Mentoring in Hospital Settings: A Systematic Review of Guidance, Care, and Professional Development
Giuliana Ventimiglia, Ilaria Setti, Marina Maffoni

TL;DR
This review finds that mentoring by senior healthcare professionals helps junior workers develop skills, confidence, and well-being, though challenges like standardization remain.
Contribution
A systematic review of mentoring in healthcare, emphasizing its impact on professional development and identifying gaps in equitable access and standardized models.
Findings
Mentoring improves clinical and transversal skills like communication and problem-solving.
Mentees experience enhanced self-efficacy, resilience, and autonomy during challenging periods.
Standardized mentoring models and inclusive environments are needed to maximize benefits.
Abstract
Background/Objectives: Mentoring is defined as a supportive relationship between an experienced professional (mentor) and a less experienced individual (mentee), influencing skill development, professional confidence, and psychological well-being. This systematic review addresses the question: “Can support from a senior colleague positively impact junior healthcare workers?” Methods: Following PRISMA 2020 guidelines, a systematic literature search was performed (January 2004–December 2024) in Web of Science, PubMed, and Scopus databases, yielding 399 studies. Results: After rigorous screening and quality assessment using the QuADS checklist, 74 studies were included in the final analysis. The reviewed articles span various healthcare fields, including nursing, medicine, and midwifery, utilizing qualitative, quantitative, observational, and mixed-methods approaches. Key findings…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
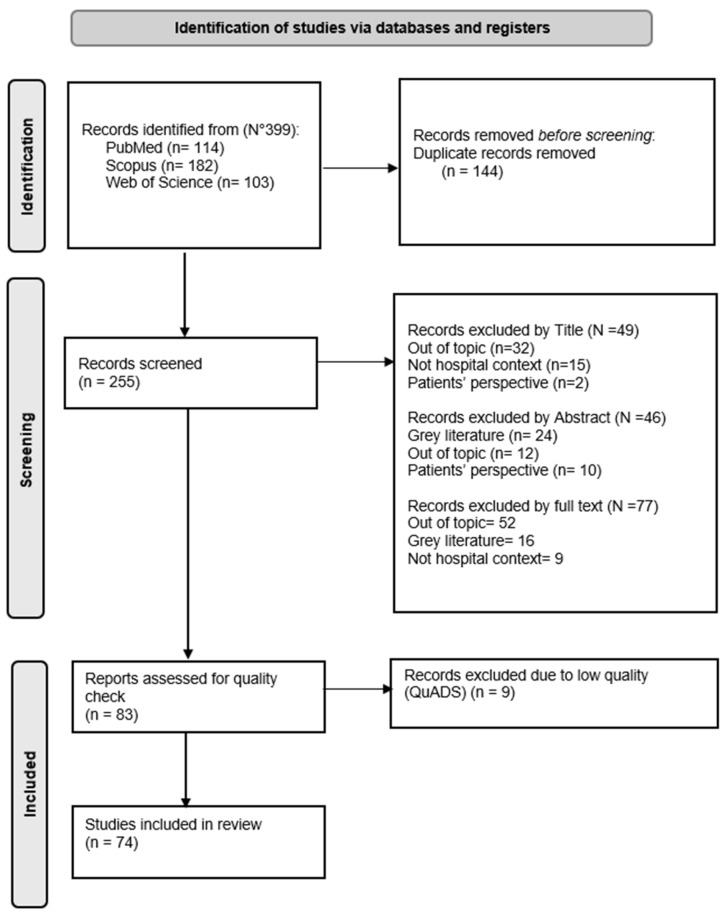 Figure 1
Figure 1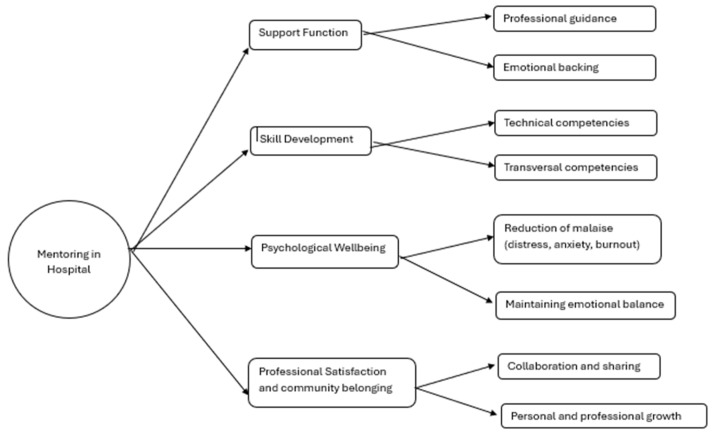 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMentoring and Academic Development · Nursing education and management · Healthcare professionals’ stress and burnout
1. Introduction
Mentoring, defined as a dynamic relationship whereby a more experienced and competent individual (mentor) actively supports the development of a less experienced person (mentee), has emerged as a fundamental component in the education and professional growth of junior healthcare professionals [1]. It is a supportive relationship focused on long-term professional growth, identity formation, and holistic support within a particular professional context. In contrast, supervision is primarily oriented toward performance evaluation, task oversight, and ensuring adherence to clinical or educational standards, while tutoring typically targets the acquisition of specific knowledge or technical skills in a more short-term and content-focused manner. Particularly, within clinical settings characterized by complex, novel challenges, mentoring plays a critical role in bridging theoretical knowledge and practical skills, fostering decision-making abilities, relational competencies, and professional identity formation [1]. Therefore, mentoring is a relational and longitudinal process that complements supervision or tutoring in healthcare education and practice.
