Effective Interventions to Prevent Breastfeeding-Related Nipple-Areolar Lesions: A Systematic Review
Ana Chagas, Fernanda Moura, Monise Bispo, Lays Medeiros, Isabelle Costa, Rhayssa Araújo

TL;DR
This study reviews effective strategies to prevent nipple injuries during breastfeeding, which can improve maternal and infant health outcomes and reduce healthcare strain.
Contribution
The study systematically identifies specific interventions, such as educational practices and natural remedies, that effectively prevent breastfeeding-related nipple injuries.
Findings
Educational practices like simulations and demonstrations by qualified professionals are effective in preventing nipple-areolar lesions.
Natural remedies such as peppermint, olive oil, and honey show effectiveness in preventing breastfeeding-related injuries.
Early identification of risk and continuous follow-up improve maternal and child outcomes.
Abstract
Public health relevance—How does this work relate to a public health issue? Nipple-areolar lesions are a public health problem because they compromise breastfeeding, leading to maternal suffering, early weaning, and negative impacts on infant health and key breastfeeding indicators.They also increase avoidable demands on health services and strain on health systems, especially in vulnerable contexts, making their prevention essential for efficient, equitable, and sustainable care. Nipple-areolar lesions are a public health problem because they compromise breastfeeding, leading to maternal suffering, early weaning, and negative impacts on infant health and key breastfeeding indicators. They also increase avoidable demands on health services and strain on health systems, especially in vulnerable contexts, making their prevention essential for efficient, equitable, and sustainable care.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
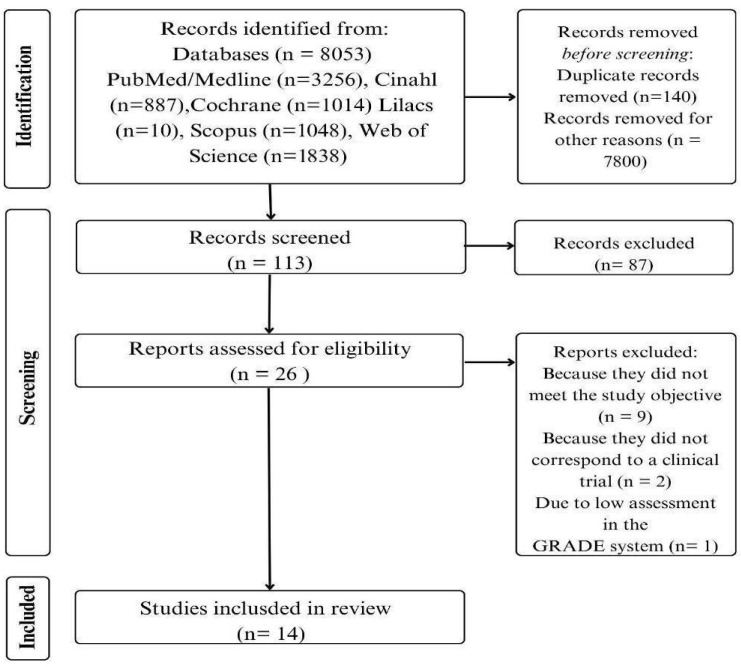 Figure 1
Figure 1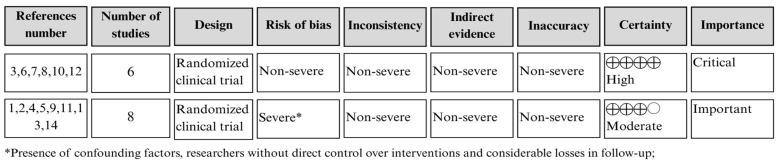 Figure 2
Figure 2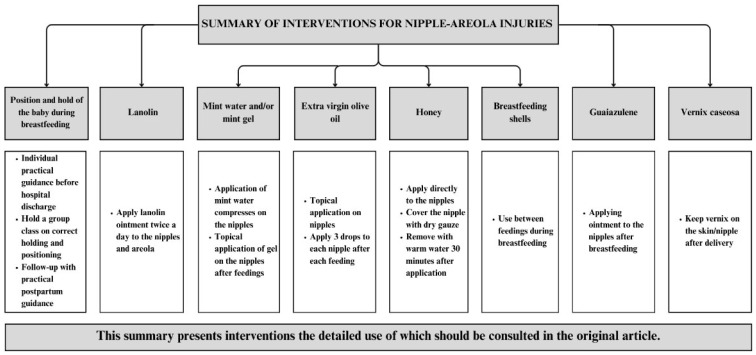 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreastfeeding Practices and Influences · Breast Implant and Reconstruction · Neonatal skin health care
1. Introduction
The World Health Organization (WHO) recommends exclusive breastfeeding for the first six months of life, continuing until at least two years of age, alongside the introduction of complementary foods [1]. This practice is the best choice for the growth and development of infants due to the nutritional and immunological properties of breast milk, as well as the opportunity to establish and strengthen the emotional bond between mother and baby [2].
