Operationalizing Co-Design in Exercise Interventions with Indigenous Peoples in Australia: Development and Cultural Adaptation of the PrIDE Tools
Morwenna Kirwan, Connie Henson, Blade Bancroft-Duroux, Kerri Colegate, Cheryl Taylor, David Meharg, Neale Cohen, Kylie Gwynne

TL;DR
This paper describes the development of culturally adapted exercise tools for Indigenous Australians to address diabetes and heart disease through co-design and transparent methods.
Contribution
The study introduces the PrIDE tools, developed through Indigenous-governed co-design and systematic cultural adaptation frameworks.
Findings
Four culturally adapted tools were developed using Indigenous governance and frameworks like CHRI and COM-B.
Transparent documentation via MADI supports reproducibility and cultural safety in health interventions.
The Success Plan integrates clinical yarning into routine practice for culturally congruent care.
Abstract
Public health relevance—How does this work relate to a public health issue? Indigenous Australians experience a disproportionate burden of type 2 diabetes and cardiovascular disease, with earlier onset, higher prevalence, and greater complications than other Australians, reflecting the profound impacts of colonization and ongoing structural inequities.Limited peer-reviewed evidence exists on culturally adapted exercise interventions co-designed with Indigenous Australians living with type 2 diabetes; substantial gaps remain in transparent reporting of Indigenous governance, cultural adaptation processes, and behavioral mechanisms. Indigenous Australians experience a disproportionate burden of type 2 diabetes and cardiovascular disease, with earlier onset, higher prevalence, and greater complications than other Australians, reflecting the profound impacts of colonization and ongoing…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
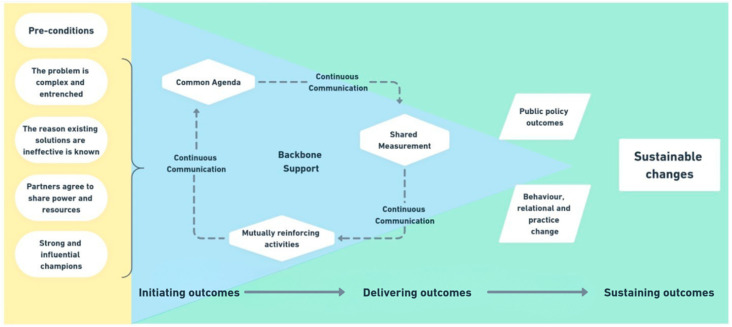 Figure 1
Figure 1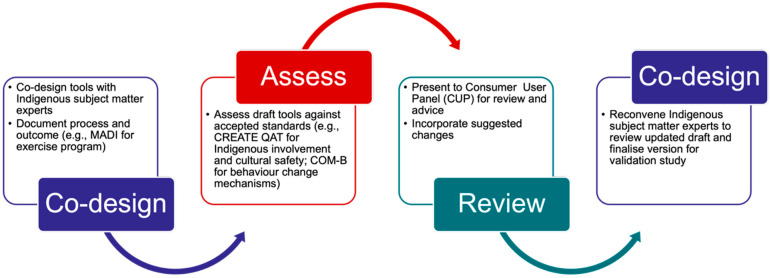 Figure 2
Figure 2 Figure 3
Figure 3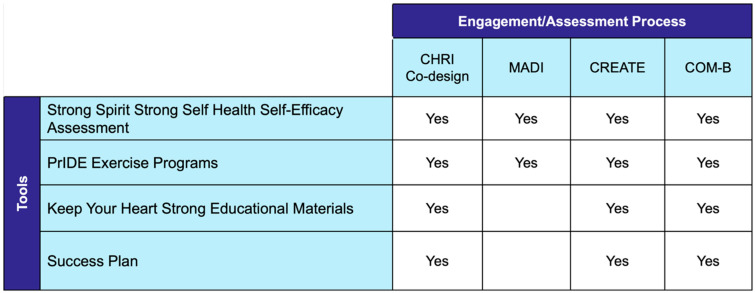 Figure 4
Figure 4 Figure 5
Figure 5- —Australian Medical Research Future Fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIndigenous Health, Education, and Rights · Health Policy Implementation Science · Athletic Training and Education
1. Introduction
Aboriginal and Torres Strait Islander peoples (hereafter referred to as Indigenous Australians) belong to the world’s oldest continuing cultures, with deep knowledge systems and strong community connections that have sustained health and wellbeing for millennia. However, the impacts of colonization and ongoing structural inequities have resulted in a disproportionate burden of type 2 diabetes (T2DM) and cardiovascular disease (CVD), characterized by earlier onset, higher prevalence, and greater complications than other Australians [1,2,3,4]. These disparities reflect the profound impact of social, cultural, historical, and structural determinants of health [5]. Addressing these health inequities through culturally safe, community-led approaches is essential for advancing health equity and honoring Aboriginal and Torres Strait Islander peoples’ right to health and self-determination [6,7,8].