The mentoring relationship has long been studied, but only recently has it gained widespread recognition as a key factor in professional competency development, especially in healthcare contexts demanding adaptability and resilience. Indeed, a growing body of theoretical work has sought to unpack the multifaceted nature of mentoring, highlighting its roles in professional development, identity formation, and psychological well-being. Among these, Kram’s Mentor Role Theory distinguishes between career and psychosocial functions of mentoring [2], the Job Demands–Resources (JD-R) model frames mentoring as a key job resource that buffers work demands [3,4], and Self-Determination Theory (SDT) emphasizes the importance of autonomy, competence, and relatedness for motivation and well-being [5]. Overall, effective mentoring programs have demonstrated improvements in academic performance and motivation, and significant psychological benefits that help reduce stress and anxiety, and prevent burnout among trainees [6,7]. Adequate preparation of mentors for the emotional and psychological dimensions of this role enhances the relational support they provide, benefiting both mentees and mentors themselves by fostering their reflective, communicative, and problem-solving skills [6,8].
Mentoring models are diverse, including peer mentoring, group mentoring, and mosaic mentoring, each adapted to specific educational needs and organizational contexts. Peer mentoring offers relatable support for trainees through mentors with slightly more experience, while group mentoring exposes mentees to multiple perspectives, thus enriching learning and promoting inclusivity [9,10]. Mosaic mentoring involves a network of mentors with varied expertise, particularly beneficial for underrepresented groups, by providing culturally sensitive and multilateral guidance [11,12].
In demanding clinical environments such as hospitals, where experiences can be emotionally taxing, mentoring extends beyond skill transmission to include psychological support, contributing to enhanced well-being, stress management, and sense of belonging within professional teams [1,13]. Importantly, mentoring has been shown to influence career choices positively by encouraging pursuit of challenging specialties and reducing attrition by providing stable and empathetic guidance during transitions, such as from academic study to clinical practice [14,15].
Despite increased scholarly interest, the mentoring literature is characterized by conceptual and methodological heterogeneity, with varying definitions, roles, goals, and assessment tools across disciplines and settings [16,17]. Emerging mentoring formats, including virtual platforms and co-productive, non-hierarchical relationships, broaden the traditional understanding of mentoring but also highlight the need for standardized frameworks and robust evaluation instruments tailored to healthcare environments [14,15].
Previous systematic reviews have examined mentoring in healthcare but reveal key gaps that this study addresses. Specifically, prior reviews have targeted mentoring across select healthcare professional groups, primarily focusing on nursing, medical, allied health professions and social care students or early career professionals. For instance, Guo et al. [18] examined peer mentoring exclusively among undergraduate nursing students, while Ellis et al. [19] focused on medical students and early career physicians, and Juntunen et al. (2024) [20] addressed undergraduate healthcare, social care, and medical students in various healthcare contexts. To our knowledge, no comprehensive synthesis spans all healthcare specialties in hospital settings.
This review fills that gap by providing a multidisciplinary evidence synthesis that emphasizes senior mentoring’s role—regardless of specialty, whether medical, nursing, or other allied health professions —in fostering professional skills and psychological resilience during clinical transitions. Specifically, it addresses the research question (i.e., whether support from a senior colleague positively impacts junior healthcare workers), structured using the PICo framework (Population, Phenomenon of Interest, and Context) appropriate for qualitative and mixed-methods evidence synthesis:
- Population: Junior healthcare professionals (physicians, nurses, midwives, and other allied health professions).
- Phenomenon of Interest: Senior mentoring and its impact on professional and personal growth.
- Context: Hospital and healthcare settings.
