Multimodality Imaging in Cardiac Metastasis of Cutaneous Melanoma: Case Report and Systematic Review
Karina L. Lara-Sampayo, Juan Carlos Ibarrola-Peña, Miranda de la Pena-Tamez, Jose A. Salinas-Casanova, Rafael Garcia, Carlos Jerjes-Sanchez, Jose Gildardo Paredes-Vazquez, Erasmo de la Pena-Almaguer

TL;DR
This paper reports a case of melanoma spreading to the heart and reviews 27 cases to highlight the challenges in diagnosing and managing cardiac metastases from melanoma.
Contribution
The study provides a systematic review and case report emphasizing the role of multimodal imaging in diagnosing cardiac metastases from melanoma.
Findings
Multimodal imaging, including echocardiography and CMR, is critical for diagnosing cardiac metastases in melanoma.
Cardiac metastases from melanoma often affect the left ventricular free wall and interventricular septum.
Early detection and accurate diagnosis are needed to improve outcomes in patients with cardiac metastases from melanoma.
Abstract
Background: Cardiac metastases from cutaneous melanoma are uncommon and often underdiagnosed due to their variable and frequently asymptomatic presentation. To better describe their clinical features, diagnostic strategies, and outcomes, we performed a systematic review of published case reports and present an illustrative clinical case. Case presentation: We report the case of a 67-year-old man with a history of stage IIA cutaneous melanoma who presented with progressive fatigue and dyspnea. Disease recurrence was confirmed by skin biopsy. Multimodal imaging, including echocardiography, FDG PET-CT, and cardiac magnetic resonance (CMR), demonstrated extensive myocardial infiltration consistent with cardiac metastases. Despite treatment with immunotherapy, the patient experienced progressive clinical deterioration and died six months after diagnosis. Discussion: The systematic review…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
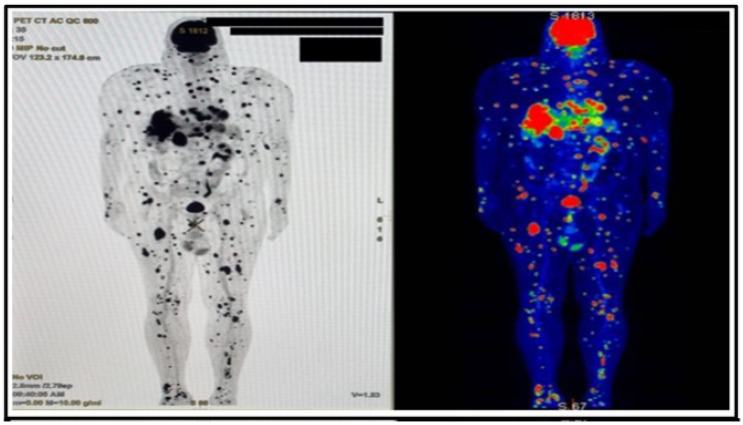 Figure 1
Figure 1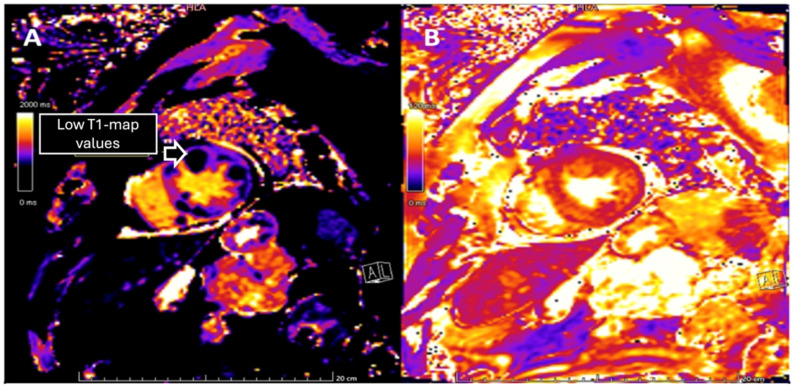 Figure 2
Figure 2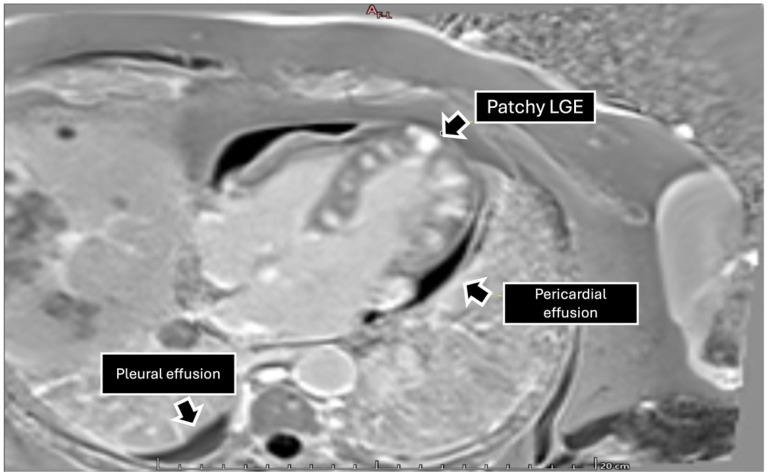 Figure 3
Figure 3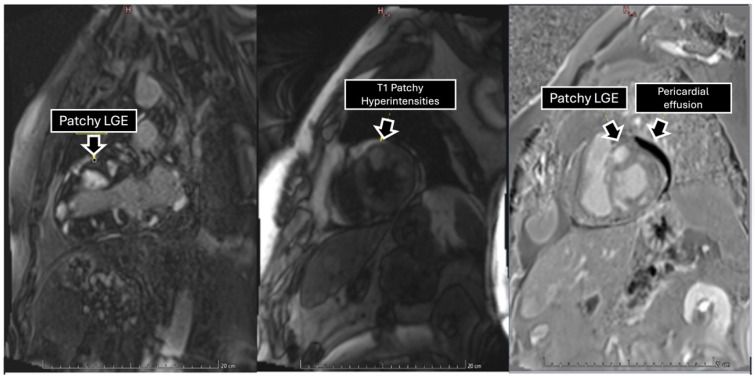 Figure 4
