Association of IMP3 and CD10 Expression with Clinicopathological Features and Outcomes in Phyllodes Tumors: A Retrospective Single-Center Study
Hülya Odabaşı Bükün, Erdem Çubukçu, Adem Deligönül, Ahmet Bilgehan Şahin, Alper Coşkun, Gül Akın, Çağla Karaoğlu, Ali Aktaş, İlkay Gönül, Mine Özşen, Seyit Ali Volkan Polatkan, Türkkan Evrensel

TL;DR
This study explores how IMP3 and CD10 protein levels in phyllodes tumors relate to tumor grade and patient survival, finding that IMP3 is linked to more aggressive tumors and worse survival.
Contribution
The study identifies IMP3 as a potential biomarker for predicting malignancy and survival in phyllodes tumors.
Findings
IMP3 expression was strongly associated with higher tumor grade, larger size, and stromal atypia.
IMP3 status significantly predicted poorer overall survival in phyllodes tumors.
CD10 expression did not show significant associations with tumor grade or survival outcomes.
Abstract
Background/Objectives: Phyllodes tumors (PTs) are rare fibroepithelial breast neoplasms with highly variable clinical behavior. Identifying predictive immunohistochemical markers is crucial for early detection of lesions with malignant potential and appropriate treatment selection. This study aimed to evaluate the association of insulin-like growth factor II mRNA-binding protein 3 (IMP3) and cluster of differentiation 10 (CD10) expression with histopathological grade and survival outcomes in PTs. Methods: We retrospectively analyzed sixty-eight female patients with