Understanding the Association Between Substance Use and Loneliness in Midlife and Older Adults
Hermine Poghosyan, Jennifer McIntosh, Sayantani Sarkar, S. Raquel Ramos, Ophelia Empleo-Frazier, Nicole Colline, Shelli L. Feder

TL;DR
This study finds a link between substance use and loneliness in adults aged 50 and older, highlighting the need for targeted public health strategies.
Contribution
The study provides new evidence of a statistically significant association between substance use and increased loneliness in midlife and older adults.
Findings
Substance users had a 17% higher risk of feeling lonely always/usually compared to non-users.
The association remained significant after adjusting for covariates like age, sex, and health status.
Abstract
Public health relevance—How does this work relate to a public health issue? Loneliness is a growing public health concern and is highly prevalent among adults aged ≥50 years.Substance use is a significant public health burden, as it places individuals at increased risk for morbidity and mortality. Loneliness is a growing public health concern and is highly prevalent among adults aged ≥50 years. Substance use is a significant public health burden, as it places individuals at increased risk for morbidity and mortality. Public health significance—Why is this work of significance to public health? Substance use and loneliness are increasing among adults aged ≥50 years, posing a growing public health burden.Understanding the link between substance use and loneliness can inform targeted prevention and early-intervention strategies for adults aged ≥50 years. Substance use and loneliness…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
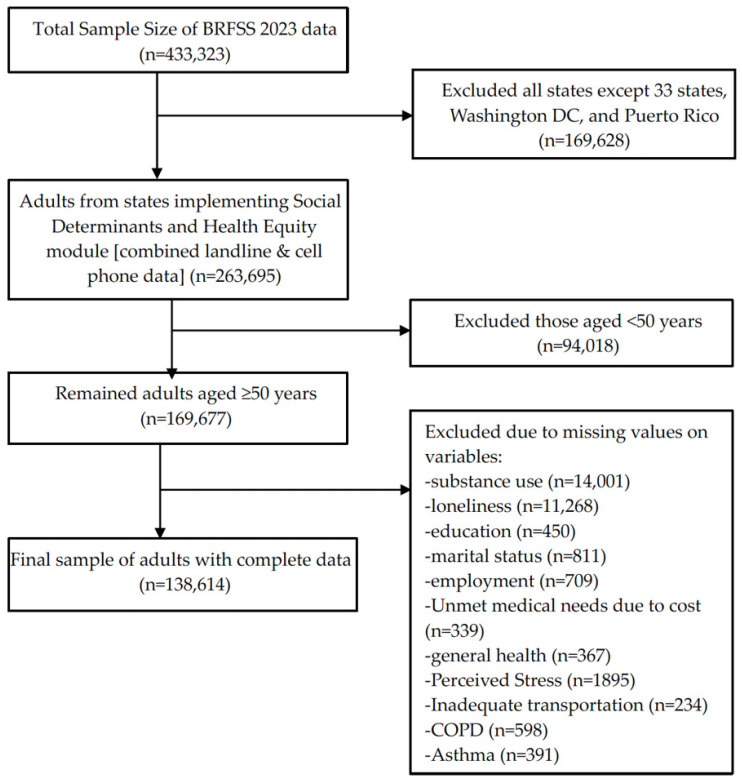 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealth disparities and outcomes · Substance Abuse Treatment and Outcomes · Employment and Welfare Studies
1. Introduction
Loneliness and social isolation have emerged as pressing public health crises due to their profound impact on mental, emotional, and physical well-being [1,2,3]. Loneliness is a complex emotional state characterized by feelings of isolation and disconnection with a perceived discrepancy between an individual’s desired and actual social connections [1,4]. Conversely, social isolation refers to the objective condition of having minimal social relationships, roles, and interactions [5,6]. According to the World Health Organization, approximately 16.0% of people, one in six, experience loneliness globally, including 11.8% of older adults [7].