Regular, structured exercise is central to T2DM management and CVD prevention [9,10]. Clinician-led, community-based group exercise interventions have improved glycemic control, physical function, cardiovascular risk factors, and psychosocial outcomes in adults with T2DM, indicating effectiveness in general populations [10,11]. However, this evidence cannot be assumed to transfer directly to Indigenous populations [12,13,14]. A systematic review of community-based exercise interventions with Indigenous peoples from high-income colonized countries managing T2DM identified limited published evidence, with substantial heterogeneity in design, delivery, and reporting [15].
International evidence is limited but suggests promise. In one supervised group exercise intervention with Indigenous Polynesian adults with T2DM, participants demonstrated improvements in cardiometabolic outcomes and quality of life [16,17]. However, this study emphasized outcomes rather than documenting development processes, Indigenous governance, or cultural adaptation approaches, limiting reproducibility and knowledge translation to other Indigenous populations. This scarcity is reinforced by a systematic review of exercise-based interventions for Indigenous adults, which – although focused on chronic lung disease rather than T2DM—identified only one eligible study and highlighted inconsistent reporting of Indigenous governance, engagement, and cultural safety processes [18]. These findings suggest that limited transparency in co-design and governance is a broader issue in Indigenous exercise intervention research, extending beyond specific disease contexts.
Several exercise programs involving Indigenous Australians are described in the gray literature; however, few report peer-reviewed outcomes or provide sufficiently detailed, repeatable methods to support replication [19,20]. One notable exception is the Ironbark Program [21,22,23], a community-based fall prevention intervention for older Indigenous Australians incorporating group exercise and yarning. The program demonstrated improvements in physical function and high acceptability. While Ironbark provides an important example of culturally safe exercise delivery, its primary focus was feasibility and outcomes rather than systematic documentation of Indigenous-governed cultural adaptation processes or behavior change mechanisms. Together, this literature highlights a critical gap in exercise interventions developed with Indigenous Australians living with T2DM, where transparent, replicable documentation of cultural adaptation processes—particularly when grounded in behavioral theory—remains largely absent.
Against this background, the national Beat It program provided a strong evidence base for cultural adaptation. The Diabetes Australia program represents one of Australia’s most established evidence-based exercise interventions for adults with T2DM. Delivered as an eight-week supervised program by Accredited Exercise Physiologists (AEPs), the Beat It program has been found to improve physical function, strength, and psychosocial outcomes [24], with benefits maintained at 12-month follow-up [25]. The program has proven adaptable across diverse contexts, including online delivery [26] and cultural adaptation for Mandarin-speaking Chinese Australians [27]. Qualitative research identified core mechanisms supporting program success: clinician supervision, group cohesion, capability building, individualized adaptation, and delivery flexibility [28]. This body of work establishes Beat It as a mature, evidence-based program with well-articulated mechanisms.
Co-design has emerged as an effective method for developing culturally safe, acceptable, and effective health interventions [29]. Recent T2DM initiatives demonstrate the value of privileging Indigenous knowledge systems, lived experience, and governance throughout program development [30,31]. Internationally the OL@-OR@ mHealth program co-designed with Māori and Pasifika communities demonstrated that transparent Indigenous-governed co-design enhanced acceptability, engagement, and trust, even when short-term clinical effects were modest [32]. This finding highlights an important principle: documenting development processes matters as much as evaluating outcomes, because cultural safety and community trust are prerequisites for effectiveness and scalability [6,7]. A systematic review of Indigenous health interventions found frequent claims of cultural adaptation; however, Indigenous leadership, governance, and deep participation in intervention design were uncommon, with many studies relying on consultation rather than shared decision-making [14].
