Cardiac CT Angiography in Diagnosing Patent Foramen Ovale: A Study on Patients with Suspected Patent Foramen Ovale-Associated Stroke
Lijie Sun, Chong Zheng, Zhenxing Fan, Jing Gao, Zhi Liu, Jin Si, Keling Xiao, Ming Yi, Haoyu Zhang, Jinghao Sun, Yijin Liu, Yang Hua, Yingqi Xing, Jie Lu, Jing Li

TL;DR
This study shows that cardiac CT scans can help diagnose a heart condition called patent foramen ovale, especially in patients with larger blood flow between heart chambers.
Contribution
The study identifies that cardiac CTA's effectiveness in detecting PFO depends on the size of the right-to-left shunt.
Findings
Cardiac CTA had a sensitivity of 70% and a specificity of 100% for detecting PFO compared to TEE.
Patients with moderate-to-large shunts had a 90% CTA sensitivity for PFO detection.
Small shunts were more likely to result in false-negative CTA results.
Abstract
Background: Cardiac computed tomographic angiography (CTA) detects patent foramen ovale (PFO) with variable accuracy. This study investigated factors affecting CTA detectability for PFO in patients with suspected PFO-associated stroke. Methods: Consecutive patients with cryptogenic stroke and positive findings on contrast transcranial Doppler (cTCD) examinations were enrolled between November 2020 and April 2023 in this retrospective study. Each participant underwent transesophageal echocardiography (TEE) and cardiac CTA. Patients with confirmed PFO on TEE were categorized into two groups based on CTA detectability: the CTA-positive group (PFO identified by CTA) and the CTA-negative group (PFO missed by CTA). Univariate and multivariate logistic regression analyses were performed to identify predictors of CTA false-negative results. Results: Among 108 patients (mean age 46.7 ± 14.9…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
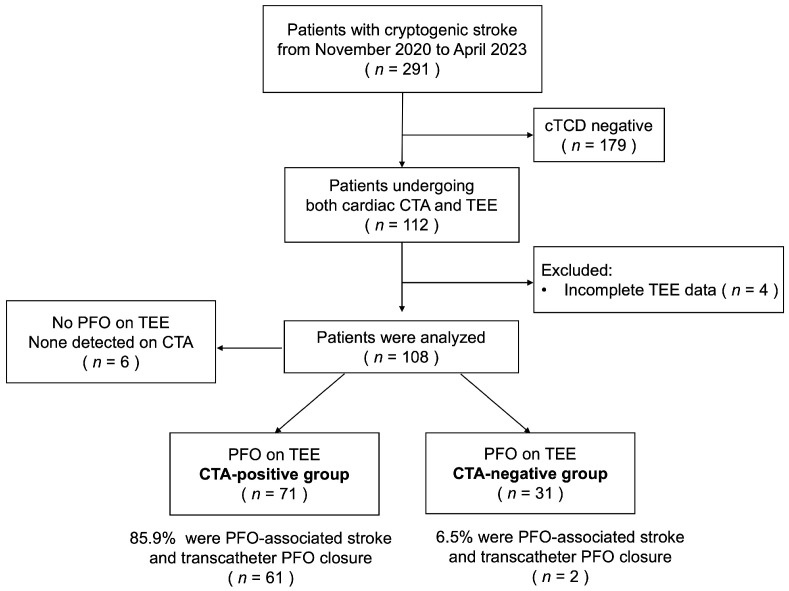 Figure 1
Figure 1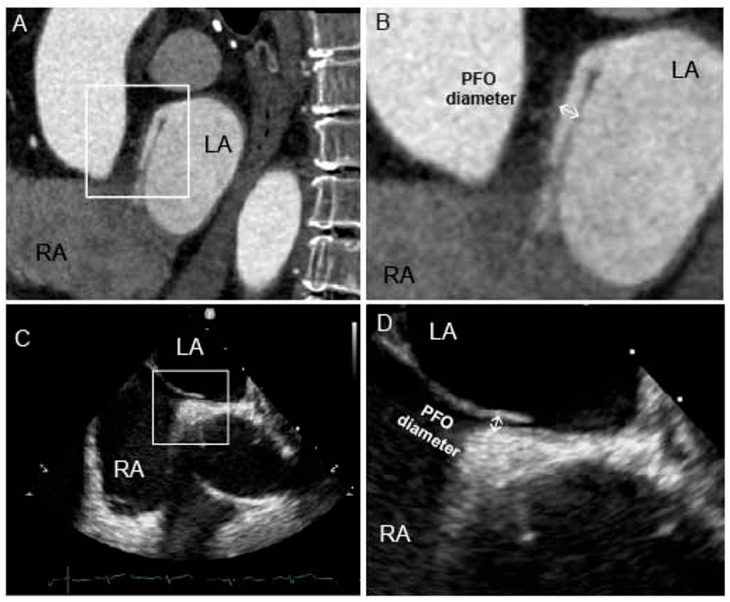 Figure 2
Figure 2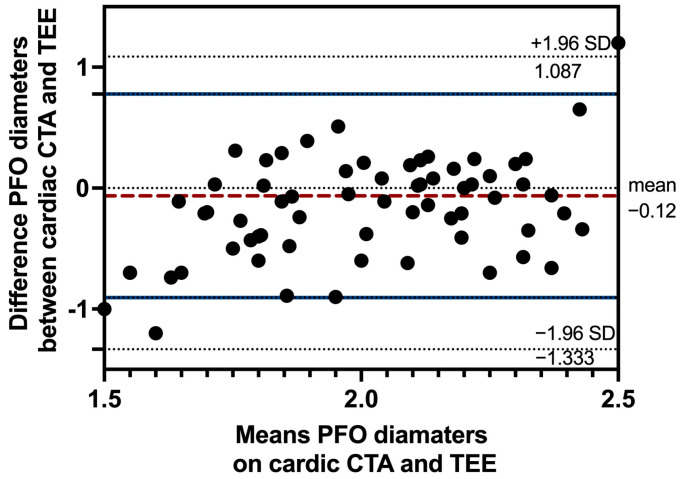 Figure 3
Figure 3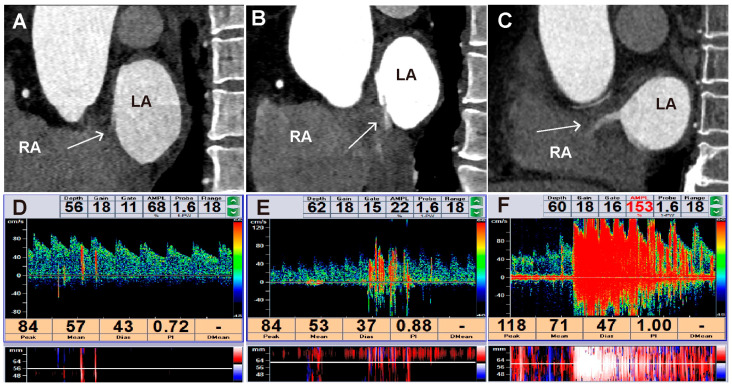 Figure 4
Figure 4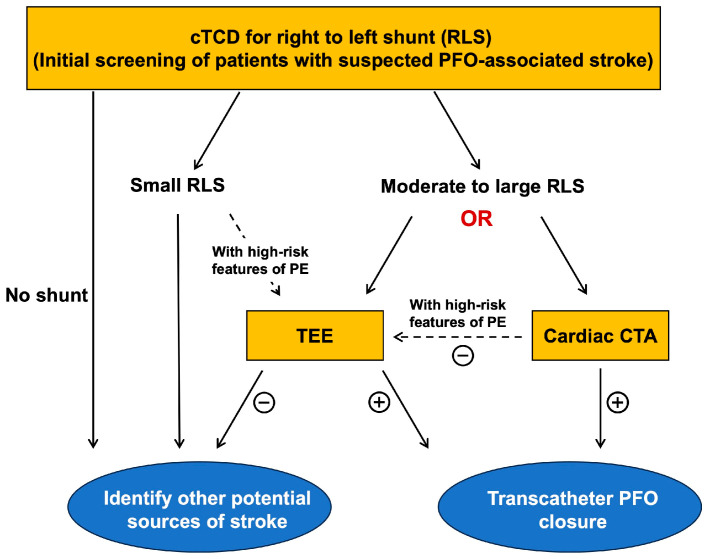 Figure 5
Figure 5- —National Natural Science Foundation of China
- —Beijing Municipal Public Welfare Development and Reform Pilot Project for Medical Research Institutes