Additionally, breastfeeding is essential for the maturation of the infant’s physiological systems, as it provides immunological, nutritional, and biological compounds that support early-life development [3].
Breastfeeding plays a critical role in the maturation of the infant’s physiological systems, contributing to immune protection, gastrointestinal development, and neurocognitive outcomes, as well as reducing the risk of infectious diseases and long-term chronic conditions. For mothers, it offers protection against breast and ovarian cancer, helps prevent postpartum hemorrhage, and reduces the risk of chronic diseases such as type 2 diabetes and cardiovascular conditions [4].
Despite its importance, breastfeeding rates in the Americas, for example, only show about 38% of babies under six months of age who are exclusively breastfed, which is below the target of at least 70% by 2030 [1,5]. Various factors contribute to this, particularly in the first weeks of the postpartum period when the most common breast complications occur, such as the development of nipple-areolar lesions. Although highly prevalent, these lesions should not be overlooked [6,7].
Nipple-areolar lesions are characterized by alterations in the nipple-areolar skin, identified by changes in color, thickness, fluid content, or tissue loss. In most cases, these lesions are associated with early weaning due to pain and difficulties in achieving proper latch-on by the infant [8,9,10]. These lesions typically persist for an average of seven days postpartum, with healing time depending on their severity and extent, potentially lasting one to two weeks. They affect approximately 58% of postpartum women, highlighting their high prevalence in this population [11].
The etiology of nipple-areolar lesions is multifactorial and involves maternal, infant-related, and breastfeeding management factors. Commonly reported causes include improper positioning and latch, ineffective sucking patterns, prolonged or frequent feeding without adequate milk transfer, nipple engorgement, and excessive friction or moisture on the nipple-areolar complex. Infant anatomical conditions that compromise oral function also play a significant role. In particular, a short sublingual frenulum (ankyloglossia) may restrict tongue mobility, impair effective latch and milk extraction, and increase mechanical stress on the nipple, thereby contributing to nipple pain and tissue damage in breastfeeding women [9,10,11].
Given the high prevalence of nipple-areolar lesions and their negative impact on breastfeeding continuation, identifying effective preventive interventions is essential to support sustained breastfeeding and maximize its health benefits for both mothers and infants. In this process, it is important to highlight that in the context of areola-nipple lesions related to breastfeeding, preventive strategies can be conceptually divided into primary prevention, which aims to avoid the onset of tissue damage, and secondary prevention, focused on the management of already established lesions.
However, the existing literature has predominantly emphasized treatment approaches, while evidence specifically addressing primary prevention is still limited. Therefore, this study focuses exclusively on primary prevention interventions, defined as strategies implemented before the development of areola– nipple lesions to reduce their occurrence.
Thus, the objective of this study is to synthesize the evidence on effective interventions for preventing nipple-areolar lesions caused by breastfeeding.
2. Methods
2.1. Study Design, Period, and Location
This is a systematic review of efficacy, conducted using a self-developed protocol and guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (Supplementary Material PRISMA checklist) [12] and the Joanna Briggs Institute Manual for Evidence Synthesis (Aromataris) [13].