Although mentoring can occur across diverse healthcare contexts—including outpatient clinics and community-based services—this study focuses specifically on hospital settings. Hospitals are characterized by high workload, complex interprofessional teams, and intense emotional demands, which may amplify both the need for mentoring and the associated risks. By concentrating on this environment, we aim to examine mentoring within a context where supervision is often formalized, roles are clearly defined, and institutional structures are more visible, thereby facilitating a more in-depth exploration of mentoring dynamics in acute-care systems.
Therefore, this systematic review synthesizes current evidence to examine whether and how senior mentoring supports the professional and personal development of junior healthcare professionals in hospital settings, regardless of their specific role. Although the preponderance of existing literature focuses on nursing and medical education, similar challenges are increasingly recognized within all allied health professions. Distinct from previous reviews that addressed mentoring in specific nursing contexts or focused broadly on educational outcomes [19,20], this review uniquely integrates the psychological well-being dimension within the multidisciplinary hospital setting. Unlike prior work, we synthesize evidence spanning the entire continuum of clinical training—from students to early career professionals—identifying how mentoring acts not only as an educational tool but as a critical buffer against occupational stress in high-intensity clinical environments. Moreover, this review elucidates effective mentoring approaches, highlights benefits and challenges, and proposes directions for future research and practice to strengthen mentoring as a foundational element for developing competent, resilient, and well-supported healthcare professionals.
2. Materials and Methods
2.1. Study Design and Protocol
This study was designed as a systematic literature review to identify, evaluate, and synthesize available evidence regarding the role of mentoring in the training and professional development of healthcare students, with a specific focus on trainees in hospital settings. A systematic review design was selected over a scoping or realist review because the primary objective was not merely to map the available literature or explore theoretical mechanisms, but to critically appraise the quality of evidence and synthesize specific outcomes regarding the impact of mentoring [21]. This approach allows for a more rigorous assessment of the effectiveness of mentoring interventions in the clinical setting.
A formal protocol was not registered in the PROSPERO database; however, the review followed a pre-defined internal protocol developed by the research team to ensure consistency and transparency.
The review process followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement guidelines, ensuring transparency, methodological rigor, and replicability [22]. The PRISMA 2020 framework was selected to improve the reporting quality of the review, adhering to its 27-item checklist and flow diagram requirements. As noted by Pati and Lorusso [23], a systematic review offers a consistent and universally recognized method to minimize bias and enhance the credibility of the research process. This approach was chosen over a traditional narrative review to provide a more objective and comprehensive evaluation of the scientific evidence, thereby creating a solid foundation for decision-making in clinical and academic contexts.
Moreover, this review was guided by the methodological framework of the Joanna Briggs Institute (JBI) for systematic reviews of mixed evidence [24]. This ensures our approach to search, selection, and synthesis adheres to established rigorous standards.
2.2. Search Strategy
To comprehensively identify relevant literature, a systematic search was conducted across three major international electronic databases: Web of Science, PubMed, and Scopus, deemed to provide the most robust coverage of the general clinical hospital setting. The search strategy employed a specific string of keywords combined with Boolean operators (AND, OR) to target the population, intervention, and outcomes of interest. The search string used was as follows: (“mentoring” OR “mentorship” OR “tutoring” OR “tutorship” OR “mentor-mentee relationship” OR “mentor”) AND (“medical student” OR “psychology student*” OR “nursing student*” OR “nurs* student*” OR “health care student*” OR “healthcare student*” OR “physiotherapy student*” OR “therap* student*” OR “physical therapy student*”) AND (“psychological wellbeing” OR “psychological well-being” OR “mental health”)*. The search strategy combined MeSH terms such as ‘Mentors’, ‘Education, Medical’, and ‘Interprofessional Relations’ with free-text keywords including ‘mentoring’, ‘preceptorship’, and ‘junior health personnel’. These were combined using the Boolean operators OR (within concepts) and AND (between concepts).
We used language (English, Italian, Spanish) and date (January 2004–December 2024) filters directly in the database searches.
2.3. Eligibility Criteria
Strict inclusion and exclusion criteria were defined to select high-quality studies relevant to the research question. The time frame for inclusion was set from January 2004 to December 2024, based on the observation by Ulrich et al. [25] that the volume of healthcare research significantly increased after 2004.
The inclusion criteria required studies to focus on support provided by senior professionals to junior operators or trainees. We included both undergraduate students and early career professionals to capture the full continuum of clinical education and professional socialization. Moreover, eligible papers must use experimental designs (including quantitative, qualitative, or mixed-methods), be conducted specifically within hospital settings, and be published in peer-reviewed indexed journals. Additionally, full-text articles had to be available in English, Italian, Spanish.
