Perioperative Ozoralizumab Management for Patients with Rheumatoid Arthritis Who Underwent Orthopaedic Surgery: A Retrospective Case Series
Keiichiro Nishida, Yoshihisa Nasu, Ryozo Harada, Ryuichi Nakahara, Masahiro Horita, Masamitsu Natsumeda, Shuichi Naniwa, Toshifumi Ozaki

TL;DR
This study examines the safety of stopping ozoralizumab before surgery in rheumatoid arthritis patients, finding no major complications.
Contribution
Provides first evidence on perioperative management of ozoralizumab in rheumatoid arthritis patients undergoing surgery.
Findings
No surgical site infections or delayed wound healing occurred after ozoralizumab discontinuation.
A mean discontinuation period of 34.9 days was observed without major complications.
One patient experienced a rheumatoid arthritis flare before resuming ozoralizumab.
Abstract
Background/Objectives: Launched in Japan in 2022, ozoralizumab (OZR) is a novel, anti-tumour necrosis factor (TNF)-α inhibitor for treating rheumatoid arthritis (RA) that is refractory to conventional therapies. However, there is a lack of evidence regarding its perioperative management. Methods: This retrospective case series included nine patients with RA who underwent a total of 12 either RA-related (n = 9) or unrelated (n = 3) orthopaedic procedures. We reviewed patient demographics, surgical procedures, perioperative OZR discontinuation periods, and postoperative complications. Results: The mean preoperative OZR discontinuation period was 15.8 days (range, 2–25 days). Sutures were removed at a mean of 12.8 days postoperatively (range, 11–14 days) after adequate wound healing had been confirmed. The mean total discontinuation period was 34.9 days (range, 27–43 days). No cases of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
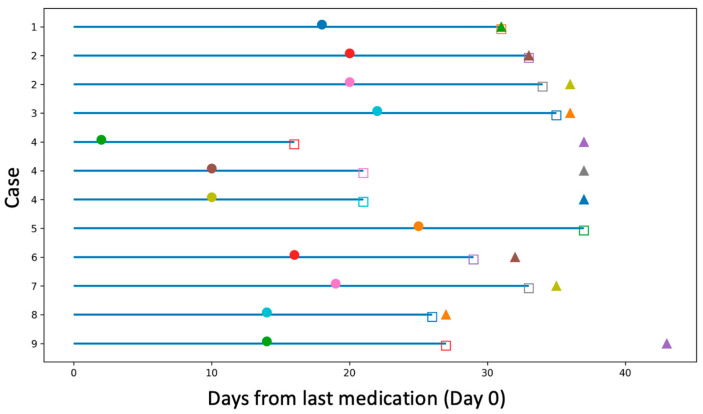 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRheumatoid Arthritis Research and Therapies · Medical and Biological Ozone Research · Spondyloarthritis Studies and Treatments
1. Introduction
Launched in Japan in December 2022, ozoralizumab (OZR) is a novel, anti-tumour necrosis factor (TNF)-α inhibitor for patients with rheumatoid arthritis (RA) who display an inadequate response to conventional therapies [1]. OZR is a small-molecule antibody preparation based on Nanobody^®^ (Ablynx NV, Ghent, Belgium) technology, consisting of a single-domain antibody derived from the variable region of llama heavy-chain antibodies. With a molecular weight of 38 kDa—approximately a quarter that of conventional immunoglobulin G [2]—OZR may access disease target sites that are less accessible to traditional antibodies.
Preclinical studies have demonstrated that OZR has an extended half-life due to its albumin-binding moiety, allowing for its administration at four-week intervals [3]. However, its prolonged retention at inflammatory sites raises concerns regarding perioperative safety in orthopaedic surgery. Although several guidelines address the perioperative management of established TNF inhibitors [4,5,6], no data are currently available for OZR. This study is the first to describe the perioperative clinical course of patients with RA undergoing orthopaedic surgery while receiving OZR.
