Association of Arterial Velocity Pulse Index and Arterial Pressure–Volume Index with Central Arterial Stiffness and Cardiac Function in the Japanese Population
Hiroto Hommo, Takuya Sugawara, Hikaru Ueno, Honoka Kawashima, Kotaro Uchida, Shintaro Minegishi, Lin Chen, Rie Sasaki-Nakashima, Tabito Kino, Kentaro Arakawa, Michiko Sugiyama, Noriyuki Kawaura, Koichi Tamura, Kiyoshi Hibi, Tomoaki Ishigami

TL;DR
This study finds that high Arterial Velocity Pulse Index and Arterial Pressure–Volume Index are linked to increased arterial stiffness and heart function issues in Japanese patients.
Contribution
The study identifies hemodynamic and echocardiographic characteristics associated with elevated AVI and API in a Japanese population.
Findings
High AVI/API groups had higher brachial and central systolic BP and pulse pressure.
High-risk groups showed greater wave amplitudes and prolonged ejection duration.
Impaired diastolic function was observed without reduced LVEF in high AVI/API groups.
Abstract
Background: The Arterial Velocity Pulse Index (AVI) and Arterial Pressure–Volume Index (API) are novel non-invasive indices of arterial stiffness derived from cuff-oscillometric measurements. Previous studies have shown that elevated AVI and API are associated with the severity of coronary artery disease and the ability to predict future cardiovascular events. However, the hemodynamic and echocardiographic characteristics of patients with concomitantly high AVI and API remain unclear. Methods: We retrospectively analyzed 112 consecutive cardiovascular outpatients (mean age 69.1 ± 12.2 years, 64.3% male) seen between January and April 2019 at Yokohama City University Hospital. The AVI and API were measured using a multifunctional sphygmomanometer (PASESA AVE1500, Shisei Datum, Japan) and averaged over a maximum of three measurements. Patients were classified into four groups according to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
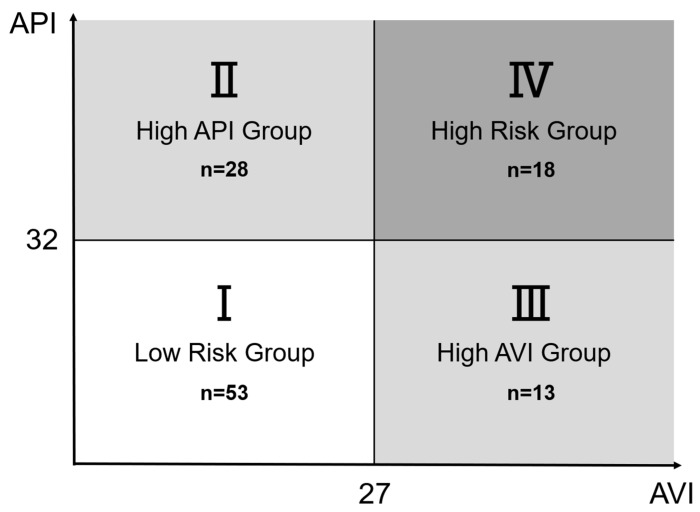 Figure 1
Figure 1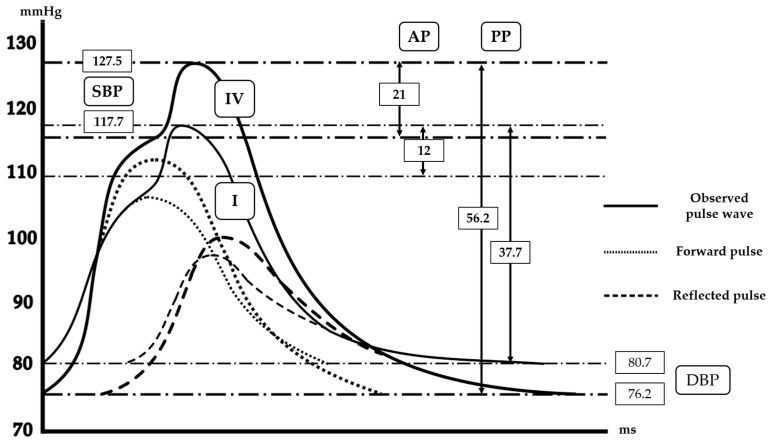 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Health and Disease Prevention · Cardiovascular Disease and Adiposity · Blood Pressure and Hypertension Studies
1. Introduction
Arterial stiffness is a recognized marker of vascular aging and an independent predictor of cardiovascular morbidity and mortality [1,2,3,4]. The development of reliable, non-invasive, and easily obtainable arterial stiffness indices is therefore of significant clinical interest.