Conversely, the exclusion criteria eliminated studies addressing support for professionals managing territorial or outpatient patients (non-hospitalized contexts) and studies with mixed samples where less than 50% of participants worked in a hospital setting. A threshold of ≥50% hospital-based activity was established to ensure that the primary learning environment was the clinical ward rather than the academic classroom. Articles reporting the perspectives of patients or non-healthcare individuals were also excluded, as were grey literature sources such as editorials, commentaries, theses, and opinion papers. Secondary research, including systematic reviews and meta-analyses, was similarly omitted from the final selection.
Regarding the distinction between mentoring and tutoring, although ‘tutoring’ was included in the initial search string to ensure sensitivity (capturing studies that might use the terms interchangeably), strict conceptual filtering was applied during manual screening. Studies describing purely task-oriented, short-term tutoring interventions without the longitudinal, relational, and holistic support characteristics of mentoring defined in the Introduction were excluded.
These criteria were developed to operationalize the PICo-formulated review question stated in the Introduction, ensuring focus on senior mentoring (Phenomenon of Interest) for junior professionals (Population) in hospital contexts.
2.4. Study Selection and Data Extraction
The selection process was documented to ensure reproducibility. All retrieved records were imported into Microsoft Excel for deduplication. Duplicates were identified by exact matching of DOI (primary), followed by title/author fuzzy matching using conditional formatting and SORT/FILTER functions.
Subsequently, title/abstract and full-text screening were conducted independently by two reviewers (VG and MM). Discrepancies were resolved through discussion with a third expert (IS) to prevent arbitrary exclusion and ensure reliability. Inter-rater reliability statistics (e.g., Cohen’s Kappa) were not calculated; instead, we adopted a consensus-based approach typical of qualitative synthesis, where disagreements are resolved through discussion to deepen the interpretative understanding of the data. Only records reaching unanimous agreement proceeded to the following selection stages and were finally included in the review.
Firstly, titles were screened to exclude clearly irrelevant studies based on the established criteria. Abstracts of the remaining records were then reviewed to assess eligibility regarding the study objective, context, and design. Finally, the full texts of potentially eligible articles were retrieved and critically examined to confirm adherence to the inclusion criteria.
Data extraction was conducted using an ad hoc form informed by the research team’s prior experience with systematic reviews of mixed-methods healthcare literature. The form was iteratively refined through team discussion to ensure comprehensive capture of key study characteristics (author, year, design, population, mentoring intervention, outcomes).
2.5. Quality Assessment
To evaluate the methodological quality of the included studies, the Quality Assessment with Diverse Studies (QuADS, [26]) tool was employed. This is specifically designed to appraise studies with diverse designs—including qualitative, quantitative, and mixed-methods research—making it particularly suitable for this review. The QuADS tool consists of 13 criteria assessing aspects such as the theoretical rationale, clarity of objectives, appropriateness of the study design, data collection and analysis methods, and discussion of limitations. Each item is scored on a scale from 0 to 3 (where 0 indicates no information and 3 indicates clear and complete description), allowing for a consistent and nuanced evaluation of the evidence strength across methodologically heterogeneous studies.
2.6. Data Synthesis
Inductive meta-aggregation followed the JBI guidelines for mixed-methods reviews [24]. For qualitative studies, findings, participant quotes, and author interpretations were directly extracted from results/discussion sections. Quantitative data were transformed into qualitative findings through a two-step process: (1) abstraction—extracting key results, statistics, and their interpretations from Results/Discussion sections; (2) qualitativization—reformulating these as textual statements. That is, quantitative results were “qualitized” by converting statistical significance into narrative statements of “positive/negative association” before aggregation. These analyses were conducted independently by two reviewers (G.V. and M.M.). Similar-meaning statements were grouped into categories, which were then aggregated into analytical themes through team discussion, with discrepancies resolved by I.S.
3. Results
3.1. Search Results and Study Selection
The systematic literature search, conducted in adherence to the PRISMA 2020 guidelines [22], identified a total of 399 records from three major databases: Scopus (n = 182), PubMed (n = 114), and Web of Science (n = 103). Following the initial removal of 144 duplicates, 255 unique records remained for screening.
In the first stage, title screening led to the exclusion of 49 articles: 32 were unrelated to the review topic, 2 focused exclusively on the patient perspective rather than that of professionals, and 15 were set in non-hospital contexts. Subsequently, the abstracts of the remaining articles were reviewed, resulting in the exclusion of 46 additional records. Reasons for exclusion at this stage included irrelevance to the topic (n = 12), focus on patient perspectives (n = 10), classification as grey literature (e.g., editorials, theses, opinion papers) (n = 24).