2. Patients and Methods
This retrospective case series was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Okayama University (No. 2505-043) on 17 October 2025. Written informed consent was obtained from all participants. In this study, data were collected from all patients with RA who underwent orthopaedic surgery at our institutions between 1 September 2020 and 31 March 2025 while receiving OZR therapy. All patients fulfilled the 1987 revised American College of Rheumatology criteria for RA [7].
Nine patients were included (six women and three men), with a mean age of 62.7 years (range, 40–82) and a mean disease duration of 31.9 years (range, 10–49). The mean preoperative DAS28-CRP was 2.4 (range, 1.24–3.95). Four patients used concomitant prednisolone (range, 3.5–10 mg/day), and none had diabetes mellitus. One patient (case No.5) received 80 mg/month of OZR during a clinical trial and underwent surgery after withdrawal. The remaining eight patients received treatment with OZR at 30 mg/month. The patient characteristics before surgery are summarised in Table 1.
Collected data included surgical indications, procedure types, preoperative OZR discontinuation period, time to suture removal, total discontinuation period, and postoperative complications, including surgical site infection (SSI), delayed wound healing (DWH), and RA flare. SSI was defined according to the 2013 United States Center for Disease Control and Prevention guidelines for the prevention of SSI by National Healthcare Safety Network (available at: https://apic.org/Resource_/TinyMceFileManager/Academy/ASC_101_resources/Surveillance_NHSN/ASCA_NHSN_SSI_Surveillance_2013.pdf) (accessed on 13 January 2026). DWH was defined as cases where suture removal was later than 2 weeks after surgery or where re-suturing was required [8].
3. Results
The patients underwent a total of 12 procedures related (n = 9) or unrelated (n = 3) to the RA. One patient (case No.2) underwent two surgeries within a 10-month interval. Another (case No.4) suffered multiple traumas two days after OZR administration; this patient underwent emergency surgery for an open fracture of the femur on the day of injury, and open reduction and internal fixation for a fractured radius and posterior lumbar fusion with vertebroplasty for lumbar fracture 8 days after injury. The mean preoperative OZR discontinuation period was 15.8 (range, 2–25) days. Sutures were removed at a mean of 12.8 (range, 11–14) days postoperatively after wound healing had been confirmed. The mean total OZR discontinuation period was 34.9 (range, 31–37) days. No cases of SSI or DWH were observed during at least three months of follow-up. One patient (case No.4) experienced a flare-up of the disease before restarting OZR (Table 2).
The timing of medication discontinuation, surgery, suture removal, and treatment resumption was visualised using a swimmer plot, with time expressed as days from the last medication dose (Day 0) and repeated procedures in the same patient shown as separate entries (Figure 1).
4. Discussion
It has been recognised that continuing biologic disease-modifying anti-rheumatic drugs (bDMARD) in the perioperative period of orthopaedic surgery poses the potential risk of increasing SSI and DWH [9]. Longer withdrawal periods decrease such risks, but increase the chance of disease flare-ups. The patient panel participating in the ACR/AAHKS guidelines for total hip and knee arthroplasties considered the risk of infection to be much more important than the risk of flare [10]. As the British Society of Rheumatology guideline stated, “the potential benefit of preventing post-operative infections by stopping biologics should be balanced against the risk of a peri-operative flare in disease activity” [11]. The Japan College of Rheumatology clinical practice guidelines for managing rheumatoid arthritis recommend discontinuing bDMARD in the perioperative period of orthopaedic surgery (strength of recommendation: weak) [6]. In terms of the bDMARD discontinuation period, several guidelines agree that they should be withheld one dosing cycle before surgery and restarted after good surgical wound healing has been confirmed, usually around 14 days after the surgery [12,13]. However, there are no available data on OZR management, as perioperative experience with this relatively new drug is limited.