In the U.S., approximately 50.0% of the population reports experiencing loneliness, including about 34.0% of adults aged ≥50 years [8]. Loneliness has been identified as a significant risk factor for various mental and physical health problems [1,9]. Research suggests that experiencing chronic loneliness can be as harmful to health as smoking 15 cigarettes per day [1,10]. In fact, when people experience loneliness, they have a 26% higher risk of premature death [11,12]. The prevalence of loneliness, its risk factors, and consequences differ between age groups [13,14]. Previous work has shown that loneliness follows a U-shaped distribution, with peaks in late adolescence, young adulthood, and older adults [14,15]. Older adults are particularly vulnerable due to loss of close relationships, role changes, cognitive and physical decline, and impaired health status [1,16]. Moreover, loneliness among this group is particularly concerning due to its strong association with poor physical and mental health outcomes, such as cardiovascular disease, depression, anxiety, and increased mortality risk [1,17].
Substance use may exacerbate feelings of loneliness by disrupting relationships, weakening social support, and reducing social engagement. The relationship between substance use and loneliness among midlife and older adults is complex and may be influenced by various life stages and transitions. Middle to late adulthood, spanning ages 40 to 65, is a critical period during which individuals often juggle multiple roles in family, community, and work [18]. This stage, at times referred to as the “sandwich generation,” may be marked by stressors related to intergenerational dynamics, such as parenting older children, supporting grandchildren, and caring for aging parents while navigating work demands. These experiences can create significant emotional, financial, and time management strains. Studies have shown increased rates of anxiety, depression, and serious psychological distress among this group, particularly among individuals of lower socioeconomic status, women, and those identifying as lesbian, gay, bisexual, and transgender LGBTQ [19,20]; rates of antidepressant use are also higher among midlife individuals [21]. It is possible that during this period, the pressures and demands may contribute to varying levels of substance use and loneliness as individuals strive to manage these multifaceted roles.
Post-retirement, typically ages 66 to 89, is often a time when individuals may focus more on personal goals related to social relationships, as they are relieved of work- and family-related responsibilities [22]. As individuals age, relationship satisfaction tends to increase, despite a tendency for social networks to decrease [23]. However, retirement may also have negative consequences for health and well-being, potentially contributing to substance use and feelings of loneliness.
Reaching very old age, defined as 90 years and older, shifts the focus towards maintaining physical and cognitive functioning and striving for independence [22]. This stage is marked by declining capacities, increased awareness of the aging process’s irreversibility, and changes in family dynamics [24]. The transition into very old age is also marked by the sensation of progressive social exclusion associated with the loss of contemporaries or a spouse, challenges in connecting with younger generations, and a lack of meaningful community relationships [24]. These factors can lead to heightened feelings of loneliness and may influence substance use patterns as individuals navigate the realities of advanced age.
Moreover, adults aged ≥50 years are generally more vulnerable to the adverse effects of substance use, as age-related physiological changes such as slower metabolism, increased sensitivity, and other aging processes may predispose them to adverse health consequences [25,26,27,28]. Although cigarette use has declined significantly over the past decades, approximately 12.0% of adults aged ≥50 years still report current cigarette use, posing ongoing health risks in this vulnerable group [29]. Furthermore, about 10% of this age group of adults report binge alcohol drinking [29].The use of substances is often employed as a mechanism to suppress the feelings of loneliness and associated emotional distress [30]. Existing evidence has also found that the perceived feelings of loneliness can be influenced by several socio-demographic factors, such as race or ethnicity, educational level, and healthcare access. Similarly, substance use behaviors also vary widely by racial identity, educational level, sexual and gender identity, and other socio-demographic factors [9,31,32,33,34]. While substance use is well studied in the general population [35], its association with loneliness, particularly among this growing population of adults aged ≥50 years, remains inadequately studied, leaving a critical gap in understanding this association in mid and later life. Thus, this study estimated the prevalence of substance use (i.e., binge alcohol, e-cigarette, and traditional cigarette use) and loneliness among adults aged ≥50 residing in the US. Additionally, it examined the associations between substance use and self-reported loneliness among this population. By exploring these relationships, this study contributes to the expanding body of literature on aging, emotional well-being, and behavioral health, to inform both clinical practice and public health policy.
2. Materials and Methods
2.1. Data Source
This study used secondary cross-sectional data from the 2023 Behavioral Risk Factor Surveillance System (BRFSS), Social Determinants and Health Equity (SDHE) optional module [36]. The BRFSS is a nationally recognized, population-based survey designed to collect data from noninstitutionalized adults aged ≥18 across the US. Administered annually, BRFSS employs a standardized questionnaire composed of three components: a core set of questions administered by all states, optional modules that cover specific public health topics are administered by some states and state-added questions tailored to local needs. The survey collects data on socio-demographics, health-related risk behaviors, chronic health conditions, perceived health status, and access to healthcare services, among others. The total sample size for the 2023 BRFSS was 433,323, and the response rate was 44.7% [36].