Figure 4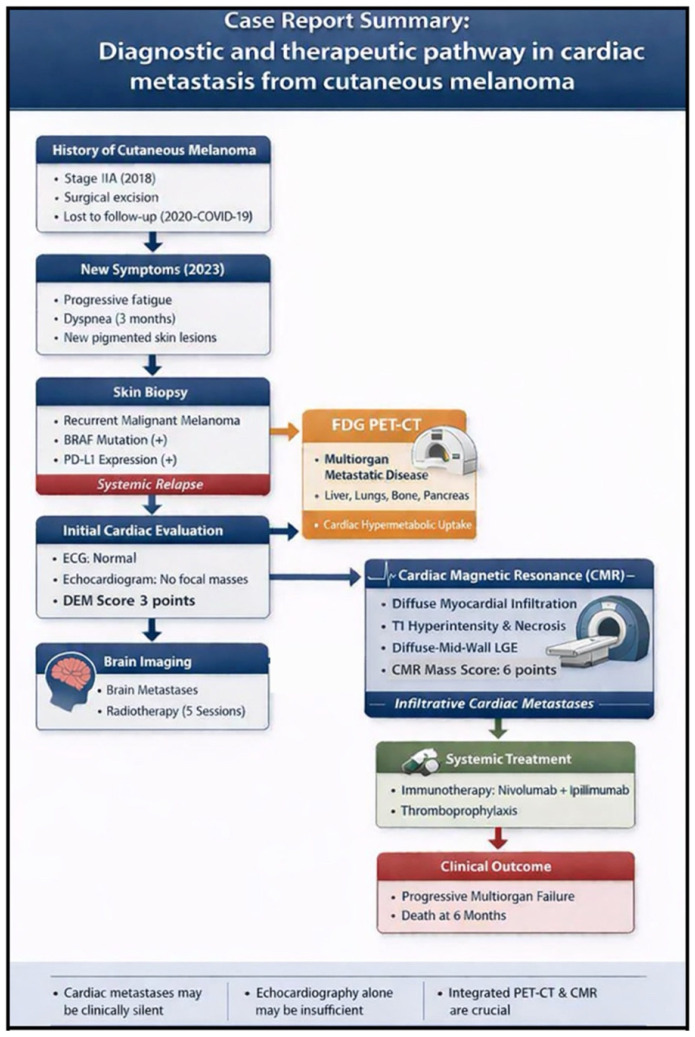 Figure 5
Figure 5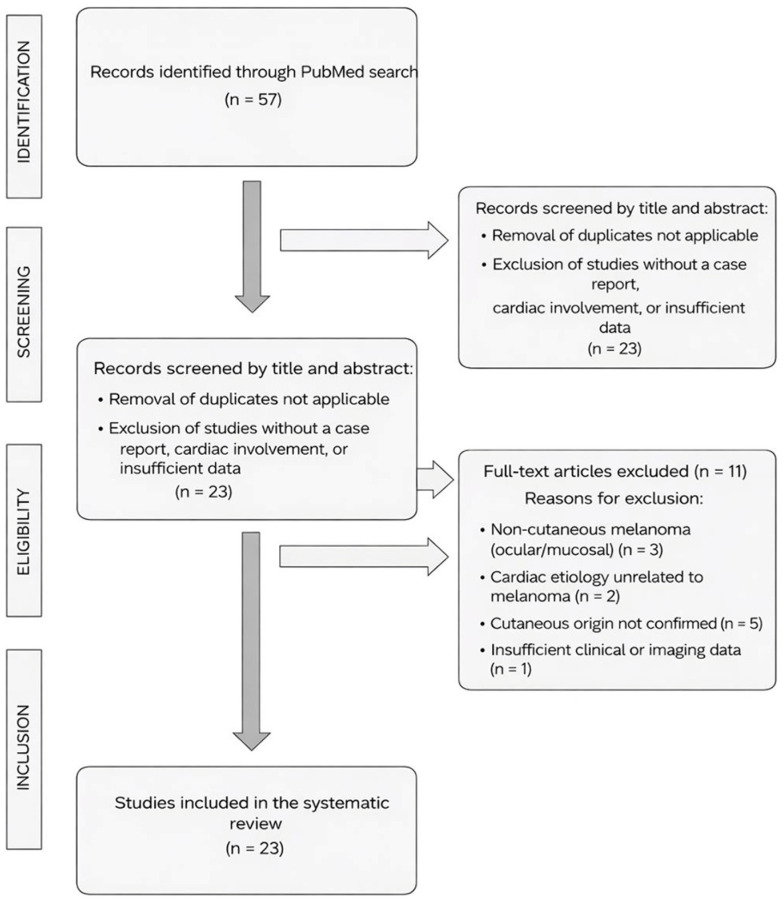 Figure 6
Figure 6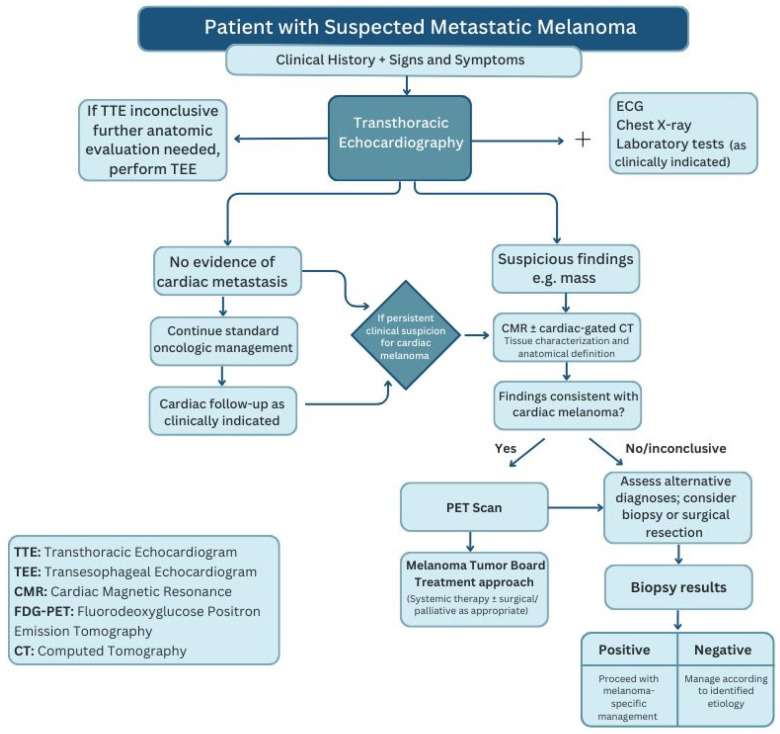 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac tumors and thrombi · Cutaneous Melanoma Detection and Management · Brain Metastases and Treatment
1. Introduction
Cardiac metastases from cutaneous melanoma are relatively common upon autopsy (50–65%) of advanced cases, but they are rarely diagnosed antemortem (<1–2%) [1]. Propensity for wide hematogenous dissemination, attributable to its embryological origin from neural crest cells, explains its ability to invade virtually any organ, including the heart [2]. This often-silent presentation can result in delayed recognition and limit opportunities for early intervention [3]. The most common signs and symptoms are nonspecific, including fatigue, tachycardia, dyspnea, arrhythmias, superior vena cava syndrome, transient ischemic attacks, congestive heart failure, pericardial effusion, edema, and right ventricular inflow or outflow obstruction [4].