PTs at Uludag University Faculty of Medicine Hospital, between 2000 and 2024. Histopathological features, IMP3 and CD10 expression, and clinical outcomes were evaluated. Disease-free survival (DFS) and overall survival (OS) were estimated using the Kaplan–Meier method and compared using the log-rank test. Results: Among the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
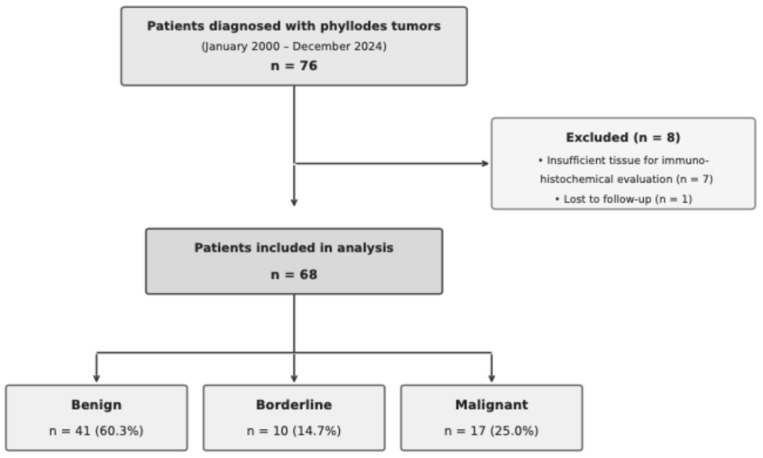 Figure 1
Figure 1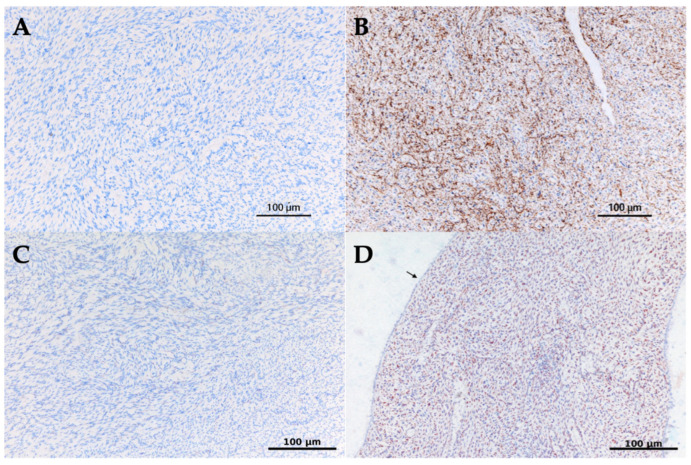 Figure 2
Figure 2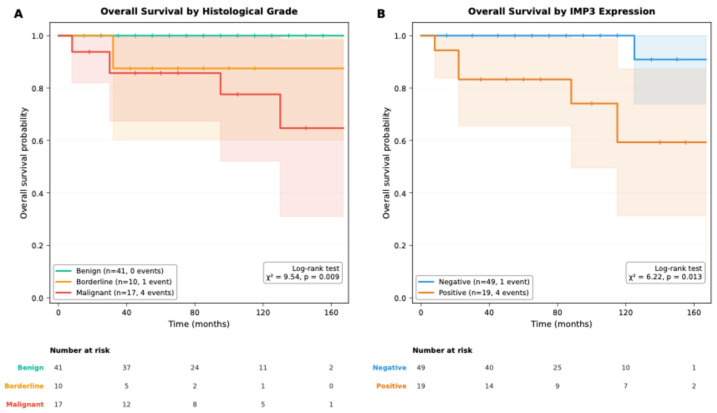 Figure 3
Figure 3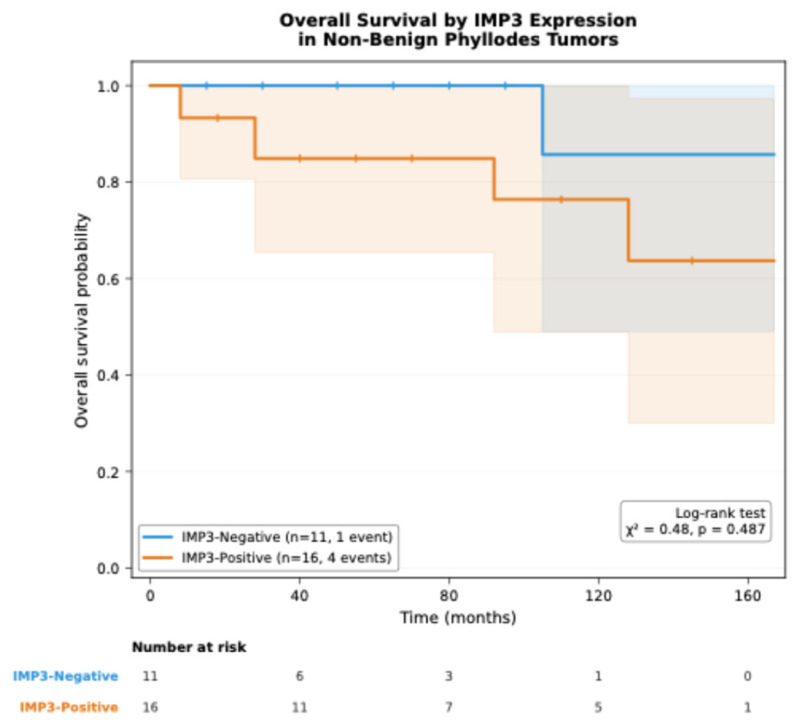 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Lesions and Carcinomas · Cancer and Skin Lesions · Breast Cancer Treatment Studies
1. Introduction
Phyllodes tumors (PTs) are rare fibroepithelial breast neoplasms representing less than 1% of all breast tumors [1,2]. They arise from the stromal component of the breast and are classified as benign, borderline, or malignant based on histological criteria [3,4,5]. Their clinical behavior is highly variable, ranging from indolent lesions to aggressive tumors capable of local recurrence or distant metastasis. Accurate grading is therefore essential for determining surgical management and follow-up strategies [6,7,8]. However, histological grade alone does not fully capture the biological heterogeneity of PTs, particularly within borderline and malignant categories, where tumors with similar histological features may demonstrate markedly different clinical outcomes.