In recent years, oscillometric techniques have enabled the assessment of arterial stiffness using simple cuff-based blood pressure measurements [5,6]. Using such an approach, the Arterial Velocity Pulse Index (AVI) and the Arterial Pressure–Volume Index (API) can be obtained with the PASESA AVE1500 system (Shisei Datum, Tokyo, Japan) [5]. The AVI reflects the characteristics of central arterial stiffness by analyzing brachial pulse waveforms recorded during suprasystolic cuff inflation, whereas the API provides an estimate of peripheral arterial compliance based on the pressure–volume relationship observed during cuff deflation.
We, along with other researchers, have previously demonstrated that both the AVI and API are correlated with the severity and complexity of coronary artery disease, and that threshold values of 27 (AVI) and 32 (API) predict cardiovascular events [1,7,8,9]. However, the cardiovascular phenotype of patients with simultaneously high AVI and API—representing both central and peripheral stiffness—remains insufficiently characterized. To date, no study has comprehensively evaluated central pulse wave characteristics and echocardiographic findings across the four AVI/API-defined categories. Therefore, whether concomitantly elevated AVI and API reflect an adverse cardiovascular phenotype remains unknown.
This study aimed to classify patients into four groups according to AVI and API cutoff values and compare central pulse wave parameters and echocardiographic findings between these groups. We hypothesized that patients with concomitantly elevated AVI and API would exhibit more adverse hemodynamic profiles and evidence of subclinical myocardial dysfunction.
2. Materials and Methods
2.1. Study Population
We retrospectively reviewed 112 consecutive outpatients who attended the Department of Cardiology at Yokohama City University Hospital between January and April 2019. The inclusion criteria were age ≥ 20 years and the availability of both AVI and API measurements, along with central pulse wave analysis and echocardiographic data. Patients with arrhythmias that interfered with the pulse wave measurements, severe valvular disease, or acute cardiovascular events within three months were excluded from this study. Because patient inclusion required successful assessment with both PASESA and SphygmoCor XCEL, the study population represents a selected cohort, and the analysis was exploratory in nature.
2.2. Measurement of AVI and API
The oscillometric assessment of arterial stiffness was performed using the PASESA AVE1500 system (Shisei-Datum, Tokyo, Japan). This device acquires brachial pulse waveforms during suprasystolic cuff inflation to derive the Arterial Velocity Pulse Index (AVI) and analyzes the pressure–volume relationship obtained during cuff deflation to calculate the Arterial Pressure–Volume Index (API). Measurements were obtained in the seated position after at least 5 min of rest in the outpatient clinic. The average of a maximum of three measurements was used for the analysis [7,8].
2.3. Group Classification
Patients were classified into four groups:
Group I: Low AVI (<27)/Low API (<32).
Group II: Low AVI (<27)/High API (≥32).
Group III: High AVI (≥27)/Low API (<32).
Group IV: High AVI (≥27)/High API (≥32).
2.4. Central Pulse Wave Analysis
Central hemodynamic parameters, including central systolic and diastolic BP, pulse pressure, augmentation pressure, augmentation index (AIx), ejection duration, aortic T2, forward and reflected wave amplitudes, and the Buckberg subendocardial viability ratio (SEVR), were assessed using SphygmoCor XCEL (AtCor Medical, Sydney, Australia). The average of a maximum of three measurements was used for the analysis.
2.5. Echocardiography
Standard transthoracic echocardiography was performed in accordance with the American Society of Echocardiography guidelines [10]. Left ventricular dimensions, ejection fraction (EF), diastolic filling parameters (E/A ratio, septal e′, and E/e′), and left atrial diameter were measured. All echocardiographic measurements were performed by experienced, certified cardiac sonographers under the supervision of cardiologists, as part of routine clinical practice at a university hospital, in accordance with the established guidelines. Although formal intra- and inter-observer variability analyses were not conducted for research purposes in this retrospective study, the measurements were obtained using standardized protocols routinely applied in daily clinical care.
