Recent Advances in AI and GenAI for Health Informatics
Sio Iong Ao, Vasile Palade, Chris Holt, Suzy Araujo, Mike Gourlay, Danina Kapetanovic

TL;DR
This paper reviews recent AI and GenAI applications in health informatics, highlighting opportunities and challenges across five key healthcare areas.
Contribution
The paper provides a broad, comprehensive review of AI in health informatics, covering five major topics and identifying common concerns and future directions.
Findings
Clinical decision support, patient care, and electronic health records are the most mentioned AI applications in health informatics.
Common concerns include patient privacy, cybersecurity, ethics, and lack of explainability in AI systems.
The review emphasizes the need for benchmarks, standardization, and engaging health professionals in AI adoption.
Abstract
The emergence of large language models (LLMs) and generative artificial intelligence (GenAI) has marked a turning point in health informatics. AI has become a very helpful tool for health informatics applications, with numerous AI applications in health informatics being reported in the last years. The objective of this paper is to synthesize the common concerns and opportunities raised by recent popular reviews on AI and health informatics. The main methodological topics covered in this up-to-date review include traditional AI, GenAI, and LLMs. The literature search was conducted through the popular academic database Scopus, which covers over one hundred million records, including both computer science and healthcare. Among these popular reviews (measured by the number of citations that each one received), clinical decision support, patient care, electronic health records, hospital…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
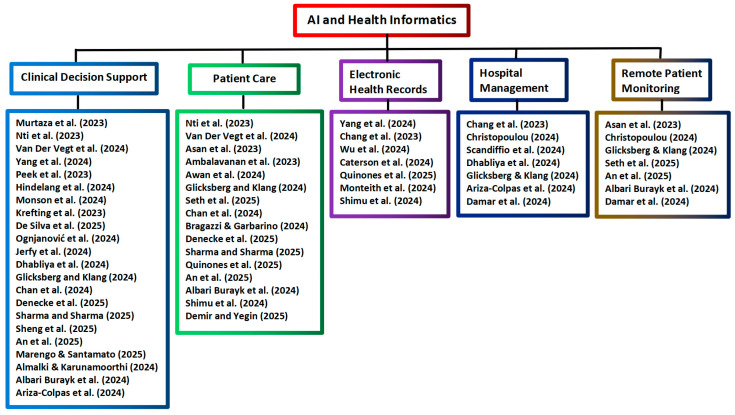 Figure 2
Figure 2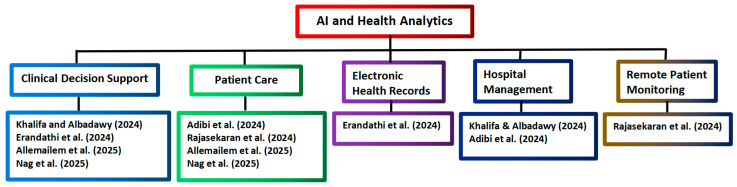 Figure 3
Figure 3| Authors | No. of Articles | Application Topics | Summaries |
|---|---|---|---|
| Murtaza et al. [ | 70 | Clinical Decision Support | It explored various techniques for generating synthetic medical data with built-in privacy safeguards and evaluated different synthetic data approaches |
| Hua et al. [ | 31 | Diagnostic Imaging | It identified the primary factors that influence how healthcare workers in medical imaging perceive and accept AI |
| Yang et al. [ | 8 | Clinical Decision Support | Nine critical areas facing difficulties due to the rapid development of big data technologies in the context of precision medicine were identified |
| Nti et al. [ | 18,729 | Clinical Decision Support | The substantial number of publications reflects the increasing emphasis on leveraging technology to improve healthcare systems. |
| Van Der Vegt et al. [ | 37 | Clinical Decision Support | It focused on the use of artificial intelligence to predict real-time clinical deterioration in hospitalized adults |
| Asan et al. [ | 20 | Patient Care | It examined the influence of AI on consumer health informatics |
| Gurmessa and Jimma [ | 14 | Diagnostic Imaging | It focused on the use of XAI in diagnosing breast cancer through mammography and ultrasound imaging |
| Yang et al. [ | 37 | Clinical Decision Support | It centered on over-sampling strategies designed to manage multi-class imbalances in medical and other datasets, aiming to enhance the accuracy of AI-based predictive models. |
| Chang et al. [ | 24 | Electronic Health Records | It explored the advantages of artificial intelligence, the Internet of Things, and personal health records in improving healthcare delivery |
| Wu et al. [ | 37 | Electronic Health Records | It assessed burnout among healthcare professionals in relation to electronic health record usage |
| Christopoulou [ | 18 | Remote Patient Monitoring | It investigated how ML is utilized in evidence-based telehealth and smart care |
| Peek et al. [ | 27 | Clinical Decision Support | It highlighted that the shift toward digital health services is driven by AI and data sharing |
| Hindelang et al. [ | 18 | Clinical Decision Support | It explored the role of chatbots in taking medical histories |
| Scandiffio et al. [ | 19 | Hospital Management | It investigated how mentoring and coaching strategies support healthcare professionals in adopting digital tools, including artificial intelligence. |
| Caterson et al. [ | 76 | Electronic Health Records | It focused on explainable AI applications in electronic health record analysis. |
| Ambalavanan et al. [ | 14 | Patient Care | It explored how AI technologies can help understand long COVID |
| Monson et al. [ | 3939 | Clinical Decision Support | It examined the use of AI in ophthalmology and vision science |
| Krefting et al. [ | 6 | Clinical Decision Support | It examined current trends and applications of clinical decision support systems in obstructive sleep apnea management |
| De Silva et al. [ | 72 | Clinical Decision Support | It explored how speech signal analysis can support the clinical decision process |
| Ognjanović et al. [ | 17 | Clinical Decision Support | It examined developments in biomedical and health informatics |
| Awan et al. [ | 5 | Patient Care | It explored the intersection of social media, crowdsourced data, and AI in public health |
| Jerfy et al. [ | 27 | Clinical Decision Support | It highlighted the implementation of natural language processing in healthcare |
| Dhabliya et al. [ | 10 | Hospital Management | It explored the advantages of AI in the healthcare domain |