Malignant PTs typically exhibit marked stromal atypia, stromal overgrowth, high mitotic activity (≥10 mitoses per 10 high-power fields [HPF]), infiltrative borders, and increased cellularity [9]. Although wide local excision remains the primary treatment, the optimal margin width and the role of adjuvant therapies remain controversial due to limited high-level evidence [6]. This uncertainty underscores an unresolved prognostic gap in contemporary clinical practice, highlighting the need for additional biomarkers that may improve risk stratification beyond conventional histopathological assessment.
Previous studies have demonstrated that several key proteins—including S100A8, Ki-67, polycomb repressive complex 2 (PRC2) and its catalytic subunit enhancer of zeste homolog 2 (EZH2), trimethylation of lysine 27 at histone H3 (H3K27me3), and programmed death-ligand 1 (PD-L1)—play important roles in the development and progression of breast fibroepithelial lesions. Accordingly, identification of these molecules may be useful in differentiating PT histologies [10,11,12,13]. Nevertheless, many of these markers have shown variable reproducibility across studies, and their prognostic utility has often been inferred from associations with histological grade rather than validated survival endpoints. Given the well-recognized diagnostic and prognostic challenges associated with PTs, there is growing interest in the application of immunohistochemical markers targeting these pathways.
In addition, several immunohistochemical markers related to the tumor microenvironment—particularly tumor-associated macrophages (TAMs)—including CD34, CD68, CD80, CD86, CD163, CD204, and CD206, as well as markers such as β-catenin, GATA3, TRPS1, cytokeratins, Ki-67, p63, amine oxidase-related proteins, epidermal growth factor receptor (EGFR), and somatostatin receptors, have been implicated in either tumor-suppressive or tumor-promoting processes [11,13,14,15,16,17]. These molecules reflect diverse biological mechanisms such as stromal–epithelial interaction, immune modulation, proliferation, and differentiation, all of which may contribute to PT behavior. Despite this expanding body of literature, the clinical applicability of many proposed biomarkers remains limited by small cohort sizes, heterogeneous study designs, and inconsistent associations with recurrence or survival outcomes.
Cluster of differentiation 10 (CD10), a stromal zinc-dependent metalloendopeptidase, has been shown to aid in distinguishing PTs from fibroadenomas and has also been associated with more aggressive clinical behavior [16,18,19]. Insulin-like growth factor II mRNA-binding protein 3 (IMP3), an oncofetal RNA-binding protein, exhibits strong stromal expression particularly in malignant and recurrent PTs and is thought to reflect increased biological aggressiveness [20,21]. However, existing studies evaluating CD10 and IMP3 in PTs are largely retrospective, often include limited patient numbers, and frequently lack long-term survival analyses, resulting in uncertainty regarding their true prognostic relevance. Moreover, data directly linking these markers to disease-free survival (DFS) and overall survival (OS) remain sparse and inconsistent.
Based on their diagnostic and prognostic relevance in mesenchymal tumors, we hypothesized that higher expression levels of CD10 and IMP3 correlate with adverse outcomes in patients with PTs. However, evidence regarding their prognostic significance—especially in relation to long-term survival—remains limited, as most available studies are constrained by small sample sizes and lack comprehensive survival analyses. Therefore, the aim of this study was to evaluate the association of IMP3 and CD10 expression with histological grade, clinicopathological features, DFS, and OS in a cohort of 68 female patients with PTs.
2. Materials and Methods
2.1. Study Design and Patient Selection
This study was conducted as a retrospective cohort analysis. All tissue specimens consisted of formalin-fixed, paraffin-embedded (FFPE) samples originally obtained for routine diagnostic purposes, and no additional tissue sampling or patient intervention was performed for research purposes. Patients diagnosed with PTs at the Department of Medical Oncology, Uludag University Faculty of Medicine Hospital, between January 2000 and December 2024 were included. Demographic information, clinical characteristics, and treatment details were obtained retrospectively from electronic medical records and archival files.
Inclusion criteria were as follows: (1) histopathologically confirmed primary breast PT using tissue blocks in the pathology archive; (2) adequate tumor sampling defined as the procurement of at least one tissue block for each 1-cm increment of the maximum tumor diameter, in accordance with the pathology team’s standardized sampling protocol; and (3) minimum follow-up duration of 6 months.