2.6. Statistical Analysis
Continuous variables are presented as mean ± standard deviation (SD) or median [interquartile range], and categorical variables are presented as number and percentage. Intergroup comparisons of continuous variables were made using Welch’s one-way analysis of variance (ANOVA) followed by Bonferroni’s multiple comparison test, or the Kruskal–Wallis test with the Steel–Dwass test. Omnibus tests and pairwise comparisons of categorical variables were performed using the chi-square test or Fisher’s exact test. Pairwise comparisons were corrected by Bonferroni correction. A two-tailed p-value < 0.05 was considered statistically significant. All statistical analyses were performed with EZR (version 1.68; Jichi Medical University, Tochigi, Japan), which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria) [11].
3. Results
A total of 112 patients were analyzed and stratified into four groups according to the AVI/API cutoff values (Group I, n = 53; Group II, n = 28; Group III, n = 13; Group IV, n = 18, Figure 1). The baseline characteristics are shown in Table 1. The patients in Groups II–IV tended to be older than those in Group I, with the highest mean age observed in Group IV. The prevalence of diabetes mellitus increased progressively from Group I to Group IV, and Group II showed the highest proportion of antidiabetic use and median HbA1c value. The use of hypolipidemic agents also showed a stepwise increase with the elevation of AVI/API values. Other comorbidities and medication use were generally comparable among the groups.
The subjects (n = 112) were classified into four groups according to their API and AVI values. Group I included subjects with standard API (<32) and AVI (<27). Group II included those with elevated API only (API ≥ 32 and AVI < 27). Group III included those with elevated AVI only (API < 32 and AVI ≥ 27). Group IV included those with both elevated API and AVI (API ≥ 32 and AVI ≥ 27). In total, 53 subjects were assigned to Group I, 28 to Group II, 13 to Group III, and 18 to Group IV.
Hemodynamic parameters
Hemodynamic data are summarized in Table 2 and Figure 2. Brachial systolic blood pressure showed a gradual increase across the groups, with Group IV demonstrating the highest values (139.2 [132.8–149] mmHg), significantly higher than those in Group I (128 [120–136.7] mmHg, p = 0.0011). A similar stepwise pattern was observed in terms of central systolic blood pressure and central pulse pressure, both of which rose progressively from Group I through to Group IV.
Indices reflecting wave reflection also demonstrated clear gradients. P1 height, forward pulse height, and reflected pulse height increased consistently across the four groups, with marked differences between Group IV and Group I (all p < 0.001). Augmentation pressure and ejection duration similarly exhibited progressive elevations from lower to higher AVI/API categories. Although the augmentation index and reflection magnitude did not differ significantly between the groups, those of Group IV were elevated compared with those of the other groups.
Echocardiographic findings
The echocardiographic data are presented in Table 3. Left ventricular size, left atrial diameter, and cardiac output were generally comparable among the four groups. The ejection fraction of Group II was significantly higher than that of Groups I and IV, but it was not significant between Group I and Group IV. However, the indices of diastolic function demonstrated stepwise deterioration in association with higher AVI/API values. Specifically, the e′ velocity decreased gradually from Group I (6.7 [5.2–8] cm/s) to Group IV (5 [4.1–5.8] cm/s) (p = 0.035 for Group IV vs. Group I), while E/e′ increased in a parallel manner (13.2 [11.1–15.1] to 9.7 [7.9–11.3], p = 0.026 for Group IV vs. Group I). These findings suggest that progressive vascular stiffening, as captured by the AVI/API, is accompanied by worsening left ventricular relaxation and elevated filling pressures.