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular and Diving-Related Complications · Vascular Anomalies and Treatments · Cardiovascular Conditions and Treatments
1. Introduction
Patent foramen ovale (PFO)-associated stroke is a recently proposed classification of ischemic stroke, occurring in patients with PFO after excluding other potential causes of stroke [1]. Epidemiological studies indicate that PFO-associated stroke accounts for 5% of ischemic strokes, with this proportion exceeding 10% in adults aged 18 to 60 years. Consequently, screening PFO should be mandatory when evaluating cryptogenic stroke [2]. Screening imaging modalities include contrast transcranial Doppler (cTCD), transthoracic echocardiography (TTE), transesophageal echocardiography (TEE), and agitated saline contrast echocardiography [3]. According to guidelines and expert consensus, TEE is regarded as the “gold standard” for diagnosing PFO and conducting anatomical evaluations prior to closure [4]. Nevertheless, it is not considered a mandatory examination. As a semi-invasive technique, TEE may induce discomfort during the procedure, which compromises patient cooperation. It is also associated, although rarely, with potential life-threatening complications [5]. Alternative modalities, such as cTCD and TTE, also have certain limitations. cTCD can reliably detect right-to-left shunt (RLS) but cannot localize the anatomical origin of the shunt [6]. TTE has limited sensitivity (50–73.3%) due to signal attenuation from thoracic structures and false positives from intrapulmonary shunt [7,8]. Therefore, optimizing the PFO diagnostic algorithm remains a clinical priority for screening causes of ischemic stroke.
Cardiac computed tomography angiography (CTA), with its high temporal and spatial resolution, enables comprehensive visualization of intracardiac pathologies including thrombi, valvular anomalies, cardiac neoplasms, and complex aortic atherosclerotic plaques [9,10]. It demonstrates considerable utility in etiological screening for acute ischemic stroke [11]. Notably, cardiac CTA facilitates non-invasive diagnosis of PFO through dynamic visualization of contrast jets and channel-like appearances (CLA), which represent the anatomical tunnel between atrial chambers [12]. But its diagnostic performance for PFO detection varies significantly across