Effects of Aquatic Exercise on Individuals with Hypertension: A Systematic Review
Hugo Rodríguez-Otero, Pablo Hernandez-Lucas, Isabel Escobio-Prieto, Eva Lantarón-Caeiro

TL;DR
This paper reviews how water-based exercise affects blood pressure in people with hypertension, finding potential benefits but noting study limitations.
Contribution
The study provides an updated systematic review on aquatic exercise effects for hypertension, highlighting methodological limitations.
Findings
Aquatic exercise is associated with blood pressure reductions in hypertensive individuals.
Common interventions include water walking and strength exercises, but not swimming.
Most studies had a moderate to high risk of bias, limiting conclusion strength.
Abstract
Introduction: Exercise has proven to be an excellent tool for improving health in individuals with hypertension. A particularly interesting environment for performing exercise is the aquatic medium, whose unique properties have shown effectiveness in reducing blood pressure values. Objective: Our objective was to provide an update on the available scientific evidence regarding the effects of aquatic exercise on individuals with hypertension. Methods: A systematic search was conducted in the databases PubMed, Web of Science, CINAHL, Sport Discus, Medline, Scopus, and PEDro. Methodological quality was assessed using the PEDro scale, and the risk of bias was evaluated using the RoB 2 tool. Results: Eleven studies were included, with a total of 402 participants, obtaining a mean score of 5.7 on the PEDro scale. Five studies presented a high risk of bias, four showed a low risk, and in two,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
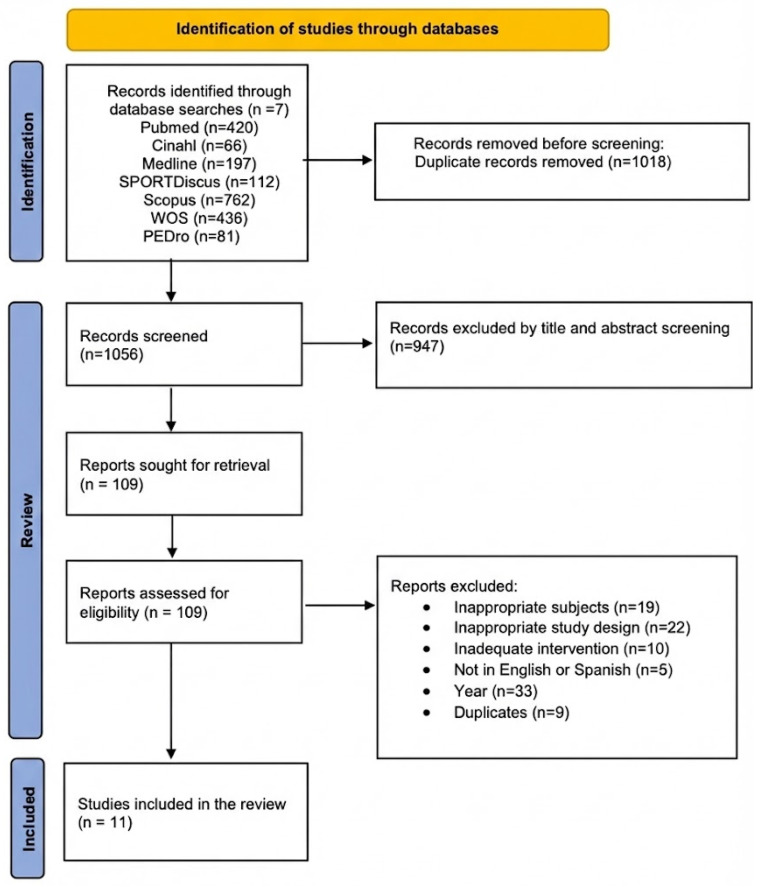 Figure 1
Figure 1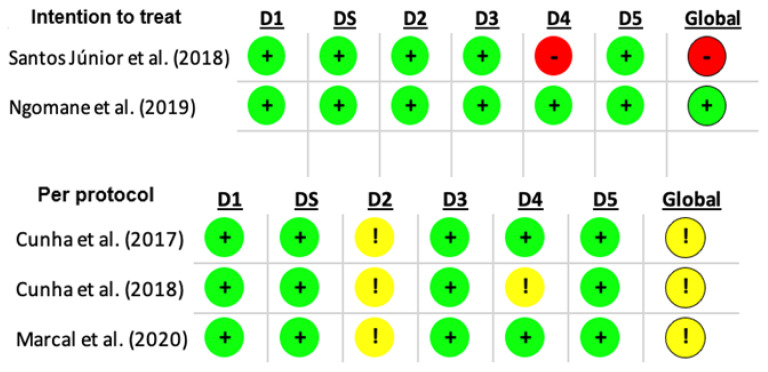 Figure 2
Figure 2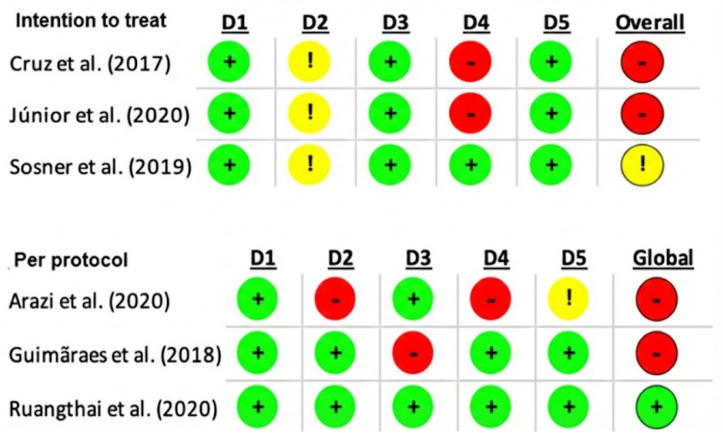 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular and exercise physiology · Physical Activity and Health · Sodium Intake and Health
1. Introduction
According to the World Health Organization, hypertension (HTN) is one of the most prevalent cardiovascular diseases worldwide, affecting a total of 1.28 billion people aged between 30 and 79, and being responsible for over 8.5 million deaths globally [1]. Additionally, having HTN is a risk factor for stroke, myocardial infarction, heart failure and chronic kidney disease at any age, as well as worsening quality of life and increasing healthcare costs [2].