4. Discussion
In this exploratory, retrospective cross-sectional study, we evaluated the prognostic significance of arterial stiffness indices, the Arterial Velocity Pulse Index (AVI), and the Arterial Pressure–Volume Index (API). Our principal findings were as follows: Firstly, when stratifying patients into four groups according to AVI/API cutoff values, which we proposed previously, the high-risk group (Group IV) demonstrated significant differences in several hemodynamic parameters compared with the low-risk group (Group I). In particular, central blood pressure (central SBP, augmentation pressure), indices of pulse wave reflection (P1 height, reflected pulse height, forward pulse height), and ejection duration were markedly elevated in Group IV. Secondly, the echocardiographic assessment revealed evidence of impaired diastolic function, including reduced e′ and increased E/e′, in the high-AVI/API group. These results suggest that patients with elevated AVI/API not only exhibit increased arterial stiffness but also subclinical left ventricular (LV) diastolic dysfunction.
From a clinical perspective, these findings are notable. The AVI and API are conventionally regarded as surrogate indices of arterial stiffness [7,8,9,12], yet our results imply that their significance extends beyond vascular mechanics. The observed associations with echocardiographic parameters indicate that the AVI/API may reflect LV filling pressures and diastolic function, thereby serving as markers that bridge vascular and cardiac dysfunction. The simultaneous elevation of forward and reflected wave amplitudes in Group IV suggests increased impedance mismatch and accelerated wave return, which are known to contribute to higher central systolic load and impaired relaxation. Given that AVI/API assessment is simple and non-invasive, these indices may offer a practical tool for risk stratification in daily clinical practice, particularly for identifying individuals at risk of adverse cardiovascular outcomes.
The present findings suggest that concomitantly elevated AVI and API values reflect a pathophysiological state characterized by increased arterial stiffness at both central and peripheral levels, which may adversely affect left ventricular diastolic function. Elevated AVI has been shown to represent increased central arterial stiffness and enhanced wave reflection, leading to higher central systolic pressure and augmented late systolic load on the left ventricle [13,14]. This increase in pulsatile afterload may impair active myocardial relaxation and contribute to diastolic dysfunction, even in the absence of overt systolic impairment [15,16,17].
In parallel, elevated API reflects reduced peripheral arterial compliance, which may further exacerbate abnormalities in ventricular–vascular coupling. Increased peripheral stiffness can alter the timing and magnitude of reflected pressure waves, reduce diastolic pressure augmentation, and impair coronary perfusion during diastole [18,19]. Such hemodynamic alterations may be particularly relevant to subclinical myocardial dysfunction, as reflected by impaired diastolic parameters such as reduced e′ velocity and elevated E/e′ ratio.
Therefore, the combined elevation of the AVI and API may represent a hemodynamically unfavorable phenotype in which both central pulsatile load and peripheral arterial compliance are compromised [20,21]. This condition may accelerate age-related ventricular–vascular stiffening and promote the development of diastolic dysfunction, a key pathophysiological feature of heart failure with preserved ejection fraction (HFpEF). Our findings support the concept that simple cuff-based arterial stiffness indices may capture clinically meaningful vascular–cardiac interactions and help identify individuals at risk of early myocardial dysfunction before the onset of overt heart failure.
Our findings are consistent with prior studies that have validated the AVI and API in comparison with carotid–femoral pulse wave velocity (ba-PWV) [3,22], one of the standard measures of arterial stiffness. Several reports have demonstrated that the AVI and API correlate with central blood pressure and augmentation indices, thereby supporting their validity as vascular biomarkers [7,8,9,23]. However, the present study extends existing knowledge by demonstrating a significant association between the AVI/API and echocardiographic indices such as e′ and E/e′. This novel observation suggests that there is a potential mechanistic link between increased arterial stiffness and LV diastolic impairment, warranting further exploration in future investigations. Future studies incorporating complementary diagnostic modalities, such as myocardial strain imaging, circulating biomarkers of myocardial stress, or cardiac magnetic resonance imaging, may further substantiate the mechanistic link between arterial stiffness and subclinical myocardial dysfunction.