Exclusion criteria were as follows: (1) male sex; (2) secondary or recurrent breast sarcoma; (3) insufficient tissue quantity or quality for immunohistochemical evaluation; (4) prior history of another primary breast malignancy or other types of malignancy; and (5) incomplete clinicopathological data (Figure 1).
2.2. Histopathological Examination
Hematoxylin and eosin-stained slides from all cases were independently re-evaluated by an experienced pathologist with at least 10 years of experience in breast pathology and classified as benign, borderline, or malignant PTs according to the 2019 World Health Organization (WHO) classification of breast tumors. Classification included stromal cellularity (mild, moderate, or marked), stromal atypia (mild, moderate, or severe), mitotic activity (<5, 5–9, or ≥10 per 10 HPF), stromal overgrowth (present or absent), and tumor borders (circumscribed versus infiltrative). Benign tumors exhibited mild stromal cellularity, absent or mild atypia, fewer than 5 mitoses per 10 HPF, no stromal overgrowth, and circumscribed borders [22]. In addition, the Ki-67 proliferation index, expressed as the percentage of positively stained stromal nuclei, was assessed by immunohistochemical staining as a supportive proliferative marker [11,23].
2.3. Immunohistochemical Evaluation
Immunohistochemical staining was performed on 4-μm sections obtained from archival paraffin blocks. Antigen retrieval was performed using CC1 Solution (pH 9) by incubating the sections at 97 °C for 60 min. Subsequently, endogenous peroxidase activity was blocked using the UV Inhibitor included in the secondary detection kit. Primary antibodies against IMP3 (clone EP286, catalog no. 433R-14, Cell Marque, Rocklin, CA, USA) and CD10 (clone SP67, catalog no. R0585578560001 Roche, Tuscon, AZ, USA) were applied, with 2 h (1:25 dilution) and 1 h incubation, respectively. In addition, estrogen receptor (ER, clone SP1; catalog no. N19436; Roche Diagnostics), progesterone receptor (PR, clone 1E2; catalog no. N13902; Roche Diagnostics), and Ki-67 (clone 30-9; catalog no. N10219; Roche Diagnostics) antibodies were used. For secondary detection, the ROCHE UltraView Universal DAB Detection Kit was used following the standard UltraView IHC protocol. All procedures were performed on the ROCHE Ventana BenchMark Ultra IHC Stainer (Roche/Ventana, Tucson, AZ, USA).
IMP3 staining was evaluated as cytoplasmic positivity in the stromal component, and staining in more than 10% of stromal cells was considered positive [21]. CD10 staining exhibited membranous and/or cytoplasmic patterns in stromal cells, and staining in more than 20% of cells was classified as positive [4]. ER and PR were evaluated as nuclear positivity in the epithelial component, and 1% or greater nuclear staining was considered positive. All immunohistochemical evaluations were performed by pathologists blinded to clinical outcomes and independent of the study hypothesis (Figure 2).
2.4. Endpoints
The primary endpoints were DFS and OS. DFS was defined as the time from surgery to documented local or distant recurrence, or death from any cause, whichever occurred first. OS was defined as the time from the date of diagnosis to death from any cause. Patients without events at last follow-up were censored at the date of last contact.
2.5. Follow-Up Procedures
Patients were followed according to a standardized institutional follow-up protocol routinely applied in clinical practice, which remained consistent throughout the study period. Follow-up data—including clinical examinations, laboratory tests, and imaging studies (chest computed tomography [CT] and breast magnetic resonance imaging [MRI])—were retrieved retrospectively from medical records. According to this protocol, patients underwent evaluation every 3 months during the first 2 years, every 6 months between years 3 and 5, and annually thereafter. No additional prospective follow-up visits or investigations were performed specifically for the purposes of this study.
A positive surgical margin was defined as the presence of neoplastic tissue in direct continuity with the inked resection margin on histopathological examination. Surgical margins were considered negative when no tumor cells were identified at the inked surface [24].