studies, with sensitivity ranging from 25% to 83% [13,14]. Kim et al. demonstrated that cardiac CTA had a sensitivity of 73.1% (95% CI 64.2–81.0%) and a specificity of 98.4% (95% CI 94.6–99.8%) in a comparative cohort of 152 stroke patients [15]. Conversely, Rinkel et al. reported the sensitivity of cardiac CTA is 25% (95% CI 14–94%) in acute ischemic stroke patients [16]. Diagnostic discrepancies may be attributed to various factors, including populations’ selection bias, individual heterogeneity, and technical parameters [17]. Identifying influencing factors could facilitate the clinical application of cardiac CTA. However, relevant research remains limited.
In this study, we investigated the potential factors affecting the detectability of cardiac CTA in the identification of PFO and to optimize the clinical application of this imaging modality in patients with suspected PFO-associated stroke.
2. Materials and Methods
Consecutive patients with suspected PFO-associated stroke admitted to Xuanwu Hospital Capital Medical University were enrolled from November 2020 to April 2023, and each patient underwent both cardiac CTA and TEE during the same hospitalization. No specific treatments were performed between the two examinations. Patients with confirmed PFO on TEE were categorized into two groups based on CTA detectability: the CTA-positive group (PFO identified by CTA) and the CTA-negative group (PFO missed by CTA). Baseline characteristics were compared between the two groups.
2.1. Study Population
The study flowchart is presented in Figure 1. All patients presenting with symptoms of ischemic stroke underwent initial evaluation in the Department of Neurology. This comprehensive evaluation included cranial CT or magnetic resonance imaging, carotid and cerebral artery ultrasonography, 24 h or longer cardiac rhythm monitoring, coagulation and immunological function tests, and cTCD examination. Patients lacking an identifiable cause of stroke and exhibiting positive findings on cTCD were considered potential candidates for PFO-associated stroke and were subsequently enrolled in this study. They were referred to the Department of Cardiology for PFO detection using TEE and cardiac CTA, the images of which were independently interpreted by specialized teams led by senior cardiologists.