2.2. Study Population
The data for the current study comes from the Districts of Columbia, 33 US states (Alabama, Alaska, Arizona, Arkansas, California, Connecticut, Delaware, Georgia, Hawaii, Idaho, Illinois, Indiana, Iowa, Kansas, Louisiana, Maine, Massachusetts, Minnesota, Mississippi, Missouri, Montana, Nevada, New Hampshire, New Jersey, New Mexico, North Carolina, North Dakota, Rhode Island, South Carolina, Utah, Virginia, West Virginia, Wisconsin) and one US territory (Puerto Rico) that administered the SDHE module in their 2023 BRFSS survey [36]. After excluding respondents from states that did not administer the SDHE module (n = 169,628) and individuals younger than 50 years (n = 94,018), the sample included 169,677 adults aged ≥50 years residing in selected US states and one territory. We further excluded observations with responses of “refused” or “don’t know/not sure,” or with missing values in the outcome, key predictor variables, or covariates. The final analytic sample included 138,614 adults aged ≥50 years. Figure 1 shows details of this study sample.
2.3. Study Variables
The primary outcome, loneliness, was measured using a single-item question from the SDHE module. Participants were asked, “How often do you feel lonely? with five response options: “always”, “usually”, “sometimes”, “rarely”, and “never”. This item measured the frequency of subjective feelings of loneliness. For the current study, responses were recoded into three categories reflecting increasing levels of loneliness frequency: (0) rarely/never, (1) sometimes, and (2) always/usually. This single-item measure of loneliness has also been used in previous research as a valid indicator of perceived loneliness [37,38].
The key predictor was self-reported substance use, which included current use of traditional cigarettes, electronic cigarettes, and binge alcohol drinking. Current traditional cigarette use was defined as having smoked at least 100 cigarettes in one’s lifetime and currently reported cigarette use every day or some days. Respondents who reported using at least 100 traditional cigarettes in their lifetime but reported no current use (former) and those who reported fewer than 100 traditional cigarettes in their entire lifetime (never) [39] are combined together for our study. This recategorization is done based on the prior published literature [40].
Current electronic cigarette use was defined as those reported using e-cigarettes every day or on some days, and individuals who reported never having used e-cigarettes and not currently using them were classified as the non-user group. Binge drinking was defined as consuming five or more alcohol drinks on a single occasion for males and four or more for females [41]. We combined these three behaviors into a binary substance use variable: (0) no substance use (participants who reported no current use of traditional cigarettes, e-cigarettes, or binge drinking), and (1) substance use (participants who reported current use of at least one of the three substances) [42].
We included a comprehensive set of covariates to adjust for potential confounding in the relationship between substance use and loneliness. Sociodemographic covariates included age (50–64, 65–74, 75–79, 80+), race and ethnicity (non-Hispanic Asian, non-Hispanic Black, Hispanic, non-Hispanic White, other race and ethnicity), sex (male, female) marital status (never married, divorced/separated, married or part of unmarried couple, widowed), education level (high school graduate or less, some college or technical school, college graduate), and employment status (employed, retired, not in a workforce). We also included variables for unmet medical needs and lack of reliable transportation. Unmet medical need (yes, no) was measured by asking participants the following question: “Was there a time in the past 12 months when you needed to see a doctor but could not because you could not afford it?” with yes/no responses. The lack of reliable transportation (yes, no) was assessed by the following question “During the past 12 months has a lack of reliable transportation kept you from medical appointments, meetings, work, or from getting things needed for daily living?”. Health-related covariates included self-reported general health status (fair/poor health, vs. good/very good/excellent health), history of asthma (yes, no), history of chronic obstructive pulmonary disease, emphysema, or chronic bronchitis (yes, no), and perceived stress. Perceived stress was measured with the following item “Stress means a situation in which a person feels tense, restless, nervous, or anxious, or is unable to sleep at night because his/her mind is troubled all the time. Within the last 30 days, how often have you felt this kind of stress?” Consistent with BRFSS, we recategorized it as a binary variable with the following categories: yes (always/usually) and no (rarely/never/sometimes) [43].
