Evaluation of Robotic Versus Laparoscopic Surgery for Right Colon Cancer Treatment: Systematic Review and Meta-Analysis
Martina Sardonini, Daniele Giuliani, Alessandro Spizzirri, Vincenzo Napolitano, Roberto Cirocchi, Luca Properzi, Francesco Brucchi, Sara Lauricella, Francesca Pennetti Pennella, Valentina Bartolini, Marco Coccetta

TL;DR
This study compares robotic and laparoscopic surgeries for right colon cancer, finding each has distinct advantages in terms of surgical outcomes and costs.
Contribution
The study provides a comprehensive meta-analysis comparing robotic and laparoscopic approaches for right colon cancer surgery, including healthcare economics.
Findings
Robotic surgery showed higher lymph node yield and lower blood loss in non-CME cases.
Laparoscopic surgery had shorter operative times and similar hospital stays compared to robotic surgery.
Robotic surgery had lower conversion rates and potentially lower readmission costs for CME cases.
Abstract
Background: Right hemicolectomy remains the standard surgical treatment for right colon diseases. This study evaluates robotic versus laparoscopic approaches to determine optimal, minimally invasive strategies, balancing technical efficacy with healthcare economics. Materials and Methods: This retrospective study evaluates robotic versus laparoscopic approaches using data from 46 studies (2003–2025) involving 36,868 patients (6,312 robotic, 30,547 laparoscopic). Primary outcomes assessed were lymph node yield, operative time, and hospital stay; secondary outcomes included blood loss, conversion rates, infections, readmissions, and costs. Results: Concerning robotic surgery, lymph node harvest was higher (MD 1.34 for CME; MD 1.27 for non-CME). Laparoscopy showed shorter operative times (MD 25.73 for CME; MD 42.45 for non-CME). Hospital stays showed no significant difference. Robotics…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
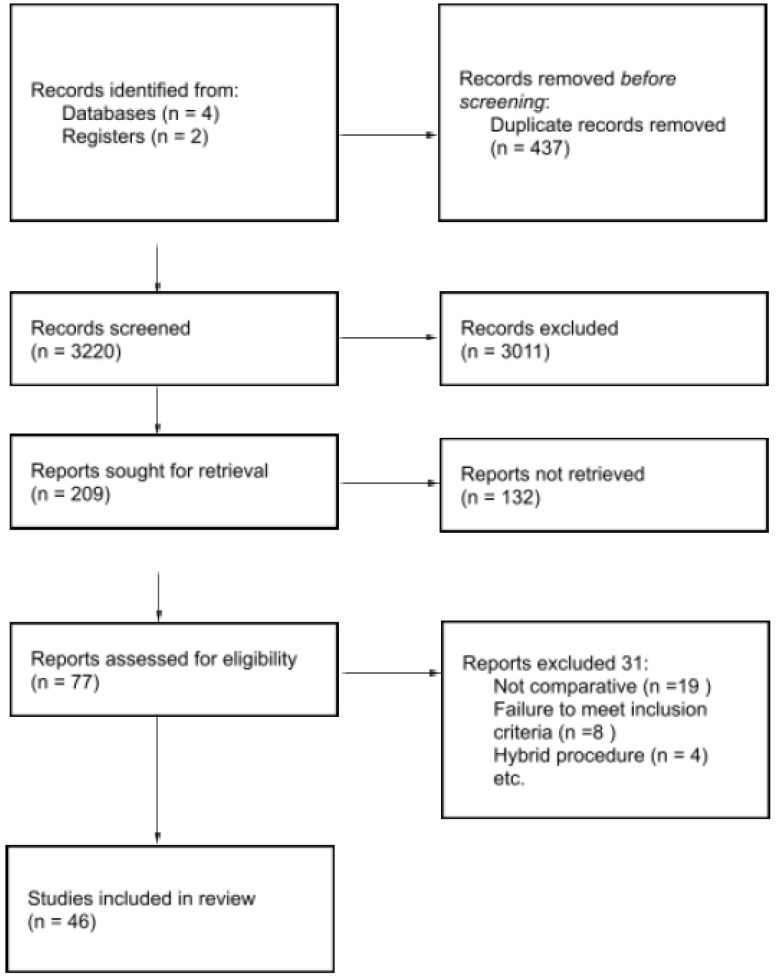 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3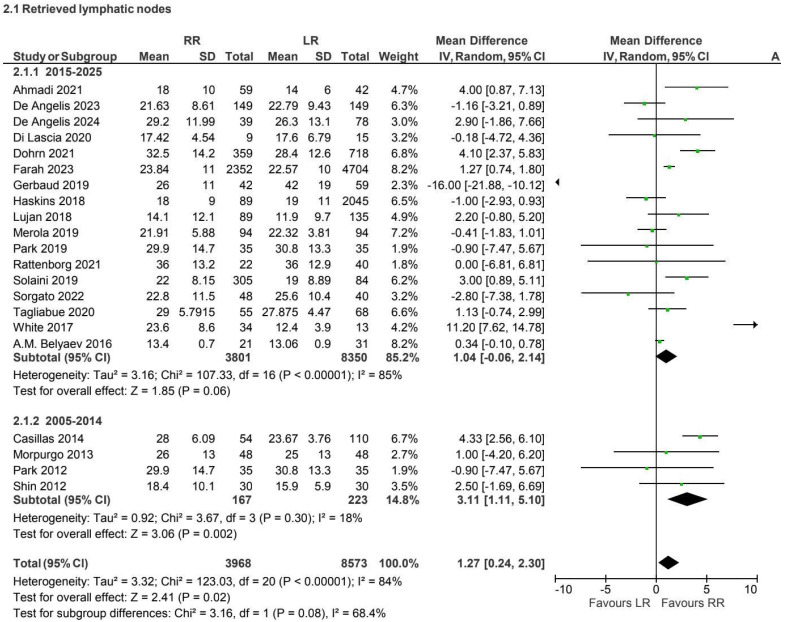 Figure 4
Figure 4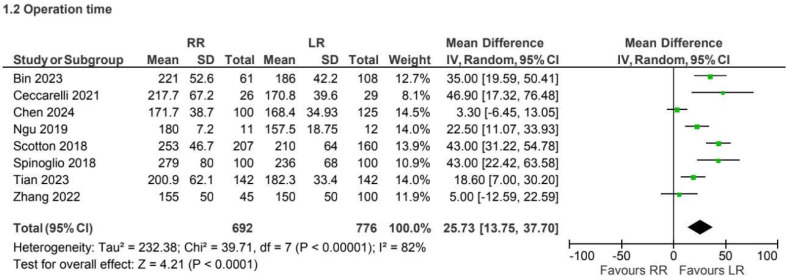 Figure 5
Figure 5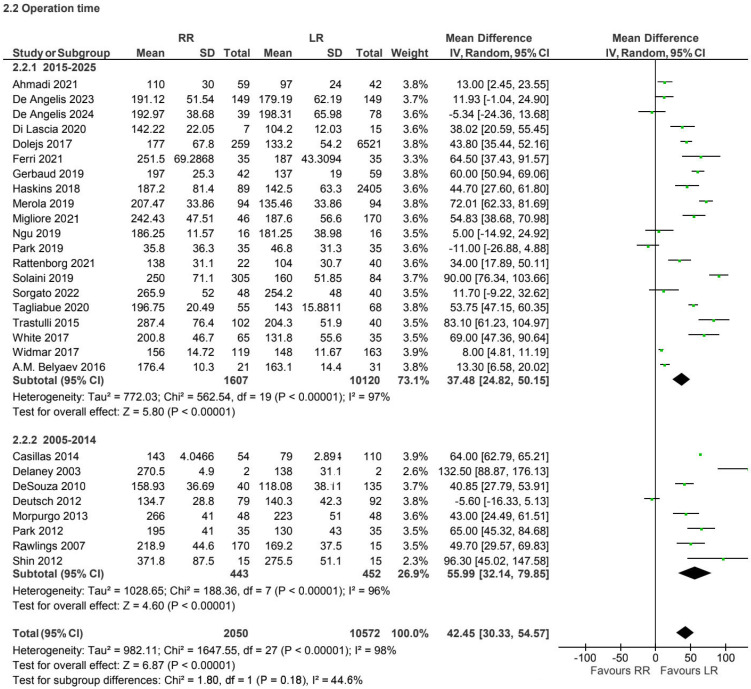 Figure 6
Figure 6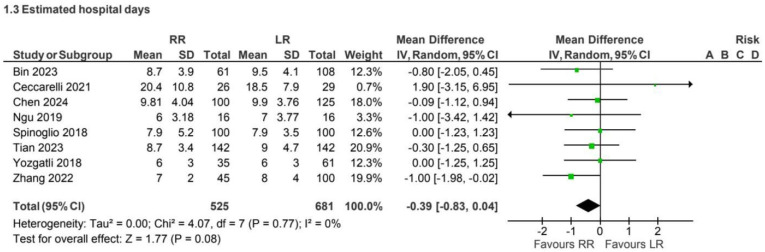 Figure 7
Figure 7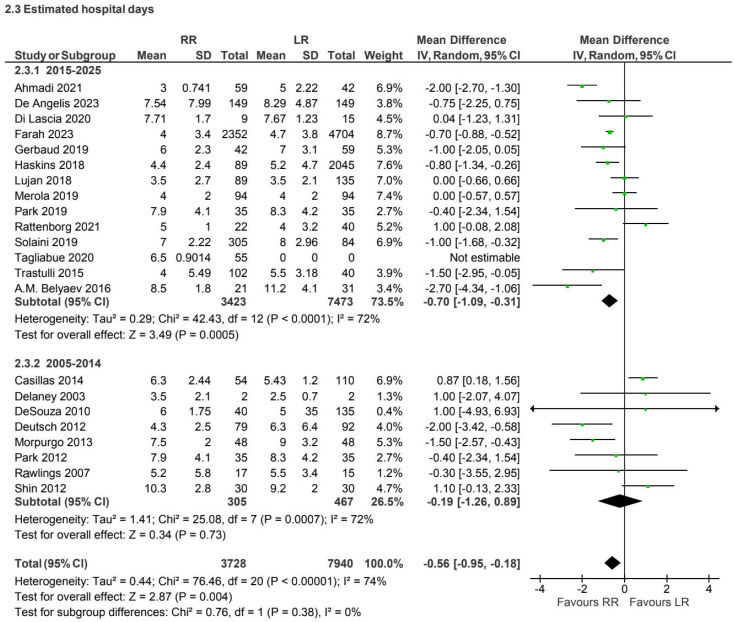 Figure 8
Figure 8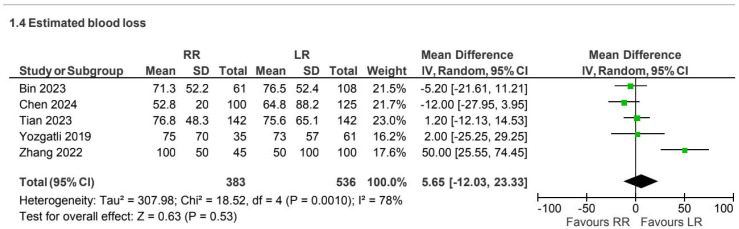 Figure 9
Figure 9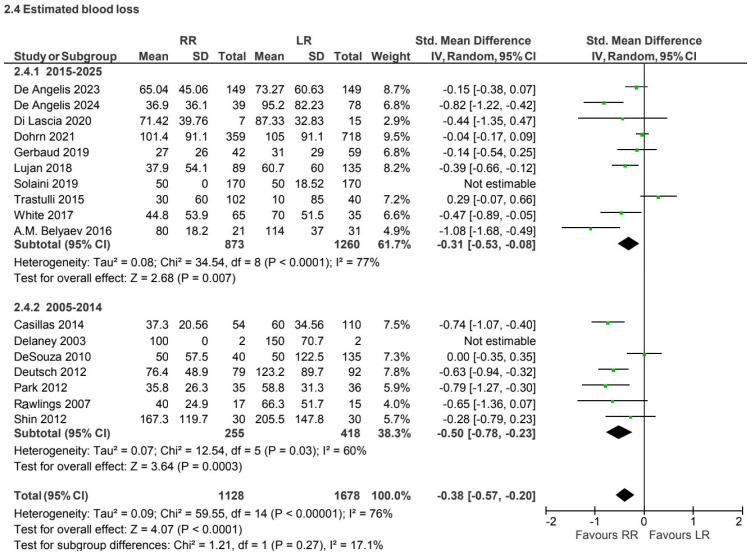 Figure 10
Figure 10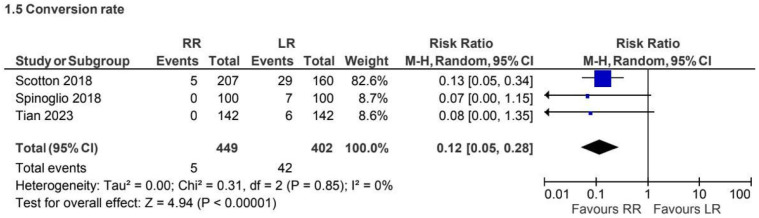 Figure 11
Figure 11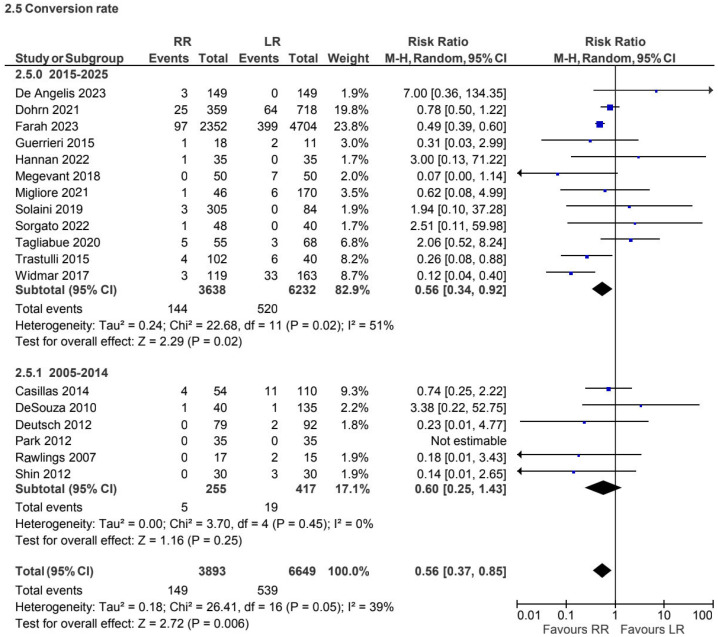 Figure 12
Figure 12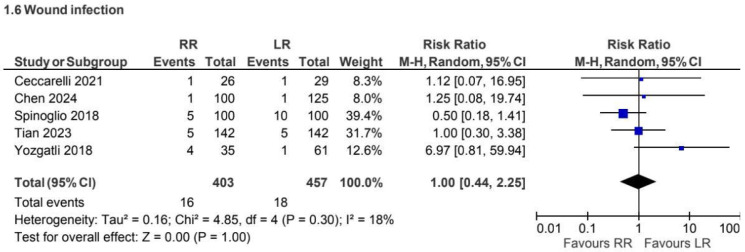 Figure 13
Figure 13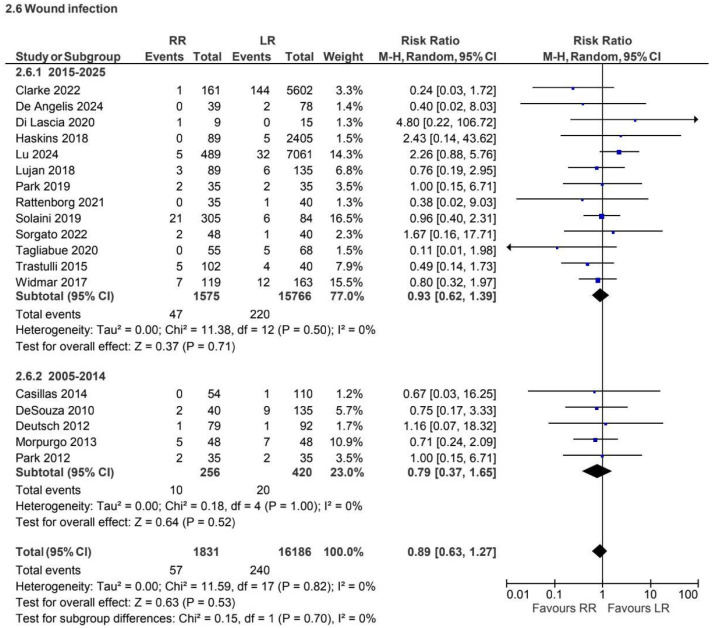 Figure 14