Cardiac metastases traditionally signal a poor prognosis, reflecting advanced disease stage. The diagnostic approach to cardiac metastases requires the complementary use of multiple imaging modalities, each providing different but crucial information: echocardiography as an initial accessible tool, cardiovascular magnetic resonance imaging (CMR) for detailed tissue characterization, and a positron emission tomography-computed tomography (PET-CT) to assess the systemic extent of the disease and guide comprehensive treatment [5].
Early and systematic use of a multimodal imaging approach is crucial for the accurate detection of cardiac involvement and the management of these complex cases. We present a case that highlights the aggressive nature of cutaneous melanoma and emphasizes the importance of a comprehensive cardiac evaluation in patients with a known history of this malignancy. Additionally, we conducted a systematic review of the literature. This review aims to identify and analyze published case reports of cardiac metastases secondary to melanoma, with a specific focus on those originating from cutaneous melanoma. The literature search was performed using the PubMed database, applying the following combination of MeSH terms and free-text keywords: (Heart Neoplasms/secondary [MeSH] OR Cardiac metastasis [tiab]) AND (Melanoma [MeSH] OR cutaneous melanoma [tiab]) AND (Echocardiography [MeSH] OR Magnetic Resonance Imaging [MeSH] OR Positron-Emission Tomography [MeSH]) AND (Case Reports [Publication Type] OR case report [tiab]). This search strategy yielded 57 case reports. Each report was reviewed to confirm the cutaneous origin of the primary melanoma and to systematically extract relevant clinical, imaging, therapeutic, and outcome data. These data formed the basis for a comprehensive case-based review and a comparative analysis of the clinical and imaging patterns associated with cardiac metastases in cutaneous melanoma.
2. Case Presentation
A 67-year-old man presented with a three-month history of progressive fatigue and dyspnea. Grayish pigmented lesions were noted on the trunk and perioral region, the largest measuring approximately 1 cm. Past medical history was significant for stage IIA cutaneous melanoma, diagnosed in 2018 and managed with surgical excision without lymphatic involvement. However, follow-up was discontinued in 2020 due to the COVID-19 pandemic. On physical examination, no additional abnormalities were detected.
A skin biopsy from one of the suspicious lesions confirmed recurrent malignant melanoma, with molecular analysis revealing a positive BRAF mutation and PD-L1 expression. Given the symptoms, concern for cardiac metastatic spread prompted further evaluation. An electrocardiogram (ECG) showed no repolarization abnormalities. Transthoracic echocardiography showed mild left atrial enlargement and inferolateral left ventricular hypertrophy, with a mildly heterogeneous infiltrative appearance, which, in the clinical context, was suggestive of an infiltrative process. Biventricular systolic function and regional wall motion were preserved, with mild left ventricular diastolic dysfunction. The DEM score was 3 points, considered suggestive of malignancy; however, no discrete intracardiac mass was identified, and no significant valvular abnormalities were observed [6]. Considering the history of melanoma and the new onset of fatigue and dyspnea, a PET-CT was performed (Figure 1), which demonstrated multiple hypermetabolic lesions in the liver, pancreas, lungs, bones, and subcutaneous/mesenteric fat, as well as suspicious uptake within the heart.