Due to the high prevalence and negative consequences of HTN, healthcare professionals are compelled to seek alternatives to pharmacological treatment [3]. Physical inactivity has significantly contributed to the exponential rise in the number of individuals affected by HTN. To address this issue, evidence shows that increasing physical activity and participating in regular exercise can achieve effects comparable to, or even greater than, pharmacological treatments, without the associated side effects [4,5,6,7].
Recent systematic reviews have reinforced this idea in individuals with HTN, showing reductions in resting blood pressure (BP) and arterial resistance [8,9]. A highly beneficial form of exercise is aquatic exercise, which enables activities to be performed with reduced gravitational impact, provides resistance through water, and allows for high-intensity workouts with lower perceived effort [10]. Additionally, the aquatic environment offers specific benefits for patients with HTN, including suppression of the sympathetic nervous system and a reduction in vascular resistance [11]. From a cardiovascular standpoint, the aquatic environment could be favourable, in addition to the well-known benefits of physical exercise. It is worth mentioning that aquatic exercise has shown positive effects in multiple systematic reviews, such as reducing fatigue in women with cancer [12], improving balance and spasticity in patients who have suffered a stroke [13], improving symptoms in people with depression [14], as well as the lipid profile and BP of individuals with diabetes mellitus [10]. Additionally, a review compiling articles up to 2017 suggests the effectiveness of aquatic exercise in reducing BP [15]. However, the effects and benefits of aquatic exercise are still being investigated today [16]. For these reasons, and because the prevalence of HTN continues to rise [17], the objective of this systematic review is to update and analyze the effects of aquatic exercise on individuals with HTN.