Figure 14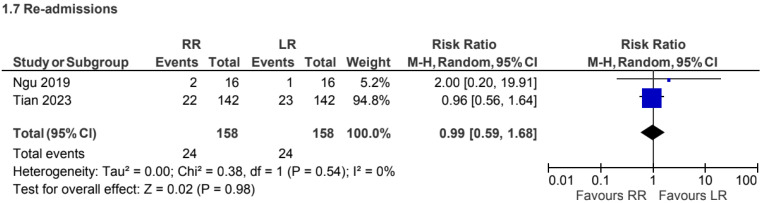 Figure 15
Figure 15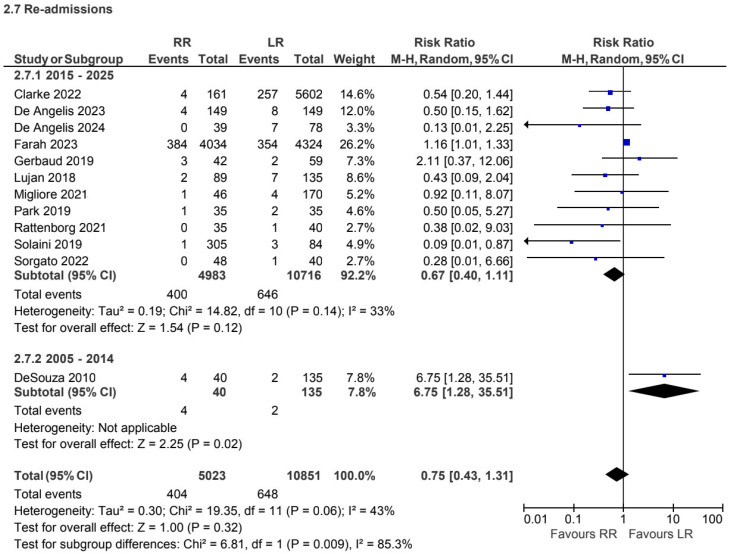 Figure 16
Figure 16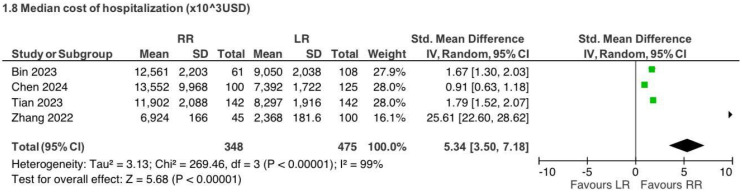 Figure 17
Figure 17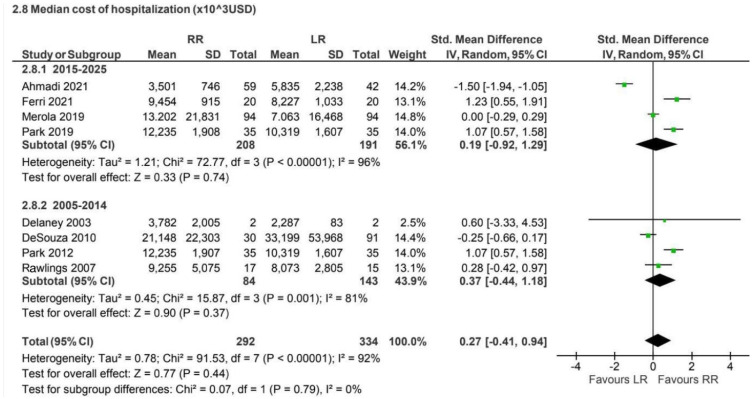 Figure 18
Figure 18Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsColorectal Cancer Surgical Treatments · Diverticular Disease and Complications · Multiple and Secondary Primary Cancers
1. Introduction
Colon cancer represents a major global health burden and remains one of the most frequently diagnosed malignancies worldwide [1]. Surgical resection is the cornerstone of curative treatment for right-sided colon cancer, with right hemicolectomy representing the standard surgical approach. Over the past decades, minimally invasive surgery has progressively replaced open techniques, demonstrating advantages in terms of postoperative recovery, reduced surgical trauma, and shorter hospital stay [1,2].
Among minimally invasive approaches, laparoscopic right hemicolectomy has become widely adopted due to its safety and reproducibility. However, laparoscopy is associated with intrinsic technical limitations, including two-dimensional visualization, restricted instrument articulation with limited degrees of freedom, and ergonomic challenges related to fixed pivot points and instrument collision [3]. These factors may complicate precise dissection of embryological planes and vascular structures, particularly in technically demanding procedures.
In 2009, the concept of complete mesocolic excision (CME) was introduced, adapting the principles of total mesorectal excision to colon cancer surgery. CME is based on sharp dissection along embryological planes, central vascular ligation, and intact mesocolic envelope removal, with the aim of improving oncological radicality through more extensive lymphadenectomy. Since its introduction, CME has been increasingly adopted, although its technical complexity has raised concerns regarding reproducibility and safety, especially when performed laparoscopically.
Robotic surgery has been proposed as a potential solution to overcome some limitations of conventional laparoscopy. Robotic platforms offer three-dimensional visualization, tremor filtration, enhanced dexterity through articulated instruments, and improved ergonomics for the surgeon [4]. These features may theoretically facilitate precise dissection during right hemicolectomy, particularly in CME procedures. Nevertheless, the widespread adoption of robotic surgery remains limited by higher costs, longer operative times, and variability related to surgeon experience and learning curves.