The systematic review was carried out in Natal, Rio Grande do Norte, Brazil, from June 2021 to July 2025. Database searches were conducted between September 2024 and July 2025.
2.2. Population or Sample and Inclusion and Exclusion Criteria
The guiding research question followed the PICO strategy (Population, Intervention, Comparison, and Outcome) (PRISMA) [12]. The defined population included lactating women at any stage of breastfeeding. Interventions encompassed any actions taken to prevent nipple-areolar lesions caused by breastfeeding, regardless of type, frequency, or intensity. Regarding comparison, since this review aims to address a broader question, all existing alternative interventions were considered (placebos, standard care, other preventive strategies, or even no intervention). The outcome was the prevention of nipple-areolar lesions caused by breastfeeding, regardless of how it was measured. Thus, the research question was formulated as follows: Which interventions are effective in preventing nipple-areolar lesions in lactating women?
Regarding eligibility criteria, this review included interventional studies, original articles available in full text, and studies addressing preventive care for nipple-areolar lesions related to breastfeeding in lactating women. Studies whose primary objective was the treatment or management of already established nipple-areolar lesions were excluded.
2.3. Study Protocol
This study was registered in the International Prospective Register of Systematic Reviews (PROSPERO), an international database of systematic reviews (identification: CRD42021278258).
The searches were carried out using the CAPES (Coordination for the Improvement of Higher Education Personnel) platform through CAFe (Federated Academic Community) access, in the Medical Literature Analysis and Retrieval System On-line/National Library of Medicine (Medline/Pubmed), Scopus, Cumulative Index to Nursing and Allied Health Literature (Cinahl), Web of Science, Cochrane and Latin American, and Caribbean Health Sciences Literature (Lilacs) databases.
The descriptors were selected from DECs/Mesh Terms in English and Portuguese. Different search strategies were tested in order to find as many potential studies as possible.
Thus, the databases Web of Science, Cochrane, and Lilacs were used: Nipple* (OR Nipple trauma OR nipple soreness OR sore nipples OR nipple fissure OR nipple cracked OR nipple cracks) AND Wound and injuries AND Breastfeeding AND Primary prevention (OR prevention) AND Clinical trial NOT Treatment. In the grassroots Medline/Pubmed, Cinahl e Scopus utilizou-se: Nipple* (OR Nipple trauma OR nipple soreness OR sore nipples OR nipple fissure OR nipple cracked OR nipple cracks) AND Wound and injuries AND Breastfeeding AND Primary prevention (OR prevention).
Each database obtained a different search strategy due to the application of filters. In the Medline/Pubmed database, the following filters were used: free full text, comparative study, clinical trial, controlled clinical trial, randomized controlled trial, teen (13–18 years), adult (19+ years) e female. In Cochrane, the following filters were used: Trials; in Scopus, open access; Web of Science, open access and article. In Cinahl, the following filters were used: full text filter; Lilacs, not filter.
2.4. Analysis of Results and Statistics
The data from the selected articles was extracted, entered, and organized in a self-made spreadsheet on the Excel 2016 platform with a description of identification (base, period, country, and authors), methodological characteristics (type of intervention, control group and intervention group, type of research, follow-up period and sample), and main results. The data was presented in the form of figures, and descriptive statistics were used, using absolute and relative frequencies.
Thus, the studies were evaluated by two independent evaluators who followed the same search protocol, selecting based on the title, abstract, and full text. If there were any discrepancies, a third reviewer was consulted.
Screening was also carried out by reading the titles and abstracts. The studies were then selected by reading the full text of the articles. The data collected during the search process was stored in a spreadsheet. The eligibility process flowchart is shown in Figure 1.
As for the certainty of the evidence, this was evaluated using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) system, and the degree of certainty was assessed using Gradepro software https://www.gradepro.org (accessed on 21 June 2021) [14]. An in-depth analysis of the methodological quality of each study was carried out by two independent reviewers. Discrepancies were analyzed by a third reviewer.