To further characterize the cardiac findings, we performed CMR, which demonstrated concentric left ventricular (LV) hypertrophy and normal global wall motion, with a preserved ejection fraction ≥70%. On T1-weighted sequences, heterogeneous cylindrical hyperintense regions with diffuse, ill-defined margins were observed throughout the LV myocardium, suggesting extensive infiltrative disease (Figure 2). Native T1 mapping revealed focal areas of low signal intensity, consistent with possible necrosis (Figure 3). Additionally, late gadolinium enhancement (LGE) demonstrated focal and diffuse predominantly mid-wall myocardial involvement, with heterogeneous gadolinium uptake in two-chamber and short-axis views, consistent with intramural necrosis and a non-coronary pattern, supporting metastatic infiltration rather than ischemic injury (Figure 4). It should be noted, however, that low native T1 values on CMR are not specific to cardiac melanoma metastases and may also be observed in other myocardial storage diseases, including myocardial iron/hemosiderin deposition and Anderson–Fabry disease [7]. Nevertheless, in the appropriate clinical context, a structured CMR-based assessment may provide incremental diagnostic value. In our patient, the CMR MASS score was 6 points, driven by infiltrative myocardial involvement, a polylobulated mass-like morphology, associated pericardial effusion, and early contrast enhancement. When low native T1 values were integrated with the patient’s oncologic history and systemic disease burden, these findings were consistent with malignant cardiac involvement.
Subsequent imaging identified brain metastases, for which the patient received five sessions of radiotherapy to the head and neck. Combined immunotherapy with nivolumab and ipilimumab was initiated in accordance with standard treatment guidelines. Anticoagulant therapy was not routinely indicated, as the patient had no established indications such as atrial fibrillation or venous thromboembolism; however, given the presence of active malignancy and cardiac involvement, which confer an increased risk of cancer-associated hypercoagulability and thromboembolic events, a Khorana Risk Score for venous thromboembolism of 2 points (intermediate risk) was calculated, and thromboprophylaxis was administered during hospitalization [8]. The patient was followed closely by a multidisciplinary team, with monitoring of both systemic and cardiac disease progression. However, six months later, multiorgan failure developed, resulting in death. A schematic summary of the case is provided in Figure 5.
3. Discussion
Cardiac metastases from cutaneous melanoma represent a rare but clinically significant manifestation of metastatic progression and are associated with substantial morbidity and mortality. This systematic review of the PubMed database, conducted by two independent reviewers with third-reviewer adjudication for discrepancies, included 27 individual cases from 23 published articles (Figure 6). Marked heterogeneity was observed in clinical presentation, timing of recurrence, anatomical distribution of cardiac involvement, and diagnostic approaches. The mean age at diagnosis was 55.9 years, consistent with previously reported series of advanced melanoma, and a male predominance was observed, with approximately two-thirds of cases occurring in men, likely reflecting both biological factors associated with more aggressive disease and behavioral factors such as lower risk awareness, delayed self-detection, and later presentation to medical care in males [9]. A detailed summary of the individual cases is provided in Table 1.
This review included only cases of cutaneous melanoma, excluding non-cutaneous melanomas due to their distinct clinical, biological, and prognostic characteristics [33]. Likewise, due to the methodology used, studies in which it was not possible to determine the classification of melanoma were excluded. Mucosal melanomas, which account for approximately 1% of all melanomas, are typically diagnosed at advanced stages due to their hidden anatomical locations and are not associated with ultraviolet radiation exposure. Furthermore, they exhibit more aggressive behavior, have a poorer prognosis, and are less responsive to standard immunotherapy, necessitating different therapeutic strategies [34,35]. The lack of randomized clinical trials and specific treatment guidelines for these subtypes reinforces the need to analyze them separately.
Echocardiography remains the first-line imaging technique for suspected cardiac masses due to its accessibility, portability, and low cost [36]. It provides valuable information on intracavitary or intramyocardial lesions, pericardial effusions, valvular abnormalities, and indirect signs such as papillary muscle infiltration. However, echocardiographic findings can sometimes be nonspecific, and image quality is operator dependent. In the reviewed cases, more than half showed echocardiographic signs suggestive of masses or tumors, underscoring its role as an initial diagnostic tool. Nonetheless, as noted previously, its findings are often nonspecific and may not confirm metastatic involvement, as demonstrated in our case.