Despite the growing body of literature comparing robotic and laparoscopic right hemicolectomy, evidence regarding their relative advantages remains heterogeneous and sometimes conflicting. In particular, the impact of robotic surgery on perioperative outcomes, technical surrogate markers of oncological adequacy, and healthcare resource utilization remains debated, especially when considering CME and non-CME procedures separately.
Therefore, the aim of this systematic review and meta-analysis was to compare robotic and laparoscopic right hemicolectomy by analyzing perioperative outcomes, short-term postoperative results, and hospitalization costs, with subgroup analyses according to the use of complete mesocolic excision. By synthesizing data from studies published over a 22-year period, this work seeks to provide a comprehensive and balanced assessment of the current evidence, while acknowledging the methodological limitations inherent to the available literature.
2. Materials and Methods
2.1. Study Design and Protocol Registration
A systematic review and meta-analysis was conducted to compare robotic and laparoscopic right hemicolectomy for colon cancer. The study was designed and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (see Supplementary Materials) [5]. The methodological approach was predefined to minimize selection and reporting bias, acknowledging the expected heterogeneity related to study design, surgical era, and institutional practice. The review protocol was prospectively registered in the PROSPERO database (registration number: CRD420251040868).
2.2. Eligibility Criteria
Randomized controlled trials and comparative observational studies evaluating robotic versus laparoscopic right hemicolectomy for colon cancer were considered eligible. Given the limited availability of randomized controlled trials in this surgical field, the majority of included studies were retrospective or prospective observational analyses. Both procedures performed with complete mesocolic excision (CME) and without CME were included. CME was defined as sharp dissection along embryological planes with central vascular ligation and intact mesocolic envelope removal.
Studies were excluded if they were non-comparative, case reports, conference abstracts, narrative reviews, or if outcome data were incomplete or not extractable for quantitative synthesis. When overlapping patient populations were identified across multiple publications, only the most recent or most comprehensive study was included to avoid data duplication.
2.3. Literature Search Strategy
A comprehensive and systematic literature search was conducted to identify relevant studies published between January 2003 and March 2025. The electronic databases Medline/PubMed, Scopus, and Web of Science were searched without language restrictions. The search strategy was developed using predefined free-text terms related to the surgical approach and anatomical site, combined through Boolean operators. The same search string was applied consistently across all databases: “Robotic” AND “Laparoscopic” AND “Right” AND “Colectomy”.
The extended time frame was intentionally selected to capture the evolution of minimally invasive and robotic techniques over time, acknowledging potential variability related to surgical era, technological development, and learning curves. Reference lists of included studies were manually screened to identify additional eligible articles. Gray literature was explored through Google Scholar to minimize publication bias.
2.4. Study Inclusion Process
All retrieved records were imported into reference management software, and duplicate entries were removed. Two reviewers (M.S. and R.C.) independently screened titles and abstracts for eligibility. Full-text articles were assessed when abstracts met the inclusion criteria or when eligibility was unclear. Discrepancies were resolved through discussion until consensus was reached.
2.5. Data Extraction
Data extraction was independently performed by the same two reviewers using a predefined data collection form. Extracted variables included year of publication, country, study design, patient selection criteria, surgical technique, use of CME, sample size, demographic characteristics, and reported outcomes. When continuous data were reported as medians with ranges or interquartile ranges, standard conversion methods were applied when feasible to allow quantitative synthesis.
2.6. Outcomes of Interest
Primary outcomes were the number of harvested lymph nodes, operative time, and length of hospital stay. Lymph node yield was considered a technical surrogate marker of oncological adequacy rather than a direct oncological outcome. Secondary outcomes included estimated intraoperative blood loss, conversion to open surgery, surgical site infection, readmission rate, and overall hospitalization costs.
Outcomes such as anastomotic leak, reoperation, thromboembolic events, postoperative ileus, incisional hernia, extraction site, and type of anastomosis (intracorporeal versus extracorporeal) were not included due to inconsistent reporting across studies and insufficient data for reliable quantitative synthesis. Subgroup analyses were conducted according to the use of CME (CME vs. non-CME).
2.7. Statistical Analysis
For dichotomous variables, risk ratios (RRs) with 95% confidence intervals (CIs) were calculated. Continuous outcomes were analyzed using weighted mean differences (WMDs) when outcomes were reported using comparable units, or standardized mean differences (SMDs) when different measurement scales or reporting methods were used. The use of standardized mean difference was primarily applied to blood loss and cost analyses due to heterogeneity in reporting units and calculation methods across studies.
Meta-analyses were performed using the Mantel–Haenszel method. Given the expected clinical and methodological heterogeneity, a random-effects model was applied for all analyses. Statistical heterogeneity was assessed using the Chi-square test and quantified by the I^2^ statistic, with values above 75% indicating substantial heterogeneity. Pooled estimates associated with high or extreme heterogeneity were interpreted with caution and considered exploratory. All analyses were conducted using Review Manager (RevMan) software version 5.3.5 (The Nordic Cochrane Centre, Copenhagen, Denmark).
2.8. Risk of Bias Assessment
The methodological quality of non-randomized studies was evaluated using the Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I) tool. Risk-of-bias judgments were classified as low, moderate, serious, or critical according to ROBINS-I guidance. Particular attention was paid to bias due to confounding, participant selection, and missing data, which were anticipated limitations of observational study designs. Graphical summaries of the risk-of-bias assessment were generated using the ROBVIS online visualization platform.