The study was conducted in accordance with the Declaration of Helsinki and received approval from the Ethics Committee of Xuanwu Hospital, Capital Medical University (NO. 2023048). Written informed consent was obtained from all patients.
2.2. Cardiac CTA Examination and Image Reconstruction
All CTA examinations were performed using a third-generation dual-source CT scanner (SOMATOM Force; Siemens Healthineers, Forchheim, Germany). The patients underwent scanning with a retrospective electrocardiograph-gated technique in a breath-holding state.
Contrast medium was administered into the right antecubital vein at a flow rate of 5.0 mL/s using a high-pressure syringe, followed by 25 mL of normal saline at the same flow rate. Automated bolus-tracking technology was used, with the region of interest positioned at the level of the descending aorta. Scanning was initiated automatically 5 s after the trigger threshold surpassed 80 Hounsfield units (HU). The scan covered an area from the tracheal bifurcation to approximately 1 cm below the diaphragmatic surface of the heart. The acquisition parameters were set as follows: tube voltage at 120 kV, tube current at 300 mA, pitch factor at 1.375, field of view at 40 cm, and slice thickness at 0.625 mm. During scanning, images with a reconstruction interval of 5 mm were automatically generated by the CT system for routine review. Total scan time ranged from 6.0 to 9.0 s.
Following acquisition, the raw CTA data were transferred to a Siemens post-processing workstation (Syngo.via VB40, Siemens Healthineers, Forchheim, Germany) for reconstruction. The images were reconstructed with a slice thickness of 1 mm and a reconstruction interval of 1 mm for further analysis, using mid-diastolic and end-systole phase. Axial images exhibiting optimal clarity and absence of motion artifacts were selected by consensus for multiplanar reconstruction of the fossa ovalis region. The criteria for detecting PFO in cardiac CTA include the presence of a CLA with a contrast jet (Figure 2A). CLA was defined as a continuous contrast-filled tract between the septum primum and septum secundum, and contrast jet was defined as a linear column of contrast agent extending from the left atrium into the right atrium during the diastolic phase. To ensure diagnostic reliability, this tract was required to be visible on at least two consecutive slices in the axial view and confirmed on sagittal or coronal views. Using the four-chamber view as an anatomical reference, sagittal–oblique planes perpendicular to the interatrial septum were generated to visualize the PFO tunnel. The PFO diameter was measured at the midpoint of the tunnel (Figure 2B). The analysis of cardiac CTA images was performed by two radiologists, both of whom were blinded to the TEE and cTCD results. Any discrepancies in interpretation were resolved by consensus.
2.3. TEE Protocol
TEE was performed using a Philips CX50 (Philips Healthcare, Andover, MA, USA) equipped with a 4–7 MHz multiplane transducer. All patients underwent a comprehensive TEE examination, which included standardized views of the interatrial septum, two-dimensional imaging, color Doppler flow assessment, and agitated saline contrast testing. The echocardiographic images were independently analyzed by two researchers. A PFO was identified as an incompletely fused interatrial channel, as shown in Figure 2C. The diameter of the PFO was measured as the maximum distance between the septum primum and septum secundum during continuous scanning of the interatrial septum (Figure 2D). The agitated saline contrast test was performed with a mixture of 9 mL of saline with 1 mL of air and a drop of the patient’s blood, which was administered through the right antecubital vein. To ensure consistency across examinations (cTCD, TEE, and CTA), the same injection site was prioritized for each patient, unless compromised venous access required a change. RLS was identified by the presence of microbubbles in the left atrium within three cardiac cycles. The shunts were categorized based on the number of microbubbles: a small shunt was defined as having 1–10 microbubbles; a moderate shunt as having 11–30 microbubbles; and a large shunt as having more than 30 microbubbles.