Recurrence was defined as the detection of tumor reappearance after initial surgical treatment and was classified as local or distant. Local recurrence was identified by radiological evidence of tumor at or adjacent to the primary surgical site, with or without histopathological confirmation when clinically indicated. Distant recurrence was defined as radiological and/or histopathological evidence of tumor involvement at sites anatomically distinct from the primary tumor location [25].
Clinical and pathological data were retrieved retrospectively from institutional medical records and pathology archives and were fully anonymized prior to analysis.
2.6. Sample Size
A post hoc power analysis was performed to evaluate the statistical adequacy of the sample size for the association between IMP3 expression and histological grade. The observed effect size was found to be large (Cramér’s V = 0.648), yielding an achieved power of 99.9% with a sample of 68 patients. Power calculations were based on observed effect sizes using Cohen’s w statistic and chi-square distribution with α = 0.05. No post hoc analysis was performed for the survival outcomes.
2.7. Statistical Analysis
Statistical analyses were performed using Jamovi (Version 2.6.44; The Jamovi Project, 2023) and JASP (Version 0.19.3; Jeffreys’ Amazing Statistics Program, 2024). Survival analyses and Cox regression models were conducted using R software (version 4.5.2; R Foundation for Statistical Computing, Vienna, Austria). A two-sided p value of 0.05 or less was considered statistically significant.
The distribution of continuous variables was assessed using the Shapiro–Wilk test and inspection of histograms. Variables not following a normal distribution were summarized as median [minimum–maximum], whereas normally distributed variables were presented as mean ± standard deviation (SD).
Comparisons of demographic and clinicopathological characteristics across histological grade groups (benign, borderline, and malignant) were performed using the Kruskal–Wallis H test for continuous variables and Pearson’s chi-square test or Fisher–Freeman–Halton exact test for categorical variables, depending on expected cell counts. When omnibus tests indicated statistically significant differences, pairwise comparisons were conducted using Bonferroni-corrected Mann–Whitney U tests for continuous variables and Bonferroni-adjusted z-tests for proportions in categorical variables. In post hoc analyses, statistically distinct subgroups within each variable category were indicated with superscript letters (a, b, c).
DFS and OS were estimated using the Kaplan–Meier method. DFS and OS curves were compared according to pathological diagnosis (benign, borderline, and malignant) and CD10/IMP3 expression status using the log-rank test. Survival curves and event counts were calculated using the survival package in R (functions Surv, survfit, and survdiff), and graphical representations were generated using the survminer package.
A p value less than 0.05 was considered statistically significant, whereas a p value between 0.05 and 0.10 was interpreted as borderline (marginal) significance in the context of a small sample size and low event rate.
2.8. Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki and relevant national regulations governing retrospective research in Türkiye. The secondary use of archived FFPE tissue samples, originally obtained for routine diagnostic purposes, is permitted under Turkish regulations provided that no additional patient intervention is performed and that patient data are anonymized (Regulation on Clinical Trials of Medicinal Products and Biological Products, Official Gazette No. 28617, 2013).
The study was approved by the Health Research Ethics Committee of Uludag University Faculty of Medicine (Decision No: 2025/538-6/2; Date: 3 March 2025). Owing to the retrospective design and the use of archived diagnostic material, the requirement for informed consent was waived.
3. Results
A total of 68 female patients with median age of 39.0 years [range: 13.9–74.0] were included in the study. Of these, 60.3% (n = 41) had benign, 14.7% (n = 10) had borderline, and 25.0% (n = 17) had malignant histological subtypes. The median follow-up time was 83.2 months (range: 3.2–166.9 months). Although patients with malignant tumors were older (median age: 46.3 years), this difference did not reach statistical significance (p = 0.054). The median tumor size was 5.0 cm (range: 1.0–14.0 cm). Although larger tumors were prominent in the malignant group, this difference was not statistically significant compared to other groups. No significant differences were observed among groups regarding surgical approach or positive surgical margins (p > 0.05). Analysis of histopathological parameters demonstrated significant differences in mitotic activity distribution among groups (p = 0.005). High mitotic activity was observed in 80.0% of malignant tumors but was absent in borderline tumors. Stromal atypia was present in 82.4% of malignant tumors compared to approximately 22.0% in benign and borderline groups (p < 0.001). Median Ki-67 proliferation index values were 25.0% in malignant, 15.0% in borderline, and 10.0% in benign tumors (p < 0.001) (Table 1).