This retrospective case series is the first to report the clinical course of RA patients who underwent orthopaedic surgeries under OZR disease control. In this study, four of the nine patients used glucocorticoid (GC), while seven used conventional synthetic disease-modifying anti-rheumatic drugs (csDMARDs), including methotrexate (MTX). GC and csDMARDs may have provided a bridging effect in controlling disease activity during OZR discontinuation. Because it has been suggested that withholding MTX perioperatively increases the risk of flares without increasing the rate of SSI and DWH, most guidelines recommend continuing MTX use throughout this period [13]. In addition, since bDMARDs are typically introduced as add-on therapy when disease control is inadequate, the effect of the continued use of GC and csDMARDs on disease flare is likely limited compared to perioperative bDMARD discontinuation.
Whether surgery timing should be determined according to their half-life or administration interval has not been well addressed, particularly since the latter is decided based on drug pharmacokinetics (PK) [14]. For TNF inhibitors with similar half-lives, such as adalimumab and certolizumab pegol (both of which have half-lives of approximately 14 days) [11], surgery is recommended at 3 weeks after the last dose, i.e., within the period when effective blood concentrations are maintained. It is recommended that another TNF-inhibitor, Golimumab (also with a half-life of approximately 14 days), be withheld for 4 weeks before surgery (after one dosing interval). In our experience, similar perioperative management did not pose a risk for postoperative infection- or wound healing-related complications [15]. It remains unclear why surgery was safe even when plasma concentrations remained within the therapeutic range. The uniquely small molecular weight of OZR may not be relevant to postoperative infection or wound healing.
In this study, all procedures were performed within 4 weeks after OZR discontinuation. Takeuchi et al. investigated the PK profile of OZR in Japanese patients with RA from the OHZORA and NATSUZORA trials. They found the t_1/2_ of OZR to be 18.2 days due to its ability to bind to human serum albumin [16]. The PK simulation showed that the estimated trough concentration of OZR was 1.2 μg/mL when 30 mg was administered at 6-week intervals, which was not below the cutoff value (1.0 μg/mL) derived from the ROC analysis of ACR20 or ACR50 response rates and trough concentrations [16]. Therefore, theoretically, if surgery is performed within 4 weeks (one dosing cycle) of the last OZR administration and OZR is restarted at two weeks postoperatively after the confirmation of wound healing, the plasma OZR concentration would not decrease below therapeutic levels. However, the effective blood concentration cutoff varies per patient and is influenced by body weight, severity of RA-related inflammation, immunogenicity, and concomitant medications such as MTX. It should be noted that pharmacokinetic extrapolation methods have not yet been directly validated in perioperative care.
One of the important observations of the present study was the absence of wound-related complications, even in patients (Case No.4) who sustained multiple traumas and underwent emergency surgery on day 2 after OZR administration. As this patient had additional surgery 8 days later, systemic inflammation persisted, with CRP levels exceeding 70 mg/L until day 14 after traumatic injury. The absence of SSI or DWH, coupled with postoperative disease flare, might be related to the depletion of initial high-concentration OZR due to bleeding from the multiple traumas and surgical injury; alternatively, it might be related to the increased OZR consumption due to elevated TNF production during systemic inflammation. Surgeons should also consider the clinical status of patients, such as their age, disease duration and activity, surgery type, and comorbidities, all of which might influence SSI and DWH development.
There is no clear evidence regarding the optimal time to restart bDMARDs in the postoperative setting, and this approach is based on standard precautions that warn against its use in patients with active infection, such as those with open wounds [10]. In patients with rheumatic diseases undergoing total joint arthroplasty, Goodman et al. described that “antirheumatic therapy should be restarted once the wound shows evidence of healing, any sutures/staples are out, there is no significant swelling, erythema, or drainage, and there is no ongoing nonsurgical site infection, which is typically ~14 days” [10]. In the current study, no complications occurred in the surgical wound, and the average period until stitch removal was approximately 13 days.