This tool has been used by systematic reviewers to analyze the quality of evidence. Figure 2 shows the design of the study, its classification in terms of risk of bias, inconsistency, indirect evidence, imprecision, importance, and certainty. The latter classification can be assessed as high (high reliability in estimating the effect), moderate (moderate confidence in estimating the effect), low (limited reliability in estimating the effect), and very low (uncertain reliability in estimating the effect) (XIE GRADE). Studies with low or very low certainty were excluded.
Furthermore, the data on the characterization of the studies is presented in a narrative synthesis shown in Table 1.
3. Results
Figure 1 shows the flowchart of the selection process for the studies that make up this systematic review. The final sample included 14 selected articles, all of which were randomized clinical trials.
One study was excluded because it had a low degree of certainty in the GRADE assessment. The study compared the use of two ointments prepared by the pharmacist at the hospital where the study was conducted.
However, women who already had nipple lesions, confirmed by visual examination, were accepted into the control and intervention groups, which could be considered a potential source of confusion in the interpretation of the results, as this was a study focused more on the treatment of nipple-areolar lesions.
In addition, the women were only monitored in part at the hospital after discharge, and they were only given instructions to continue the same practices at home. Thus, the researchers had no direct control over the control group’s non-use of the ointment. The quality assessment of the included studies using GRADE is shown in Figure 2.
Of the final sample, two articles were in the same journal, the International Breastfeeding Journal, while the rest were in different journals. Regarding the databases in which the studies were found, 30.7% were in Cochrane, 23.1% were in Scopus and Cinahl, and finally, 7.7% of the articles were identified in the Web of Science, Pubmed/Medline, and Lilacs databases.
Regarding the country of origin, the studies were produced in Turkey (30.7%), Italy, Iran, Brazil (15.4% in each country), Cuba, India, and Australia (7.7% in each country).
With regard to the year of publication, 10% of the articles were published in the last 3 years, 60% in the last 10 years, and 30% before that. Still on the subject of publications, 100% of the studies were published in English.
Prevention strategies that have shown positive results include the use of educational practices, with simulations and demonstrations of breastfeeding techniques in person with a qualified professional (a senior midwife, for example), and also through educational videos. The use of peppermint (in aqueous solution or gel), extra virgin olive oil, honey, guaiazulene ointment, and caseous vernix also emerged with good results. Table 1 details the interventions and results of each study.
The main interventions found in relation to the prevention of nipple-areolar lesions that may be helpful during clinical practice are shown in Figure 3.
4. Discussion
The main contribution of this systematic review is the grouping of interventions analyzed as effective for the prevention of breastfeeding-related nipple-areolar injuries. In this way, the description of these measures helps clinical practice by providing professionals with quick access to evidence for practice in order to aid decision-making.
Although relevant, topical therapies need to be present alongside educational actions to better help resolve the probable causes of the development of these lesions.
Another important point is the variety of methods for assessing pain, lesions, and the baby’s position during breastfeeding. As for pain, some studies used the Visual Analog Scale, while others used their own questionnaires to measure its intensity.
For nipple-areolar lesions, the Nipple Trauma Index (NTI) was used by one study, while two others assessed them with a ruler and measuring tape: 1–2 mm, mild; 2–9 mm, moderate; >10 mm, severe and/or with a yellowish color in the fissure. Areolar damage was also measured using the same criteria. Many of them did not specify the method of analysis.
Information related to position and latch-on in some contexts was measured using the LATCH scale (latch-on, audible swallow, type of nipple, comfort, and help), which corresponds to latch-on, audible swallow, type of nipple, comfort, and help. Other studies relied on visual analysis of this data by qualified health professionals and the researchers themselves. This information was used to provide guidance on the correct breastfeeding technique.
Correct guidance on positioning and latch-on are shown to prevent nipple-areolar lesions [11]. One study [29] highlights the importance of guidance on breastfeeding techniques, emphasizing the importance of this during prenatal and puerperal care in order to achieve significant results in reducing this damage. In this scenario, the professional nurse plays an important role in prophylaxis and in managing the difficulties encountered by the puerperal woman and the infant [22].