3. Results
3.1. Study Selection
The literature search yielded 3,220 records. After removal of 437 duplicates, 2,783 records were screened by title and abstract. Of these, 2,574 were excluded for not meeting the inclusion criteria. Sixty-one full-text articles were assessed for eligibility, resulting in the exclusion of 31 studies. Ultimately, 46 studies were included in the qualitative and quantitative synthesis. The study selection process is illustrated in Figure 1.
3.2. Study Characteristics
The 46 included studies comprised a total of 36,868 patients, of whom 6,312 underwent robotic surgery, and 30,547 underwent laparoscopic surgery. Most studies were conducted in Europe (45.7%), followed by Asia (21.7%) and other regions, including the United States, Russia, and Australia. Publication years ranged from 2003 to 2025. Detailed study characteristics and patient demographics are summarized in Table 1 and Table 2.
3.3. Risk of Bias Within Studies
According to the ROBINS-I assessment, the methodological quality of included studies was variable. Most studies were judged to have low to moderate risk of bias overall, while several demonstrated moderate or high risk in specific domains, particularly confounding, participant selection, and missing data. No study was classified as having a critical risk of bias. A comprehensive overview of the risk-of-bias assessment is presented in Figure 2.
3.4. Description of Studies
A total of 46 studies involving 36,868 patients (6,312 robotic and 30,547 laparoscopic) were included. The majority of studies (21 out of 46, 45.7%) were conducted in Europe, enrolling 4,321 patients (12%), with Italy contributing the highest number (15 studies). A total of 10 studies (21.7%) were performed in Asia, comprising 9,081 patients (24.6%). The remaining 14 studies (30.4%) were distributed as follows: 12 in the USA, 1 in Russia, and 1 in Australia. All included studies were published between 2003 and 2025. A detailed description of study characteristics and patient demographics is provided in Table 1.
3.5. Assessment of Risk of Bias in Included Studies
The risk of bias in the included studies was independently assessed by two authors (RC, MS).
According to the ROBINS-I tool, risk-of-bias judgment may be identified as low, moderate, serious, or critical. In total, 39 out of 46 studies were assessed as low risk of overall bias, while 7 were determined to have a moderate risk, and none had a high risk. Regarding bias due to confounding, 21 out of 46 studies were evaluated as having a low risk. Additionally, 17 studies were reported to have a moderate risk, and 7 had a high risk of bias due to confounding. In the analysis of the selection bias of study participants, 17 out of 46 reviews were evaluated as low risk and 8 as high risk. Regarding bias in the classification of the interventions, all studies had a low risk apart from five, which had a moderate risk. The risk of bias due to deviation from intended interventions was moderate in five studies and high in six studies. The evaluation of missing data bias reported that 11 studies had a low risk, 5 had a high risk, and the remaining had a moderate risk. Regarding bias in the selection of the measurement of the outcomes, 15 out of the 46 studies had a low risk, and 6 had a high risk. Additionally, for bias in the reported results, all studies were assessed as having a low risk, apart from seven that had a moderate risk and one that had a high risk, as shown in Figure 1.
4. Primary Outcomes
4.1. Retrieved Lymphatic Nodes
Seven retrospective observational studies [3,5,8,9,25,29,32] reported lymph node yield for CME procedures (1,486 patients: 690 robotic vs. 796 laparoscopic). The overall number of harvested lymph nodes was numerically higher in the robotic group (MD 1.34, 95% CI −0.59 to 3.27), although this difference was not statistically significant. Heterogeneity was substantial (I^2^ = 72%) (Figure 3).
In the non-CME subgroup, seventeen retrospective and prospective studies [4,6,7,10,13,15,17,19,20,21,23,24,27,28,30,34,36,39,40,41,43] have been reported on lymph node retrieval. Robotic surgery was associated with a statistically significant increase in lymph node yield compared with laparoscopy; however, heterogeneity was high (I^2^ = 84%) (Figure 4).
4.2. Operation Time
A total of 8 retrospective observational studies [3,5,8,9,18,25,26,32] reported operative times for 1468 patients in the CME group. Operative time was longer in the robotic group compared with laparoscopy (MD 25.73, 95% CI 13.75 to 37.70), with substantial heterogeneity (I^2^ = 82%) (Figure 5).
A total of 28 retrospective and prospective observational studies [6,7,10,13,16,17,19,20,21,22,23,24,26,27,28,33,34,35,36,37,40,41,42,43,44,45,46] reported operative time for 12,622 patients in the non-CME group. Operative time was longer in the robotic group compared with laparoscopy (MD 42.45, 95% CI 30.33 to 54.57), with considerable heterogeneity (I^2^ = 98%) (Figure 6).
4.3. Length of Hospital Stays
A total of 8 retrospective observational studies [3,8,9,18,25,26,29,32] reported the length of hospital stay for 1,206 patients undergoing CME. Hospital stays showed no clinically meaningful difference between approaches in this subgroup (Figure 7).
A total of 22 prospective and retrospective studies [4,7,13,17,19,20,21,23,24,27,28,30,36,37,39,40,41,42,43,44,45,46] involving 11,668 patients reported the length of hospital stay for non-CME procedures. A trend toward shorter hospitalization with robotic surgery was observed in more recent studies; overall heterogeneity was moderate (I^2^ = 74%) (Figure 8).
5. Secondary Outcomes
5.1. Estimated Blood Loss
Five retrospective observational studies [8,9,18,25,29] reported estimated blood loss for the CME subgroup (919 patients). No statistically significant difference was observed between approaches (MD 5.65, 95% CI −12.03 to 23.33), with substantial heterogeneity (I^2^ = 78%) (Figure 9).