2.4. Statistical Analysis
We applied recommended sampling weights to account for the complex survey design of the BRFSS and to produce nationally representative population estimates. The BRFSS weighting process includes two key steps: (1) design weighting, which corrects for unequal probabilities of participant selection, and (2) iterative proportion fitting (ranking), which aligns the sample distribution with known population benchmarks. Ranking adjusts for potential nonresponse and sampling biases using demographic variables, including sex, age, race, Hispanic ethnicity, marital status, education, homeownership, phone ownership, and geographic region [36].
First, we conducted descriptive analyses to describe the study sample characteristics, presenting frequencies and weighted percentages along with their corresponding 95% confidence intervals (CI) for all study variables. We used chi-square tests, with Wald statistics, to estimate the prevalence of substance use and loneliness across sample characteristics. To examine the association between substance use and loneliness, we conducted a weighted multivariable multinomial logistic regression analysis. In this model, loneliness was treated as a three-category outcome variable, with ‘rarely/never’ serving as the reference category and comparisons made to both ‘sometimes’ and ‘always/usually’ categories. The model was adjusted for all covariates to control for potential confounding factors. Results are presented as Relative Risk Ratios (RRR) with 95% CIs for each independent variable. All analyses accounted for the complex survey design of the BRFSS using the ‘svy’ command in STATA 18 (StataCorp LLC, College Station, TX, USA). Statistical significance was assessed using two-tailed p-values, with a threshold of <0.05 considered statistically significant.
3. Results
3.1. Sample Characteristics
The sample included 138,614 adults aged ≥50 years, representing approximately 55.4 million individuals in this age group residing in the included US states and one territory. Sample characteristics are presented in Table 1. Overall, 67.3% of participants self-identified as non-Hispanic White, 12.8% as Hispanic, 10.9% as non-Hispanic Black, and 5.0% as Asian. Just over half (50.5%) were aged 50–64, and 54.0% were women. About 35.6% had high school or lower level of education, and 16.0% were not in the workforce. About 6.0% reported unmet medical needs due to cost, and 5.2% reported inadequate transportation in the past 12 months. Overall, 24.0% reported their general health as fair or poor, 9.0% reported experiencing perceived stress, 9.8% reported having lung disease, and 13.8% reported having asthma (Table 1).
3.2. Substance Use and Loneliness
Of study participants, 19.0% reported ≥1 substance use, with 10.9% reporting traditional cigarette use, 8.9% binge drinking, and 2.1% e-cigarette use. Overall, 21.0% reported feeling lonely sometimes, and 5.1% reported feeling lonely always/usually (Table 2).
Table 3 presents the prevalence of loneliness by sample characteristics. Felling lonely always/usually was most prevalent among the younger group (aged 50–64 years), Hispanic individuals, divorced adults, those with a high school education or less, not in the workforce, those who experienced medical unmet need, had a lack of reliable transportation, and reported perceived stress.
Table 4 presents the prevalence of substance use by sample characteristics. Among those who reported the use of ≥1 substance, 8.0% reported feeling lonely always/usually, and 24.0% feeling lonely sometimes, compared to 4.4% and 20.2% among nonusers, respectively. Substance use was more prevalent among younger adults (aged 50–64 years), non-Hispanic white individuals, men, divorced/separated individuals, and those with a lower education level.
3.3. Association Between Substance Use and Loneliness
Table 5 presents results from the adjusted multivariable multinomial logistic regression analysis. Adults aged ≥50 years who reported the use of ≥1 substance had 17.0% higher relative risk of reporting feeling lonely always/usually (compared to feeling never/rarely lonely) than adults who did not report substance use, after adjusting for all covariates (RRR 1.17; 95% CI 1.10–1.35; p = 0.029). Similarly, adults who reported ≥1 substance use had 10.0% higher risk of reporting feeling lonely sometimes (compared to feeling lonely never/rarely) than those not using substances, controlled for all covariates (RRR 1.10; 95% CI 1.01–1.20; p = 0.021).
4. Discussion
Our study findings demonstrated that substance use was associated with loneliness among midlife and older adults aged ≥50 years. These findings are consistent with prior literature suggesting that individuals who use substances such as alcohol and cannabis are more likely to report feeling lonely, compared to those who do not use such substances [44,45]. A study conducted with students found that substance use behaviors, such as binge drinking, nicotine vaping, and cannabis use, may significantly increase the risk of loneliness [46]. Another study showed that cigarette smoking can heighten loneliness [47]. These findings underscore the importance of substance use as a correlate of loneliness, warranting further investigation in the midlife and older adult population.
