary dietary and lifestyle strategies can further reduce symptoms and improve overall well-being and offer opportunities for patients not able to profit from DMARDs. By considering both pharmacological solutions and evidence-based lifestyle modifications, patients may achieve better long-term outcomes, potentially requiring lower medication doses. Additionally, as mentioned above, several drugs can interfere with GMB composition, potentially affecting immunity and even medication efficacy. This is of particular importance for women, whose GMB can fluctuate in response to menstrual cycles, pregnancy, and hormonal therapies. A combined approach, incorporating targeted nutritional strategies, as well as the possible inclusion of probiotics, could help support microbiome balance and mitigate unintended side effects. Such a multifaceted strategy underscores the potential for medicine and lifestyle to work synergistically rather than independently.
The establishment of standardised, sex-specific guidelines combined with nutritional education could be of high interest, allowing patients to make informed dietary choices and thereby reducing their disease activity. Adequate nutritional education for both patient and caretaker could avoid any potential risks induced by dietary changes and restrictive food intake. Additionally, women need to be informed and prepared for potential transient side effects of fasting, including headaches, bad breath, irritability, and tiredness, amongst others. Besides targeting several issues raised above, dietary interventions are empowering and accessible for patients as they reduce their dependency and increase their autonomy. For women managing RA during pregnancy or menopause, these interventions could offer safer, non-pharmacological tools that align with both of their physiological needs.
The outlined potential of combined treatment strategies emphasises the need for more high-quality research, focusing on understanding the complex underlying mechanisms of dietary interventions, such as fasting, in RA. Studies mentioned in this article often come with limitations such as small patient groups, single-arm setups, and a short intervention period. Therefore, future research needs to focus on long-term sustainability of fasting benefits, sex-specific impacts, personalised nutritional interventions, and GMB interactions, and subsequently pave the way for a higher visibility and recognition of dietary interventions into clinical practice.
To conclude, nutrition represents a powerful, underutilised tool in RA management, particularly for women navigating distinct hormonal life stages. With growing evidence linking diet, the microbiome, and immune function, integrative, personalised treatment plans must become a non-negotiable component of patient-centred care in rheumatology.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Genovese M.C. Fleischmann R. Combe B. Hall S. Rubbert-Roth A. Zhang Y. Zhou Y. Mohamed M.F. Meerwein S. Pangan A.L. Safety and efficacy of upadacitinib in patients with active rheumatoid arthritis refractory to biologic disease-modifying anti-rheumatic drugs (SELECT-BEYOND): A double-blind, randomised controlled phase 3 trial Lancet 20183912513252410.1016/S 0140-6736(18)31116-429908670 · doi ↗ · pubmed ↗
- 2Fleischmann R. Meerwein S. Charles-Schoeman C. Combe B. Hall S. Khan N. Carter K.M. Camp H.S. Rubbert-Roth A. Efficacy and safety of upadacitinib in patients with rheumatoid arthritis and inadequate response or intolerance to biological treatments: Results through 5 years from the SELECT-BEYOND study RMD Open 202410 e 00391810.1136/rmdopen-2023-00391839059811 PMC 11284939 · doi ↗ · pubmed ↗
- 3Desai M.S. Seekatz A.M. Koropatkin N.M. Kamada N. Hickey C.A. Wolter M. Pudlo N.A. Kitamoto S. Terrapon N. Muller A. A Dietary Fiber-Deprived Gut Microbiota Degrades the Colonic Mucus Barrier and Enhances Pathogen Susceptibility Cell 201616713391353.e 132110.1016/j.cell.2016.10.04327863247 PMC 5131798 · doi ↗ · pubmed ↗
- 4Budreviciute A. Damiati S. Sabir D.K. Onder K. Schuller-Goetzburg P. Plakys G. Katileviciute A. Khoja S. Kodzius R. Management and Prevention Strategies for Non-communicable Diseases (NC Ds) and Their Risk Factors Front. Public Health 2020857411110.3389/fpubh.2020.57411133324597 PMC 7726193 · doi ↗ · pubmed ↗
- 5Gioia C. Lucchino B. Tarsitano M.G. Iannuccelli C. Di Franco M. Dietary Habits and Nutrition in Rheumatoid Arthritis: Can Diet Influence Disease Development and Clinical Manifestations?Nutrients 202012145610.3390/nu 1205145632443535 PMC 7284442 · doi ↗ · pubmed ↗
- 6Lasrado N. Jia T. Massilamany C. Franco R. Illes Z. Reddy J. Mechanisms of sex hormones in autoimmunity: Focus on EAE Biol. Sex Differ.2020115010.1186/s 13293-020-00325-432894183 PMC 7475723 · doi ↗ · pubmed ↗
- 7Scherer H.U. Häupl T. Burmester G.R. The etiology of rheumatoid arthritis J. Autoimmun.202011010240010.1016/j.jaut.2019.10240031980337 · doi ↗ · pubmed ↗
- 8Ben Mrid R. Bouchmaa N. Ainani H. El Fatimy R. Malka G. Mazini L. Anti-rheumatoid drugs advancements: New insights into the molecular treatment of rheumatoid arthritis Biomed. Pharmacother.202215111312610.1016/j.biopha.2022.11312635643074 · doi ↗ · pubmed ↗