2. Materials and Methods
2.1. Design
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA [18]) guidelines and the recommendations for their implementation in exercise, rehabilitation, and sport sciences (PERSiST [19]). It was registered in PROSPERO (registration code: CRD42024549899). The systematic search was conducted during April 2024 across seven databases: PubMed, Web of Science, CINAHL, Sport Discus, Medline, Scopus, and PEDro. The search equation included a combination of MESH terms (aquatic therapy and hypertension) and free terms, with or without truncation (using the asterisk), which provided greater variability: (aquatic aerobics, aquatic exercise, aquatic sport*, aquatic rehabilitation, aquatic activity, aquatic physical therapy, water-based exercise*, water aerobics, water exercise*, water sport*, water rehabilitation, water activity, water therapy, swimming) with Boolean operators AND and OR (Supplementary Material Table S1).
The search strategy, based on the PICOS framework, was as follows: P—population: individuals over 18 years old with HTN; I—intervention: aquatic exercise; C—comparison: another intervention, placebo, or no intervention; O—outcomes: any health variable related to hypertension (HTN) and the cardiorespiratory system, such as effects on blood pressure (BP), maximum oxygen uptake (VO2Max), and endothelial function; S—study design: randomized controlled trials.
2.2. Study Selection
First, duplicate articles were removed. The two most experienced authors in cardiac rehabilitation conducted the study selection process to ensure expert evaluation. A third reviewer resolved any discrepancies. The inter-reviewer agreement was assessed using the Kappa index, yielding a value of 0.9, indicating near-perfect agreement. Once this process was completed, each study was analyzed using the following inclusion criteria: (i) individuals over 18 years old, (ii) with HTN, (iii) randomized controlled trials (RCTs), (iv) intervention involving aquatic exercise, (v) publication in English or Spanish. Exclusion criteria were also applied: (i) full text not available, (ii) publication date earlier than 2017. The exclusion criteria were applied using a customized Microsoft Excel table to filter the results. The restriction to studies published from 2017 onwards was applied to provide an update of the most recent evidence, as the earlier literature on aquatic exercise and blood pressure had already been synthesized in a previous systematic review [15].
2.3. Data Extraction
The following data were extracted for further analysis: demographic information (title, authors, journal, and year), sample characteristics (age, sex, number of participants, inclusion/exclusion criteria, and supervisor), specific study parameters (duration of intervention, adverse events, and exercise methods), and the outcomes obtained (analyzed variables, instruments used, and follow-up duration). Tables were used to describe both the study characteristics and the extracted data.
2.4. Quality Assessment
The PEDro scale [20] was used to assess the methodological quality of the studies, and the Risk of Bias 2.0 tool (RoB 2) [21] was applied to analyze the risk of bias, differentiating between parallel and crossover studies. Two independent reviewers applied the respective scales to assess the validity of the articles. In cases of disagreement, a third reviewer was consulted to make the final decision on the studies included in the analysis.
2.5. Data Synthesis
Due to substantial heterogeneity among the included studies in terms of intervention duration, frequency, intensity, protocol design, outcome measures, and the predominance of studies assessing acute responses, a quantitative meta-analysis was not considered appropriate. Therefore, a structured qualitative synthesis was conducted. The findings were organized according to the type of intervention (acute responses vs. structured training programmes) and the cardiovascular outcomes evaluated.
3. Results
3.1. Study Selection
From the 2074 results in the initial search, 1056 articles were identified for analysis after removing duplicates. Through title and abstract screening, 947 articles were excluded for not meeting the inclusion criteria. Subsequently, the remaining 109 articles were subjected to exclusion criteria using a customized Microsoft Excel template. At the full-text stage, the most frequent reasons for exclusion were non-randomized study design, interventions not involving aquatic exercise, populations without hypertension, absence of relevant cardiovascular outcomes, and duplicate reporting of results. Finally, 11 articles were included in this review [22,23,24,25,26,27,28,29,30,31,32]. Figure 1 shows the flow diagram detailing the study selection process.
3.2. Methodological Quality and Risk of Bias in the Included Studies
The methodological quality of the studies was 4 points or higher. The highest score was 7 [29,30]. The average score of the articles was 5.7 (Table 1) [33].
In all studies, there was no selection bias. Regarding the parallel RCTs [22,23,26,28,31,32], the most common bias was the outcome measurement bias [22,23,28] (Figure 2 and Figure 3).