The remaining articles underwent a full-text review: 52 were outside the specific research scope, 9 were conducted in non-hospital settings, and 16 were grey literature. The final 83 eligible articles were then subjected to a qualitative assessment using QuADS tool ([26], See Supplementary Material S1. References of excluded articles are reported in notes at the bottom of the table) to exclude low-quality papers. Each study was independently evaluated across 13 criteria. Nine studies that demonstrated significant methodological deficiencies (scoring ≤ 1 on multiple dimensions [26]) were excluded. Consequently, 74 studies [9,10,11,12,14,16,18,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94] satisfied all quality and eligibility criteria and were included in the final systematic review. The entire selection process is illustrated in the PRISMA flow diagram (Figure 1).
3.2. Study Characteristics
The included studies demonstrated high heterogeneity regarding geographical origin and methodological approach, underscoring the global relevance and transversal nature of mentoring in healthcare. Geographically, the majority of research originated from Anglophone countries, where mentoring is a well-established professional development strategy: 22 studies were conducted in the United States, 16 in the United Kingdom, seven in Canada, and five in Australia. Contributions were also identified from Continental Europe (Spain, France, Finland, Netherlands, Hungary, Germany, Sweden, Ireland), Asia (India, Japan, Iran, Taiwan, Turkey), and Latin America (Brazil). One study was a transnational collaboration between the United States and Canada.
Methodologically, the review encompassed a diverse range of study designs. A significant portion (n = 33) employed qualitative methods, utilizing semi-structured interviews, focus groups, or observations to explore the nuances of mentoring relationships. Fifteen studies were descriptive, while eight utilized quantitative designs with structured questionnaires and statistical scales to measure outcomes such as satisfaction and performance. Nine studies adopted a mixed-methods approach, integrating qualitative depth with quantitative robustness. The remaining studies included observational (n = 3), longitudinal (n = 3), and pilot or methodological research. Regarding healthcare specialties, the most represented fields were medicine (23 studies) and nursing (18 studies), followed by contributions from midwifery, psychiatry, and clinical psychology (24 studies).
3.3. Thematic Analysis
Meta-aggregation (Section 2.6) of transformed findings from all studies provided a coherent picture of the value and impact of mentoring in hospital settings (Supplementary Material S2, [9,10,11,12,14,16,18,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94]). Specifically, the inductive analysis yielded four main themes: Support Function, Skill Development, Psychological Well-being, and Professional Satisfaction and Community Belonging. As illustrated in Figure 2, these themes are not isolated but dynamically interact; for instance, mentors’ support fosters both professional and emotional guidance.
3.3.1. Support Function
A primary theme identified was the function of support, encompassing both professional guidance and emotional backing. Numerous studies [18,31,33,35,38,39,40,42,45,47] reported that mentees viewed their mentors as stable reference figures capable of offering encouragement and active listening during periods of uncertainty. This support was found to be particularly critical during transitional phases, such as the shift from academic environments to clinical practice, and in high-pressure emotional contexts.
3.3.2. Skill Development
Mentoring was centrally linked to the development of both technical and transversal competencies. Many studies [29,38,43,45,52,62,68,77] documented improvements in specific clinical skills, problem-solving abilities, and complex case management. Parallel to technical growth, studies highlighted enhancements in communication skills, interpersonal relationship management, and interdisciplinary collaboration [12,27,30,38,45,46,56]. This process was often accompanied by increased self-confidence and self-efficacy, positively influencing decision-making autonomy and resilience in facing unforeseen situations [47,56,71,72,80]. The mentor–mentee relationship frequently emerged as a bidirectional learning process, where mentors also refined their leadership and communication capabilities.
3.3.3. Psychological Well-Being
Several studies emphasized the protective effect of mentoring on psychological well-being, noting reductions in stress, anxiety, and burnout [18,56,62,64,88]. In some instances, mentoring provided a “safe space” for sharing difficulties and reflecting on critical experiences without fear of judgment [10,11,63,75,83,84,85,86,87,88,89,90,91,92,93]. This dimension of well-being was closely tied to the ability to maintain emotional balance and redirect energy when facing obstacles.
3.3.4. Professional Satisfaction and Community Belonging
A further key theme was the enhancement of professional satisfaction and a sense of belonging to the healthcare community. Mentees reported that mentoring fostered stronger ties with the organization and the team, facilitating integration into clinical settings [29,34,45,54,56,71,74,75,76,77]. Additionally, mentoring was found to drive broader cultural changes within healthcare organizations by promoting collaboration and the sharing of best practices [38,39,43,47,65,66,67]. In specific contexts, this contributed to improvements in the overall quality of care and user satisfaction [43,44,45,46,54,60,72,77,78,92]. Overall, the results indicate that mentoring extends beyond technical training, acting as a catalyst for personal, professional, and organizational growth.