Evaluation of immunohistochemical markers revealed a strong association between IMP3 positivity and histological grade (p < 0.001). IMP3 positivity was observed in 76.5% of malignant tumors, 30.0% of borderline tumors, and 7.3% of benign tumors, with all three groups significantly different from each other. The difference in CD10 expression among groups did not reach statistical significance (p = 0.065). No significant differences were observed regarding hormone receptor positivity (p > 0.05) (Table 1).
Regarding treatment modalities, adjuvant chemotherapy was more frequent in the malignant group. Postoperative radiotherapy was administered to 58.8% of patients with malignant tumors compared with approximately 20% in benign and borderline groups. The overall mortality rate was 7.5% and showed a significant association with histological grade; mortality was 23.5% in the malignant group, 10.0% in the borderline group, and absent in the benign group (p < 0.05) (Table 1).
To further characterize the clinical significance of IMP3 expression, we analyzed its association with demographic and clinicopathological variables (Table 2). IMP3-positive tumors were significantly larger than IMP3-negative tumors (median: 7.0 cm versus 4.0 cm; p = 0.036). Stromal atypia was markedly more prevalent in IMP3-positive cases (72.2% versus 24.5%; p < 0.001). IMP3 expression showed a strong association with histological grade (p < 0.001): 68.4% of IMP3-positive tumors were malignant, compared with only 8.2% in the IMP3-negative group. Patients with IMP3-positive tumors tended to be older (median: 46.3 versus 37.6 years; p = 0.052) and had higher Ki-67 indices (median: 20.0% versus 10.0%; p = 0.061), although these differences did not reach statistical significance. No significant associations were observed between IMP3 expression and mitotic activity (p = 0.924), menopausal status (p = 0.310), or positive surgical margin status (p = 0.072).
The unadjusted Kaplan–Meier survival analyses demonstrated significant differences in OS according to histological grade and IMP3 expression in patients with PTs (Table 3). OS was significantly shorter in patients with malignant tumors compared with those with benign and borderline tumors (log-rank p = 0.009), with progressively lower 5-year OS rates observed across increasing histological grades.
In addition, in unadjusted Kaplan–Meier analysis, IMP3-positive tumors were associated with significantly reduced OS compared with IMP3-negative tumors (log-rank p = 0.013). Patients with IMP3 positivity exhibited lower mean survival times and inferior 5-year OS rates.
Figure 3 illustrates unadjusted Kaplan–Meier OS curves stratified by histological grade and IMP3 expression. OS differed significantly according to histological grade, with malignant PTs exhibiting poorer survival compared with benign and borderline tumors (log-rank χ^2^ = 9.54; p = 0.009). In addition, IMP3-positive tumors were associated with significantly reduced OS compared with IMP3-negative tumors (log-rank χ^2^ = 6.22; p = 0.013).
Based on unadjusted descriptive survival estimates, no statistically significant differences were observed in DFS according to histological grade, IMP3 status, or CD10 expression. Similarly, CD10 expression was not significantly associated with OS. These nonsignificant findings are detailed in Table 3. Univariate Cox regression analyses evaluating the association of treatment-related variables with OS and DFS are presented in Appendix A (Table A1 and Table A2).
4. Discussion
In this study, we demonstrated that IMP3 expression is strongly associated with histological grade and OS in PTs, supporting its role as a promising adjunct biomarker in this rare disease. IMP3 positivity was detected in 76.5% of malignant tumors but in only 7.3% of benign tumors. Notably, 80% of the deceased patients had IMP3-positive PTs. Although these associations, derived from descriptive comparisons and survival analyses, suggest a link between IMP3 expression and aggressive tumor behavior; they do not establish independent prognostic significance.