| Glicksberg and Klang [ | 50 | Hospital Management | It focused on the most impactful AI research in health and life sciences over the past three years |
| Seth et al. [ | 158 | Remote Patient Monitoring | It revealed prevalent topics within the Internet of Medical Things |
| Chan et al. [ | 33 | Patient Care | It focused on noninvasive blood glucose monitoring with artificial intelligence |
| Bragazzi and Garbarino [ | 8 | Patient Care | It explored the emerging field of sleep infodemiology and infoveillance |
| Denecke et al. [ | 38 | Patient Care | It identified both enablers and barriers to adopting AI in participatory health informatics |
| Sharma and Sharma [ | 12,974 | Patient Care | It emphasized AI’s transformative potential to enhance patient outcomes, streamline healthcare operations, and spark innovation across the sector |
| Quinones et al. [ | 25 | Patient Care | It explored how machine learning can predict patient-reported outcome measures following spinal surgery |
| Sheng et al. [ | 5 | Clinical Decision Support | It focused on using AI for detecting oral cancer |
| Demir and Yegin [ | 32 | Genomic Medicine | It investigated AI’s role in disease prediction and genomic data analysis |
| An et al. [ | 867 | Patient Care | It explored how artificial intelligence is being applied in obstructive sleep apnea |
| Marengo and Santamato [ | 63 | Clinical Decision Support | It focused on the use of quantum computing to enhance AI applications in medicine and its role in strengthening the security of healthcare data |
| Almalki and Karunamoorthi [ | 17 | Clinical Decision Support | Artificial intelligence is capable of contributing meaningfully to various phases of outbreak management |
| Albari Burayk et al. [ | 7 | Patient Care | It investigated diabetic ketoacidosis and hyperosmolar hyperglycemic state, in addition to current clinical protocols and treatment procedures |
| Monteith et al. [ | 5 | Electronic Health Records | It investigated the intersection of artificial intelligence, cybersecurity threats, and healthcare |
| Ariza-Colpas et al. [ | 1134 | Hospital Management | It examined the application of artificial intelligence in understanding long-term symptoms associated with COVID-19 |
| Damar et al. [ | 32,046 | Hospital Management | It explored the influence of artificial intelligence, machine learning, robotic process automation, and virtual reality on healthcare systems |
| Shimu et al. [ | 9 | Electronic Health Records | It explored the role of health informatics in addressing drug addiction |
| Authors | No. of Articles | Application Topics | Summaries |
|---|---|---|---|
| Khalifa and Albadawy [ | 30 | Hospital Management | It explored how artificial intelligence is reshaping diagnostic imaging [ |
| Adibi et al. [ | 8 | Hospital Management | It reviewed how AI contributes to healthcare in smart environments where the spaces were equipped with sensors, digital tools, and location-aware services |
| Rajasekaran et al. [ | 11 | Remote Patient Monitoring | It focused on wireless body area networks topics, like protocols, security, authentication, and embedding with AI |
| Erandathi et al. [ | 102 | Electronic Health Records | It focused on using artificial intelligence to predict complications associated with diabetes mellitus |
| Allemailem et al. [ | 15 | Clinical Decision Support | It examined the role of multi-sensor technologies in the regular surveillance of patient health |
| Nag et al. [ | 123 | Patient Care | It explored how AI technologies are reshaping patient care through the lens of emotional intelligence and person-centered interventions |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsArtificial Intelligence in Healthcare and Education · Machine Learning in Healthcare · Electronic Health Records Systems
1. Introduction
Health informatics denotes the deployment of digital tools to streamline healthcare processes, facilitate data interpretation, and support clinical judgments. Healthcare initiatives often focus on optimizing care delivery and enhancing patient outcomes through advanced digital technologies. Popular topics like decision support systems, predictive analytics, user-centered technologies, and ethical concerns are receiving growing attention in healthcare [1]. Another topic that is gaining popularity is the adoption of telehealth and mobile health technologies, especially following the onset of the COVID-19 pandemic [2].
AI demonstrates effectiveness across healthcare, including in early disease detection, drug discovery, treatment optimization, diagnostics, and decision support tools [3]. For example, in mobile health, AI is used for functions such as clinical decision support, patient education, health monitoring, remote consultations, and public health surveillance. Digital health tools like AI-driven wearable sleep monitors can help bridge knowledge gaps by disseminating reliable, evidence-based information to the public [4]. In medical imaging, AI holds the promise to boost performance and enhance patient care, as AI systems can process large volumes of imaging data and detect subtle patterns that may elude even experienced clinicians [5]. AI-driven tools are shown to be highly effective in interpreting diagnostic images like MRIs, CT scans, and X-rays. The AI application in radiological imaging has achieved diagnostic accuracy rates exceeding 90%, outperforming conventional approaches in identifying conditions like malignancies [6]. In diagnosing conditions, AI applications have also shown strong performance according to Lee and Kalpathy-Cramer [7].