4. Discussion
One of the central findings emerging from this review is that the effectiveness of mentoring cannot be attributed to a single factor, but rather to a complex interplay between the quality of the relationship, institutional support, and specific mentor training. This evidence confirms previous literature describing mentoring as a bidirectional relational process capable of influencing both academic and personal domains [18].
Overall, our findings can be interpreted through several theoretical lenses that elucidate the mechanisms linking mentoring to professional and psychological outcomes. Consistent with Kram’s Mentor Role Theory, the participants reported benefits that align with both career functions (e.g., skill acquisition, professional guidance) and psychosocial functions (e.g., emotional support, role modeling) [2]. The explicit engagement with these psychosocial functions suggests that mentoring provides a protective space for identity formation, which is critical during transition phases in healthcare careers.
Furthermore, regarding psychological well-being, the results support the Job Demands–Resources (JD-R) model [3,4]. In the high-demand context of healthcare—characterized by emotional exhaustion and heavy workloads—mentoring acts as a vital job resource. By providing social support and constructive feedback, mentoring buffers the physiological and psychological costs of these job demands, thereby reducing the risk of burnout and enhancing engagement. Additionally, from the perspective of Self-Determination Theory (SDT, [5]), the mentoring relationship likely fosters psychological well-being by satisfying the basic psychological needs for competence (through professional development) and relatedness (through the mentor–mentee bond), which are prerequisites for intrinsic motivation and mental health in clinical settings.
Thus, our findings align with the main theoretical frameworks introduced. The emotional support identified in our themes maps directly to the ‘psychosocial functions’ of Kram’s theory [2] and the ‘relatedness’ need in Self-Determination Theory [5]. Furthermore, the role of mentors in reducing burnout validates the Job Demands–Resources (JD-R) model [3,4], positioning mentoring as a key ‘job resource’ that buffers the high demands of hospital care.
Specifically, this review highlights that mentor availability, empathy, and the capacity to provide constructive feedback are essential conditions for creating a meaningful experience, consistent with findings by Nebhinani et al. [42] and Abrams et al. [67].
Specifically, mentoring has a critical role in fostering psychological safety which allows junior professionals to ask questions, admit errors, and seek feedback without fear of negative consequences. Our findings suggest that effective mentoring creates a ‘safe container’ for learning, which is essential for mitigating burnout and enhancing professional confidence in high-pressure hospital environments.
A comparison with international literature reveals interesting divergences. For instance, Gardner [95], reflecting on doctoral nursing education in the United States, highlights that the mentoring relationship plays a crucial role not only in emotional and professional support but also in the construction of academic and research identity. Although this aspect is considered less prominent in the European studies included in this review, it represents a relevant insight, demonstrating how mentoring can assume different meanings depending on the context and level of training.
More recent systematic reviews provide further nuance. Ellis et al. [19] demonstrated that structured mentoring, coaching, and peer-support programs are associated with improved well-being and reduced burnout among physicians, reinforcing the protective role of mentoring in high-stress clinical environments. In line with these results, our review suggests that the psychological support and guidance provided through the mentor–mentee relationship can buffer occupational stress and enhance resilience.
Similarly, Juntunen et al. (2025) [20] synthesized qualitative evidence on the competencies required for mentoring interprofessional students in clinical practice, emphasizing skills such as facilitating reflective learning, fostering collaboration, and supporting professional identity development. Overall, these pieces of literature suggest that mentoring is not limited to personal and relational growth but can also serve as a fundamental vehicle for developing innovative professional skills, which are now indispensable for clinical practice.
From a geographical perspective, it is observed that studies from non-European contexts (such as India or the United States) place greater emphasis on the educational dimension and academic career construction. In contrast, European and South American studies more strongly highlight the function of psychological support and guidance through difficulties [66]. This difference likely reflects the varying weight that different educational and healthcare systems attribute to the technical versus the relational dimensions of mentoring.