Detecting cardiac metastases requires a robust diagnostic framework due to their variable presentation and frequently asymptomatic course. The implementation of a multimodal imaging strategy that integrates complementary techniques substantially enhances lesion detection and characterization. This approach improves diagnostic accuracy and facilitates more informed treatment planning and timing. The combined use of echocardiography, CT, CMR, and functional imaging enables a more comprehensive assessment of cardiac involvement and extracardiac disease, thereby supporting timely and appropriate therapeutic decision-making. However, among cases evaluated using a multimodal diagnostic approach, survival outcomes remained highly heterogeneous, with both long-term survivors and early mortality reported, precluding definitive conclusions regarding its impact on prognosis.
Cardiac metastases can involve the myocardium thickness, although the epicardium is the most common location. The pericardium and myocardium are commonly involved with multifocal, small lesions [37]. Within the myocardium, the free wall of the left ventricle and the interventricular septum are the most frequently affected regions, a pattern consistent with our clinical case. This predilection is likely related to their greater myocardial mass, rich coronary blood supply, and high perfusion, which facilitate hematogenous tumor cell seeding and infiltration [4]. In contrast, the endocardium is less frequently involved; when affected, it typically results from tumor extension into the cardiac chambers and may produce intracavitary lesions capable of obstructing ventricular outflow. According to current clinical standards, CMR is considered the gold standard for tissue characterization, due to its excellent spatial resolution and versatile pulse sequences. One significant advantage of CMR over other imaging techniques, such as CT, is that it does not involve ionizing radiation, making it a safer option for patients. Additionally, its excellent contrast resolution allows for a more precise assessment of the nature and origin of cardiac and pericardial masses. CMR also excels in providing high-resolution anatomical detail, often clarifying complex anatomical relationships. This detailed imaging capability enables the accurate determination of tumor extent, facilitating more effective surgical or ablative planning [13].
In cutaneous melanoma cases, lesions are commonly hyperintense on T1-weighted images due to melanin’s paramagnetic effects, although amelanotic variants may not follow this pattern [38]. The use of LGE sequences is especially valuable for detecting diffuse infiltration that may not correspond to a coronary artery territory [39]. In our review, over half of the cases included CMR, facilitating improved diagnostic planning and therapeutic decisions. In our patient, CMR provided detailed, personalized clinical insights. These findings highlight the importance of integrating CMR into diagnostic workflows, as it allows for anatomical and tissue characterization that other modalities may overlook.
When there is suspicion of metastatic spread, it becomes crucial to use additional imaging techniques that provide a more comprehensive and detailed assessment. CT is commonly used for both initial staging and follow-up, mainly due to its widespread availability, cost-effectiveness, and reasonable accuracy. In patients with cutaneous melanoma, CT has an overall sensitivity of approximately 58% and a specificity of nearly 70% for identifying metastases. PET-CT has substantially improved diagnostic capabilities in metastatic melanoma [40]. This advanced imaging modality is valuable not only for diagnosis but also for staging and ongoing monitoring. By providing whole-body imaging in a single session, PET-CT enables the detection of metastases throughout the body, including the heart and other organs. A key advantage is its ability to detect metabolic changes before structural abnormalities become evident [41]. Specifically, FDG-PET-CT exhibits superior sensitivity (~98.7%) compared to FDG-PET alone (~88.9%) and CT alone (~69.7%) [42]. Since melanoma metastases avidly uptake the FDG tracer, standardized uptake values (SUVs) assist in differentiating normal cardiac tissue from metastatic lesions, improving diagnostic confidence and guiding treatment planning. Although fewer than 25% of patients in our review underwent PET imaging, most of these demonstrated clinically relevant findings with diagnostic and prognostic value, supporting the expanding role of PET-CT in the evaluation of metastatic cutaneous melanoma.
From a diagnostic standpoint, echocardiography was the most frequently reported imaging modality, used in approximately 80% of cases and typically employed as the first-line diagnostic tool. However, echocardiography alone was often insufficient for comprehensive lesion characterization. Cardiac magnetic resonance imaging emerged as the second most frequently utilized imaging modality, reflecting its key role in tissue characterization and assessment of myocardial and pericardial involvement. In addition, CT and/or FDG PET-CT were used in approximately half of the cases to further delineate tumor extent and evaluate extracardiac disease burden. Notably, nearly two-thirds of patients required a multimodal imaging approach, while only a minority of cases (approximately one-third) had all three imaging modalities—echocardiography, cardiac MRI, and CT/FDG PET-CT—reported.