Thus, health education on breastfeeding has been shown to be the most cited approach, with a moderate level of certainty, especially when it is based on guidance, training, and answering questions, and is shown to be effective in reducing the appearance of breast cracks [15,21,22].
Furthermore, the considerable increase in the integration of technological resources in society reinforces the importance of developing innovative means of promoting health education in order to make this process more attractive and dynamic [30]. In this way, the study cited in this paper [23] used video as a visual tool to teach the correct way to breastfeed and prevent complications such as breast fissures, showing positive data in relation to this prevention.
In addition, one of the ways of carrying out health education is counseling and/or training the patient. Among the studies mentioned [21], an education protocol was developed which was applied in separate groups and involved common care, guidance through leaflets, and direct training with demonstration of the appropriate technique. Among these, the option which resulted in the most positive data on the prevention of nipple lesions was training with demonstration. This study presents a moderate level of certainty.
The length of the teaching sessions has also been shown to be relevant in this prevention. One study [22], with a moderate level of certainty, added an additional hour of teaching to the standard education offered by the hospital and found a reduction in nipple trauma, while another study [15], with a high level of certainty, added 30 min to the unit’s routine education and found no statistical difference.
There is also a practice that should be applied from the moment the pregnancy is discovered and after the birth, and that is support. In order to provide quality health education, it is necessary to maintain a support network that includes the patient, the professional, the family, and the partner or friends, as this allows women to feel more secure in the care they receive and to practice the guidelines during their daily lives [15].
As for the care guidelines that should be provided by professionals, they have a direct influence on the success of breastfeeding, with nurses playing an important role in this process [31]. However, another study reinforces the importance of adequate training for these professionals, which is influenced by the context of the practice, respecting the need for changes in the work process and the balance between evidence-based practice and social relevance [32].
This once again confirms the importance of professionals seeking and carrying out constant updating and training during their work. This search for complementary training can and should be encouraged by educational institutions but also by health institutions through the creation of actions, programs, and projects that, in the future, will generate positive results for the healthcare environment, in which professionals can always be looking to develop better care alternatives for the population in general [33].
Considering natural intervention products, those containing peppermint stand out in the literature [16,17,18]. Peppermint belongs to the Mentha genus within the Lamiaceae family and is widely used in the production of infusions, gels, topical formulations, flavorings, and essential oils. Its anti-inflammatory, antioxidant, and analgesic properties have been attributed mainly to menthol, which exerts a local cooling effect and has been associated with pain relief and skin comfort in various clinical contexts [34].
In the context of breastfeeding, peppermint-based preparations have been used primarily for topical application to relieve nipple pain and prevent nipple-areolar lesions. Studies have reported favorable outcomes among women who applied absorbent cotton soaked in peppermint water to the breasts, although these investigations lacked a control group or direct comparison with breast milk application [16,17]. The available studies involving Mentha piperita demonstrated a high level of certainty regarding their reported outcomes; however, methodological limitations should be acknowledged when interpreting these findings.
Furthermore, to date, none of the studies included in this review reported an association between topical peppermint use and reduced milk production. Nevertheless, given the limited number of studies and the absence of outcomes specifically measuring lactation volume, further research is warranted to better explore this relationship. Consequently, the topical use of peppermint for nipple care should be approached with careful clinical judgment and caution, particularly in the absence of robust evidence addressing its effects on milk supply.
In Brazil, the Ministry of Health recommends the application of expressed breast milk to the nipple-areolar complex after each feeding and/or after bathing as a preventive measure against nipple lesions [35]. Breast milk represents a cost-free and readily accessible preventive strategy for breastfeeding women. Although one comparative study suggested lower effectiveness compared to peppermint-based interventions, its established safety profile and accessibility support its continued recommendation within breastfeeding care.
Lanolin is a substance extracted from sheep’s wool and used as a base for the development of cosmetics and pharmacological products.