Despite these advances, substantial gaps remain. Many interventions labeled “co-designed” provide limited methodological detail on cultural adaptation decisions, how Indigenous governance shaped content, or how Indigenous knowledge systems informed theoretical mechanisms [29], a limitation also noted in a recent systematic review of Indigenous health intervention research [14]. The Preventing Indigenous CVD and Diabetes through Exercise (PrIDE) study was developed to address these gaps. The PrIDE study represents a co-designed adaptation of Beat It incorporating wearable technology for T2DM prevention and management and CVD risk reduction [33].
This paper reports the co-design and development of four PrIDE tools: the culturally adapted PrIDE Exercise Program, the Strong Spirit Strong Self self-efficacy assessment, Keep Your Heart Strong educational materials, and the Success Plan. In the PrIDE study protocol, these tools were identified as Phase 1 outputs (1, 3, and 5) [33]. By providing transparent documentation of cultural adaptation processes and theory-informed design decisions, this work offers practical guidance for operationalizing co-design of evidence-based exercise interventions with Indigenous Australians.
2. Materials and Methods
2.1. Study Design and Governance
This study employed a co-design approach underpinned by the Co-design Health Research and Innovation (CHRI) model [34], which emphasizes collective impact, power sharing, and resource sharing throughout the research process. The CHRI model privileges Indigenous perspectives and knowledges, recognizes community contributions meaningfully, and considers sustainability from the outset [34].
Indigenous governance was established at two levels. First, the CHRI Consumer Advisory Group (CAG), chaired by Associate Professor Cara Cross, a Worimi/Biripai (North Coast of New South Wales) Indigenous Australian woman, provided overarching governance across all CHRI research projects, meeting quarterly to review research plans and ensure consumer-focused, accessible, and meaningful research. Second, a project-specific Consumer User Panel (CUP) was established to provide dedicated cultural oversight and community voice specifically for the PrIDE study. The CUP comprised four Aboriginal and/or Torres Strait Islander members with deep community connections, representing diverse nations and bringing varied perspectives across age, gender, and health experiences. The CUP provided cultural guidance throughout tool development, including input into design, review of materials for clarity and cultural safety, and ensuring local cultural and community perspectives were centered.
2.2. The CHRI Model of Co-Design
The CHRI model (Figure 1) requires four pre-conditions to be met: the problem is complex and entrenched, the reason that existing solutions are ineffective is known, partners agree to share power and resources, and strong and influential champions are present. The model emphasizes the collective rather than individuals or hierarchies, aligns with respectful engagement and decision-making with Indigenous Elders and communities, enabling significant and measurable improvement to complex health challenges [34]. Adapted from collective impact [35], the CHRI model incorporates five conditions for collective impact: common agenda, backbone support, continuous communication, shared measurement, and mutually reinforcing activities. These conditions support progression through three phases: initiating outcomes, delivering outcomes, and sustaining outcomes. The model ultimately aims to achieve sustainable changes through public policy outcomes and behavior, relational, and practice change [34].
For the PrIDE tool development, the pre-conditions were established through recognition of the complex and entrenched nature of T2DM and CVD in Indigenous Australian communities, understanding the barriers to the existing interventions, an agreement to share power and resources through the CUP governance structure, and leadership from Indigenous investigators and community champions. The tool development phase focused on initiating outcomes through establishing a common agenda for culturally adapted and newly developed tools, providing backbone support through the CHRI infrastructure, maintaining continuous communication through yarning circles, implementing shared measurement through the Aboriginal and Torres Strait Islander Quality Appraisal Tool, and engaging in mutually reinforcing activities across the co-design team. The delivering and sustaining outcomes phases will occur during program implementation and evaluation.
The CHRI model recognizes community contributions in meaningful and significant ways, including opportunities to participate as co-authors on publications and creating local employment opportunities such as Indigenous research assistants [34].
2.3. Indigenous Research Methodologies
Yarning circles were used as the primary method for knowledge sharing and co-design. Yarning, an Indigenous research methodology, is a conversational method that involves storytelling and knowledge sharing, emphasizing the establishment of a level platform for knowledge exchange between all participants, recognizing each individual as expert in their own right, and promoting open sharing of experiences and ideas [36]. Between 3 and 5 yarning sessions were conducted for each tool. CUP yarning sessions were held in Bidjigal Country (Sydney, NSW, Australia) or online in 2025.
2.4. Ethical Approval
Ethics approval was obtained from the Aboriginal Health and Medical Research Council of NSW (AHMRC) (Approval #2479/25). The study was conducted in accordance with the National Health and Medical Research Council (NHMRC) guidelines for ethical research with Indigenous communities [37].