3.3. Sample Characteristics
The age of participants in most studies was over 60 years [24,25,27,28,29,30,31]. Only three studies included individuals under 55 years of age [23,26,32]. Two studies included only women [22,28] (Table 2).
The total sample analyzed across the 11 included studies comprised 402 participants, of whom 185 engaged in aquatic exercise, 55 participated in dry-land training, and 162 were allocated to the control group. In terms of BP levels, the minimum inclusion criterion in all studies was ≥130/85 mmHg. However, in 63.6% of the studies, participants were required to have BP levels of ≥140/90 mmHg to be included in the study [23,24,25,26,27,29,30] (Supplementary Material Table S2). No adverse effects were reported in any of the studies included in the systematic review [22,23,24,25,26,27,28,29,30,31,32].
3.4. Characteristics of the Intervention
The interventions analyzed showed considerable variability in design, ranging from single-session protocols assessing acute responses to multi-week programmes aimed at inducing training adaptations. In 54.5% of the studies, a single aquatic exercise session was conducted, and the hypotensive response and BP behavior were assessed over the 24 h post-session [24,25,27,28,29,30]. Additionally, five studies conducted an intervention consisting of two or three weekly sessions over 2, 8, or even 12 weeks [22,23,26,31,32]. Session duration generally ranged from 40 to 60 min [22,23,24,25,26,27,28,31], except for three studies where it was 30 min [29,30,32] (Table 2).
The aquatic exercise sessions were divided into a 5–10 min warm-up, a main part lasting between 30 and 40 min, and a 5–10 min cool-down in all studies [22,23,24,25,26,27,28,29,30,31], except for one study where the main part lasted for 20 min [32]. Most sessions consisted of aerobic exercises (walking or running) combined with strength-resistance exercises against the water (moving different body segments, weight transfers, and/or functional movements) [22,23,24,25,27,28,31]. Notably, none of the interventions included swimming.
To calculate exercise intensity, most studies used maximum heart rate [22,24,25,27], the Rate of Perceived Exertion scale [29,30] or the Borg scale [23,26,31]. In two other studies, Peak Power Output [32] and heart rate reserve [28] were used.
In all the studies analyzed, the water temperature was around 30 °C [23,24,25,26,27,28,29,30,31,32], except for the study by Arazi et al. [22], where the temperature ranged from 34 to 36 °C.
Regarding the control groups, in three studies [22,23,26], participants were instructed to maintain their daily life activities. In two studies, water immersion was performed [27,30]. In four studies, participants remained seated or standing in conditions similar to the intervention group [24,25,29]. In two studies, they performed exercise. And in one study, the control condition was not specified [31] (Supplementary Material Table S3).
3.5. Results of the Studies Provided in Relation to BP, VO2max, and Endothelial Function
Studies assessing acute post-exercise responses reported BP changes within 24 h following aquatic exercise sessions. In contrast, studies evaluating multi-week training programmes reported reductions in resting BP measured at post-intervention time points. Most included studies reported reductions in BP following aquatic exercise, although the timing and magnitude varied across protocols and assessment windows [22,23,24,25,26,27,28,29,30,31,32]. Only a limited number of training-based studies assessed cardiorespiratory fitness; among those, improvements in VO_2_max were reported in some trials, while others did not observe significant changes. Specifically, Arazi et al. [22] reported a significant increase in the aquatic exercise group compared with baseline values. However, in the studies by Júnior et al. [27] and Ruangthai et al. [31], no significant improvements in this variable were observed in any of the groups. Endothelial function and oxidative stress markers were assessed in fewer studies, with some studies reporting significant changes and others reporting no significant differences. As for endothelial function, the studies by Ngomane et al. [29] and Marcal et al. [30] did not report significant changes in endothelial reactivity in the groups that performed aquatic exercise compared to other groups. Nonetheless, Ruangthai et al. [31] found significant improvements in oxidative stress markers and endothelial function in the aquatic exercise group compared to the control and land-based exercise groups (Table 2).