AI tools become multifaceted digital aides for healthcare professionals [8]. AI is able to rapidly incorporate new medical information into its operational base, maintaining an up-to-date knowledge set that allows it to recommend the latest evidence-based treatments. In contrast, healthcare professionals must dedicate significant time to remain current with emerging medical literature, which may in turn limit their capacity to do so effectively [9]. AI can also enhance operational workflows by cutting down the time clinicians spend on repetitive managerial duties by as much as 70% in some tasks, according to Spatharou et al. [10].
This review investigates the contexts and details of the selected recent review articles on AI, GenAI, LLMs, and health informatics, such that practitioner audiences may benefit from more information about how these AI advances have already passed the pilot stages and have been implemented in many real-world health systems. Other names of traditional AI include narrow AI or weak AI, which refers to the intelligent execution of specific tasks [11]. GenAI may be regarded as the next AI generation that is capable of developing something new, while LLMs refer to AI, and in particular deep learning, for natural language processing for handling advanced human language-based tasks [12]. Section 2 describes our methods for identifying relevant recent review articles. In Section 3, we present the results of our literature searches and analysis. In Section 4, the focus is on the synthesis and discussion of the concerns in these reviews, such that high-level issues common across different health informatics topics are identified. Section 5 presents some conclusions. For the convenience of those readers who may like to have more information about the common terms in health informatics and AI, Appendix A presents a brief description of some popular medical terms and technologies mentioned in the reviews. Appendix B provides a brief description and explanation of how some common AI tools provide assistance in health informatics. Appendix C and Appendix D present more details about the reviews listed in Table 1 and Table 2, respectively.
2. Methods
Objective: The focus of this study is to synthesize the common concerns and opportunities raised by recent popular reviews on AI in health informatics.
Our literature search was conducted on 30 June 2025 through the popular academic database Scopus. The reason for choosing Scopus was that it is a comprehensive database of over one hundred million high-impact records, covering well a broad array of topics on both computer science and healthcare, which fits very well with the objective of our review. It consisted of the following two steps to select the recent popular reviews on AI and health informatics:
Literature Search I: The search was restricted to the Scopus terms “article title, abstract, and keywords”. The search was restricted to the combination “Artificial Intelligence” AND “Health Informatics”. The years covered were from 2023 onwards, and the article type was restricted to the type “review”. Another search was conducted with the restriction “Artificial Intelligence” AND “Health Analytics”.
Literature Search II: In this second stage, the focus is on the combination “Artificial Intelligence” AND “topic name”, where “topic name” refers to the popular topics of AI applications in health informatics. Here, the popular topics refer to the health informatics topics that have been frequently mentioned in the reviews, identified by analyzing the contexts of the above reviews by human experts. The goal of this stage was to select the highly cited reviews covering the popular topics for further analysis by human experts one by one. It was noted that, when setting the threshold at the 10 highly cited reviews for each topic, quite a number of highly cited reviews are excluded. On the other hand, when the threshold is set at values larger than 20, a few reviews that have only zero citations are included. Thus, the threshold of the 20 highly cited reviews was selected.
Note: It would be helpful to explicitly acknowledge that the limitations of this review include the citation lag, particularly given how quickly GenAI deployment and practice-based learning are evolving relative to citation cycles. Therefore, some interesting frontier GenAI deployments may not be included in this review, even though our supplementary literature search done on 20 January 2026 highlights our efforts to partly address this citation lag.
Supplementary Update I: a supplementary literature search was conducted on 20 January 2026, following the same procedure as the Literature Search I, in order to update the new literature data that have became available during the drafting of this review article.
Supplementary Update II: similarly, another supplementary literature search with the combination restriction using the terms “Artificial Intelligence” AND “Health Analytics” was conducted on the same day, i.e., 20 January 2026, following the same procedure as outlined in the above Literature Search II.
3. Results
3.1. Literature Search Results of AI and Health Informatics/Analytics
Literature Search I: For the combination “Artificial Intelligence” AND “Health Informatics”, a total of 40 reviews were found. For the combination “Artificial Intelligence” AND “Health Analytics”, a total of 6 reviews were found. Therefore, by combining these two searches together, a total of 46 reviews have been found. Key observations: It was found that 22 reviews covered clinical decision support, while the number of reviews covering patient care, electronic health records, hospital management, and remote patient monitoring were 16, 7, 7, and 7, respectively. It should be noted that there were reviews that covered several topics.
Literature Search II: For the five popular topics (clinical decision support, patient care, electronic health records, hospital management, and remote patient monitoring), a total of 100 influential review articles have been identified, and it was found that there were ten duplicate records. Note: The main reason for review article duplication is that a popular review may cover more than one topic. That review may appear as our selected review in multiple topic lists if it is popular across multiple topics. When we counted the total number of unique reviews that were covered in this review, we did not count this type of popular review multiple times. For the convenience of the practitioners, we make an effort to include these popular reviews in different topic lists. If a review that was popular across several topics was only included in one of its lists, some practitioners who were mainly interested in AI applications in one topic and who skipped other topic lists might have the chance of missing a few popular reviews on their specific target topic.