2.5. Tool Development Process
Four tools were developed using the CHRI co-design model in parallel: three culturally adapted tools (the PrIDE Exercise Program, the Strong Spirit Strong Self health self-efficacy assessment tool, and Keep Your Heart Strong educational materials) and one newly developed tool (Success Plan). Both the Strong Spirit Strong Self self-efficacy questionnaire and the Success Plan tool utilize clinical yarning as the delivery method. Clinical yarning is a culturally safe communication approach frequently used in health care, facilitating shared discussion between the research assistant or accredited exercise physiologist and the participant [36,38]. It progresses through interconnected phases: social yarning establishes rapport and trust, diagnostic yarning explores the topic through story-sharing, and management yarning facilitates collaborative planning [36,38]. This structured yet flexible approach is open-ended, story-based, and participant-led, creating space for self-expression and shared understanding. Clinical yarning is culturally centered; shows respect towards Indigenous Australians, privileging Indigenous ways of knowing and communicating; and allows these tools to function as collaborative conversations rather than formal assessments [36,38]. Each tool followed this cycle, with cultural adaptations documented using MADI [39] and all tools reviewed by the CUP for cultural safety and appropriateness. Tool development followed an iterative co-design, assessment, and review cycle, summarized in Figure 2.
2.6. PrIDE Exercise Program
The cultural adaptation of the Beat It program was led by an Indigenous accredited exercise physiologist (AEP) from the research team (author BBD), a Bundjalung/Gumbaynggirr (Mid-North Coast region of New South Wales) Indigenous Australian man, with Beat It Program content expertise. The cultural adaptation was systematically documented using the Model for Adaptation Design and Impact (MADI) framework [39], with BBD leading the adaptation process collaboratively with the CHRI co-design team. The completed MADI outlines the specific adaptations made across key program areas including AEP preparation, participant resources, assessment procedures, and program delivery methods. The PrIDE Exercise Program incorporates a combination of aerobic, resistance, balance, and flexibility training, with individualized progression prescribed and supervised by accredited exercise physiologists. Exercise prescription is consistent with contemporary clinical guidelines for adults with T2DM and national physical activity recommendations, including combined aerobic and resistance training and a reduction in sedentary behavior [9,40,41,42].
2.7. Strong Spirit Strong Self Health Self-Efficacy Assessment Tool
The 10-item New General Self-Efficacy (NGSE) scale [43] was culturally adapted for assessing health self-efficacy with Indigenous Australians managing T2DM. The adaptation was led by author KC, a Noongar researcher from the Whadjuk clan, in collaboration with author CT, a Whadjuk Noongar Elder. Yarning sessions were conducted with CT, a second Noongar Elder with deep community and cultural knowledge, and an Aboriginal health and community worker with frontline perspectives and expertise from the Champion Centre on Whadjuk/Noongar Country (Perth, WA, Australia).
Multiple yarning sessions allowed for reflection, clarification, and shared understanding to ensure the adapted tool was culturally grounded, practical, and aligned with community expectations and experiences. The adapted tool was renamed “Strong Spirit Strong Self” to reflect its cultural grounding and was subsequently reviewed by the CUP for cultural safety and appropriateness.
2.8. Keep Your Heart Strong Educational Materials
Heart health educational materials were culturally adapted from the National Heart Foundation’s “10 Steps to Protect Your Heart” resource. The National Heart Foundation is the peak body for heart disease prevention and support in Australia, working to improve heart health outcomes for all Australians through research, advocacy, public awareness campaigns, and accessible resources [44]. The Heart Foundation’s “10 Steps to Protect Your Heart” resource is available on their dedicated Indigenous Australians health webpage [45] (Figure 3 shows the original resource).
The adaptation was led by an Indigenous team member and AEP (author BBD), who reviewed the resource and identified opportunities to enhance accessibility by replacing clinical terminology with everyday language and streamlining content. Working collaboratively with the CHRI co-design team, culturally adapted educational materials were created in two formats: a brochure featuring Markeeta’s (Wemba Wemba) artwork “Paths You Take,” and an animation with voice-over narration by BBD.