IMP3 is a well-established oncofetal protein implicated in tumor progression and consistently linked to poor clinical outcomes across multiple malignancies [26]. It enhances metastatic potential through induction of epithelial-mesenchymal transition [27], and promotes tumorigenesis via post-transcriptional regulation of IGF-II mRNA translation, integrating mRNA stability with oncogenic signaling pathways [28]. In line with its pro-tumorigenic role, IMP3-positive tumors in our cohort exhibited more aggressive clinicopathological features, including higher grade, larger tumor size, and increased stromal atypia. These findings are in accordance with those of Bellezza et al., who reported strong stromal IMP3 positivity in 56% of malignant PTs and demonstrated higher expression in recurrent tumors [21]. However, in the present study, the observed association between IMP3 positivity and mortality was based solely on group-level comparisons and Kaplan–Meier survival analyses. Because of the very low number of outcome events (n = 5 deaths), regression-based risk estimation was not performed. Therefore, the data do not allow assessment of whether IMP3 provides prognostic information independent of histological grade. A supplementary Kaplan–Meier analysis restricted to non-benign (borderline and malignant) tumors did not demonstrate a statistically significant difference in OS according to IMP3 status (log-rank p = 0.487; Figure A1).
CD10-positive patients exhibited lower 5-year DFS rates than CD10-negative patients (60.5% versus 88.6%, respectively); however, the difference did not translate into a statistical significance. Similarly, OS was comparable between the same groups. In PTs, CD10 expression is primarily confined to the stromal component and is associated with higher histological grade and invasive growth patterns, suggesting a role in stromal activation and tumor aggressiveness [29]. While our results do not fully support a prognostic role for CD10, they indicate the need for validation in larger cohorts before definitive conclusions can be drawn.
In our study, pathological grade emerged as the strongest predictor of OS (p = 0.009), with a mortality rate of 23.5% in the malignant group compared with no deaths in the benign group.
Our study has several strengths, including a homogeneous cohort from a single institution and comprehensive immunohistochemical evaluation. To our knowledge, this is among the first studies to evaluate IMP3 and CD10 together with survival endpoints in a Turkish PT cohort.
Nevertheless, this study also has several limitations. First, the single-center, retrospective design may limit the generalizability of the findings. In addition, the very low number of outcome events, particularly deaths (n = 5), substantially constrained statistical inference, precluding regression-based analyses and formal evaluation of independent prognostic values of IMP3 or CD10 beyond other clinicopathological variables. Another important limitation is the long inclusion period spanning more than two decades (2000–2024). Although this extended timeframe was necessary due to the rarity of PTs, it may have introduced temporal heterogeneity that could influence survival outcomes independently of tumor biology. Consequently, the observed associations—particularly those involving IMP3 expression and OS—may partly reflect treatment-era or management-related differences rather than intrinsic prognostic effects alone. Given the limited number of outcome events, comprehensive stratified or sensitivity analyses according to treatment modalities (such as radiotherapy or chemotherapy) were not feasible, and these potential confounding effects could not be fully addressed.
Furthermore, all histopathological and immunohistochemical evaluations were performed by a single, experienced pathologist. Although this approach ensured internal consistency in slide interpretation and scoring, it precluded assessment of interobserver variability. Although the scoring criteria used predefined cutoff values (>10% for IMP3 and >20% for CD10), cases with staining intensities near these thresholds may be subject to interpretation differences among observers. As a result, the reproducibility of IMP3 and CD10 expression assessment across different observers could not be evaluated, which may limit the applicability of the findings to broader pathology practice. Future multicenter studies incorporating independent or blinded multiobserver assessments would be valuable to confirm the robustness and reproducibility of these results.
Finally, treatment-related confounding represents an additional limitation. Surgical and adjuvant treatment modalities were more frequently applied in patients with aggressive disease, reflecting confounding by indication rather than true treatment effects. Given the descriptive nature of the analyses and the limited number of events, adjustment for treatment-related variables was not feasible. In addition, detailed information regarding surgical margin width was not consistently available due to the retrospective nature and long inclusion period. Therefore, margins were categorized dichotomously as positive or negative. Similarly, adjuvant treatment data were recorded as binary variables, and information on specific regimens, indications, or timing was incomplete, precluding regimen-specific analysis.