A further critical element concerns risk factors. In healthcare settings, several potential risks can undermine the effectiveness and safety of mentoring relationships. These include excessive workload and time constraints on mentors, power imbalances between senior mentors and junior mentees, mismatched expectations about the goals of mentoring, and inadequate psychological safety, which may discourage open disclosure of stress or errors. Systematic and scoping reviews in graduate medical education and nursing highlight that poorly structured programs, lack of mentor training, and insufficient institutional oversight can amplify these risks, sometimes leading to disillusionment or even unprofessional behavior [33,96,97]. Our review confirms that barriers such as lack of time, organizational difficulties, and power dynamics can compromise the trust relationship, as discussed by Nebhinani et al. [42]. The hierarchical nature of healthcare can introduce complex power dynamics into the mentoring relationship. If not managed carefully, these dynamics may inhibit open communication. Future mentorship programs must therefore include specific training on navigating hierarchy to ensure the relationship remains supportive rather than directive. However, the novelty emerging here is that such difficulties should not be viewed exclusively as obstacles, but as useful indicators for understanding the organizational conditions necessary to render programs truly effective. In this sense, limitations become opportunities to rethink mentoring as a more structured device, capable of integrating emotional support, clinical skill development, and professional growth. Ultimately, the results of this review appear largely consistent with established literature but also offer new perspectives. On one hand, they confirm the centrality of the relationship and institutional support, as clearly defined meeting schedules, shared expectations, and institutional support can reduce key risk factors while preserving the benefits of mentoring for professional development and psychological well-being [97]. On the other hand, they suggest that mentoring must be conceived as a flexible tool, capable of adapting to different educational levels, specific cultural contexts, and the new challenges facing healthcare professions, such as digitalization and the increasing complexity of required competencies.
4.1. Strengths and Limitations
This systematic review has several notable strengths. First, it followed a rigorous methodological approach guided by the PRISMA 2020 statement [22], ensuring a transparent, reproducible, and comprehensive selection process. The search strategy was extensive, covering three major international databases (Web of Science, PubMed, Scopus) and including a broad range of healthcare disciplines (medicine, nursing, psychology, and physiotherapy), which enhances the generalizability of the findings to the wider healthcare context. Furthermore, the use of the QuADS tool [26] allowed for a consistent evaluation of studies with heterogeneous designs—qualitative, quantitative, and mixed-methods—providing a nuanced assessment of the evidence quality. The inclusion of studies from diverse geographical regions (Europe, North America, Asia, and South America) also strengthens the review by offering a global perspective on mentoring practices, highlighting both cross-cultural commonalities and context-specific differences.
However, the study also presents some limitations. First, despite the rigorous search strategy, limiting the inclusion criteria to articles published in English, Italian, Spanish may have led to the exclusion of relevant studies published in other languages, potentially introducing a language bias. However, these languages were selected based on the authors’ proficiency to ensure accurate data extraction. Similarly, while the exclusion of specialized databases such as CINAHL and PsycINFO may introduce some selection bias, the selected databases (PubMed, Scopus, and Web of Science) were deemed to provide the most robust coverage of the general clinical hospital setting central to our research question. Second, the significant heterogeneity of the included studies—ranging from varying mentoring definitions and models to different assessment tools and outcomes—made it challenging to perform a quantitative meta-analysis. Consequently, the findings are presented as a narrative synthesis, which, while rich in detail, limits the ability to statistically quantify the overall impact of mentoring interventions. In addition, given the qualitative, thematic nature of our review, in which the focus was on interpretive analysis of mentoring experiences and their practical implications, we did not calculate formal inter-rater reliability statistics (e.g., Cohen’s kappa) for the screening and selection process. While disagreements were resolved through discussion and consensus, the absence of a quantified measure of agreement may reduce the transparency of the selection phase compared with reviews that explicitly report such indices [98]. Again, regarding quality assessment, the decision to exclude studies with a QuADS score of ≤1 was intended to preserve the methodological reliability of the synthesis by removing sources with critically insufficient reporting. However, we acknowledge this threshold constitutes a selection bias, as it may have led to the omission of studies that possessed valid field insights but lacked rigorous academic reporting standards. Third, many included studies employed cross-sectional designs or relied on self-reported measures of satisfaction and well-being, which may be subject to social desirability bias and do not allow for causal inferences regarding the long-term efficacy of mentoring. Additionally, although the review identified key themes such as support and skill development, the variability in how “mentoring” is operationalized across institutions suggests that caution is needed when directly comparing results across different healthcare settings. A further limitation is that the study focuses exclusively on hospital settings, which may limit the transferability of our findings to outpatient or community-based contexts where mentoring may occur in more informal or decentralized ways. Again, while this study includes participants from various stages of professional development, it was designed to assess general trends within the clinical setting. Future studies should aim to explicitly distinguish and compare outcomes between undergraduate students, postgraduate trainees, and early career professionals to better understand group-specific dynamics.