Multimodality imaging is central to the evaluation of cardiac tumors, while endomyocardial biopsy is reserved for selected cases with inconclusive noninvasive findings. Endomyocardial biopsy is avoided in high-embolization-risk intracardiac masses, but when indicated, image guidance improves its safety and diagnostic yield [43,44,45].
Effective management of metastatic cardiac melanoma necessitates systemic therapy. While surgical resection may alleviate symptoms in isolated cardiac metastases, most patients present with disseminated disease, which is unsuitable for surgery. Conventional chemotherapy shows limited benefit; however, targeted therapies and immune checkpoint inhibitors (e.g., nivolumab and ipilimumab) have improved survival in metastatic melanoma, including cardiac involvement [39]. Available evidence suggests that immunotherapy and chemotherapy demonstrate comparable effectiveness in cardiac metastases to that observed in metastases at other organ sites, with immunotherapy showing concordant response rates and acceptable safety profiles in most patients. Overall survival is influenced by multiple factors, including the stage and biology of the primary malignancy, the presence of additional metastatic sites, the specific site of cardiac involvement, and the efficacy of supportive and palliative measures [46]. The use of palliative radiotherapy in cardiac metastases has been limited due to technical challenges and concerns regarding radiation-induced cardiac toxicity. However, it may be considered in selected cases for symptom control [47]. Early detection, genomic profiling to guide therapeutic prioritization, and personalized multimodal treatment strategies remain critical to optimizing outcomes. Ongoing research into novel immunotherapies holds promise for future advances.
Survival outcomes across the reported cases were highly heterogeneous, likely reflecting both the aggressive biological behavior of metastatic melanoma and the variability inherent to case-based reports. Among the 27 cases included, 11 patients were reported to have died, 6 were alive at last follow-up, and survival status was not reported in 10 cases, highlighting the substantial degree of incomplete outcome reporting in the literature. To reduce the potential for outcome overestimation and misclassification bias, only cases with explicitly reported vital status were included in survival assessments. Within this subset (n = 17), the mortality rate was 62.9%, underscoring the generally poor prognosis associated with cardiac involvement by melanoma. Most reported deaths occurred within a short period following diagnosis, often within weeks to months, whereas longer survival was observed primarily in selected patients who underwent surgical resection combined with systemic therapy.
Our systematic review revealed a frequent lack of coordinated imaging protocols in reported cases, in contrast to the comprehensive workup conducted in our patient. Our evaluation included a focused physical exam for cutaneous recurrence and active screening for cardiovascular symptoms. ECG showed no repolarization abnormalities, followed by transthoracic echocardiography, PET/CT, and CMR, collectively providing precise delineation of disease extent. This structured, stepwise approach, summarized in Figure 7, contrasts with many reports in which some imaging modalities are omitted.
Although intracardiac masses are often documented with echocardiography, CT, or CMR, few studies employ an integrated imaging strategy that enables a comprehensive diagnostic evaluation. Additionally, key clinical variables—such as ECG findings, the interval between primary melanoma and cardiac metastasis, cardiovascular symptoms, treatment approaches, and patient outcomes—are inconsistently reported, limiting meaningful clinical interpretation. In our review, fewer than 25% of cases described multimodal imaging, including echocardiography, CMR, and CT/PET integration. Even in these, clinical progression and outcomes were variably documented, with most cases reporting fatal outcomes at publication. These observations highlight the importance of standardized, detailed reporting in future studies to improve diagnostic accuracy and inform clinical decision-making.
Interpretation of outcome data is inherently constrained by limitations intrinsic to the available literature, including retrospective, case-based reporting, short and heterogeneous follow-up durations, and incomplete documentation of clinical course and survival outcomes. These limitations restrict the ability to draw definitive conclusions regarding prognosis and necessitate cautious interpretation of the findings. Future studies would benefit from more standardized and comprehensive reporting of diagnostic pathways, imaging strategies, follow-up duration, and survival outcomes to improve the quality and comparability of evidence related to cardiac involvement in melanoma. In this context, the present case illustrates how a structured multimodal diagnostic approach can support detailed characterization of cardiac involvement and provide a comprehensive descriptive framework to inform clinical assessment in similar cases.