A study carried out showed that its use is a widespread practice within health services and among professionals who work with breastfeeding, as it has positive repercussions on the care of the lesion from pregnancy to after childbirth. However, although there is proof of its effectiveness in treating nipple-areolar lesions, no evidence was found to support its use for prevention, as shown in the results of this article, with a moderate level of certainty [24,36].
As for guaiazulene (a derivative of plants such as Matricaria chamomilla L., Callis intratropica blue, among others), which is natural from azulene and fat-soluble, it has great anti-inflammatory, anti-infectious, antioxidant, and antifungal properties and is widely used in cosmetics and health care [37]. According to a published study, the compound is also effective in preventing nipple cracks, as highlighted after measuring the effect of guaiazulene ointment and the use of breast milk as an intervention in nipple-areolar lesions in breastfeeding women [27].
When it comes to products based on natural compounds, it is possible to see positive results with extra virgin olive oil, with more than a 97% absence of lesions in the women who used it, in a study with a high degree of certainty. This product has properties that aid healing and prevent inflammation, without showing any adverse effects in the studies [20,25].
Another alternative involves applying honey to the areola. Research involving the application of this substance [19] shows a high level of certainty and describes that honey helps prevent breastfeeding injuries. In this sense, the mechanism of action of honey and its therapeutic actions derive from its antioxidant, antimicrobial, and anti-inflammatory properties. In addition, this product has the ability to stimulate the immune system, cell proliferation, and autolytic debridement, so it can significantly help regenerate skin lesions [38].
However, although some studies included in this review report the use of honey as a topical intervention for nipple-areolar lesions, this practice requires careful consideration. According to the American Academy of Pediatrics, honey intake is contraindicated for infants under 12 months of age due to the risk of infant botulism. Although the application described in the included studies refers to topical use on the mother’s nipple, rather than direct oral consumption by the infant, there is still a potential risk of indirect ingestion during breastfeeding [39].
Therefore, the use of honey on the nipples cannot be universally recommended and should be approached with caution, strict hygiene measures, and professional guidance. Thus, it is noted that future studies should prioritize safer alternatives with well-established safety profiles for both mother and baby.
In relation to vernix caseosa, which is a whitish, oily substance that covers the skin of the newborn at birth, one study showed that it was effective in preventing nipple lesions and relieving pain when compared to breast milk, although care and proper preparation are needed when collecting and storing vernix for use after childbirth [28].
Regarding the evaluation of the use of breastfeeding shells, which are plastic or silicone devices that cover the areola and nipple inside the bra, creating a space for ventilation and avoiding contact with the fabric of clothing, they do not prevent nipple-areolar lesions or pain, as highlighted in the study [26]. Correcting the baby’s grip and positioning is a more satisfactory intervention.
Finally, this research is a means of updating health professionals on how to prevent nipple-areolar lesions in order to help reduce pain and inflammation. Most of the selected studies relate effects from some substance and instructions to the mother, showing that breastfeeding and correct latch-on are essential for preventing injuries and promoting comprehensive care.
One of the limitations found during the search was that most of the studies focused on the treatment of nipple-areolar lesions. In other words, research into prevention is less frequent and needs to be encouraged. In addition, there are few more recent studies on the subject. Most of them cover a period of more than five years. Future research could benefit from expanding search sources to include different databases and journals, thereby covering a more complete spectrum of the available literature.
It is also suggested that other comparative clinical trials be conducted on the use of honey, olive oil, and peppermint, as well as testing other educational strategies using educational technologies, such as realistic simulations, educational podcasts, and teaching using virtual reality, among others.
Although there are some studies addressing this topic, this study adds value in several key aspects, such as its strictly preventive scope and standardized primary outcome (incidence of nipple-areolar lesion), avoiding the heterogeneity of reviews that combined prevention, treatment, and nonspecific pain, updating the body of evidence, incorporating studies published after the time cuts of previous reviews, and a more informative analytical synthesis, with subgroups for potential effect modifiers.