Thus, a total of 136 influential review articles have been identified after our Literature Searches I and II. All of these reviews are in English, and there are no further restrictions in the search results, besides the ones stated above. Figure 1 shows the framework of our Literature Search I and Literature Search II.
Supplementary Update I: A total of 89 review articles have been found (Note: Two Scopus search records were not included, as they were either only an overview of articles that were presented in a specific conference, or a column of articles in a particular journal). With the additional filter of the years covered set as 2023, 2024, and 2025, the total number of review articles has reduced to 54 reviews. In other words, there were only a total of 35 review articles that had been published before 2023, while fourteen new reviews have been published in 2025 after our literature search on 30 June 2025. For these fourteen new reviews, their main topics remain the same as the other 40 reviews in 2023, 2024, and 2025. Another observation is that in 2023, only 8 review articles were found. In 2024 and 2025, the number of review articles had increased rapidly to 24 reviews and 22 reviews, respectively. On the other hand, generally speaking, these 8 reviews in 2023 received much more citations than the reviews in 2024, while the reviews in 2024 have also obtained more citations than those published in 2025. The citation numbers of these eight reviews in 2023 are respectively: 136, 35, 20, 13, 12, 7, 3, and 0. The citation numbers of the twenty-four reviews in 2024 are respectively: 66, 50, 32, 29, 25, 22, 19, 16, 13, 11, 10, 6, 6, 6, 5, 5, 3, 3, 2, 1, 1, 1, 0, and 0. The citation numbers of the twenty-two reviews in 2025 are respectively: 7, 6, 5, 4, 3, 2, 2, 2, 2, 2, 1, 1, 1, 0, 0, 0, 0, 0, 0, 0, 0, and 0. This observation agrees with the fact that it takes time for other scientists to digest their findings and then cite their works.
Supplementary Update II: A total of 9 review articles have been found (Note: One Scopus search record was not included, as it is an editorial section of a specific journal). With the additional filter of the years covered set as 2023, 2024, and 2025, the total number of review articles has reduced to 7 reviews. In other words, there were only a total of 2 review articles that had been published before 2023, while one new review was published in 2025 after our literature search on 30 June 2025. In 2023, 0 review articles were found. In 2024 and 2025, the number of review articles had increased rapidly to 4 reviews and 3 reviews, respectively. On the other hand, generally speaking, the reviews in 2024 have obtained more citations than those published in 2025. The citation numbers of the four reviews in 2024 are respectively: 256, 63, 20, and 3. The citation numbers of the twenty-two reviews in 2025 are respectively: 3, 1, and 0.
When comparing the contexts of the reviews from the literature search on 30 June 2025 and the reviews from the supplementary update on 20 January 2026, the main topics of these reviews remain the same, i.e., clinical decision support, patient care, electronic health records, hospital management, and remote patient monitoring. The analysis of the selected reviews on AI applications in health informatics is presented in Table 1, and the tree diagram for grouping the AI and health informatics applications selected from Scopus is shown in Figure 2.
Tree diagram grouping the AI and health informatics applications from Scopus [1,4,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50].
The above forty reviews in Table 1 focus on several main topics of health informatics. Nineteen of the above reviews focus on covering only one topic in each review, while in seventeen reviews, two topics are covered in each review. In three other reviews by Yang et al. [15], An et al. [43], and Albari Burayk et al. [46], three topics are covered in each review. There is only one review by Glicksberg and Klang [35] that covers five topics of AI applications in health informatics. The analysis of the selected reviews on AI applications in health analytics is presented in Table 2, and the tree diagram for grouping the AI and health analytics applications selected from Scopus is shown in Figure 3.
Tree diagram grouping the AI and health analytics applications from Scopus [5,52,53,54,55,56].
The above six reviews in Table 2 focus on several main topics of health analytics. In five reviews, two topics are covered in each review. In another review by Khalifa and Albadawy [5], three topics (hospital management, diagnostic imaging, and clinical decision support) are covered.
3.2. Recent AI Applications in Clinical Decision Support
The goal for decision support in healthcare is to integrate sophisticated computational techniques that replicate expert medical reasoning. These systems should aim not only to emulate clinical expertise but also to elevate the overall standard of healthcare delivery [57]. In clinical decision-making, AI enhances complex diagnostic and therapeutic procedures by seamlessly integrating with existing healthcare systems to deliver a more holistic understanding of a patient’s condition. Clinical decision support tools powered by AI contribute to better patient outcomes by analyzing large-scale data, uncovering hidden patterns, and delivering evidence-based guidance. AI-based clinical decision support can also help minimize false alarms and ease the burden on medical personnel [58]. These AI models have also shown strong performance in risk stratification and forecasting cardiac events [59]. The majority (85%) reported improved clinical outcomes following implementation of clinical decision support systems according to Wingfield et al. [60]. The main tools, summaries, key concerns, and opportunities of the selected reviews of AI applications in clinical decision support are highlighted in Table 3.
Among the AI tools listed in Table 3, traditional machine learning methods are still very popular, especially for prediction purposes in works by Revilla-León et al. [63], Lambert et al. [65], Poweleit et al. [67], Gala et al. [59], Khalifa and Albadawy [5], Theodosiou and Read [71], Aminizadeh et al. [73], Sakagianni et al. [74], and Jeong et al. [75]. GenAI is gaining its popularity in health informatics in the studies of Eggmann et al. [61], Chen and Esmaeilzadeh [62], Bhayana [64], Cascella et al. [8], Akinci D’Antonoli et al. [69], and Theodosiou and Read [71].