2.9. The Success Plan
The Success Plan is a newly developed tool designed to facilitate exercise program selection and goal setting in a culturally safe manner. The tool was led and co-developed by an Indigenous AEP (author BBD) in collaboration with the co-design research team. The Success Plan comprises five sequential questions that guide participants through values identification, goal setting, preference assessment, strategy planning, and program selection. The tool reframes traditional pre-exercise questionnaires using simple, strengths-based language that considers the Indigenous Australian context while maintaining important clinical information. The tool was reviewed by the CUP, with feedback leading to refinements in language, tone, and framing, and the inclusion of Elders as role models within the tool to ensure relevance across age groups and cultural contexts.
2.10. Assessment of Cultural Appropriateness
All four tools were assessed using the Aboriginal and Torres Strait Islander Quality Appraisal Tool (CREATE) [46] to ensure that they met best practice standards for Indigenous health research. The 14-item CREATE tool assesses domains including community need and consultation, Indigenous leadership and governance, cultural protocols, intellectual property, research paradigm, a strengths-based approach, capacity strengthening, and reciprocal learning opportunities.
2.11. Behavior Change Mechanism Analysis
All four tools were analyzed using the COM-B model (Capability, Opportunity, Motivation—Behavior) [47,48,49] to map how tool features align with determinants of behavior change. The COM-B model, a component of the Behavior Change Wheel, posits that behavior occurs when individuals have the capability (physical and psychological), opportunity (social and physical), and motivation (reflective and automatic) to perform it [49]. Each tool component was mapped to the six COM-B domains to assess comprehensive coverage of behavior change mechanisms and to examine how cultural adaptation reconceptualizes these mechanisms in Indigenous contexts. The COM-B analysis presented below reflects an interpretive mapping of behavior change mechanisms as operationalized through co-design in PrIDE, rather than a claim of universal applicability or demonstrated effectiveness.
Figure 4 summarizes the engagement, adaptation, quality appraisal, and behavior change analysis processes applied to each tool.
2.12. Data Management
Tool development processes were documented following principles of Indigenous data sovereignty, with community ownership of knowledge ensuring research outcomes were meaningful and culturally relevant to Indigenous Australian communities and researchers [37].
This paper reports the co-design and development phase only; evaluation of effectiveness, acceptability, and psychometric properties will be undertaken and reported following the implementation of the PrIDE study.
3. Results
3.1. Overview of Tools Developed
Four tools were successfully developed through the co-design process: three culturally adapted tools (the PrIDE Exercise Program, the Strong Spirit Strong Self health self-efficacy assessment tool, and Keep Your Heart Strong educational materials), and one newly developed tool (Success Plan).
3.2. Cultural Appropriateness Assessment
All tools met requirements across key domains of the Aboriginal and Torres Strait Islander Quality Appraisal Tool. Items related to intellectual property agreements and translation to policy/practice and community benefit were marked as “not applicable” as these tools are in the design phase and have not yet been implemented in community settings. Full results are presented in Table 1.
3.3. PrIDE Exercise Program Adaptations
The cultural adaptation of the Beat It program preserved core evidence-based mechanisms while enhancing cultural safety, participant engagement, and program accessibility. Adaptations were systematically documented across nine key areas using the MADI framework. The full documentation is presented in Table 2.
3.4. Strong Spirit Strong Self Health Self-Efficacy Tool
The cultural adaptation of the NGSE scale preserved core self-efficacy theory while integrating cultural enhancements that reflect Indigenous worldviews and ways of being. The adaptation maintained the 10-item structure to allow for equivalent comprehensiveness and direct comparison with the original tool. Response-scale language was adapted from formal academic terms to everyday language to increase clarity and accessibility. The administration method was adapted from self-administered questionnaire to conversational administration by the research assistant using clinical yarning [36,38].
Content validity was established through yarning with Elders and the community in Nyoongar Country (Perth, WA, Australia). Face validity was established through the co-design process and CUP review. Psychometric validation will be conducted through the PrIDE study, assessing internal consistency reliability, sensitivity to change, convergent validity, known-groups validity, and exploratory factor analysis to examine dimensionality. The full MADI documentation is presented in Table 3.
3.5. Keep Your Heart Strong Educational Materials
Heart health educational materials were culturally adapted from the National Heart Foundation’s evidence-based “10 Steps to Protect Your Heart” resource (Figure 3). The adaptation enhanced accessibility by streamlining ten steps to three essential messages delivered through strengths-based framing: (1) make heart-healthy choices, (2) yarn with your clinic mob, and (3) cut back on smokes and alcohol. For the first two messages, framing statements are directly supported by specific, actionable examples provided within the materials to ensure clarity and practical relevance. The adaptation replaced clinical terminology (e.g., “manage your cholesterol”) with everyday language and actionable guidance that resonates with community ways of communicating about health.