Therefore, our study stands out by synthesizing exclusively the evidence on effective interventions to prevent nipple-areolar lesions, applying methodological rigor (PRISMA, registration in PROSPERO, quality assessment with GRADE) and incorporating recent publications not included in previous reviews. Thus, it contributes by offering clear support for clinical practice and the formulation of healthcare strategies, filling a gap that still exists in the literature.
5. Conclusions
It was found that effective prevention interventions for nipple-areolar lesions related to breastfeeding are mainly based on health education and the use of accessible natural products, such as formulations based on peppermint, honey, extra virgin olive oil, and breast milk.
Among these strategies, educational interventions focused on health promotion were described in the vast majority of results because, even if another therapy is chosen, it should be presented in conjunction with guidance and training, teaching the correct breastfeeding positions and the correct latch when sucking breast milk, situations that help prevent nipple-areolar lesions.
The evidence indicates that preventive interventions were applied under specific conditions, considering factors such as formulation, frequency of use, and the postpartum period. Therefore, the decision to use these interventions should take all these points into account (product presentation, frequency of use, postpartum period, among others).
Thus, we reiterate that the absence of standardized protocols reinforces the need for more high-quality research to establish clear, evidence-based guidelines focused exclusively on primary prevention for the use of the interventions found.
Therefore, the importance of these interventions lies in their low cost, feasibility, and potential for home implementation, factors that will influence public health. When supported by adequate professional guidance and contextualized to the needs of lactating women, these strategies can reduce pain, prevent the appearance of nipple-areola lesions, and contribute to the continuation of breastfeeding.
Consequently, strengthening primary prevention interventions represents a relevant and accessible approach to reduce early weaning and promote maternal and child health.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO NMH NHD Global Nutrition Targets 2025—Breastfeeding Policy Brief Available online: https://iris.who.int/bitstream/handle/10665/149022/WHO_NMH_NHD_14.7_eng.pdf?sequence=1(accessed on 8 February 2025)
- 2Victora C.G. Bahl R. Barros A.J. França G.V. Horton S. Krasevec J. Murch S. Sankar M.J. Walker N. Rollins N.C. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect Lancet 201638747549010.1016/S 0140-6736(15)01024-726869575 · doi ↗ · pubmed ↗
- 3Christian P. Smith E.R. Lee S.E. Vargas A.J. Bremer A.A. Raiten D.J. The need to study human milk as a biological system Am. J. Clin. Nutr.20211131063107210.1093/ajcn/nqab 07533831952 PMC 8106761 · doi ↗ · pubmed ↗
- 4Louis-Jacques A.F. Stuebe A.M. Enabling breastfeeding to support lifelong health for mother and child Obstet. Gynecol. Clin. N. Am.20204736338110.1016/j.ogc.2020.04.00132762923 · doi ↗ · pubmed ↗
- 5Rollins N.C. Bhandari N. Hajeebhoy N. Horton S. Lutter C.K. Martines J.C. Piwoz E.G. Richter L.M. Victora C.G. Why invest, and what it will take to improve breastfeeding practices?Lancet 201638749150410.1016/S 0140-6736(15)01044-226869576 · doi ↗ · pubmed ↗
- 6Oliveira F.S. Vieira F. Cecilio J.O. Guimarães J.V. Campbell S.H. The effectiveness on health education to prevent nipple trauma from breastfeeding: A systematic review Rev. Bras. Saúde Matern. Infant.20202034736910.1590/1806-93042020000200002 · doi ↗
- 7Patil D.S. Pundir P. Dhyani V.S. Krishnan J.B. Parsekar S.S. D’Souza S.M. Ravishankar N. Renjith V. A mixed-methods systematic review on barriers to exclusive breastfeeding Nutr. Health 20202632334610.1177/026010602094296733000699 · doi ↗ · pubmed ↗
- 8Cervellini M.P. Coca K.P. Gamba M.A. Marcacine K.O. Abrão A.C.F.V. Construction and validation of an instrument for classifying nipple and areola complex lesions resulting from breastfeeding Rev. Bras. Enferm.202275 e 2021005110.1590/0034-7167-2021-005134614083 · doi ↗ · pubmed ↗