Finally, our synthesis remains largely narrative and does not systematically compare the strength of effects across different mentoring models or healthcare disciplines. In addition, it should be also noted that the theoretical frameworks (Kram’s Mentor Role Theory [2], JD-R [3,4], and SDT [5]) were applied retrospectively to interpret the synthesized findings rather than to guide the initial systematic search and data extraction. While this inductive approach was chosen to minimize confirmation bias and allow themes to emerge naturally from the data, it may have limited the specific theoretical depth compared to a purely deductive review designed explicitly to test these models. In addition, we did not perform a formal analysis of regional differences, so the geographical distribution of studies is presented primarily to illustrate the global scope of the literature rather than to identify meaningful regional patterns.
4.2. Practical Implications
The data collected in this review confirm that mentoring extends beyond the transmission of technical skills to play a broader role in sustaining emotional well-being, reducing stress and burnout, strengthening self-efficacy, and fueling motivation.
These findings have significant practical implications, as evidenced by the work of Bellodi and Dolhnikoff [52], who investigated the experiences of medical students with performance difficulties. The authors demonstrate how a structured academic mentoring program can offer concrete support to these students, addressing both educational and emotional needs. In this sense, mentoring reveals itself as an instrument of equity, capable of reducing the risk of exclusion and supporting those in situations of greater vulnerability. These data underscore the practical importance of developing personalized programs, supported by institutions, that can genuinely respond to the needs of the student population.
Furthermore, the review draws attention to the accessibility and inclusivity of mentoring. The study by Gerk et al. [63], conducted among medical students in Brazil, highlighted how gender discrimination influences career aspirations and conditions access to mentoring figures. Not all students have equal opportunities to benefit from this tool; without targeted interventions, there is a risk that inequalities may be amplified rather than reduced. This finding calls for the design of equitable mentoring models that are sensitive to diversity and capable of breaking down barriers related to gender and other forms of discrimination.
Thus, to translate these findings into practice, healthcare institutions should formalize mentoring programs by establishing clear objectives and allocating protected time, rather than relying on informal support. Crucially, mentors require specific training focused on soft skills and psychological safety, ensuring they are equipped to support personal growth beyond technical clinical expertise. Finally, it is vital to explicitly distinguish the developmental role of a mentor from the evaluative role of a clinical supervisor to prevent role ambiguity and conflict.
5. Conclusions
Mentoring represents a central instrument for accompanying healthcare students along their educational and professional paths. It emerges as a relational and educational device with great potential, yet its effectiveness depends on how it is conceived, structured, and made accessible. The practical implications indicate a need for targeted programs capable of supporting even the most fragile students, while future perspectives urge the construction of inclusive pathways oriented toward social justice. Only in this way can mentoring fully express its transformative function, contributing to individual growth, the strengthening of professional communities, and the improvement of healthcare and educational systems. Therefore, the main implication for healthcare education policy is that structured mentoring programs should be formally integrated into postgraduate training curricula in hospital settings to systematically support the professional development and psychological well-being of junior healthcare workers.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Elce Y. The Mentor-Mentee Relationship, Addressing Challenges in Veterinary Medicine Together. The Veterinary clinics of North America Small Anim. Pract.2021511099110910.1016/j.cvsm.2021.04.02334238600 · doi ↗ · pubmed ↗
- 2Kram K.E. Mentoring at Work: Developmental Relationships in Organizational Life Scott, Foresman & Co.Glenview, IL, USA 1985
- 3Demerouti E. Bakker A.B. Nachreiner F. Schaufeli W.B. The job demands-resources model of burnout J. Appl. Psychol.20018649951210.1037/0021-9010.86.3.49911419809 · doi ↗ · pubmed ↗
- 4Bakker A.B. Demerouti E. The Job Demands-Resources model: State of the art J. Manag. Psychol.20072230932810.1108/02683940710733115 · doi ↗
- 5Ryan R.M. Deci E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being Am. Psychol.200055687810.1037/0003-066X.55.1.6811392867 · doi ↗ · pubmed ↗
- 6Altonji S.J. Baños J.H. Harada C.N. Perceived Benefits of a Peer Mentoring Program for First-Year Medical Students Teach. Learn. Med.20193144545210.1080/10401334.2019.157457930776921 · doi ↗ · pubmed ↗
- 7Sutkin G. Littleton E.B. Kanter S.L. How surgical mentors teach: A classification of in vivo teaching behaviors part 2: Physical teaching guidance J. Surg. Educ.20157225125710.1016/j.jsurg.2014.10.00425468768 · doi ↗ · pubmed ↗
- 8Biber D. Rothman R. Mental health literacy training for college female peer mentors: A pilot study High. Educ. Ski. Work-Based Learn.20231418119110.1108/HESWBL-06-2023-0148 · doi ↗