2.4. Contrast-Enhanced Transcranial Doppler (cTCD) Examination
cTCD was performed using a Multi-DopX4 TCD detector (DWL, Solingen, Germany) with a 2 MHz probe, which facilitated monitoring of the middle cerebral artery through the temporal window. The agitated saline contrast test was carried out as previously described. The agitated saline solution was injected three times at rest and three times during the Valsalva maneuver, which was standardized by instructing patients to exhale forcefully into a manometer until achieving and maintaining a pressure of 50–60 mmHg for at least 5–7 s. Based on the appearance of microbubbles in the cTCD spectrum, shunts were categorized into three grades: a small shunt with 1–10 microbubbles; a moderate shunt with 11–30 microbubbles; and a large shunt with more than 30 microbubbles or when individual microbubbles were indistinguishable within the cTCD spectrum.
2.5. Statistical Analysis
Using TEE as the reference standard, the diagnostic performance of cardiac CTA for PFO detection were evaluated. A Shapiro–Wilk test was used to verify whether continuous variables met the normal distribution. Continuous variables with normal distribution were presented as mean ± standard deviation, and non-normal variables were reported as median (interquartile range). Group comparisons were made using Fisher’s exact test, χ2 test, or Student’s t tests, as appropriate. The agreement between TEE and cardiac CTA for measuring the diameter of PFO was calculated using Bland–Altman plots. To identify independent predictors of CTA false-negative results, a multivariate logistic regression analysis was performed. Variable selection was guided by statistical significance (p < 0.05 in univariate analysis) and clinical relevance. Specifically, potential confounders known to influence cardiac imaging quality or PFO characteristics were included if they met the statistical threshold. All statistical analyses were performed by using SPSS software (version 26.0, IBM SPSS, Chicago, IL, USA). Statistical significance was assumed at a level of p ≤ 0.05.
3. Results
3.1. Diagnostic Accuracy of Cardiac CTA in Detecting PFO
A total of 108 patients were included in the study, with a mean age of 46.7 ± 16.9 years, and 47.2% of them were male. Of these, 102 patients (94%) were diagnosed with a PFO through TEE, while 6 patients (5.6%) were not diagnosed with PFO. Cardiac CTA accurately identified PFO in 71 (69.6%) of all patients with PFO, while it failed to visualize PFO in 31 (30.4%) patients. Furthermore, cardiac CTA correctly identified all patients without PFO. As demonstrated in Table 1, the sensitivity of cardiac CTA was 70% (95% CI 61–79%), while its specificity was 100% (95% CI 54–100%). The positive and negative predictive values were 100% (95% CI 95–100%) and 16% (95% CI 6–32%), respectively.
3.2. Agreement Between Cardiac CTA and TEE in Measuring PFO Diameter
The diameter of the PFO is a critical anatomical parameter for transcatheter closure in patients with PFO-associated strokes. We analyzed agreement between cardiac CTA and TEE in measuring PFO diameter. This analysis included images from 71 patients with PFO confirmed by both modalities (Figure 2). The average PFO diameter measured by cardiac CTA was 2.03 ± 0.59 mm, compared to 2.15 ± 0.36 mm by TEE. In Figure 3, Bland–Altman plots demonstrated a mean inter-method difference of −0.12 ± 0.62 mm, with 95% limits of agreement ranging from −1.33 mm to 1.09 mm. The distribution of differences showed no systematic bias trend across measurement ranges, with 3/71 (4.2%) data points outside the 95% limits of agreement.
3.3. Patient Characteristics
Patients were categorized into two groups based on CTA detectability for PFO detection: CTA-positive group (PFO identified by CTA) and CTA-negative group (PFO missed by CTA). Table 2 presents the baseline characteristics of both groups. Patients in the CTA-positive group were younger (44.0 ± 12.8 vs. 52.9 ± 17.5 years, p = 0.005) and had a lower prevalence of chronic disease, including hypertension (25.4% vs. 54.8%, p = 0.004) and coronary artery disease (CAD) (1.4% vs. 22.6%, p < 0.001), compared with those in the CTA-negative group. The RoPE score in the CTA-positive group was significantly higher than in the CTA-negative group (6.1 ± 1.8 vs. 4.5 ± 2.2 score, p < 0.001). The proportion of patients classified as ‘probable’ under the PASCAL classification system was greater in the CTA-positive group than in the CTA-negative group (39.4% vs. 9.7%, p < 0.001).