4. Discussion
The purpose of this systematic review was to evaluate the effects of aquatic exercise on individuals with HTN. The main findings indicate that aquatic exercise may contribute to reductions in BP levels [22,23,24,25,26,27,28,29,30,31,32], and may also be associated with improvements in cardiorespiratory fitness, such as VO_2_max [22,31] and cardio metabolic parameters [31]. It is important to distinguish between statistical significance and clinical relevance. While several studies demonstrated significant reductions in blood pressure, the clinical impact of these changes may differ depending on their magnitude and whether they represent acute responses or sustained adaptations. Even modest reductions in blood pressure have been associated with reduced cardiovascular risk at the population level; however, the heterogeneity of protocols and predominance of acute studies in this review limit direct clinical extrapolation. More consistent reductions in blood pressure were observed in studies involving structured multi-week programmes that combined aerobic and resistance exercise in thermoneutral water, particularly among participants with moderate hypertension. In contrast, single-session interventions produced more variable responses, reflecting the transient nature of acute post-exercise hypotension. Differences in baseline BP levels may also have influenced the magnitude of change, with participants presenting higher initial BP values showing greater absolute reductions.
Regarding structured exercise, the results of this review are consistent with the effects of exercise on BP found in other reviews, showing a reduction in BP [9,34]. Performing exercise, regardless of its intensity, has been shown to reduce the risk of hypertensive incidents and improve endothelial pathophysiology in individuals with HTN [34]. In HTN, the endothelium can experience dysfunction, leading to several adverse changes: decreased nitric oxide production, increased production of reactive oxygen species, inflammation, and procoagulation [35]. Multiple reviews have demonstrated positive effects in individuals with HTN, regardless of the type of exercise (aerobic, resistance, or isometric), age, sex, or ethnicity [36,37,38].
Most reviews have evaluated the effects of exercise on hypertension primarily on land [36,37,38]. However, the aquatic environment offers multiple advantages over land-based exercise, allowing individuals with comorbidities to engage in physical activity [39]. Additionally, energy expenditure in water is similar to that of land-based exercise [40]. In recent years, aquatic exercise has gained popularity due to its unique benefits, such as the natural resistance of water, which enables low-impact yet effective training for muscle strengthening and the management of chronic conditions [10]. Furthermore, it reduces body weight and joint stress, making it accessible to most individuals [41,42]. Additionally, Zhou et al. [16] highlight that, due to these benefits, research on aquatic exercise and its impact on cardiovascular health has increased. Angraini et al. [43], in a broader review on hydrotherapy, suggest that aquatic exercise could significantly reduce blood pressure in patients with hypertension. Similarly, a 2018 review, which included both healthy adults and individuals with hypertension, reported comparable benefits [37].
The effectiveness of exercise in lowering BP may be greater in aquatic environments compared to land-based exercise, likely due to the physiological changes induced by partial body immersion, such as reduced vascular tone and peripheral vascular resistance [11]. These effects may enhance the body’s response to exercise in water compared to land-based exercise [11]. Water immersion affects the cardiovascular system by redistributing blood flow to the heart due to hydrostatic pressure gradients [44,45]. This may increase cardiac output and contribute to a hypotensive response, which can also be influenced by water temperature [44,45]. However, it should be noted that most of these mechanistic explanations are based on established physiological principles and the previous literature, as only a limited number of included studies directly assessed endothelial or oxidative stress markers.
Water immersion alone could trigger a hypotensive response [46]. This may partly explain the variability observed among the included studies. For example, Marçal et al. [30] did not observe significant BP changes compared to the control condition despite 30 min of water immersion, whereas Santos Júnior et al. [27] reported significant hypotensive responses under similar immersion durations [27].