3.3. Recent AI Applications in Patient Care
Through the integration of patient-specific data, including medical histories and personal traits, AI technologies offer targeted insights that support the design of customized treatment strategies [5]. The use of AI and big data analytics have bolstered capabilities in forecasting disease outbreaks and tailoring medical interventions to individual patients, resulting in a 22% drop in repeat hospitalization [78]. By taking over repetitive administrative and clinical jobs, AI can free up time for clinicians to engage more meaningfully with patients, enhancing care quality [79]. This kind of proactive patient engagement can lead to improved outcomes and reduced healthcare costs, according to Davenport and Kalakota [80]. These intelligent models also support remote care and ensure patients stick to their treatment regimens [81]. AI also has high potential in aiding the care of patients with long-term illness and individual-focused care, which emphasizes aligning medical decisions with each patient’s individual inclination, beliefs, and requirements [82]. The main tools, summaries, key concerns, and opportunities of the selected reviews of AI applications in patient care are highlighted in Table 4.
Among the AI tools listed in Table 4, traditional machine learning methods are still very popular, especially for analysis purposes in studies by Vora et al. [81], Muteeb et al. [3], Maleki Varnosfaderani and Forouzanfar [85], Kufel et al. [87], Bekbolatova et al. [89], Krishnan et al. [9], O’Connor et al. [92], Marques et al. [94], and Hughes et al. [96]. GenAI is gaining its popularity in health informatics in the studies by Alowais et al. [83], Al Kuwaiti [84], Maleki Varnosfaderani and Forouzanfar [85], Safranek et al. [93], and Garg et al. [97].
3.4. Recent AI Applications in Electronic Health Records
An electronic health record (EHR) is a digital alternative to traditional paper medical files. It captures a wide array of patient information, including past diagnoses, test results, medications, vaccination records, and treatment plans [99]. These records typically contain both structured elements like numerical lab results and unstructured elements like clinical notes, with EHR unstructured data being the dominant data source according to Hossain et al. [100]. The adoption of EHR systems marks a transformative shift in healthcare information management, offering substantial improvements in patient care, decision-making, and managerial effectiveness [101]. Over the last decade and a half, the most significant technological shift in healthcare has been the widespread adoption of EHRs [102]. In 2009, only a small fraction of U.S. hospitals had implemented EHRs; by 2019, they had become nearly universal according to the Office of the National Coordinator for Health Information Technology [103].
Popular AI applications in EHR include tasks like predictive analytics and classification. Traditional rule-based systems often fall short in precision when compared to machine learning algorithms, according to Davenport et al. [80]. The rich, high-dimensional nature of EHR data, which may not be handled well by rule-based systems, enables deep exploration by advanced AI tools like deep learning and the discovery of previously unrecognized trends. Deep learning transformers can be deployed to provide a tailored solution for EHR data [104]. This AI architecture can effectively capture patient histories using various contextual embeddings such as age, timeline position, visit frequency, and event type. AI systems can analyze a variety of data in EHRs to detect early indicators of health conditions, and LLMs can automate the identification of HER reports to improve the timeliness of necessary subsequent procedures [69]. As a result, AI systems can support faster intervention and potentially better long-term outcomes. Because of AI’s high potential, giant technology corporations like Amazon were developing a novel AI tool to extract meaningful insights from unstructured EHR entries and clinical documentation [105]. The main tools, summaries, key concerns, and opportunities of the selected reviews of AI applications in electronic health records are highlighted in Table 5.
Among the AI tools listed in Table 5, traditional machine learning methods are still very popular, especially for information processing purposes in the works of Al Kuwaiti et al. [84], Hossain et al. [100], Zhang et al. [108], Wang and Wang [109], Marques et al. [94], Chakraborty et al. [112], Gupta and Kumar [115], Ullah et al. [116], Armoundas et al. [117], Gupta et al. [118], Knevel and Liao [119], Thakkar et al. [120], and Jimma [121]. GenAI is gaining its popularity in health informatics in the studies of Al Kuwaiti et al. [84], Harrer [107], Akinci D’Antonoli et al. [69], Chakraborty et al. [112], and Wachter and Brynjolfsson [113].
3.5. Recent AI Applications in Hospital Management
AI is able to contribute to improvements in hospital administration in many ways, while effective management of staff, equipment, and operating room scheduling is essential for high-quality surgical care [122]. AI technologies are instrumental in forecasting surgery durations, managing room availability, and anticipating cancellations [123]. Automated systems handle tasks like medical coding, invoicing, and scheduling, which not only cut costs but also reduce staff workload, enabling them to devote more time to direct patient care [124,125]. Process automation has lightened the managerial burden in healthcare facilities by 40% in the study by Baskar et al. [126]. AI-powered computerization in management is able to shorten waiting times by approximately 30%, thereby enhancing hospital throughput [127]. AI tools like virtual assistants and chatbots, which can work around the clock, help streamline services ranging from clinical documentation and appointment scheduling to personalized patient care [128,129]. AI translation tools and speech recognition systems also break down communication barriers [130,131]. The main tools, summaries, key concerns, and opportunities of the selected reviews of AI applications in hospital management are highlighted in Table 6.