Overall, these limitations underscore the need for larger, prospective, multicenter studies with more uniform treatment protocols to clarify the prognostic relevance of IMP3 and CD10 and to determine whether these markers provide incremental value beyond established histopathological classification.
From a clinical standpoint, our findings do not support immediate changes in management or follow-up strategies based solely on IMP3 status. Rather, IMP3 should be viewed as a biologically plausible and potentially informative adjunct marker that may complement, but not replace, established histopathological risk stratification. Prospective, multicenter studies with larger event numbers are required to determine whether IMP3 provides incremental prognostic value beyond histological grade.
5. Conclusions
In conclusion, our study suggests that IMP3 expression is closely associated with higher histological grade and poorer OS in PTs, supporting its role as a promising adjunct prognostic marker. CD10 expression showed a nonsignificant trend toward shorter DFS and requires further evaluation. Although IMP3 appears biologically linked to aggressive tumor behavior, its incremental prognostic value beyond histological grade could not be definitively established in this cohort. Therefore, IMP3 should currently be considered a hypothesis-generating biomarker rather than a clinically actionable determinant, pending validation in larger, prospective, multicenter studies with sufficient outcome events.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1ToméA. Figueiredo J. Antunes S. Trindade M. Travancinha D. Breast Phyllodes Tumor: A Tumor with Unpredictable Clinical Behavior Cureus 202315 e 3753710.7759/cureus.3753737193421 PMC 10182856 · doi ↗ · pubmed ↗
- 2Chow Z.L. Gudi M. Tan P.H. Fibroepithelial Lesions: An Update for Daily Practice (Part-II)Surg. Pathol. Clin.20251870170610.1016/j.path.2025.05.00641224413 · doi ↗ · pubmed ↗
- 3Niyonkuru E. Nisabwe S. Sami Z. Faizi I. Mazti A. Elkarroumi M. Karkouri M. Cystic Squamous Metaplasia in a Giant Benign Phyllodes Tumor of the Breast: A Case Report J. Surg. Case Rep.20232023 rjad 40210.1093/jscr/rjad 40237502602 PMC 10371490 · doi ↗ · pubmed ↗
- 4Shubham S. Ahuja A. Bhardwaj M. Immunohistochemical Expression of Ki-67, P 53, and CD 10 in Phyllodes Tumor and Their Correlation with Its Histological Grade J. Lab. Physicians 20191133033410.4103/JLP.JLP_106_1931929699 PMC 6943865 · doi ↗ · pubmed ↗
- 5Zhang Y. Kleer C. Phyllodes Tumor of the Breast: Histopathologic Features, Differential Diagnosis, and Molecular/Genetic Updates Arch. Pathol. Lab. Med.201614066567110.5858/arpa.2016-0042-RA 27362571 · doi ↗ · pubmed ↗
- 6Reason E. Thomas S. Plichta J. Botty van den Bruele A. Hwang E. Tong B. Larrier N. Factor R. Grilley-Olson J. Rosenberger L. Utility of the Singapore Recurrence Nomogram in a US Cohort with a Higher Proportion of Borderline and Malignant Phyllodes Tumours J. Clin. Pathol.20257874074710.1136/jcp-2025-21025240830046 · doi ↗ · pubmed ↗
- 7Guillot E. Couturaud B. Reyal F. Curnier A. Ravinet J. LaéM. Bollet M. Pierga J. Salmon R. Fitoussi A. Management of Phyllodes Breast Tumors Breast J.20111712913710.1111/j.1524-4741.2010.01045.x 21251125 · doi ↗ · pubmed ↗
- 8Ben Hassouna J. Damak T. Gamoudi A. Chargui R. Khomsi F. Mahjoub S. Slimene M. Ben Dhiab T. Hechiche M. Boussen H. Phyllodes Tumors of the Breast: A Case Series of 106 Patients Am. J. Surg.200619214114710.1016/j.amjsurg.2006.04.00716860620 · doi ↗ · pubmed ↗