In our study of adults aged ≥50 years, we found that the prevalence of loneliness (sometimes/usually/always) was approximately 26%. A very recent study published with a much older age group (≥65) found a comparatively lower prevalence of loneliness (11.6%) [48]. These differing findings may be due to age differences and life stages of individuals in the study samples, particularly the inclusion of a comparatively younger age group (50–64 years old) in our sample. It is essential to note that these results may also be influenced by the life stages and transitions experienced by this age group. For instance, individuals at this stage often navigate multiple roles across family, community, and work [18]. This period may be characterized by the stressors of being in a “sandwich generation” with intergenerational dynamics, such as parenting older children, supporting grandchildren, and caring for aging parents, all while managing the demands of employment. Additionally, individuals in this cohort may be preparing for retirement, experiencing widowhood, and facing the changes associated with their children moving out, leading to “empty nest” situations.
Moreover, the literature suggests that loneliness is significantly associated with various negative health outcomes and medication use among older adults [11,49]. For instance, individuals who felt lonely were more likely to use antidepressants (27.0%) and benzodiazepines (11.0%) [49]. Furthermore, when individuals experience loneliness, they have a 26% higher risk for premature death [11]. In aggregate, these findings highlight the importance of comprehensive approaches to support the health and well-being of these individuals. Healthcare providers should routinely screen this group of individuals for loneliness, in addition to screening for substance use. Our findings suggested that substance use remains a significant concern in this aging population, with 19.0% of participants reporting the use of ≥1 substance. This is alarming as substance use places these individuals at increased risk for morbidity and mortality, while also complicating the management of chronic diseases that are highly prevalent in this age group such as cardiovascular disease, cancer, and diabetes [50,51,52]. Implementing tailored intervention programs to effectively reduce the burden of substance use among adult populations is urgently needed.
Our study findings showed that among the sample, some groups were more likely to report loneliness than others. For example, among racial and ethnic groups, loneliness was most prevalent among Hispanic individuals compared to their non-Hispanic white counterparts. A study conducted by Tibirica and colleagues (2022) investigated loneliness among Hispanic/Latinx men aged 50–68 years in the US and similarly reported higher levels of loneliness in this group compared to non-Hispanic individuals [53]. One potential explanation might be differences in social and structural factors that may contribute to increased loneliness among Hispanic individuals, such as language barriers, under-resourced community dwellings, and a lack of social support, underscoring the need for culturally responsive strategies and interventions to address loneliness. We also found that women were less likely than men to experience loneliness. However, evidence regarding sex differences in loneliness presents mixed results. Nicolaisen & Thorsen (2024) examined gender differences in loneliness over a 15-year time frame and found that older women, aged 60–80 years, experienced elevated levels of loneliness compared to men [54]. In contrast, a meta-analysis conducted by Maes et al. (2019) reported that men were slightly lonelier than women [55]. Similar findings have been observed in another study [56]. Future research is needed to clarify gender and sex differences associated with loneliness among midlife and older adults.
Several psychosocial and structural factors were also significantly associated with loneliness among our sample. Participants who experienced perceived stress during the past 30 days had 182% increased risk of feeling lonely. Stress, characterized by feelings of tension, anxiety, and restlessness, often accompanied by sleep disturbances, has been shown to intensify loneliness and may also increase vulnerability to substance use [57,58]. Those in the sample who lacked reliable transportation, which kept them from going to medical appointments, meetings, or work, had a 134% increased risk of reporting feeling lonely usually/always. Research conducted by Henning-Smith (2020) revealed that inadequate access to affordable and reliable transportation limits older adults’ ability to engage in community activities, attend medical appointments, and maintain social ties [59,60]. Our study findings highlight the importance of implementing interventions that address social determinants of health, demographic factors, and routine screening for substance use and loneliness among adult populations.