Fifteen prospective and retrospective studies [6,7,15,19,24,27,30,34,36,37,39,41,42,43,44,45,46] reported blood loss for the non-CME subgroup (2,806 patients). Robotic surgery was associated with lower estimated blood loss (SMD −0.38, 95% CI −0.57 to −0.20), with high heterogeneity (I^2^ = 76%) (Figure 10).
5.2. Conversion from Minimally Invasive to Open Right Hemicolectomy
A total of 3 retrospective observational studies [5,29,32] including 851 patients, reported conversion rates for the CME subgroup. Conversion occurred in 1% versus 10% of cases in the robotic and laparoscopic groups, respectively. Robotic surgery was associated with a lower conversion rate (RR 0.12, 95% CI 0.05 to 0.28) (Figure 11).
A total of 18 retrospective and prospective studies [4,7,10,12,15,20,22,27,31,33,37,38,39,41,42,43,44,45], including 10,542 patients, reported conversion rates for the non-CME subgroup. Robotic surgery was associated with a lower conversion rate compared with laparoscopy (RR 0.56, 95% CI 0.37 to 0.85), with low heterogeneity (I^2^ = 39%) (Figure 12).
5.3. Wound Infection
A total of 5 retrospective observational studies [3,5,18,25,32], including 860 patients, reported wound infection for CME procedures. No statistically significant difference was observed between approaches (RR 1.00, 95% CI 0.44 to 2.25), with low heterogeneity (I^2^ = 18%) (Figure 13).
A total of 18 retrospective and prospective studies [2,6,10,11,17,19,20,21,27,28,30,33,37,39,40,42,43,44], including 18,017 patients, reported wound infection for non-CME procedures. No statistically significant difference was observed between approaches (RR 0.89, 95% CI 0.63 to 1.27) (Figure 14).
5.4. Readmission Rate
A total of 2 retrospective observational studies [5,26], including 316 patients, reported readmission rates for CME procedures. No statistically significant difference was observed between robotic and laparoscopic approaches (RR 0.99, 95% CI 0.59 to 1.68) (Figure 15).
A total of 12 retrospective and prospective studies [4,6,7,10,11,17,21,22,24,27,30,44], including 15,874 patients, reported readmission rates for non-CME procedures. No statistically significant difference was observed between robotic and laparoscopic approaches (RR 0.75, 95% CI 0.43 to 1.31) (Figure 16).
5.5. Hospitalization Cost (Reported in US Dollars)
Four retrospective observational studies [3,5,8,9] reported hospitalization costs for CME procedures (823 patients). Robotic surgery was associated with higher hospitalization costs compared with laparoscopy (SMD 5.34, 95% CI 3.50 to 7.18), with extreme heterogeneity (I^2^ = 99%) (Figure 17).
Eight retrospective and prospective studies [13,16,21,23,43,44,45,46] reported hospitalization costs for non-CME procedures (626 patients). No statistically significant difference was observed between approaches (SMD 0.27, 95% CI −0.41 to 0.94), with substantial heterogeneity (I^2^ = 92%) (Figure 18).
6. Discussion
Right-sided colon cancer surgery remains technically demanding due to the anatomical complexity of mesocolic planes, vascular variability, and lymphatic drainage patterns. The introduction of complete mesocolic excision (CME), aimed to improve oncological radicality by applying the principles of embryological plane dissection to colon cancer surgery. Over the past two decades, minimally invasive approaches have progressively replaced open surgery, with laparoscopic right hemicolectomy becoming widely adopted as a standard technique [4,5].
More recently, robotic platforms have been introduced with the aim of overcoming some intrinsic limitations of laparoscopy, including restricted instrument articulation, two-dimensional visualization, and ergonomic constraints [5,16]. The present systematic review and meta-analysis synthesized data from 46 comparative studies published between 2003 and 2025, including more than 36,000 patients, to evaluate perioperative and short-term outcomes of robotic versus laparoscopic right hemicolectomy, stratified by CME and non-CME techniques. Given the observational nature of most included studies and the substantial heterogeneity observed across several outcomes, the findings should be interpreted with appropriate caution.
Lymph node yield represents a technical surrogate marker of oncological adequacy rather than a direct measure of oncological effectiveness. In this analysis, robotic surgery was associated with a modest increase in the number of retrieved lymph nodes, particularly in non-CME procedures [6,7,10,13,17,19,20,21,23,24,27,28,30,34,36]. However, the absolute differences were small and characterized by high heterogeneity, suggesting that factors such as surgeon experience, learning-curve effects, institutional protocols, and patient selection may have contributed substantially to these findings. Importantly, no conclusions regarding oncological superiority can be drawn in the absence of long-term outcomes such as disease-free or overall survival, which were not consistently reported across the included studies.
Operative time consistently favored the laparoscopic approach in both CME and non-CME subgroups [3,5,8,9,18,26,29,32]. This finding remained stable across different publication periods and likely reflects the additional setup time, docking procedures, and technical complexity associated with robotic surgery, particularly during earlier phases of adoption. While operative duration is an important efficiency metric, its clinical relevance should be interpreted in the context of overall perioperative outcomes and institutional expertise.
Length of hospital stay showed no clinically meaningful differences between approaches in most analyses, although a trend toward shorter hospitalization with robotic surgery was observed in more recent non-CME studies [6,7,13,17,19,20,21,23,24,27,28,30,36]. This temporal pattern may reflect increasing familiarity with robotic platforms, improvements in perioperative care, and enhanced recovery protocols rather than an intrinsic advantage of the surgical approach itself.