Among the AI tools listed in Table 6, traditional machine learning methods are still very popular, especially for management supporting purposes in the works of Srivani et al. [132], Zuhair et al. [133], Almotairi [134], MacMath et al. [135], Gazerani [136], Bellini et al. [123], Hashemi et al. [137], Mumtaz et al. [138], Vargas et al. [140], Wingfield et al. [60], Tamir-Degabli et al. [144], Sánchez Suárez et al. [145], Green and Castro [146], and Auza-Santivañez et al. [149]. GenAI is gaining its popularity in health informatics in the studies of Bellanda et al. [139], Sánchez Suárez et al. [145], Green and Castro [146], and Kim et al. [147].
3.6. Recent AI Applications in Remote Patient Monitoring
AI plays a key role in enhancing the ecosystem of remote patient monitoring (RPM) systems, which are commonly employed to track the health of patients from a distance, including those receiving in-home care or hospitalized individuals. AI-assisted RPM systems have significantly advanced the delivery of care by enabling continuous, tailored data monitoring and processing in real time, according to Patel et al. [150]. AI-powered remote monitoring has the potential to lower re-hospitalization rates and improve chronic disease management. The sensor data from RPM need advanced AI systems to process and analyze in real time [151]. Both traditional and deep learning methods can be deployed to analyze vital signs and categorize physical activity, like heart rate, blood pressure, respiratory rate, and oxygen saturation. The proactive capability of AI tools for predictive analytics and clinical decision-making can help prevent health deterioration and optimize care [152]. The main tools, summaries, key concerns, and opportunities of the selected reviews of AI applications in remote patient monitoring are highlighted in Table 7.
Among the AI tools listed in Table 7, traditional machine learning methods are still very popular, especially for decision-making supports in the studies of Shaik et al. [153], Carini and Seyhan et al. [154]; Nashwan et al. [155]; Akinola and Telukdarie [157]; Liang et al. [158], Jayousi et al. [159], Park et al. [160], Patel et al. [150], Hamid et al. [161], Jin et al. [162], Olawade et al. [164], Umer et al. [165], Kraman et al. [166], Rabiee [168], and Glyde et al. [169]. GenAI is gaining its popularity in health informatics in the study of Umer et al. [165].
4. Discussion About the Common Concerns Synthesised from Reviews, and Future Directions
The objective of this section is to discuss the common concerns raised by the selected reviews and to highlight some future directions, as the advancement of AI in health informatics comes with many limitations. Major concerns include patient privacy, cybersecurity, ethics, clinical accountability, engaging health professionals, benchmarks and standardization, and lack of explainability.
Concerns about patient privacy: Privacy threats stem from adversarial efforts to extract confidential data, leading to potential information breaches according to Qayyum et al. [170]. Privacy concerns related to AI can be broken down into three key phases: (I) Data Collection: risks include tampered input devices, falsified data, and breaches of data regulations; (II) Training: threats involve adversarial inputs and compromised training datasets leading to flawed models; and (III) Deployment: issues include the spread of misinformation or hallucinated outputs and exploitation through adversarial attacks. Because AI tools are trained on vast and often sensitive patient data, they can be vulnerable to misuse and data breaches [171]. Specific concerns involve unauthorized identification, biometric data misuse, and unintended AI-derived inferences about sensitive health conditions. Protecting privacy is hampered by challenges such as maintaining scalability, interpretability, data authenticity, system robustness, and achieving a balance between data utility and confidentiality [106]. Despite these difficulties, it is necessary to ensure that actions are taken for compliance with data privacy regulations like GDPR and HIPAA, according to Baskar et al. [126]. A differential privacy policy is helpful for protecting sensitive health data while still allowing for practical usage.
Concerns about cybersecurity: Hospitals using AI and IoT have reported a 32% spike in cybersecurity incidents, underscoring the need for advanced encoding and secure verification protocols [172]. Protecting patient information may need the deployment of advanced techniques such as data encryption and decentralized data management. With the recent advances of LLMs in health informatics, this introduces new concerns related to patient privacy and cybersecurity that must be actively addressed [61]. Strict regulations for protecting patient data are needed, as chatbots often process highly sensitive health information and must be safeguarded against unauthorized access or data breaches.
Concerns about ethics: Glicksberg and Klang [35] emphasized that the speed of developing robust regulation should match the rapid evolution of new AI technologies, while Chan et al. [37] emphasized the need of addressing regulatory concerns in future AI-powered monitoring technologies. Even though there is a growing movement to define ethical frameworks for AI use in healthcare, much broader regulatory cooperation will be essential to tackle complex legal questions involving liability and intellectual property. Ethical standards must guide all innovations in healthcare technologies. Principles like equity, transparency, and respect for patient rights should guide decision-making processes, especially in critical care. Actionable regulatory structures must evolve continuously, while ethics must be foundational to any regulatory framework governing AI in health informatics. Organizations may individually propose ethnic guidelines. As an example, the American Medical Association [173] has initiated a set of principles to guide the design, deployment, and application of AI technologies. Nevertheless, efforts by an individual organization may only generate a limited impact. Broad cooperation is needed to promote principles that emphasize the importance of transparency, equity, and responsibility in AI development and use. Mechanisms should be set up for ongoing oversight and system updates to ensure AI remains safe, ethical, and clinically effective after deployment. Woodman and Mangoni [77] and Pinto-Coelho [86] suggested that the development of explainable systems is worthy for future AI systems, such that the regulatory expectations in healthcare may be satisfied.