The Keep Your Heart Strong brochure and animation feature Markeeta’s artwork “Paths You Take” and include voice-over narration by BBD. CUP feedback was highly positive, with members highlighting the culturally appropriate color palette, integration of Indigenous artwork and visual elements, simplicity of messaging, and use of accessible language. The brochure (Figure 5) will be distributed at program registration and the animation shared on the study’s social media platform.
3.6. The Success Plan
The Success Plan integrates multiple theoretical frameworks to support culturally safe, participant-centered decision-making. The tool comprises five sequential questions delivered through clinical yarning. The theoretical rationale for each tool component is presented in Table 4.
3.7. Behavior Change Mechanisms: COM-B Analysis
COM-B analysis identified how tool features align with behavior change domains. The PrIDE Exercise Program maps to all six components through its comprehensive adaptations. Strong Spirit Strong Self corresponds to psychological capability and reflective motivation through culturally appropriate assessment that reconceptualizes the capability to include collective, cultural, and spiritual dimensions. Keep Your Heart Strong educational materials align with psychological capability through accessible health information, social and physical opportunity through multiple distribution channels and social connection framing, and both reflective and automatic motivation through strengths-based messaging and culturally resonant visual elements. The Success Plan integrates features that map across all components through a process that corresponds to psychological capability for planning, opportunity assessment through constraint identification and strategy planning, and reflective and automatic motivation. The complete COM-B mapping for all four PrIDE tools is presented in Supplementary Table S1.
3.8. CUP Feedback and Iterative Refinement
The CUP provided substantive feedback across all four tools, resulting in 1–3 rounds of revision for each tool. Primary improvements included adjustments to language, tone, and framing to ensure accessibility, cultural appropriateness, and respectful communication across age groups and literacy levels. For example, a CUP review of the Success Plan led to the addition of “Be a role-model for my community” as a program goal option; the removal of “I will” prefixes from barrier-planning options, as CUP members identified this phrasing as pressuring rather than supportive; and the substitution of “family” with “mob” to better reflect community language and collective responsibility. Elder perspectives were integrated throughout tools to reflect intergenerational knowledge and support structures. The CUP provided guidance on integration of licensed artwork throughout materials and refinement of delivery methods to ensure cultural safety and participant comfort.
4. Discussion
4.1. Principal Findings
This study developed four tools for the Preventing Indigenous CVD and Diabetes through Exercise (PrIDE) study [33] using co-design following best practice frameworks: three culturally adapted tools (the PrIDE Exercise Program from Beat It, the Strong Spirit Strong Self from NGSE, the Keep Your Heart Strong from Heart Foundation resources) and one newly developed tool (the Success Plan). All tools met Indigenous health research quality standards via the Aboriginal and Torres Strait Islander Quality Appraisal Tool [46], were governed through Indigenous leadership structures (CAG and CUP), and utilized Indigenous research methodologies, primarily yarning [36].
Indigenous leadership throughout the development process ensured that cultural knowledges and Indigenous epistemologies shaped tool design from inception rather than through consultation. This approach aligns with emerging diabetes co-design initiatives in Australia that privilege Indigenous governance and lived experience [30,31], and extends them by embedding structured adaptation and theory mapping within an exercise intervention context.
MADI documentation provides transparent, prospective recording of adaptation decisions while preserving core evidence-based mechanisms and enhancing cultural safety, addressing a gap where cultural adaptations are often reported superficially, limiting replication. COM-B analysis revealed how co-design reconceptualized the operationalization of behavior change mechanisms: psychological capability was conceptualized to include collective, cultural, and spiritual dimensions; social opportunity was understood as requiring deliberate creation through Indigenous leadership and trusted relationships; and motivation was operationalized holistically and relationally. The evaluation of effectiveness, acceptability, and scalability will be reported following PrIDE implementation.