This study has several limitations that should be acknowledged. Firstly, this was a single-center, retrospective study with a relatively small sample size and a short enrollment period, which may limit the generalizability of the findings. Secondly, patient inclusion was restricted to those who underwent both oscillometric arterial stiffness assessment (AVI/API using PASESA) and central hemodynamic evaluation using SphygmoCor XCEL, resulting in a selected study population and an exploratory study design. Thirdly, the number of clinical events was limited, precluding definitive conclusions regarding prognostic outcomes. In addition, although the sex distribution was documented, the limited sample size did not allow for robust sex-specific analyses. Because formal multivariable regression analyses were not performed, we cannot exclude the possibility that age-related differences may have contributed to the observed intergroup differences, particularly between the low-risk and high-risk AVI/API categories. Future multicenter prospective cohort studies and interventional trials with larger populations are warranted to validate the prognostic significance of AVI/API cutoff values and clarify their role in cardiovascular risk stratification.
5. Conclusions
In conclusion, the present study demonstrates that concomitantly elevated AVI and API values are associated with adverse central hemodynamics and impaired left ventricular diastolic function in a Japanese outpatient population. These findings suggest that the combined assessment of central and peripheral arterial stiffness using simple cuff-based oscillometric indices may provide clinically meaningful insights into subclinical myocardial dysfunction. Given their non-invasive nature and ease of use in routine clinical practice, the AVI and API may serve as practical tools for early cardiovascular risk stratification, particularly in patients at risk of diastolic dysfunction and heart failure with preserved ejection fraction. Further large-scale, prospective studies are warranted to confirm these observations and determine whether targeted interventions based on AVI/API profiles can improve clinical outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zhou J. Wang Y. Feng Y. Chen X. Zhang Q. New indices of arterial stiffness correlate with disease severity and mid-term prognosis in acute decompensated heart failure Intern. Emerg. Med.20211666166810.1007/s 11739-020-02486-x 32888111 · doi ↗ · pubmed ↗
- 2Miyoshi T. Ito H. Shirai K. Horinaka S. Higaki J. Yamamura S. Saiki A. Takahashi M. Masaki M. Okura T. Predictive Value of the Cardio-Ankle Vascular Index for Cardiovascular Events in Patients at Cardiovascular Risk J. Am. Heart Assoc.202110 e 02010310.1161/JAHA.120.02010334369198 PMC 8475039 · doi ↗ · pubmed ↗
- 3Tomiyama H. Shiina K. State of the Art Review: Brachial-Ankle PWVJ. Atheroscler. Thromb.20202762163610.5551/jat.RV 1704132448827 PMC 7406407 · doi ↗ · pubmed ↗
- 4Alanis G.A. Boutouyrie P. Abouqateb M. Bruno R.M. Climie R.E. van Sloten T. Danchin N. Pannier B. Laurent S. Jouven X. Vascular ageing manifestations and hypertension in the community Am. J. Prev. Cardiol.20252110091810.1016/j.ajpc.2024.10091839807445 PMC 11728902 · doi ↗ · pubmed ↗
- 5Komine H. Asai Y. Yokoi T. Yoshizawa M. Non-invasive assessment of arterial stiffness using oscillometric blood pressure measurement Biomed. Eng. Online 201211610.1186/1475-925X-11-622325084 PMC 3359259 · doi ↗ · pubmed ↗
- 6Liang F. Takagi S. Himeno R. Liu H. A computational model of the cardiovascular system coupled with an upper-arm oscillometric cuff and its application to studying the suprasystolic cuff oscillation wave, concerning its value in assessing arterial stiffness Comput. Methods Biomech. Biomed. Eng.20131614115710.1080/10255842.2011.61030521916678 · doi ↗ · pubmed ↗
- 7Sasaki-Nakashima R. Kino T. Chen L. Doi H. Minegishi S. Abe K. Sugano T. Taguri M. Ishigami T. Successful prediction of cardiovascular risk by new non-invasive vascular indexes using suprasystolic cuff oscillometric waveform analysis J. Cardiol.201769303710.1016/j.jjcc.2016.06.00427590415 · doi ↗ · pubmed ↗
- 8Doi H. Ishigami T. Nakashima-Sasaki R. Kino T. Chen L. Arakawa K. Teranaka S. Minegishi S. Abe K. Ishikawa T. New non-invasive indexes of arterial stiffness are significantly correlated with severity and complexity of coronary atherosclerosis Clin. Exp. Hypertens.20184118719310.1080/10641963.2018.146507229737880 · doi ↗ · pubmed ↗