Concerns about clinical accountability: AI models may reinforce or introduce biases, potentially compromising diagnostic accuracy and the fairness of treatment recommendations [174]. Even though GenAI has raised the algorithmic capability of the AI tools, the probabilistic, non-deterministic outputs of this paradigm challenge traditional notions of validation, auditability, and clinical accountability. Health practitioners face challenges that the probabilistic, non-deterministic outputs from this paradigm differ significantly from the traditional notions of validation, auditability, and clinical accountability in the healthcare industry. Sauerbrei et al. [90] emphasized that special efforts are needed to ensure AI systems are transparent, unbiased, and accountable. Building trust in AI systems depends heavily on ensuring transparency in how decisions are made and establishing clear lines of accountability among developers, institutions, and practitioners. In addition, it is crucial to identify and mitigate biases in AI models that could exacerbate healthcare disparities. Algorithmic bias may be actively mitigated through inclusive datasets and continuous validation.
Concerns about engaging health professionals: Beyond the efficiency gains and reshaping patient care through AI and person-centered interventions, AI and GenAI are reshaping skills, roles, and trust calibration among healthcare professionals. As the healthcare professionals have generally been slow to integrate them into clinical workflows [175], it is necessary that healthcare organizations build trust in AI among professionals. Lambert et al. [65] stressed the importance of involving healthcare professionals early in AI development and emphasized the need for tailored training programs to ensure smooth adoption in clinical environments. It is important to ensure consistent AI literacy among health practitioners [176] by developing actionable plans of tailored AI training programs for the medical staff members. According to Khalifa and Albadawy [5], there should be enough future initiatives focusing on developing ethical standards, equipping healthcare workers with appropriate training, and ensuring that AI advancements remain focused on patient needs. Many case studies have already focused on showing excellent model performance and technical capability for even the traditional machine learning tools in various medical applications. Here, an interesting perspective is highlighted, which is about the difference between algorithmic capability and capability-in-use. In real-world healthcare practice, value is often determined by integration into clinical workflows, organizational readiness, and governance. As outlined in studies like Liang et al. [158] and Bignami et al. [151], the need for advanced infrastructure and staff training still remains a major limitation. Therefore, there exists a need to focus more on the real-world implementation of how to effectively incorporate AI into pre-surgical planning, clinical workflows, etc.
Concerns about benchmarks and standardization: The absence of standardized outcome metrics is a main hindrance to clinical decision support systems [177]. In order to fully harness the potential of biomedical big data, it is essential to effectively tackle a range of challenges related to data quality, algorithm efficiency, security protocols, and standardization across systems [15]. In response to the growing need for robust evaluation of AI tools, more efforts and actions should be put into the development of new frameworks and benchmarks for AI tools. It is encouraging to notice that new reporting frameworks such as STARD-AI, PROBAST-AI, SPIRIT-AI, CONSORT-AI, and DECIDE-AI have emerged. The DECIDE-AI guideline, in particular, addresses the evaluation of ML tools in early-stage, small-scale clinical settings, according to Vasey et al. [178].
Concerns about lack of explainability: The deployment of explainable AI may address the concerns about the lack of explainability in AI applications and has been gaining popularity in health informatics applications. Caterson et al. [26] focused on explainable AI applications in electronic health record analysis. Hulsen [72] talked about the need to make AI more explainable in future applications. Woodman and Mangoni [77] raised the need to develop explainable ML approaches that align with ethical standards and regulatory expectations in healthcare. Nevertheless, revealing how an AI model arrives at decisions could inadvertently expose sensitive patient data or enable malicious manipulation through reverse engineering [179]. The use of XAI introduces challenges related to data privacy and system security [72].
One future direction is to focus on how to fully utilize these new AI paradigms in healthcare with synthetic data by generative AI. Synthetic data presents a promising route to overcoming the privacy issues often associated with using real patient information in AI applications, according to Murtaza et al. [13]. With the recent advances in generative AI technologies, synthetic data is increasingly seen as a privacy-compliant alternative to real datasets and is gaining traction in healthcare communities. Chen et al. [180] emphasized that synthetic data plays a valuable role in evaluating novel artificial intelligence algorithms.
Another future development may focus on enhancing chatbot models with advanced AI for history-taking and incorporating them into clinical decision support systems for real-time, evidence-based recommendations [24]. Despite its capabilities, ChatGPT has notable flaws, such as factual inaccuracies, nonsensical content, and an inability to reliably provide medical advice. Given these limitations, ChatGPT is currently unsuitable for decision-making purposes in clinical environments [181]. Additionally, despite their utility, current chatbot systems still fall short in replicating the empathy and psychological understanding that human beings naturally offer, according to Li et al. [182].
The third future direction is about how to better implement/embed AI tools like LLMs for tasks related to electronic health records and hospital management in real-world healthcare environments. For example, AI can enhance evidence-based medical imaging selection. In documentation, AI can be deployed to automatically generate and update medical records by integrating data from various systems, reducing manual entry errors and enabling better-informed clinical decisions [183]. In inventory management, predictive AI models help hospitals maintain optimal supply levels by analyzing usage patterns and external factors like seasonal illnesses [184,185]. Financially, AI supports hospitals by automating tasks such as revenue forecasting, invoice auditing, and financial reporting, contributing to more strategic resource planning [186,187]. Deeper embedding of AI technologies into real-world settings may lead to even better healthcare operations.