Several limitations of this study should be acknowledged. Firstly, its small sample size, absence of a control group, and retrospective nature limit the generalizability of the conclusions regarding OZR’s perioperative safety. In addition, due to the small sample size, we were unable to compare the results of low- and high-risk procedures to determine whether the preoperative discontinuation period of up to 4 weeks is equally safe across different levels of surgical complexity. Secondly, most patients had relatively well-controlled disease activity without major metabolic comorbidities such as diabetes mellitus, which might affect the SSI and DWH rates. Thirdly, only one patient received the higher 80 mg dose of OZR, limiting conclusions regarding dose-dependent effects.
5. Conclusions
In conclusion, the present study provides preliminary clinical evidence that withholding OZR up to 4 weeks before orthopaedic surgery and restarting it after wound healing has been confirmed to represent a reasonable perioperative management strategy, although individualised decision-making remains essential. More data from larger prospective or retrospective multicentre studies are needed to establish proper perioperative OZR management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ishiwatari-Ogata C. Kyuuma M. Ogata H. Yamakawa M. Iwata K. Ochi M. Hori M. Miyata N. Fujii Y. Ozoralizumab, a Humanized Anti-TN Falpha NANOBODY((R)) Compound, Exhibits Efficacy Not Only at the Onset of Arthritis in a Human TNF Transgenic Mouse but Also During Secondary Failure of Administration of an Anti-TN Falpha Ig G Front. Immunol.20221385300810.3389/fimmu.2022.85300835273620 PMC 8902368 · doi ↗ · pubmed ↗
- 2Tanaka Y. Ozoralizumab: First Nanobody(R) therapeutic for rheumatoid arthritis Expert. Opin. Biol. Ther.20232357958710.1080/14712598.2023.223134437431762 · doi ↗ · pubmed ↗
- 3Oyama S. Ebina K. Etani Y. Hirao M. Kyuuma M. Fujii Y. Iwata K. Ogawa B. Hasegawa T. Kawano S. A novel anti-TNF-alpha drug ozoralizumab rapidly distributes to inflamed joint tissues in a mouse model of collagen induced arthritis Sci. Rep.2022121810210.1038/s 41598-022-23152-636302840 PMC 9613905 · doi ↗ · pubmed ↗
- 4Khader S.G. Hussain W.H.Z. Moorthy A. Rheumatology patients on immunosuppressive treatment and their perioperative management: Review of recommendations Musculoskelet. Care 20232157157510.1002/msc.172136461920 · doi ↗ · pubmed ↗
- 5Rezaieyazdi Z. Sahebari M. Khodashahi M. Preoperative Evaluation and Management of Patients Receiving Biologic Therapies Arch. Bone Jt. Surg.2019722022831312678 PMC 6578481 · pubmed ↗
- 6Ito H. Nishida K. Kojima T. Matsushita I. Kojima M. Hirata S. Kaneko Y. Kishimoto M. Kohno M. Mori M. Non-drug and surgical treatment algorithm and recommendations for the 2020 update of the Japan College of Rheumatology clinical practice guidelines for the management of rheumatoid arthritis-secondary publication Mod. Rheumatol 202333364510.1093/mr/roac 01935294030 · doi ↗ · pubmed ↗
- 7Arnett F.C. Edworthy S.M. Bloch D.A. Mc Shane D.J. Fries J.F. Cooper N.S. Healey L.A. Kaplan S.R. Liang M.H. Luthra H.S. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis Arthritis Rheum.19883131532410.1002/art.17803103023358796 · doi ↗ · pubmed ↗
- 8Kadota Y. Nishida K. Hashizume K. Nasu Y. Nakahara R. Kanazawa T. Ozawa M. Harada R. Machida T. Ozaki T. Risk factors for surgical site infection and delayed wound healing after orthopedic surgery in rheumatoid arthritis patients Mod. Rheumatol.201626687410.3109/14397595.2015.107313326357931 · doi ↗ · pubmed ↗