4.2. Comparison with Prior Work
The published evidence on culturally adapted exercise interventions for Indigenous Australians with T2DM remains limited [15]. Previous reviews have noted not only the paucity of Indigenous exercise interventions, but also the limited reporting of development processes and Indigenous governance, constraining reproducibility and translation to other communities [18]. International evidence is sparse; one supervised community-based group exercise intervention with Indigenous Polynesian adults demonstrated improvements in quality of life and cardiometabolic outcomes [16,17]. However, this evidence focused primarily on outcome evaluation and provided limited detail on program development processes, governance structures, or systematic cultural adaptation approaches, constraining reproducibility and transferability to other Indigenous populations. PrIDE extends this evidence base by pairing an established, evidence-based exercise program with Indigenous governance and explicitly documenting cultural adaptation using structured frameworks, responding to calls for greater transparency, Indigenous leadership, and methodological rigor in co-designed health interventions [34]. While specific cultural adaptations are necessarily locally determined, the process framework—combining Indigenous-governed co-design (CHRI model), structured adaptation documentation (MADI), quality appraisal (CREATE), and theory mapping (COM-B)—is transferable to exercise intervention development with Indigenous peoples in other high-income colonized countries. Critically, this study positions cultural adaptation processes and theory-informed design decisions as primary objects of inquiry rather than implicit background activity.
4.3. Tool-Specific Contributions
Strong Spirit Strong Self addresses a recognized gap in Indigenous health research regarding culturally appropriate measurement. Western self-efficacy instruments privilege individualistic constructs that may be misaligned with Indigenous worldviews [7,66]. While Bandura [67] acknowledged that efficacy beliefs operate through both personal and collective agency, standard self-efficacy questionnaires typically operationalize the construct within individualistic frameworks. Yet self-efficacy—belief in one’s capability to take action—is strengthened, supported, and sustained through relationships and social context for all people [68]. For Indigenous Australians, this relational foundation is particularly salient, with family, Elders, community, and culture recognized as essential sources of strength that lift and sustain the individual [7]. Strong Spirit Strong Self preserves the theoretical core of self-efficacy while reconceptualizing its sources to include family, Elders, culture, spirit, and community, reflecting relational and collective dimensions of capability.
The Success Plan demonstrates how traditional intake processes can be reframed through strengths-based language and clinical yarning for culturally safe decision-making while maintaining clinical utility. By positioning barrier navigation as proactive coping drawing on collective resources, it integrates behavioral theory with Indigenous relational values.
Keep Your Heart Strong illustrates that even resources targeting Indigenous audiences benefit from Indigenous-led adaptation. Indigenous review identified barriers in clinical language, framing, and information density. Streamlining content and reframing through strengths-based language enhanced the accessibility while maintaining evidence-based content.
4.4. Co-Design and Behavior Change Mechanisms
COM-B analysis revealed how co-design reshaped the operationalization and interpretation of behavior change mechanisms. Psychological capability was conceptualized to include collective efficacy, cultural knowledge, and spiritual strength, positioning family, Elders, and community as intrinsic capability resources rather than external supports—challenging individualistic assumptions in Western self-efficacy models [7,66].
Social opportunity was conceptualized as a prerequisite for engagement rather than optional enhancement. Historical trauma, ongoing racism, and institutional mistrust necessitate deliberate creation of social opportunity through Indigenous leadership, culturally congruent communication, and trusted intermediaries [34]. Analysis revealed that PrIDE incorporated features mapping to social opportunity through governance structures, recruitment strategies, and delivery approaches.
Motivation was conceptualized holistically and relationally, with goals anchored in family and community responsibilities rather than solely individual outcomes, extending autonomy-focused theories to include culturally congruent autonomy grounded in interdependence [51]. COM-B mapping identified that Keep Your Heart Strong’s integration of Indigenous artwork, voice-over, and relational framing (“yarn with your clinic mob”) aligns with automatic motivation through cultural resonance while streamlined content corresponds to psychological capability.
These findings demonstrate how co-design informs application of established behavior change frameworks in culturally congruent ways, advancing the understanding of theory operationalization in Indigenous health contexts.
4.5. Strengths and Limitations
A key strength of this work is the use of structured co-design and adaptation frameworks alongside Indigenous governance and research methodologies. The integration of the CHRI model, MADI framework, and Aboriginal and Torres Strait Islander Quality Appraisal Tool provided methodological rigor while centering Indigenous leadership and accountability.
Several limitations should be noted. Psychometric validation of Strong Spirit Strong Self is pending and will be conducted during PrIDE implementation. Tool effectiveness and acceptability have not yet been evaluated and will be reported separately. Tool development occurred with specific communities and may not generalize across the diversity of Indigenous Australian nations, languages, and cultural practices; further adaptation may be required in new contexts.