The anatomical characteristics of PFO and the functional shunt between the two groups are shown in Table 3. There were no statistically significant differences in anatomical parameters as measured by TEE between groups, including PFO diameter, atrial septal aneurysm, Eustachian valve and atrial septal defect. Nevertheless, the prevalence of moderate to large RLS was significantly higher in the CTA-positive group compared to the CTA-negative group, as determined by contrast-enhanced TEE (67.6% vs. 25.8%, p < 0.001) and cTCD (77.5% vs. 22.5%, p < 0.001).
3.4. The Factors Influencing the Agreement Between Cardiac CTA and TEE
The factors influencing the agreement between cardiac CTA and TEE were investigated using both univariable and multivariable logistic regression analyses, with results presented in Table 4. After adjusting for age, gender, hypertension, CAD, and LA diameter, moderate to large RLS was significantly associated with a significantly reduced risk of a false-negative CTA result (OR 0.113, 95% CI 0.035–0.365, p < 0.001).
Table 5 displays the sensitivity of cardiac CTA in diagnosing PFO among various subgroups. Among the 61 patients with PFO who had moderate to large RLS confirmed by cTCD, cardiac CTA correctly diagnosed PFO in 55 patients, achieving a sensitivity of 90.16% (95% CI 82.69–97.64%). Figure 4 illustrates the different grades of interatrial shunt observed using cardiac CTA and cTCD.
4. Discussion
Our findings suggest that cardiac CTA can serve as an effective diagnostic tool for patients with suspected PFO-associated stroke. Its diagnostic performance appears more reliable for identifying PFO in patients with moderate-to-large RLS than in those with small RLS. Given that patients with moderate to large RLS are considered candidates for transcatheter PFO closure, our results also indicate that cardiac CTA can serve as a valuable diagnostic tool in these patients.
Unlike traditional treatments for atherosclerosis-related stroke, transcatheter closure demonstrated superior efficacy over medical therapy in preventing stroke recurrence in patients with PFO-associated stroke [18]. It is crucial to accurately identify PFO in patients with cryptogenic stroke to select the most appropriate treatment strategy [19]. TEE, considered the “gold standard” for PFO diagnosis, has limited applicability due to its semi-invasive procedure, which is often not well tolerated [20]. Although complications are rare, they can occur during the procedure. Furthermore, many primary healthcare facilities often lack TEE equipment, and reliance on TTE combined with agitated saline contrast may lead to underdiagnosis of PFO [21]. TEE is not considered a mandatory examination for screening PFO according to current guidelines [3,4]. Alternative imaging modalities are essential to enhance the diagnostic algorithms for PFO.
Cardiac CTA is a reliable alternative modality for evaluating cardioembolic sources in ischemic stroke, capable of imaging and diagnosing PFO [22,23]. However, its diagnostic performance for PFO detection varies across different studies. Lee et al. reported that the sensitivity and specificity of cardiac CTA were 89.4% and 92.3%, respectively [13], while Kara et al. reported a sensitivity of 53% and a specificity of 75% [24]. These variations may be attributed to differences in the selection of target populations. In cohorts of acute stroke patients, the sensitivity of cardiac CTA for diagnosing PFO was only 25% [16], whereas it increased to 81.8% in patients with ischemic stroke [13]. This study reported 70% sensitivity for PFO detection using cardiac CTA in patients suspected of having PFO-associated strokes. This sensitivity is slightly lower than that reported in studies using dedicated PFO protocols. This discrepancy is likely attributable to the retrospective nature of our study, where the primary indication for cardiac CTA in most patients was the evaluation of coronary artery disease rather than PFO screening. Consequently, a standard coronary CTA protocol was utilized without the Valsalva maneuver, and image acquisition timing was optimized for the coronary arteries rather than the right atrium. Thus, the diagnostic efficacy of cardiac CTA may be influenced by patient heterogeneity and diagnostic criteria. Unlike TEE, which directly visualizes the anatomical details of the primary and secondary septum through ultrasound signals, cardiac CTA utilizes on X-ray tomography technology to identify PFO, mainly through the anatomical features of CLA or contrast jets between the left and right atrium. Miki et al. found that the positive predictive value of “CLA combined with contrast jet” was higher (90.5%) than that of CLA alone (45.7%) for PFO detection [23]. These findings underscore the significant impact of interatrial shunt characteristics on the diagnostic accuracy of cardiac CTA for PFO.