The fourth future direction is to deploy more AI paradigms for healthcare, for example, continual learning, transfer learning, and few-shot learning, which are gaining traction from practitioners [188]. These advanced AI tools can allow effective model development, even with limited datasets. It became well-known that predictive models trained within a single health system often perform poorly when applied to new settings or populations, limiting their transferability, according to Wiens et al. [189]. On the other hand, some earlier studies show that advanced AI tools like transfer learning and few-shot learning could overcome these kinds of issues and successfully brought important advancements for AMR research [190].
The fifth future direction is about how to apply AI with social media data for better healthcare. AI has the potential to provide essential processing for social media data, according to Adishesha et al. [191], while social media content offers rich data that can inform various applications, including healthcare. There are opportunities for AI applications in sentence prediction and user-generated tagging. For example, AI-powered content analysis could provide a better understanding of public sentiment, opinions, and attitudes, particularly regarding digital education, during the COVID-19 pandemic [192].
The sixth future direction is to promote more multinational efforts of AI initiatives in health informatics in developing countries. As noted by Jimma [121], most AI research outputs to date have originated from wealthier nations, despite the fact that the majority of the world’s population lives in low- and middle-income countries. According to the 2021 Stanford AI Index, East Asia led AI-related academic publications with 26.7% of the total, followed by the United States with 14% [193]. This imbalance stems from disparities in research funding, infrastructure, institutional priorities, capacity, and even language barriers, according to Reis et al. [194]. More multinational efforts of AI initiatives for developing countries may help improve this imbalance. For example, AI-powered RPM is making psychiatric care more accessible in remote and underserved areas [195]. Through encrypted video consultations, psychiatrists can remotely assess and treat patients, ensuring consistent care and enabling collaboration with local health providers to deliver more holistic support [196,197]. Similarly, AI tools enable self-monitoring and remote diagnostics in eye care [162]. Better augmented reality and virtual reality technologies may further enhance remote consultations, according to Kouijzer et al. [198].
5. Conclusions
Sustainable healthcare represents a comprehensive approach to healthcare delivery that incorporates not only clinical outcomes but also economic, social, and environmental factors. The rapid advancement of technologies like artificial intelligence, the Internet of Things, big data analytics, and cloud computing are playing a crucial role in promoting the development of sustainable healthcare, according to Pammi et al. [199]. AI models contribute to healthcare sustainability by improving overall efficiency in healthcare [200], which in turn supports long-term organization sustainability.
A major future vision of AI in health informatics is to develop AI-assisted tools, like reliable virtual clinical assistants, to enable sustainable healthcare. These AI-powered virtual clinical assistants should be capable of deepening patient engagement, providing individualized health guidance, and supporting long-term stewardship of chronic illnesses [8]. It would also be interesting to explore the combination of blockchain technologies in the deployment of AI tools, as highlighted by Zhao et al. [201]. As shown by Qi et al. [202], traditional machine learning may not be able to provide desirable performance when handling complex issues. Applications of contrastive learning [203] may be very helpful for some difficult health informatics issues. While developing any of these AI projects in healthcare, collaborations among different stakeholders are needed to tackle the key concerns identified in this review for achieving better AI-assisted sustainable healthcare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nti I.K. Adekoya A.F. Weyori B.A. Keyeremeh F. A bibliometric analysis of technology in sustainable healthcare: Emerging trends and future directions Decis. Anal. J.2023810029210.1016/j.dajour.2023.100292 · doi ↗
- 2Wang B. Asan O. Mansouri M. Systems approach in telemedicine adoption during and after COVID-19: Roles, factors, and challenges IEEE Open J. Syst. Eng.20231384910.1109/OJSE.2023.3265430 · doi ↗
- 3Muteeb G. Rehman M.T. Shahwan M. Aatif M. Origin of Antibiotics and Antibiotic Resistance, and Their Impacts on Drug Development: A Narrative Review Pharmaceuticals 202316161510.3390/ph 1611161538004480 PMC 10675245 · doi ↗ · pubmed ↗
- 4Bragazzi N.L. Garbarino S. The Complex Interaction Between Sleep-Related Information, Misinformation, and Sleep Health: Call for Comprehensive Research on Sleep Infodemiology and Infoveillance JMIR Infodemiology 20244 e 5774810.2196/5774839475424 PMC 11681283 · doi ↗ · pubmed ↗
- 5Khalifa M. Albadawy M. AI in diagnostic imaging: Revolutionising accuracy and efficiency Comput. Methods Programs Biomed. Update 2024510014610.1016/j.cmpbup.2024.100146 · doi ↗
- 6Anthopoulos L. Karakidi M. Tselios D. Defining the “Smart Hospital”: A Literature Review Springer Berlin/Heidelberg, Germany 2024 Available online: https://link.springer.com/chapter/10.1007/978-3-031-60218-4_15(accessed on 11 February 2026)
- 7Lee A. Taylor P. Kalpathy-Cramer J. Tufail A. Machine learning has arrived!Ophthalmology 20171241726172810.1016/j.ophtha.2017.08.04629157423 · doi ↗ · pubmed ↗
- 8Cascella M. Semeraro F. Montomoli J. Bellini V. Piazza O. Bignami E. The Breakthrough of Large Language Models Release for Medical Applications: 1-Year Timeline and Perspectives J. Med. Syst.2024482210.1007/s 10916-024-02045-338366043 PMC 10873461 · doi ↗ · pubmed ↗