4.6. Implications for Practice and Research
Health services can use PrIDE as a model for implementing exercise interventions for Indigenous Australians with T2DM, with MADI documentation providing detailed adaptation guidance. Strong Spirit Strong Self provides a culturally appropriate self-efficacy instrument for Indigenous populations; researchers should prioritize culturally adapted outcome measures over standard Western instruments. The Success Plan demonstrates clinical yarning integration into routine practice for culturally safe assessment and shared decision-making, applicable beyond exercise interventions. Keep Your Heart Strong demonstrates value in review of existing resources to enhance accessibility. Sustainability has been considered within the design of the PrIDE tools through alignment with routine accredited exercise physiologist practice and existing service workflows, supporting ongoing use beyond the research phase.
For researchers, this body of work demonstrates feasibility of systematic cultural adaptation using established frameworks. The CHRI model and MADI framework combination provides methodological rigor while centering Indigenous knowledge, leadership, and community control. Indigenous-governed work ensures cultural authenticity unachievable through consultation-based approaches. Future research should prioritize Indigenous leadership in systematic adaptations for chronic disease prevention and management interventions.
Implementation in remote and rural communities will provide evidence on effectiveness, acceptability, and scalability. Evaluation will examine improvements in cardiovascular risk factors, physical fitness, and self-efficacy, and whether improvements are sustained. Process evaluation will identify implementation facilitators and barriers, informing scale-up planning and policy.
5. Conclusions
This research demonstrates systematic adaptation and development of tools for Indigenous health through Indigenous-governed co-design processes honoring Indigenous knowledge systems while maintaining evidence-based mechanisms. The three culturally adapted tools and newly developed Success Plan address evidence gaps in interventions with Indigenous Australians. MADI documentation and theoretical rationale provide a model for future cultural adaptation and development of research. PrIDE study implementation will provide evidence on effectiveness, acceptability, and scalability to inform practice, policy, and research aimed at improving health equity with Indigenous Australians.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Brown A. Carrington M.J. Mc Grady M. Lee G. Zeitz C. Krum H. Rowley K. Stewart S. Cardiometabolic Risk and Disease in Indigenous Australians: The Heart of the Heart Study Int. J. Cardiol.201417137738310.1016/j.ijcard.2013.12.02624388543 · doi ↗ · pubmed ↗
- 2Australian Institute of Health and Welfare Aboriginal and Torres Strait Islander Health Performance Framework—Summary Report Leading Causes of Mortality Australian Institute of Health and Welfare Canberra, Australia 2024
- 3Australian Institute of Health and Welfare Australian Burden of Disease Study: Impact and Causes of Illness and Death in Aboriginal and Torres Strait Islander People 2018 Australian Burden of Disease Study Series No. 26Australian Institute of Health and Welfare Canberra, Australia 2022
- 4Australian Institute of Health and Welfare Rural and Remote Health Available online: https://www.aihw.gov.au/reports/rural-remote-australians/rural-and-remote-health(accessed on 20 May 2025)
- 5Brown A. Kritharides L. Overcoming Cardiovascular Disease in Indigenous Australians Med. J. Aust.2017206101210.5694/mja 16.0069328076740 · doi ↗ · pubmed ↗
- 6Bainbridge R. Mc Calman J. Clifford A. Tsey K. Cultural Competency in the Delivery of Health Services for Indigenous People Australian Institute of Family Studies Australian Institute of Health and Welfare Canberra, Australia 2015978-1-74249-766-2
- 7Dudgeon P. Harris J. Newnham K. Brideson T. Cranney J. Darlaston-Jones D. Hammond S.W. Herbert H. Homewood J. Page S. Working Together: Aboriginal and Torres Strait Islander Mental Health and Wellbeing Principles and Practice 2nd ed. Dudgeon P. Milroy H. Walker R. Kulunga Research Network West Perth, WA, USA 2014978-0-9579494-4-7
- 8De Zilva S. Walker T. Palermo C. Brimblecombe J. Culturally Safe Health Care Practice for Indigenous Peoples in Australia: A Systematic Meta-Ethnographic Review J. Health Serv. Res. Policy 202227748410.1177/1355819621104183534875923 · doi ↗ · pubmed ↗