Our results suggest that the degree of the interatrial shunt significantly influences the diagnostic accuracy of cardiac CTA in diagnosing PFO. Left-to-right shunting is common in most patients with PFO and right-to-left shunting [25]. Cardiac CTA relies on the pressure gradient between the left and right atrium to facilitate the shunting of contrast agent, thereby indirectly imaging the shunting. Insufficient pressure or small shunt volumes may lead to insufficient contrast agent shunting signs, potentially resulting in undetected PFOs. In addition, patients with PFO accompanied by moderate to large RLS requires special attention in clinical practice, given their high risk of stroke induced by thrombus passage through the PFO. Patients with a RoPE score exceeding [6] and a large shunt are classified as “probable” according to the PASCAL classification system, suggesting a causal relationship between their strokes and the PFO. These patients are likely to benefit from transcatheter PFO closure [17]. Consequently, the degree of interatrial shunt not only influences the diagnostic accuracy of cardiac CTA for PFO detection but also plays a crucial role in risk stratification and therapeutic decision-making in PFO-associated stroke. Therefore, it is essential to evaluate the degree of right–left shunting by cTCD before cardiac CTA for PFO detection. However, it is important to acknowledge the technical limitations of standard cardiac CTA. In our study, patients performed a standard inspiratory breath-hold solely to minimize respiratory motion artifacts. The absence of a Valsalva maneuver is a critical factor limiting diagnostic sensitivity, particularly for small shunts. Under resting conditions without provocation, the interatrial pressure gradient may be insufficient to open the flap valve of a small PFO, causing it to remain functionally closed and undetectable on static CT images. Future studies implementing technical adjustments could significantly enhance diagnostic accuracy. Specifically, dynamic CTA, which acquires images throughout the cardiac cycle during a Valsalva maneuver, has shown promise in visualizing the transient opening of the PFO flap. Additionally, incorporating delayed-phase imaging may help capture shunts that are not visible during the peak arterial phase.
Evaluating the anatomical structure of PFO and measuring its diameter are crucial for selecting the appropriate occluder devices for transcatheter PFO closure. Saremi et al. reported that the capability of cardiac CTA to measure key anatomical features of the PFO, including the length of the free edge of interatrial septum, the length of the fossa ovalis, and the thickness of the septum secundum [26]. Similarly, Xiong et al. found that cardiac CTA and TEE provided consistent measurements of the PFO tunnel length and the diameter of the left atrial entrance [14]. The present study showed that PFO diameters measured by cardiac CTA showed consistency with the results of the TEE measurement. However, the absence of standardized cardiac CTA protocols for measuring PFO anatomical structures may result in significant discrepancies across different studies, thereby limiting the clinical applicability of this technique.
Given the high specificity of cardiac CTA observed in our study, we propose enhancements to the diagnostic and treatment algorithm for PFO-associated stroke (Figure 5). After excluding common etiologies in stroke patients, those exhibiting a moderate to large shunt, as indicated by cTCD, and suspected of having a PFO-associated stroke, may benefit from cardiac CTA. Patients with a CTA-confirmed PFO may proceed directly to closure therapy, whereas those with negative CTA findings should undergo further evaluation with TEE. This modality can identify PFO and other potential cardiac sources of embolism. This diagnostic algorithm streamlines clinical workflows and minimizes unnecessary invasive procedures.