When performing exercise in water, it is important to consider water temperature, as studies have shown that the water’s temperature can produce different physiological effects on the body [45,47,48]. For example, water slightly cooler than body temperature reduces overheating, warm water may relieve joint pain, and cold water lowers heart rate and/or cardiac output [45,47,48]. Additionally, temperatures around 30 °C influence metabolism due to increased sympathetic system activation [49]. Generally, recommendations for moderate-to-vigorous intensity aquatic exercise in elite athletes suggest maintaining water temperatures between 25 °C and 28 °C [50]. However, other authors recommend that the water temperature be neutral, between 33.5 °C and 35.5 °C [44]. This allows for sufficiently prolonged immersion periods for exercise in various pathologies [44]. In the studies analyzed, the water temperature in all but one study was around 30 °C, except for the study by Arazi et al. [22], where the temperature ranged from 34 to 36 °C, as the study was conducted in volcanic waters. Higher than recommended temperatures have been suggested to potentially influence the hypotensive response [51].
When it comes to the type of exercise used, the included studies utilized aerobic and/or resistance training against water [22,23,24,25,27,28,31] at a moderate intensity. However, a meta-analytic review suggests that the most effective type of exercise for reducing systolic and diastolic BP is isometric exercise [9]. This may be due to its acute activation of the metaboreflex, which reduces oxidative stress in tissues, improves endothelial function, and promotes changes in baroreflex sensitivity, as well as long-term balance in the autonomic nervous system [52]. Some of these effects might also be achieved through prolonged aquatic exercise [53]. Nonetheless, it would be interesting to evaluate BP responses to an aquatic exercise program incorporating isometric exercise.
The intensity used in most studies was moderate [22,23,25,26,28,29,30,31], except for the study by Santos Júnior et al. [27], where they reached up to 89% of maximum heart rate, and Sosner et al. [32], where they achieved 100% of peak oxygen power. In the latter, a greater reduction in BP was observed within 24 h post-exercise compared to the moderate exercise group [32]. However, it is important to note that, in the review conducted by Caldas Costa et al. [54], both the moderate-intensity exercise group and the high-intensity group achieved similar reductions in BP. These findings were supported by a later review by Leal et al. [55].
Regarding the duration of the interventions, only five studies [22,23,26,31,32] included multiple sessions to promote chronic adaptations rather than acute hypotensive responses. Long-term BP reduction may result from improved baroreflex sensitivity, achievable after ~8 weeks of training [53,56]. However, these mechanistic interpretations are based on physiological rationale and the previous literature, as most included studies did not directly measure these pathways.
Analyzing the studies that aimed to assess changes in VO2max [22,23,28], significant improvements were only observed in the study by Arazi et al. [22]. This may be related to the fact that detectable improvements in VO_2_max generally require interventions lasting at least 4–8 weeks [57]. Among the studies analyzed, only two reached the minimum duration of 4 weeks [22,23].
Several studies [22,23,24,25,32] have reported 100% adherence to the exercise program [22,23,24,25,32]. This may be due to the fact that aquatic exercise is enjoyable, provides a change in environment, and results in a lower perceived effort compared to land-based exercise [10,58].
This review presents several methodological limitations that should be considered when interpreting the findings. The included studies showed marked variability in intervention characteristics, such as duration (single-session vs. multi-week programmes), frequency, intensity, water temperature, and outcome measures, which limits direct comparisons and reduces the generalizability of the results. Furthermore, the predominance of studies assessing acute post-exercise responses, compared with fewer trials evaluating structured training interventions, complicates interpretation of sustained effects. The absence of long-term follow-up data and the lack of meta-analytic synthesis further constrain the strength of the conclusions.
In addition, the overall methodological quality of the studies was moderate, with several trials presenting a high risk of bias, particularly in outcome measurement and blinding procedures, which are common challenges in exercise research. The relatively small number of eligible studies, together with the limited number of randomized controlled trials, reduces the overall certainty of the evidence. The restriction to publications from 2017 onwards may have excluded relevant earlier trials and introduced temporal bias. Similarly, restricting inclusion to studies published in English or Spanish may have excluded relevant evidence in other languages and represents a potential source of language bias. The possibility of publication bias cannot be ruled out, as studies reporting positive findings are more likely to be published. These methodological issues restrict the strength of the conclusions and limit the generalizability of the findings to broader hypertensive populations. Future research should prioritize well-designed longitudinal trials to better clarify long-term adaptations and underlying physiological mechanisms.