A notable strength of this study was the use of large nationally representative population-based data drawn from the 33 US states and one US territory that have contributed to the SDHE optional module. The relationship between loneliness and substance use is nuanced for aging populations. However, this study is not without limitations. Despite the large sample size, this study may not be generalizable to all US adults aged ≥50 years, as it did not include samples from all states, nor did all states administer the SDHE optional module of the BRFSS. All variables included in the study were self-reported and thus are at risk of response, recall, and social desirability bias. The cross-sectional design of the current study prevents establishing the causal relationship between substance use and loneliness. The temporality of the analysis may not adequately capture social issues affecting the aging population. Unequal group sizes for the substance use variable may have reduced statistical power and increased the risk of Type II error. Therefore, these findings should be interpreted with caution, and future research should aim for more balanced group sizes to facilitate replication. Loneliness in this study is measured with a single-item question that reflects its frequency, not its magnitude or severity. In addition, loneliness is a complex, self-perceived feeling that may arise due to multiple factors or a combination of such factors, such as limited social network, lack of closeness or poor relationship quality, lack of sense of belongingness in the social network, living arrangements, poor self-perceived health, and mental conditions such as depression [61]. Our study also did not include variables that may influence self-reported loneliness, such as an individual’s social network. Furthermore, our study has also investigated substance use as a binary variable, limiting the frequency, type, and extent of substance use that may influence the perception of loneliness. Future investigations should include a more thorough set of variables and validated loneliness scales to investigate the relationship between substance use and loneliness. Understanding contributing factors of loneliness in this growing population can guide primary prevention strategies and early treatment plans, delay long-term health effects, and thus decrease morbidity and mortality associated with loneliness.
5. Conclusions
Substance use is common among midlife and older adults and is associated with a higher likelihood of loneliness. Study findings highlight the emergent need for healthcare providers to integrate substance use and loneliness screening into routine clinical practice, particularly among adults aged ≥50. Our findings also emphasize the need to implement evidence-based interventions that address loneliness to mitigate the adverse effects of substance use and loneliness.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1U.S. Department of Health and Human Services Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community 2023 Available online: https://www.hhs.gov/sites/default/files/surgeon-general-social-connection-advisory.pdf(accessed on 15 February 2025)37792968 · pubmed ↗
- 2Zeas-Siguenza A. Ruisoto P. Koldewyn K. Muntane F. Benach J. Beyond clinical risk: Tackling loneliness through a population health lens Front. Psychol.202516160906010.3389/fpsyg.2025.160906040900956 PMC 12400030 · doi ↗ · pubmed ↗
- 3Zeas-Siguenza A. Voldstad A. Ruisoto P. Ganho-Avila A. Guiomar R. Cacho R. Muntane F. Benach J. Loneliness as a Public Health Challenge: A Systematic Review and Meta-Analysis to Inform Policy and Practice Eur. J. Investig. Health Psychol. Educ.20251513110.3390/ejihpe 1507013140709964 PMC 12293955 · doi ↗ · pubmed ↗
- 4Prohaska T. Burholt V. Burns A. Golden J. Hawkley L. Lawlor B. Leavey G. Lubben J. Perissinotto C. van Tilburg T. Consensus statement: Loneliness in older adults, the 21st century social determinant of health?BMJ Open 202010 e 03496710.1136/bmjopen-2019-03496732788184 PMC 7422633 · doi ↗ · pubmed ↗
- 5Badcock J. Holt-Lunstad J. Garcia E. Bombaci P. Lim M. Position Statement: Addressing Social Isolation and Loneliness and the Power of Human Connection Global Initiative on Loneliness and Connection (GILC)Washington, DC, USA 2022143 Available online: https://www.gilc.global/_files/ugd/410bdf_74fffc 2d 18984 b 0e 8217288 b 1b 12d 199.pdf(accessed on 10 October 2025)
- 6Holt-Lunstad J. Steptoe A. Social isolation: An underappreciated determinant of physical health Curr. Opin. Psychol.20224323223710.1016/j.copsyc.2021.07.01234438331 · doi ↗ · pubmed ↗
- 7World Health Organization [WHO] Reducing Social Isolation and Loneliness Among Older People 2025 Available online: https://www.who.int/activities/reducing-social-isolation-and-loneliness-among-older-people(accessed on 6 October 2025)
- 8Malani P. Singer D. Kirch M. Solway E. Roberts S. Smith E. Hutchens L. Kullgren J. Trends in Loneliness Among Older Adults from 2018–2023 (University of Michigan National Poll on Healthy Aging, March 2023)University of Michigan Ann Arbor, MI, USA 202310.7302/7011 · doi ↗