Among secondary outcomes, robotic surgery demonstrated lower conversion rates to open surgery in both CME and non-CME procedures [5,29,32]. This finding may be related to improved visualization, instrument articulation, and ergonomic advantages offered by robotic systems, particularly in technically challenging cases. Estimated blood loss was generally low in both approaches, with a modest advantage for robotic surgery in non-CME procedures [6,7,15,19,24,27,30,34,36]; however, variability in reporting methods and measurement techniques limits the interpretability of this outcome.
No significant differences were observed in wound infection or readmission rates between robotic and laparoscopic approaches [3,5,18,25,32]. It should be noted that definitions of surgical site infection varied across studies, and important postoperative complications such as anastomotic leak, reoperation, thromboembolic events, postoperative ileus, and incisional hernia could not be analyzed due to inconsistent reporting. Similarly, data regarding anastomotic technique (intracorporeal versus extracorporeal), extraction site, patient comorbidities, and neoadjuvant treatments were insufficient for meaningful quantitative synthesis.
Cost analysis represented one of the most heterogeneous outcomes, reflecting differences in healthcare systems, reimbursement models, institutional accounting methods, and the long study period considered [3,5,8,9,13,16,21,23,43,44,45,46]. While laparoscopic surgery was generally associated with lower costs, particularly in CME procedures, these findings should be regarded as exploratory and not directly comparable across settings.
Overall, the substantial heterogeneity observed across multiple outcomes underscores the influence of non-technical factors, including study design, geographic region, surgeon expertise, and temporal evolution of surgical technology. These elements limit the strength of pooled estimates and highlight the need for cautious interpretation.
7. Conclusions
This systematic review and meta-analysis suggest that both robotic and laparoscopic right hemicolectomy are safe and effective minimally invasive approaches, each associated with distinct technical and perioperative characteristics. Robotic surgery may offer advantages in terms of conversion rates and selected technical surrogate markers, while laparoscopic surgery remains more efficient with respect to operative time and overall costs.
However, the observed differences are generally modest and characterized by substantial heterogeneity, limiting definitive conclusions regarding clinical or oncological superiority. In the absence of robust long-term oncological outcomes and standardized reporting of key postoperative complications, surgical approach selection should be guided by surgeon expertise, institutional resources, patient characteristics, and procedural complexity rather than by expectations of inherent superiority.
Future prospective studies and randomized trials with standardized outcome definitions, long-term follow-up, and detailed reporting of perioperative variables are needed to better define the role of robotic surgery in right-sided colon cancer and to clarify its potential benefits within contemporary surgical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lin C.-Y. Liu Y.-C. Chen C.-C. Chen M.-C. Chiu T.-Y. Huang Y.-L. Chiang S.-W. Lin C.-L. Chen Y.-J. Lin C.-Y. Robotic-assisted colon cancer surgery: Faster recovery and less pain compared to laparoscopy in a retrospective propensity-matched study Cancers 20251724310.3390/cancers 1702024339858025 PMC 11764117 · doi ↗ · pubmed ↗
- 2Lu C.-C. Lu C.-T. Chang K.-Y. Chun-Li W. Wu C.-Y. Robot-assisted vs. laparoscopic right hemicolectomy in octogenarians and nonagenarians: An analysis of the US nationwide inpatient sample 2005–2018 Aging Clin. Exp. Res.20243619310.1007/s 40520-024-02833-439311977 PMC 11420325 · doi ↗ · pubmed ↗
- 3Chen E. Zhang W. Chen L. Robotic right colectomy versus laparoscopic right colectomy in patients with right colon cancer: A comparative study BMC Surg. Endosc.2024352039204810.1186/s 12893-024-02593-y 39455989 PMC 11515452 · doi ↗ · pubmed ↗
- 4Farah E. Abreu A.A. Rail B. Salgado J. Karagkounis G. Zeh H.J.III Polanco P.M. Perioperative outcomes of robotic andlaparoscopic surgery for colorectal cancer: A propensity score-matched analysis World J. Surg. Oncol.20232127210.1186/s 12957-023-03138-y 37644538 PMC 10466759 · doi ↗ · pubmed ↗
- 5Tian Y. Xiong D. Xu M. Fan Q. Zheng H. Shen H. Huang B. Wang L. Li C. Zhang A. Robotic versus laparoscopic right hemicolectomy with complete mesocolic excision: A retrospective multicenter study with propensity score matching Front. Oncol.202313118747610.3389/fonc.2023.118747637333806 PMC 10273266 · doi ↗ · pubmed ↗
- 6de’Angelis N. Schena C.A. Espin-Basany E. Piccoli M. Alfieri S. Aisoni F. Coccolini F. Frontali A. Kraft M. Lakkis Z. Robotic versus laparoscopic right colectomy for nonmetastatic p T 4 colon cancer: A European multicentre propensity score-matched analysis Color. Dis.2024261576158510.1111/codi.1708938978153 · doi ↗ · pubmed ↗
- 7de’Angelis N. Piccoli M. Casoni Pattacini G. Winter D.C. Carcoforo P. Celentano V. Coccolini F. Di Saverio S. Frontali A. Fuks D. Right colectomy with Intracorporeal anastomosis: A European multicenter propensity score matching retrospective study of robotic versus laparoscopic procedures World J. Surg.2023472039205110.1007/s 00268-023-07031-337188971 · doi ↗ · pubmed ↗
- 8Bin H. Tian Y. Zheng H. Tong W. Yao H. Short- to mid-term efficacy of robot-assisted versus laparoscopic-assisted right hemicolectomy with complete mesocolic excision for right-sided colon cancer: A single-center and single-surgeon experience China J. Gen. Surg.20233249750510.7659/j.issn.1005-6947.2023.04.003 · doi ↗