Limitations
There are some limitations. First, this is a small-scale retrospective analysis, and some patients lacked original imaging data, which restricted the concurrent assessment of additional anatomical features such as PFO length and atrial septum secundum thickness. Second, cardiac CTA images were reconstructed using only mid-diastolic and end-systole phase, which precluded evaluation of the entire cardiac cycle. This imaging method potentially led to incomplete characterization of PFO dynamics and false-negative results. Third, the inability to perform the Valsalva maneuver during cardiac CTA limited the assessment of shunts through the PFO under standard imaging conditions. Future research should explore the integration of advanced techniques that enable the performance of Valsalva maneuver during cardiac CTA, thereby facilitating the evaluation of right-to-left shunts. In addition, our cohort was highly enriched with PFO-positive patients (prevalence 94.4%); selection bias may limit the generalizability of our findings. The specificity and negative predictive value cannot be reliably estimated due to the extremely low number of negative cases. Consequently, the reported diagnostic performance of cardiac CTA should not be generalized and must be interpreted with caution in unselected populations. Furthermore, the number of false-negative events in our cohort was relatively small (n = 31). While we included significant confounders in the multivariate model to adjust for bias, we acknowledge that the low events-per-variable ratio may lead to model overfitting and wider confidence intervals for some covariates. However, the primary association between shunt size and detection failure remained highly significant and robust. Finally, the image analysis in our study was performed by two radiologists using a consensus approach. Consequently, inter-observer variability was not strictly assessed, which may limit the reproducibility of our findings regarding subjective morphological features.
5. Conclusions
Cardiac CTA demonstrates high diagnostic value for PFO evaluation, particularly in patients with moderate-to-large RLS, where it shows superior accuracy compared to cases with small shunts. Therefore, in patients with suspected PFO-associated stroke who have positive preliminary screening results, cardiac CTA serves as a valuable tool for anatomical characterization and pre-procedural planning prior to transcatheter closure.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Elgendy A.Y. Saver J.L. Amin Z. Boudoulas K.D. Carroll J.D. Elgendy I.Y. Grunwald I.Q. Gertz Z.M. Hijazi Z.M. Horlick E.M. Proposal for updated nomenclature and classification of potential causative mechanism in patent foramen ovale–associated stroke JAMA Neurol.20207787810.1001/jamaneurol.2020.045832282016 · doi ↗ · pubmed ↗
- 2Saver J.L. Mattle H.P. Thaler D. Patent foramen ovale closure versus medical therapy for cryptogenic ischemic Stroke Stroke 2018491541154810.1161/STROKEAHA.117.01815329760277 · doi ↗ · pubmed ↗
- 3Pristipino C. Sievert H. D’a Scenzo F. Mas J.L. Meier B. Scacciatella P. Hildick-Smith D. Gaita F. Toni D. Kyrle P. European position paper on the management of patients with patent foramen ovale. General approach and left circulation thromboembolism Eur. Heart J.2019403182319510.1093/eurheartj/ehy 64930358849 · doi ↗ · pubmed ↗
- 4Silvestry F.E. Cohen M.S. Armsby L.B. Burkule N.J. Fleishman C.E. Hijazi Z.M. Lang R.M. Rome J.J. Wang Y. Guidelines for the echocardiographic assessment of atrial septal defect and patent foramen ovale: From the American Society of Echocardiography and Society for Cardiac Angiography and Interventions J. Am. Soc. Echocardiogr.20152891095810.1016/j.echo.2015.05.01526239900 · doi ↗ · pubmed ↗
- 5Hilberath J.N. Oakes D.A. Shernan S.K. Bulwer B.E. D’a Mbra M.N. Eltzschig H.K. Safety of transesophageal echocardiography J. Am. Soc. Echocardiogr.2010231115112710.1016/j.echo.2010.08.01320864313 · doi ↗ · pubmed ↗
- 6Palazzo P. Heldner M.R. Nasr N. Alexandrov A.V. Transcranial doppler with microbubbles: Screening test to detect and grade right-to-left shunt after an ischemic stroke: A literature review Stroke 2024552932294110.1161/STROKEAHA.124.04690739268611 · doi ↗ · pubmed ↗
- 7Mojadidi M.K. Winoker J.S. Roberts S.C. Msaouel P. Zaman M.O. Gevorgyan R. Tobis J.M. Accuracy of conventional transthoracic echocardiography for the diagnosis of intracardiac right-to-left shunt: A meta-analysis of prospective studies Echocardiography 2014311036104810.1111/echo.1258324689727 · doi ↗ · pubmed ↗
- 8Oliva L. Horlick E. Wang B. Huszti E. Hall R. Abrahamyan L. Developing a random forest algorithm to identify patent foramen ovale and atrial septal defects in Ontario administrative databases BMC Med. Inform. Decis. Mak.2022229310.1186/s 12911-022-01837-235387650 PMC 8988372 · doi ↗ · pubmed ↗