4. New Challenges Arise
Diagnosing intracavitary cardiac tumors remains a clinical challenge, particularly in melanoma patients, where cardiac metastases are both rare and often clinically silent. This reality demands a high index of suspicion, even in the absence of overt cardiovascular symptoms. Early implementation of integrated imaging techniques—combining structural, functional, and metabolic assessments—is crucial not only for accurate diagnosis but also for timely therapeutic planning. As systemic therapies evolve, especially with the emergence of immune checkpoint inhibitors, the landscape of treatment for metastatic melanoma continues to shift. Nevertheless, the prognosis for patients with cardiac involvement remains poor, highlighting the need for earlier detection strategies and robust follow-up protocols for high-risk populations [48].
5. Considerations
This case illustrates the aggressive nature of metastatic melanoma and emphasizes the necessity of detailed cardiovascular evaluation in patients with this malignancy. Utilizing an integrated imaging approach—particularly with CMR and PET-CT—enables precise lesion characterization and staging, both essential for informed clinical decisions. While CMR excels in tissue differentiation, PET-CT provides vital insights into systemic disease burden.
Despite advances in immunotherapy improving outcomes for some patients, many still present with advanced disease, limiting curative options. Early detection and multidisciplinary, individualized management are crucial for improving prognosis in this challenging population. Future efforts should focus on risk-adapted surveillance and the integration of emerging imaging biomarkers to enable earlier diagnosis and intervention.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bortolotti U. Tursi V. Milano A. Mazzucco A. Gallucci V. Intracardiac metastatic melanoma: Report of a case mimicking a right atrial myxoma, with a review of the literature Tex. Heart Inst. J.19901713615227400 PMC 326472 · pubmed ↗
- 2Rastrelli M. Tropea S. Rossi C.R. Alaibac M. Melanoma: Epidemiology, Risk Factors, Pathogenesis, Diagnosis and Classification In Vivo 2014281005101125398793 · pubmed ↗
- 3Goodall J. Beveridge N.E.R. Rasoul D. Bhamidipati K.R. Metastatic melanoma to the heart causing ventricular tachycardia: Looking beyond the troponin BMJ Case Rep.202215 e 24765810.1136/bcr-2021-247658 PMC 913419835613832 · doi ↗ · pubmed ↗
- 4Tesolin M. Lapierre C. Oligny L. Bigras J.-L. Champagne M. Cardiac Metastases from Melanoma Radio Graphics 20052524925310.1148/rg.25104505915653599 · doi ↗ · pubmed ↗
- 5Goldberg A.D. Blankstein R. Padera R.F. Tumors Metastatic to the Heart Circulation 20131281790179410.1161/CIRCULATIONAHA.112.00079024126323 · doi ↗ · pubmed ↗
- 6Paolisso P. Bergamaschi L. Angeli F. Belmonte M. FoàA. Canton L. Fedele D. Armillotta M. Sansonetti A. Bodega F. Cardiac Magnetic Resonance to Predict Cardiac Mass Malignancy: The CMR Mass Score Circ. Cardiovasc. Imaging 202417 e 01611510.1161/CIRCIMAGING.123.01611538502734 PMC 10949976 · doi ↗ · pubmed ↗
- 7Kottam A. Hanneman K. Schenone A. Daubert M.A. Sidhu G.D. Gropler R.J. Garcia M.J. on behalf of the American Heart Association Council on Cardiovascular Radiology and Intervention State-of-the-Art Imaging of Infiltrative Cardiomyopathies: A Scientific Statement From the American Heart Association Circ. Cardiovasc. Imaging 202316 E 934E 95110.1161/HCI.000000000000008137916407 · doi ↗ · pubmed ↗
- 8Chang H.-M. Okwuosa T.M. Scarabelli T. Moudgil R. Yeh E.T.H. Cardiovascular Complications of Cancer Therapy J. Am. Coll. Cardiol.2017702552256510.1016/j.jacc.2017.09.109529145955 PMC 5825188 · doi ↗ · pubmed ↗