5. Conclusions
Aquatic exercise appears to be a potentially effective and safe alternative for reducing blood pressure in individuals with hypertension, although these findings should be interpreted with caution given the moderate methodological quality and risk of bias identified in several included studies. This systematic review analyzed eleven studies with 402 participants, where the interventions included water walking, mobility exercises, strength training, and high-intensity interval training. The results show a significant reduction in blood pressure compared to control groups, along with improvements in VO_2_max and oxidative stress markers. These effects may be partly explained by the reduction in peripheral vascular resistance induced by immersion, along with lower perceived effort and a change in environment, which enhance exercise adherence.
Most studies included patients with moderate to high hypertension, although some considered mild cases, suggesting benefits across different disease severities. However, it is important to note that most of the available evidence relates to acute post-exercise responses, while only a smaller number of studies investigated structured programmes lasting several weeks. Therefore, evidence supporting chronic cardiovascular adaptations remains preliminary. Due to variability in protocols and lack of follow-up, more rigorous and prolonged trials are needed to consolidate the evidence and define an optimal aquatic exercise program.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zhou B. Carrillo-Larco R.M. Danaei G. Riley L.M. Paciorek C.J. Stevens G.A. Gregg E.W. Bennett J.E. Solomon B. Singleton R.K. Worldwide Trends in Hypertension Prevalence and Progress in Treatment and Control from 1990 to 2019: A Pooled Analysis of 1201 Population-Representative Studies with 104 Million Participants Lancet 202139895798010.1016/S 0140-6736(21)01330-134450083 PMC 8446938 · doi ↗ · pubmed ↗
- 2Zhou B. Perel P. Mensah G.A. Ezzati M. Global Epidemiology, Health Burden and Effective Interventions for Elevated Blood Pressure and Hypertension Nat. Rev. Cardiol.20211878580210.1038/s 41569-021-00559-834050340 PMC 8162166 · doi ↗ · pubmed ↗
- 3Valenzuela P.L. Carrera-Bastos P. Gálvez B.G. Ruiz-Hurtado G. Ordovas J.M. Ruilope L.M. Lucia A. Lifestyle Interventions for the Prevention and Treatment of Hypertension Nat. Rev. Cardiol.20211825127510.1038/s 41569-020-00437-933037326 · doi ↗ · pubmed ↗
- 4Fiuza-Luces C. Garatachea N. Berger N.A. Lucia A. Exercise Is the Real Polypill Physiology 20132833035810.1152/physiol.00019.201323997192 · doi ↗ · pubmed ↗
- 5Naci H. Salcher-Konrad M. Dias S. Blum M. Sahoo S.A. Nunan D. Ioannidis J.P.A. How Does Exercise Treatment Compare with Antihypertensive Medications? A Network Meta-Analysis of 391 Randomised Controlled Trials Assessing Exercise and Medication Effects on Systolic Blood Pressure Br. J. Sports Med.20195385986910.1136/bjsports-2018-09992130563873 · doi ↗ · pubmed ↗
- 6Pescatello L.S. Mac Donald H.V. Lamberti L. Johnson B.T. Exercise for Hypertension: A Prescription Update Integrating Existing Recommendations with Emerging Research Curr. Hypertens. Rep.2015178710.1007/s 11906-015-0600-y 26423529 PMC 4589552 · doi ↗ · pubmed ↗
- 7Hanssen H. Boardman H. Deiseroth A. Moholdt T. Simonenko M. Kränkel N. Niebauer J. Tiberi M. Abreu A. Solberg E.E. Personalized Exercise Prescription in the Prevention and Treatment of Arterial Hypertension: A Consensus Document from the European Association of Preventive Cardiology (EAPC) and the ESC Council on Hypertension Eur. J. Prev. Cardiol.20222920521510.1093/eurjpc/zwaa 14133758927 · doi ↗ · pubmed ↗
- 8Saco-Ledo G. Valenzuela P.L. Ruilope L.M. Lucia A. Physical Exercise in Resistant Hypertension: A Systematic Review and Meta-Analysis of Randomized Controlled Trials Front. Cardiovasc. Med.2022989381110.3389/fcvm.2022.89381135665271 PMC 9161026 · doi ↗ · pubmed ↗